
If you’re a practice owner looking to outsource mental health billing, you’re probably exhausted from chasing insurance payments. If you run a mental health practice and you’re still handling billing in-house, there’s a good chance you’re leaving somewhere between $30,000 and $100,000 on the table every single year — and not even knowing it.
That’s not a scare tactic. That’s what the numbers show when you actually pull the AR aging reports, count the abandoned denials, and add up what a full-time biller really costs after benefits, payroll taxes, and turnover risk.
This guide breaks down all of it — the real cost of in-house billing, the 12 specific benefits of outsourcing, what an ROI model actually looks like for practices your size, and a step-by-step process for making the switch without disrupting your cash flow. Whether you’re a solo therapist weighing your options or a 10-provider group that suspects your current setup is underperforming, you’ll find clear, specific answers here.
What Is Outsourced Mental Health Billing?
Outsourced mental health billing means hiring a specialized external company to handle your entire revenue cycle — from insurance verification and coding through claim submission, denial management, and patient collections. Unlike a general medical billing service, a behavioral health specialist understands the nuances of psychotherapy CPT codes, MHPAEA parity compliance, and the documentation requirements that separate a paid claim from a denied one.
Here’s what this guide covers:
- The true cost of keeping billing in-house (most practice owners underestimate this by 50%)
- 12 data-backed benefits of outsourcing, with real numbers for each
- An honest ROI breakdown by practice size
- How to know if outsourcing is right for your specific situation
- A week-by-week transition guide that protects your cash flow
- 15 questions to ask any billing company before you sign a contract
Table of Contents
The Real Cost of In-House Mental Health Billing
What You’re Actually Paying (Most Practice Owners Underestimate By 50%)
Most practice owners think their billing costs them whatever their biller earns. “I pay her $52,000 a year,” they say. “That’s my billing cost.”
It isn’t. Not by a long shot.
When you run the real numbers — the ones your accountant would want you to track on a P&L statement — the true cost of an in-house biller for a three-provider group typically lands between $84,000 and $140,000 annually. Here’s why.
The salary is just the foundation. On top of base pay, you’re covering a benefits package that adds roughly 25% — health insurance, dental, vision, and retirement contributions run employers about $13,000 to $14,000 per year for a full-time employee. Then come payroll taxes: Social Security, Medicare, and federal and state unemployment taxes together add another 9 to 10% of wages, which works out to roughly $5,000 on a $52,000 salary.
From there, the costs get less visible. Your biller needs a desk, a computer, software licenses, and a clearinghouse subscription. That’s another $2,500 to $3,600 per year just for the technology side. Add continuing education, AAPC certification maintenance, and the 15 days of PTO you’re paying for when she isn’t working — and you’re closing in on $85,000 before you account for what happens when she leaves.
Turnover is the number that nobody calculates. According to MGMA data, business operations staff in medical practices — including billers — turn over at rates exceeding 33% in recent years. When a billing specialist leaves, the costs include recruiting, the lost productivity during the open position, the training ramp-up for a new hire, and the claims that age and expire during the chaos. Replacement costs for a specialized position run 50 to 150% of annual salary. For a $52,000 biller, that’s a $26,000 to $78,000 hit every time someone quits. Even annualized conservatively, that’s $7,800 to $12,600 per year baked into your true cost.
Then there’s the denial problem — and this is where the real money disappears.
Behavioral health claims are denied at rates that run 85% higher than general medical claims. Industry benchmarks show in-house billing teams in mental health practices average denial rates between 10% and 20%. The deeper problem: research consistently finds that 50 to 65% of those denied claims are never reworked or resubmitted. They just disappear. On a $600,000 practice with a 12% denial rate and 60% abandonment, that’s roughly $43,000 in revenue that evaporated — not because payers refused to pay, but because nobody followed up.
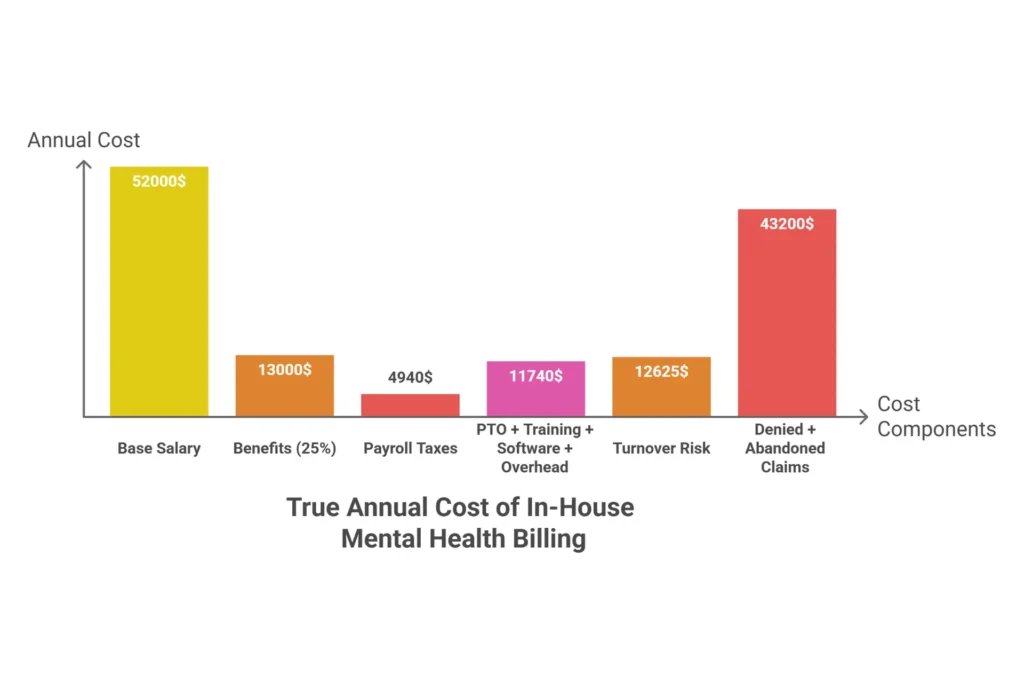
The full cost model for a three-provider practice looks like this:
| Cost Component | Annual Amount |
|---|---|
| Base Salary | $52,000 |
| Benefits Package (25%) | $13,000 |
| Employer Payroll Taxes | $4,940 |
| PTO + Sick Leave (15 days) | $3,000 |
| Training + AAPC Certification | $500 |
| Billing Software + Clearinghouse | $2,500 |
| Office Overhead (desk, tech, internet) | $6,240 |
| Subtotal Before Turnover + Losses | $82,180 |
| Annualized Turnover Risk | $12,625 |
| Error + Denial Losses (on $600K) | $43,200 |
| TRUE ANNUAL IN-HOUSE COST | $137,000+ |
Compare that to outsourcing the same function at 7% of collections: $42,000 per year. That’s a difference of $95,000 — and the outsourced option actually performs better on every measurable metric.
In the higher-cost states like California, New York, and Massachusetts, biller salaries run $65,000 to $80,000, pushing the true cost even higher. In Texas, Ohio, and Florida, salaries are lower ($45,000 to $58,000), but the denial problem and turnover risk are identical.
The “but my biller knows the practice” objection comes up every time this conversation happens. It’s understandable. Familiarity has real value. But here’s the honest counter: familiarity isn’t a billing KPI. If your familiar biller has a 16% denial rate and is abandoning 60% of those denials, she’s costing your practice more than a specialized outsourced team would — even if she’s been there for six years.
FREE PRACTICE AUDIT
Want to know what your practice is actually spending on billing?
Our Free Practice Revenue Audit runs the exact cost model above using your real numbers — and shows you the difference outsourcing would make for your practice specifically. Takes 48 hours. No obligation.
Request Your Free Audit →Top 12 Benefits of Outsourcing Mental Health Billing
When mental health practices make the switch to outsourced billing, they don’t just gain a service. They gain a financial infrastructure that’s almost impossible to build on your own — specialized expertise, enterprise-level technology, and accountability structures that in-house billing simply can’t match.
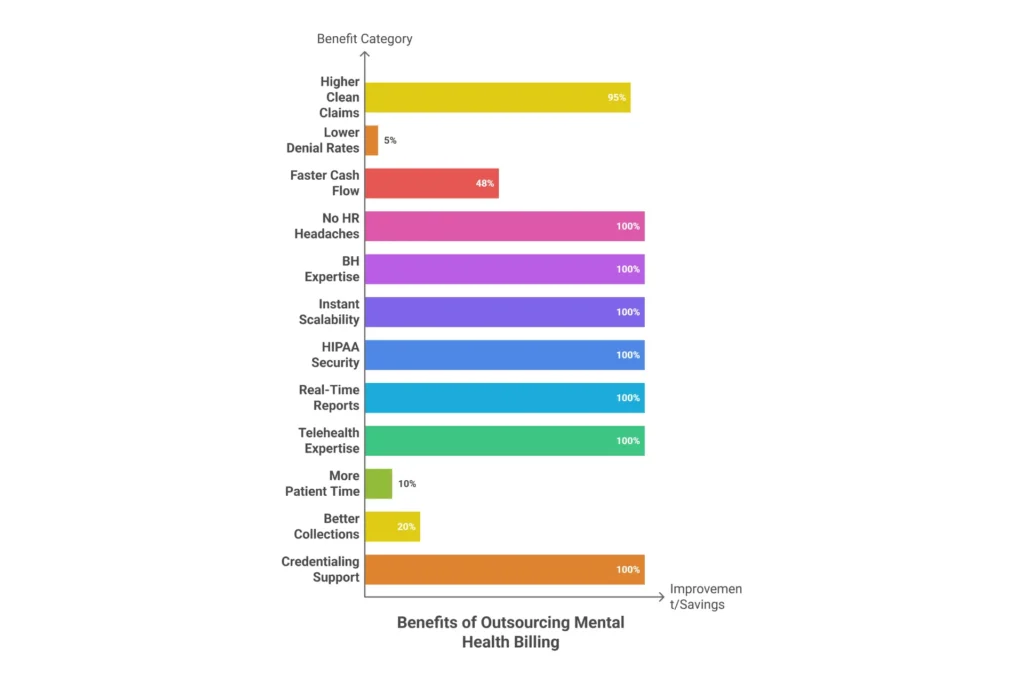
Here are the 12 most significant benefits, each with specific numbers rather than vague promises.
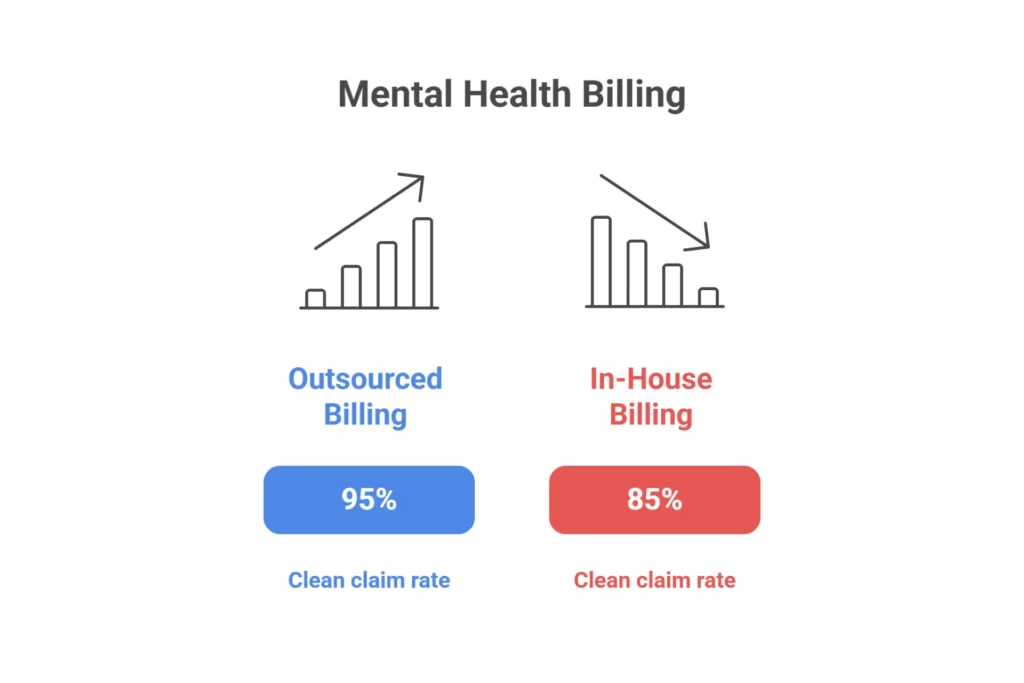
Benefit 1: Higher Clean Claim Rates
Specialized behavioral health billing companies consistently achieve clean claim rates of 92% to 98% , compared with the 80% to 90% average for in-house billing teams. For a $600,000 practice, a 10-point improvement in clean claims translates directly into faster reimbursement and $15,000 to $25,000 less in rework costs annually. This happens because outsourced coders build their entire career around behavioral health CPT codes — not just basic medical billing with an occasional 90837 thrown in.
Benefit 2: Dramatically Lower Denial Rates
In-house mental health billing teams average denial rates of 10% to 20% . Outsourced behavioral health specialists typically drive this down to 2% to 8% . The difference is expertise: knowing that BCBS requires different documentation for 90837 than UnitedHealthcare does, understanding when and how to use the 90785 interactive complexity add-on, and staying current on MHPAEA parity enforcement rules that most in-house billers have never read. A 5-point denial rate improvement on $600,000 in annual collections recovers $30,000 in previously lost revenue.
Benefit 3: Faster Reimbursement and Better Cash Flow
The average days-in-accounts-receivable for in-house mental health billing ranges from 45 to 60 days. With a professional outsourced team, that typically drops to 25 to 35 days. On $600,000 in annual collections, cutting 15 days off your AR cycle frees up roughly $24,000 in immediate working capital — money that was technically yours but sitting in the payers’ hands. For smaller practices, that difference can mean making payroll without stress.
Benefit 4: No More HR Headaches
The average biller turnover event costs $25,250 when you account for recruiting, temporary coverage, onboarding, and lost productivity. With an outsourced service, that risk disappears. Your vendor’s HR problems are your vendor’s problems — not yours. You also stop paying 9.5% in employer payroll taxes and stop covering PTO gaps when your biller is sick or on vacation.
Benefit 5: Genuine Behavioral Health Expertise
General medical billing and behavioral health billing are genuinely different disciplines. Mental health billing requires working knowledge of MHPAEA federal parity laws, 42 CFR Part 2 confidentiality rules for substance use disorder claims, crisis billing codes like 90839 and 90840 , and the documentation thresholds that distinguish a 90834 from a 90837. Most in-house billers who came from general medical practices have to learn this on your dime. Specialized outsourced teams arrive already knowing it.
Benefit 6: Scalability Without Growing Pains
When your practice adds two new therapists, your claim volume doubles. An in-house billing team either gets overwhelmed — and your denial rate climbs — or you have to hire. With an outsourced service, your billing scales instantly. The fee scales proportionally with revenue, meaning your billing cost per provider doesn’t change whether you have three clinicians or eight.
Benefit 7: Enhanced HIPAA Compliance and Security
Reputable behavioral health billing companies maintain HITRUST or SOC 2 Type II certification , sign Business Associate Agreements before they touch a single claim, use encrypted data handling, and conduct annual third-party security audits. For small practices, replicating this level of IT security internally is genuinely expensive. Outsourcing transfers a significant portion of HIPAA compliance risk to a vendor built to carry it.
Benefit 8: Real-Time Reporting You Can Actually Use
With a quality outsourced service, you stop relying on your biller’s end-of-month verbal summary. Instead, you have a secure dashboard showing AR aging by payer, denial rate trends, net collections by provider, and month-over-month performance comparisons — updated daily. This is the kind of financial visibility that lets practice owners make strategic decisions rather than reactive ones.
Benefit 9: Telehealth Billing Expertise
Telehealth billing rules are still evolving in 2026, and they vary by payer, state Medicaid program, and whether the service is video or audio-only. The difference between POS 02 (telehealth provided outside the patient’s home) and POS 10 (telehealth in the patient’s home) sounds minor — but using the wrong code can result in systematic denials across hundreds of claims. Specialized billing companies track CMS and AMA updates in real time and apply the correct modifiers automatically.
Benefit 10: More Time for What Actually Matters
APA research consistently finds that clinicians spend four to six hours per week on billing-related administrative tasks — follow-up calls, denial appeals, claim status checks. For a provider billing at $150 per hour, that’s $31,000 to $46,800 per year in lost clinical capacity. Outsourcing gives those hours back. Some practice owners use them to see more patients. Others use them to finally work normal hours.
Benefit 11: Professional Patient Collections
Patient responsibility collections are handled differently when your billing partner uses systematic, professional processes — automated statements, text-to-pay portals, and staff trained in sensitive conversations about cost. Most outsourced services improve self-pay collection rates by 15% to 25% over ad-hoc in-house efforts. On a practice where 10% of revenue is patient responsibility, that improvement alone adds $9,000 to $15,000 annually.
Benefit 12: Proactive Credentialing Support
Credentialing gaps and delays are one of the most common causes of preventable revenue freezes in mental health practices. A new therapist who can’t bill for 60 to 90 days after hire is costing the practice real money every week. Many outsourced billing partners include proactive credentialing management — CAQH profile updates, re-credentialing deadline tracking, new payer enrollment — as part of their service, eliminating the delays that cost practices 8% to 12% of potential new-hire revenue in the first quarter.
12 Benefits of Outsourcing Mental Health Billing — Summary
| Benefit | Key Data Point | Annual Impact on $600K Practice |
|---|---|---|
| 1. Higher Clean Claim Rates | 92–98% vs. 80–90% in-house | $15K–$25K less in rework costs |
| 2. Lower Denial Rates | 2–8% vs. 10–20% in-house | $30K+ in recovered revenue |
| 3. Faster Reimbursement | 28 days-in-AR vs. 45–60 days | $24K in freed working capital |
| 4. No HR/Turnover Risk | $25,250 per turnover event; 33% annual turnover rate | $7,800–$12,600 annualized risk eliminated |
| 5. BH Coding Expertise | MHPAEA, 42 CFR Part 2, 90785, telehealth modifiers | Prevents 8–12% of specialty-related denials |
| 6. Instant Scalability | Scales from 3 to 10+ providers without hiring | No performance drop during growth |
| 7. HIPAA + Data Security | SOC 2 Type II / HITRUST certified; BAA standard | Breach risk transferred to certified vendor |
| 8. Real-Time Reporting | Daily, weekly, monthly dashboards | Strategic decisions based on real data |
| 9. Telehealth Expertise | POS 02 vs 10, modifier 95, FQ, audio-only rules | 98%+ telehealth claim acceptance |
| 10. Clinical Time Recovered | 5–10 hours/week returned to providers | $39K–$78K in reclaimed clinical capacity |
| 11. Better Patient Collections | 15–25% improvement in self-pay collections | $9K–$15K additional on 10% patient responsibility |
| 12. Credentialing Support | Proactive CAQH, re-credentialing, new enrollments | Prevents 60–90 day new-hire revenue freeze |
How Outsourced Mental Health Billing Increases Revenue — The ROI Breakdown
Here’s the number every practice owner actually wants: how much more money will we collect?
Let’s start with the formula. Net Collections Rate equals total payments received divided by total allowable charges after contractual adjustments. Industry benchmarks say 90% to 95% is a healthy target. Practices below 85% are leaving meaningful money on the table. In-house mental health billing typically produces net collections rates of 75% to 85% . Outsourced behavioral health specialists consistently achieve 92% to 98% .
On $600,000 in annual billings, the difference between an 82% in-house rate and a 92% outsourced rate is $60,000 in additional collected revenue. That’s not a hypothetical. That’s the math.
Specific Revenue Leakage Points Outsourcing Captures
The 90785 Problem: Interactive complexity is a legitimate add-on code for standard psychotherapy sessions that involve crisis, caregivers, or language barriers. Research suggests that 40% to 60% of eligible mental health practices never bill it — not because it doesn’t apply, but because their billers don’t know the four criteria or don’t have a workflow to catch it. On 200 eligible sessions per year at $20 per add-on, that’s $4,000 in annual revenue sitting uncaptured.
Underpayment Detection: BCBS, Aetna, and UnitedHealthcare routinely process claims at rates below contracted amounts — often 5% to 15% below what your fee schedule says you’re owed. Most in-house billers don’t have the time or tools to audit every EOB against contracted rates. Outsourced companies with underpayment detection software catch these systematically. Annual recovery for a mid-size practice typically runs $15,000 to $30,000 in recaptured underpayments.
Timely Filing Losses: When a biller is sick, on vacation, or in the middle of leaving the practice, claims sit. Most commercial payers have 90-day filing windows. After that, the claim is gone. Outsourced teams with redundant staffing and daily submission protocols don’t miss filing deadlines.
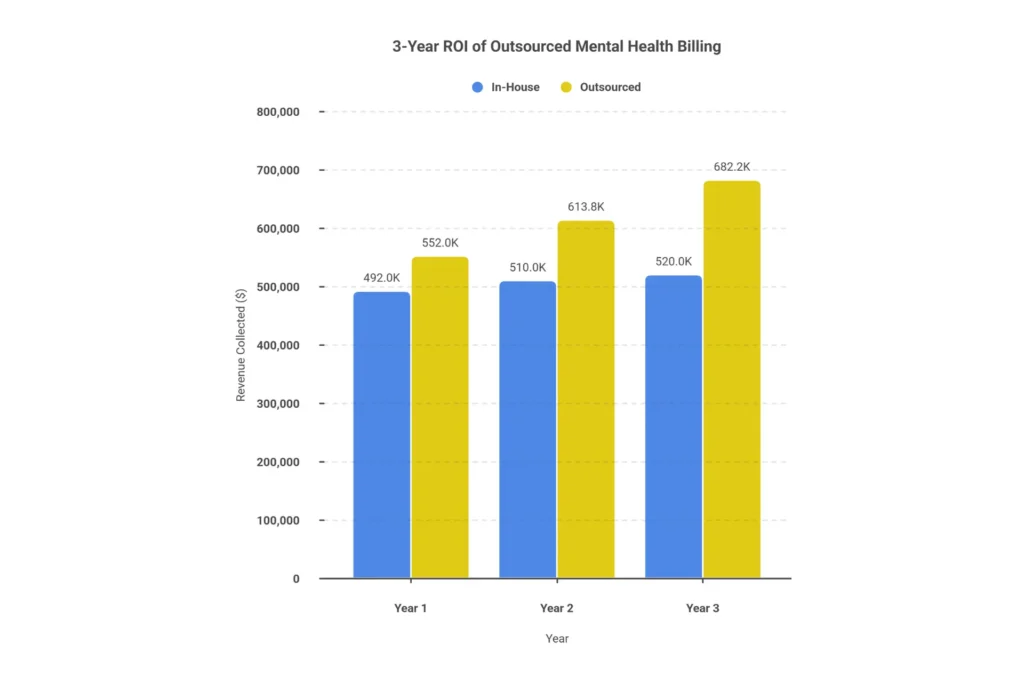
The 3-Year ROI Picture
For a three-provider practice billing $600,000 annually:
| Metric | Year 1 In-House | Year 1 Outsourced | Year 2 | Year 3 |
|---|---|---|---|---|
| Net Collections Rate | 82% | 92% | 93% | 94% |
| Revenue Collected | $492,000 | $552,000 | $613,800 | $682,200 |
| Billing Cost | $84,615 (in-house) | $42,000 (7% fee) | $42,966 | $47,754 |
| Annual Revenue Lift | — | +$60,000 | +$61,800 | +$68,400 |
| Cost Savings | — | $42,615 | $43,467 | $45,000 |
| Total Annual Benefit | — | $102,615 | $105,267 | $113,400 |
| Cumulative 3-Year Benefit | — | — | — | $321,282 |
Practice Size ROI Comparison
| Solo ($150K Rev) | Small Group ($400K Rev) | Mid-Size ($1M Rev) | |
|---|---|---|---|
| In-House Billing Cost | $18,000 (part-time) | $84,615 (1 FTE) | $220,000 (2 staff + mgr) |
| Outsourcing Cost (7%) | $10,500 | $28,000 | $70,000 |
| Net Collections Improvement | +$12,000 | +$32,000 | +$80,000 |
| Total Annual Benefit | $19,500 | $88,615 | $230,000 |
| Payback Period | 1.5 months | 2 months | Under 2 months |
For most practices, outsourcing pays for itself by month two or three. The revenue lift and cost savings combined exceed the monthly fee well before the end of the first quarter.
FREE TOOL
Mental Health Billing ROI Calculator
Enter your practice numbers to see your estimated annual benefit from outsourcing.
Is Outsourcing Mental Health Billing Right for Your Practice?
Is outsourcing medical billing a good idea?
Yes, for most practices generating over $20,000 monthly in insurance revenue. Outsourcing typically improves net collections from 75-85% to 92-98%, recovers 80-90% of denied claims versus 35-50% in-house, and reduces Days in AR from 60+ to under 35. It eliminates staff turnover costs and allows clinicians to focus on patient care.
Outsourcing mental health billing is the right choice for most therapy practices that handle insurance billing, have two or more providers, and are dealing with denial rates above 10%. It’s most valuable when a practice is growing, experiencing billing staff turnover, or struggling with telehealth billing accuracy. Solo self-pay practices are the primary exception.
That said, the decision isn’t identical for every practice. Here’s how it breaks down by size:
| Practice Type | Revenue Range | Recommended Approach | Primary Reason |
|---|---|---|---|
| Solo, cash-pay only | Under $100K | Self-bill or EHR software | No insurance complexity |
| Solo, 1-2 insurers | $100K–$200K | EHR billing or evaluate outsourcing | Run the ROI math |
| Solo, 5+ insurers | $150K–$250K | Strong case to outsource | Complexity exceeds one person |
| Small group, 2–5 providers | $300K–$800K | Outsource | Clear ROI, scalability |
| Mid-size, 6–15 providers | $800K–$3M | Outsource or hybrid | Scale justifies either |
| Large group, 15+ providers | $3M+ | Hybrid or internal department | Scale supports internal team |
Eight Signs You Should Outsource
- Your denial rate is above 12%
- Your days-in-AR exceed 40 days
- Your net collections rate is below 88%
- You’ve had biller turnover in the past two years
- You’re billing more than three insurance panels
- Your practice is growing faster than your billing can keep up
- You’re spending more than three hours per week on billing issues personally
- You genuinely don’t know what your denial rate is right now
When Outsourcing Probably Isn’t the Move
- You’re entirely cash-pay with zero insurance claims
- You’re under $100,000 in annual revenue and the outsourcing fee would represent more than 20% of that
- You already have an in-house team achieving 95%+ clean claims and 4% denial rates. Those practices exist — they’re the exception, not the rule, but they exist.
The Offshore/India Outsourcing Question
Practices searching for “cheap outsource mental health billing” will find plenty of India-based services advertising 4% to 5% fees. The appeal is obvious. The risk is real.
Mental health billing requires fluency in MHPAEA parity laws, 42 CFR Part 2 confidentiality requirements for substance use disorder claims, and US payer-specific authorization rules that change frequently. Enforcing HIPAA jurisdiction against an offshore vendor is genuinely difficult. Timezone gaps of 12 hours make real-time payer follow-up impractical. And the specialized behavioral health coding knowledge — the stuff that actually prevents denials — is harder to maintain when you’re not embedded in the US payer system daily.
For most mental health practices, the 2% to 3% fee savings don’t offset those risks.
Self-Assessment Checklist
If you answer yes to five or more of the following, outsourcing will almost certainly improve your financial performance:
| Question | Yes/No |
|---|---|
| Is your denial rate above 10%? | ☐ |
| Are your days-in-AR above 40? | ☐ |
| Have you experienced biller turnover in the past 24 months? | ☐ |
| Do you bill five or more insurance panels? | ☐ |
| Has your practice added providers in the past year? | ☐ |
| Do you bill for telehealth services? | ☐ |
| Does your practice handle any substance use disorder claims? | ☐ |
| Do you spend time each week personally chasing billing issues? | ☐ |
In-House vs. Outsourced Mental Health Billing — The Full Comparison
Is it better to outsource mental health billing or keep it in-house?
For most practices generating over $200,000 in annual insurance revenue, outsourcing is financially superior. Outsourcing delivers 92-98% net collections versus 75-85% in-house, reduces denial rates from 10-20% to 2-8%, and cuts Days in AR from 60 to under 35. A 4-provider group typically saves $102,000+ annually through outsourcing versus maintaining an in-house biller.
Outsourced mental health billing outperforms in-house billing on most measurable financial metrics: outsourced services average 96.5% clean claim rates versus 88% in-house, 28 days-in-AR versus 45 to 60 days in-house, and cost 5% to 9% of collections versus $58,000 to $97,500 for a full-time in-house biller — while eliminating HR risk and providing behavioral health specialization that generalist billers can’t match.
A Month in the Life: Two Identical Practices
Imagine two identical three-provider therapy groups. Same EHR, same payer mix, same collection goal of $600,000 per year. Practice A has a full-time in-house biller. Practice B uses a specialized outsourced service.
By the end of month one: Practice A has submitted 87% of claims cleanly. Thirteen percent are pending denials. The biller is prioritizing the new submissions and hasn’t worked the denial queue yet. Practice B has submitted 96% of claims cleanly, the 4% that bounced back were flagged and corrected same-day, and the denial queue from the previous month has been worked down by 80%.
By the end of month three: Practice A’s AR is sitting at 51 days. Two of the denied claims from month one expired their filing window while the biller was on vacation. Practice B’s AR is at 29 days. Their vendor flagged a systematic BCBS underpayment on 90837 and recovered $4,200 in recoupment.
By the end of year one: Practice A collected $492,000 and spent $84,615 in billing costs. Practice B collected $552,000 and paid $42,000 in outsourcing fees. The difference is $102,615 — more than a full-time employee’s salary — in Practice B’s favor.
Comprehensive Comparison Table
| Comparison Point | In-House | Outsourced |
|---|---|---|
| Annual Cost (3 providers) | $84,615 | $42,000 |
| Clean Claim Rate | 80–90% | 92–98% |
| Denial Rate | 10–20% | 2–8% |
| Days in AR | 45–60 | 25–35 |
| Net Collections Rate | 75–85% | 92–98% |
| Denial Recovery Rate | 35–50% | 80–90% |
| Staff Turnover Risk | 15–33% annually | Zero |
| Telehealth Billing Accuracy | Variable (frequent errors) | Expert (2026 rule current) |
| 42 CFR Part 2 Knowledge | Rarely trained | Standard expertise |
| Scalability | Requires new hire | Immediate |
| Reporting Quality | Basic EHR exports | Real-time dashboards |
| Credentialing Support | Internal delays | Proactive management |
| After-Hours Coverage | None | Team coverage |
| Performance Accountability | Internal, hard to enforce | SLA-backed benchmarks |
| Contract Flexibility | Fixed cost | Month-to-month available |
The Hybrid Model
The hybrid model deserves mention for larger practices. Some groups keep a front-end coordinator for patient intake, eligibility verification, and scheduling — functions that benefit from in-person presence — while outsourcing the back-end claims submission, denial management, and AR follow-up. This works well for practices above $1.5M in revenue and gives you the relationship benefits of in-house staff alongside the performance benefits of specialized billing.
EHR Integration
For EHR integration: TherapyNotes, SimplePractice, Kareo, and AdvancedMD all integrate with quality outsourced billing services. You should never have to change your EHR to accommodate a billing company. If a vendor tells you otherwise, that’s a red flag.
How to Transition to Outsourced Billing Without Disrupting Collections
The number one fear that stops practice owners from making the switch is losing revenue during the changeover. It’s a legitimate concern — and it almost never happens when the transition is done right.
The fear is usually based on assumptions: that the new vendor won’t understand the practice, that claims will fall through the cracks, that cash flow will dry up during the handoff. In reality, a well-structured transition maintains 95%+ of normal cash flow throughout the process and often creates a cash spike during months two and three as old AR gets recovered.
The Three Real Risks — and How to Prevent Each
| Risk | Prevention |
|---|---|
| Lost claims | Parallel processing — both in-house and outsourced submit simultaneously for 4 to 6 weeks before full handover |
| Cash flow gap | 30-day collections reserve + claims submitted every single business day during transition |
| Vendor learning curve | Week-one preparation — complete payer list, fee schedule, credentialing status, and active authorization inventory |
Pre-Transition Checklist (Before You Sign Anything)
☐ Pull a current AR aging report — document every open claim by age bucket
☐ List all active prior authorizations with expiration dates
☐ Compile credentialing status for all providers across all payers
☐ Calculate your baseline KPIs: current denial rate, days-in-AR, net collections rate
☐ Document your EHR and which modules you’re using for billing
Week-by-Week Transition Timeline
Weeks 1–2: Contract signed, Business Associate Agreement executed, EHR access granted to vendor. Fee schedule loaded and verified. CAQH profiles reviewed for all providers.
Weeks 3–4: Parallel processing begins. Vendor submits all new claims; in-house process handles existing open AR. Claims submit rate compared daily.
Weeks 5–8: Full handoff. Vendor takes complete responsibility for new claim submission. Legacy AR either remains with in-house (wind-down) or transfers to vendor on agreed contingency terms.
Weeks 9–12: First performance review. Denial rates, DAR, and net collections rate compared against your pre-transition baseline. Optimization of any payer-specific issues.
Month 4 and beyond: Full steady-state operations. Weekly reporting, monthly review calls, quarterly payer contract audits.
State-Specific Considerations
Practices in Florida, Texas, Connecticut, Virginia, Ohio, Massachusetts, Delaware, and Michigan all follow the same general transition framework, but state Medicaid programs each have their own portal enrollment requirements:
- Florida: FMMIS portal access must be verified in week one
- Texas: TMHP authorization transfer procedures should be confirmed
- Connecticut: HUSKY Health program has specific EDI enrollment steps
- Ohio: ODM portal enrollment must be current
- Virginia: Cardinal Care provider IDs need verification
- Massachusetts: MassHealth enrollment steps should be initiated week one
- Michigan: MiHIN requirements demand vendor familiarity
- Delaware: DHSS portal access is essential — don’t rely on batch file transfers
Ask your vendor specifically whether they have active access to your state’s Medicaid portal before you sign.
Staff Transition Options
Option A: The Lateral Move (Recommended) — Move your biller to Patient Care Coordination. They know your patients; have them focus on intake, benefit verification, and front-end collections. Keeps institutional knowledge while offloading technical back-end work.
Option B: The 90-Day Wind-Down — Keep biller to manage “Legacy AR” (old claims). Once cleared and new firm stable, the role naturally concludes.
Option C: The Clean Break — 4-8 week severance package. Cleanest but loses institutional knowledge.
What NOT to do: Don’t have your old biller “supervise” the new company. Creates defensive environment where they try to prove new firm is failing.
FREE DOWNLOAD
30-60-90 Day Billing Transition Checklist
Use this checklist to keep your transition on track and protect your cash flow throughout the process.
What to Expect When You Outsource Mental Health Billing
Once you’ve made the switch, a professional behavioral health billing service should feel less like handing something off and more like gaining a financial co-pilot who’s watching your numbers more carefully than you ever could.
The First 90 Days: What It Looks Like at a Quality Service
Days 1–3: Contract and BAA signed, EHR access granted, kickoff call completed. Vendor reviews existing payer contracts for rate accuracy. Any credentialing gaps flagged immediately.
Week 1: Fee schedule verified and loaded. Active authorizations reviewed. ERA/clearinghouse enrollment submitted to primary payers. Kickoff questions addressed — if your vendor can’t answer questions about 42 CFR Part 2 or 90785 interactive complexity criteria in week one, that’s a problem.
Week 2: First batch of new claims submitted. First ERAs received. Any immediate submission issues caught and corrected.
Month 2: Daily rhythm established. Denial patterns from weeks two and three identified and systematically addressed. Account manager fully familiar with your payer mix and coding patterns.
Month 3: Formal 90-day performance review. Current metrics benchmarked against your pre-transition baseline. If you’re not seeing measurable improvement in clean claims and denial rates by month three, that conversation needs to happen.
Reporting Standards You Should Demand
| Report | Frequency | What It Should Contain |
|---|---|---|
| Claims Submission | Daily | Claims submitted, total value, any same-day rejections |
| Denial Summary + AR Snapshot | Weekly | Denial codes, aging bucket movements, action items |
| Full Financial Report | Monthly | Charges, payments, adjustments, NCR, payer breakdown |
| Performance vs. Baseline | Quarterly | Year-over-year comparison, contract optimization |
Performance Benchmarks — Elite vs. Acceptable vs. Red Flag
| KPI | Elite | Acceptable | Red Flag |
|---|---|---|---|
| Clean Claim Rate | 95%+ | 90–94% | Below 90% |
| Net Collections Rate | 95%+ | 90–94% | Below 90% |
| Days in AR | Under 30 | 30–45 | Above 45 |
| Denial Rate | Under 5% | 5–10% | Above 10% |
| Denial Resolution Time | Under 5 days | 5–10 days | Over 10 days |
| Claims Submission Lag | Under 24 hours | 24–48 hours | Over 48 hours |
Six Signs Your Outsourced Service Is Underperforming
- Claims are consistently taking more than 48 hours to submit after session documentation
- Denial rate is still above 10% after the first 90 days
- You’re getting monthly PDF reports only — no real-time dashboard access
- Account manager turnover has happened twice in your first year
- You’re the one who discovers payer underpayments, not your vendor
- Collections haven’t exceeded your pre-outsourcing baseline by month three
Communication Standards
- Dedicated account manager (not a general support ticket queue)
- Response to inquiries within four business hours
- Weekly 30-minute calls during month one and two
- Monthly review meetings thereafter
15 Questions to Ask Any Outsourced Mental Health Billing Partner
Before you sign any billing service contract, ask every one of these questions. The answers — and how confidently they’re delivered — will tell you everything you need to know.
FREE VENDOR EVALUATION TOOL
15-Question Billing Partner Checklist
Print and bring to any vendor call. Evaluate any billing company in 15 minutes — before you sign anything.
SPECIALIZATION
Q1: What percentage of your billing portfolio is behavioral health?
- Why it matters: A vendor who bills ten specialties equally doesn’t have the depth of behavioral health knowledge you need.
- Good answer: “Behavioral health represents 75% or more of our client base.”
- Red flag: “We bill all specialties — we’re very adaptable.”
Q2: What are the five CPT codes you bill most often in mental health, and what are your denial rates by code?
- Why it matters: A specialist can answer this instantly. A generalist has to look it up.
- Good answer: Rattles off 90837, 90834, 90791, 90847, 90846 with specific denial rates per code.
- Red flag: Hesitation, vague answers, or “we track denials overall, not by code.”
Q3: Do your coders hold behavioral health-specific credentials or AAPC certifications?
- Why it matters: CPC certification + behavioral health continuing education is the minimum standard.
- Good answer: Specific credentials listed, ongoing AAPC education confirmed.
- Red flag: “Our team has medical billing experience.” (Doesn’t answer the question.)
Q4: Do you have current experience with my EHR and my specific payer mix?
- Why it matters: EHR integration affects submission speed and data accuracy. Payer-specific knowledge affects denial rates.
- Good answer: Names your EHR, describes how they connect, and mentions payer-specific rules for your top three insurers.
- Red flag: “We work with all EHRs” without specifics.
PERFORMANCE
Q5: What is your average clean claim rate across behavioral health clients?
- Good answer: 95% or higher, with data to back it up.
- Red flag: Below 90%, or “we don’t track that metric specifically.”
Q6: What is your average days-in-AR?
- Good answer: Under 35 days.
- Red flag: Above 45 days, or inability to answer.
Q7: What is your average net collections rate for mental health practices?
- Good answer: 93% or higher.
- Red flag: Anything below 88%, or “it depends on the practice.”
Q8: What is your denial rate and first-pass resolution rate?
- Good answer: Denial rate below 5%, first-pass resolution above 85%.
- Red flag: Denial rate above 10% or inability to provide both numbers.
TECHNOLOGY
Q9: Do you integrate directly with my EHR, or do you use manual exports?
- Why it matters: Manual CSV exports introduce errors and delay. Direct integration is the standard.
- Red flag: “We’ll just use a spreadsheet export.”
Q10: What reporting do I get, and can I see a sample dashboard right now?
- Good answer: Shows you an actual dashboard with daily, weekly, and monthly reporting views.
- Red flag: “We send a monthly PDF summary.”
Q11: Do I have 24/7 access to my data?
- Good answer: Yes — real-time portal with AR aging, denial trends, and provider-level collections.
- Red flag: Data access requires requesting a report.
COMPLIANCE AND TERMS
Q12: Are you HIPAA compliant and will you sign a BAA before we share any data?
- Good answer: Immediate yes, confirmed SOC 2 or HITRUST certification, BAA provided as standard.
- Red flag: Any hesitation, or “we’ll get to that after onboarding.”
Q13: How do you handle 42 CFR Part 2 compliance for substance use disorder claims?
- Good answer: Describes specific consent tracking protocols and staff training.
- Red flag: Blank stare or “that’s the same as HIPAA, right?” (It isn’t.)
Q14: Are your contracts month-to-month, or are you requiring annual commitments?
- Good answer: Month-to-month available after a 90-day ramp period.
- Red flag: 12-month minimum required from day one, especially with early termination penalties.
Q15: How do you handle my existing open AR during transition, and what is your fee structure for legacy claims?
- Good answer: Clear explanation of parallel processing, contingency fee for old AR (25–35% of recovered amount is standard), timeline for AR wind-down.
- Red flag: Vague answer, or “we charge the same percentage on everything.”
The Behavioral Health Specialization Test
Ask these three questions at the end of any vendor call. A behavioral health specialist answers without hesitation:
- What are the four criteria for the 90785 interactive complexity add-on?
- What is the difference between POS 02 and POS 10 for telehealth billing in 2026?
- How does 42 CFR Part 2 affect the way you handle claims for a client receiving both psychotherapy and substance use disorder treatment?
If they hesitate, look something up, or give a vague answer, they’re a general billing service pretending to be a behavioral health specialist. The fee savings aren’t worth what that costs you in denied claims.
Steps to Switch to Outsourced Mental Health Billing
Ready to make the move? Here’s the complete process — including the steps most practices skip that create problems later.
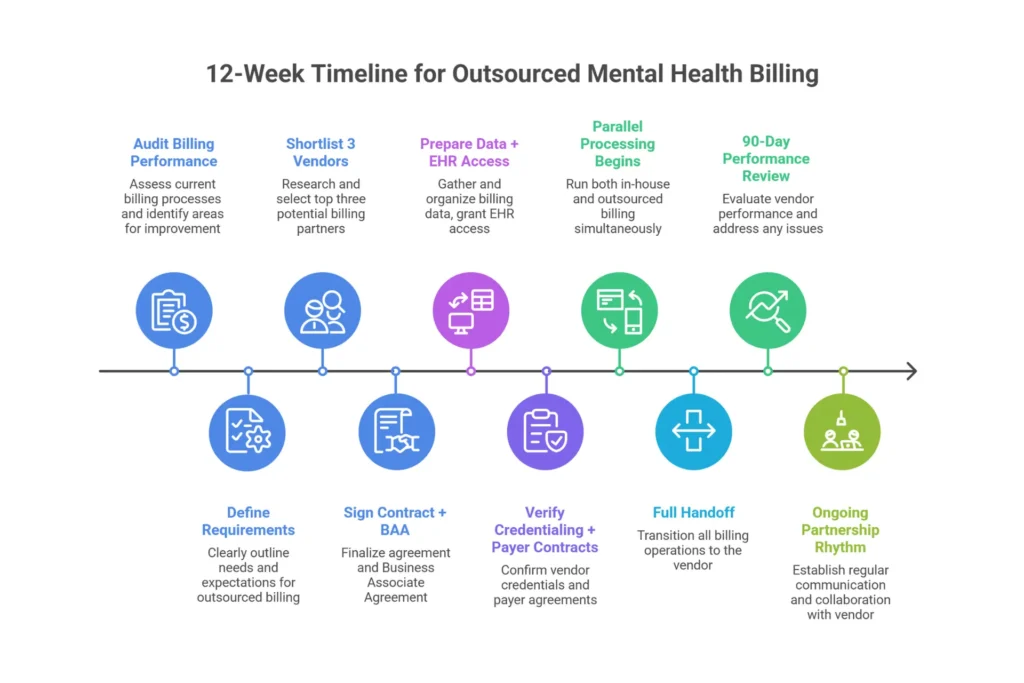
Phase 1: Decision and Selection (Steps 1–4)
Step 1: Audit Your Current Billing Performance (Time: 2–4 hours)
Pull three reports from your EHR: your AR aging summary, your denial log for the past 90 days, and your net collections rate. Calculate your true in-house billing cost using the model in the section above. This gives you the baseline you’ll compare against after transition. If you can’t pull these reports, that itself is data — you’re flying blind on your own practice’s financial health.
Step 2: Define What You Need (Time: 1 hour)
Write down: your EHR system, your full payer list, whether you bill for telehealth, whether you have any SUD (substance use disorder) clients requiring 42 CFR Part 2 handling, your practice’s growth plans for the next 12 months, and your non-negotiables on reporting and communication. This list becomes your vendor evaluation criteria.
Step 3: Research and Shortlist Three Billing Services (Time: 1 week)
Search the AAPC directory at aapc.com for behavioral health billing companies. Ask for referrals from your state mental health association. Search “mental health billing services [your state]” and check the results critically. Use the 15-question checklist from the previous section to evaluate each one — especially the specialization test questions. Don’t shortlist more than three; you’ll waste time and confuse the decision.
Step 4: Select Your Partner and Execute the Contract and BAA (Time: 1–3 days)
Review the contract specifically for: performance guarantees (ask for 95%+ clean claims in writing), whether it’s month-to-month or annual, who owns your data, and transition assistance language. Sign the Business Associate Agreement before you share a single patient name, date of service, or claim detail. No BAA = no sharing. That’s not negotiable.
Phase 2: Transition and Optimization (Steps 5–10)
Step 5: Prepare Your Data and Systems (Time: 1–2 days)
Share with your new vendor: current AR aging report, list of all active authorizations with expiration dates, credentialing status for each provider across all payers, current fee schedule, and your payer contract rates if you have them.
Step 6: Grant EHR Access and Verify Technical Setup (Time: Day 1)
Role-based EHR access should be configured before any claims are touched. Clearinghouse enrollment, ERA setup, and remittance testing should be completed before the first claim is submitted. If your vendor tries to skip this verification step, push back.
Step 7: Run Parallel Processing (Duration: 4–8 weeks)
This is the step most practices want to skip, and it’s the most important one. New claims go to the outsourced service starting day three to five. Open AR stays with your current process. Both are running simultaneously. This prevents the cash flow gap that people fear, and it lets you compare submission quality side by side before full handover.
Step 8: Complete the Full Handoff (Weeks 5–8)
Vendor takes full responsibility for all new claims. Old billing access is archived but preserved for audit purposes. Legacy AR is either wound down internally or transferred to the vendor under agreed contingency terms.
Step 9: The 90-Day Performance Review
Compare your current denial rate, days-in-AR, and net collections rate against the baseline you established in Step 1. If you’re not seeing measurable improvement on all three metrics, have that conversation with your account manager before month four.
Step 10: Establish the Ongoing Partnership Rhythm
Monthly report reviews, quarterly performance meetings, annual fee schedule and payer contract review. Never set-and-forget a billing relationship — the payer landscape changes constantly, and your vendor should be proactively flagging changes that affect your collections.
The Four Mistakes That Cause Transition Problems
- Letting the in-house biller go on day one before parallel processing is running
- Not pulling an AR aging report before transition starts (you lose visibility on what you’re owed)
- Choosing the cheapest vendor without verifying behavioral health specialization
- Not getting performance benchmarks in writing in the contract
For practices in Texas and Ohio specifically: TMHP and ODM portal enrollment can take two to three weeks for a new vendor to complete. Start this in week one of your transition planning, not after you sign the contract.
TAKE THE NEXT STEP
Ready to Eliminate Billing Headaches — and Recover Revenue You’re Currently Losing?
Elite Med Financials specializes exclusively in behavioral health revenue cycle management. Our free Practice Revenue Audit analyzes your last 90 days of claims, identifies every denial pattern and underpayment, and shows you exactly what outsourcing would mean for your practice — in real numbers, not estimates.
No obligation. No pressure. Practices we audit typically discover $30,000 to $95,000 in recoverable annual revenue they didn’t know existed.
Serving mental health practices in Florida, Texas, Connecticut, Virginia, Ohio, Massachusetts, Delaware, Michigan, and all 50 states.
Voice Search Q&A
Q: Is outsourcing medical billing a good idea?
For most mental health practices handling insurance billing, yes — outsourcing is a better financial decision than in-house billing. Specialized outsourced services consistently achieve 95% to 98% clean claim rates compared with the 80% to 90% average for in-house teams, and practices typically see 10% to 15% more revenue collected annually. The math works because outsourcing costs 5% to 9% of collections while delivering results that are simply out of reach for a single in-house biller.
Q: How much does it cost to outsource mental health billing?
Most behavioral health billing companies charge 7% to 9% of net monthly collections. In real dollars, a solo therapist collecting $150,000 per year would pay roughly $10,500 to $13,500 annually. A small group collecting $600,000 would pay around $42,000. A mid-size practice at $1 million would pay $70,000 to $90,000. Most practices see the fee offset by revenue improvement within the first 60 to 90 days.
Q: How much do mental health billers charge as employees?
An in-house mental health biller earns $45,000 to $75,000 in base salary, but the true fully-loaded cost — including benefits, payroll taxes, software, overhead, and annualized turnover risk — typically runs $58,000 to $97,500 per year. That doesn’t include the revenue lost to denied and abandoned claims, which can add another $20,000 to $45,000 annually on a mid-size practice.
Q: What are the top five denials in mental health billing?
The five most common claim denials in mental health billing are: authorization missing or expired, patient eligibility not in effect on date of service, coding errors or incorrect CPT code for session length, timely filing limit exceeded, and medical necessity documentation insufficient. Behavioral health claims are denied at rates 85% higher than general medical claims, but specialized billing companies resolve 85% or more of denials on first appeal.
Q: How many claims should a biller work per day?
A full-time in-house biller typically processes 30 to 40 claims per day when balancing all their other responsibilities. A dedicated outsourced specialist working in a team environment processes 80 to 120 claims per day — the throughput difference is one of the main reasons outsourced billing produces faster reimbursements and lower days-in-AR.
Q: Will medical billers be replaced by AI?
AI is changing billing workflows — eligibility verification, claim scrubbing, and payment posting are increasingly automated. But behavioral health billing still requires human expertise for MHPAEA parity appeals, 42 CFR Part 2 compliance, crisis code documentation review, and complex denial appeals. The best billing services in 2026 use AI tools to handle the repetitive work while experienced specialists handle the judgment calls that determine whether your claims get paid.
Q: What is the golden rule of medical billing?
Bill accurately, bill completely, and bill on time. In mental health billing specifically, accuracy means correct CPT codes matched to documented session length, appropriate modifier usage (90785, modifier 95 for telehealth), and correct ICD-10 codes with sufficient specificity. Completeness means including all MHPAEA parity documentation. On time means submitting within 24 to 48 hours — long before any payer’s timely filing window closes.
Q: How do I find a mental health billing company?
Start by defining your EHR, payer mix, and any specialty needs (telehealth, SUD billing). Search the AAPC member directory and ask for referrals from your state mental health association. Shortlist three vendors and evaluate each using the 15-question checklist in this article, with particular attention to the behavioral health specialization test. Verify SOC 2 or HITRUST certification before sharing any patient data.
Q: Should I outsource my mental health billing?
If your practice handles insurance billing, has more than one or two payers, and your denial rate is above 10%, outsourcing will almost certainly improve both your revenue and your quality of life. The practices that generally shouldn’t outsource are cash-pay only practices under $100,000 annually, or those that already have a certified behavioral health billing specialist achieving 95%+ clean claims. For everyone else, the financial case is compelling.
Q: How long does it take to transition to outsourced mental health billing?
A well-run transition takes 8 to 12 weeks. The critical phases are: system access and setup in weeks one and two, EDI and ERA enrollment in weeks three through five (the slowest phase — payers move at their own pace), parallel processing in weeks five through eight, and full handover in weeks eight through ten. Cash flow stays at 95%+ of normal throughout when the transition is managed with a parallel processing phase.
FAQ
What are the main benefits of outsourcing mental health billing?
The three categories of benefit are financial, clinical, and operational. Financially: clean claim rates rise from 80% to 90% in-house to 92% to 98% outsourced, denial rates drop from 10% to 20% down to 2% to 8%, and days-in-AR compress from 45 to 60 days to 25 to 35 days. That combination typically generates 10% to 15% more revenue for the same work. Clinically: providers reclaim 5 to 10 hours per week previously spent on billing issues. Operationally: you eliminate HR risk, turnover disruption, and the burden of staying current on constantly changing payer rules.
Is outsourcing mental health billing worth it financially?
For practices generating more than $200,000 in annual insurance revenue, the ROI is almost always positive within 90 days. A three-provider group at $600,000 in collections typically sees $102,000 or more in combined cost savings and revenue improvement in year one — against an outsourcing fee of $42,000. The three-year cumulative benefit exceeds $300,000 in most modeled scenarios. The rare exceptions are very small practices or those already achieving elite performance metrics in-house.
How much does outsourcing mental health billing cost?
Expect to pay 7% to 9% of net monthly collections for a quality behavioral health billing specialist. Some companies offer flat-fee models or per-claim pricing — flat fees work better for high-volume, lower-dollar practices; percentage models work better for most behavioral health practices where claim values vary significantly. The fee should cover all billing functions: coding review, claim submission, denial management, AR follow-up, and reporting. Services charging below 5% are typically submit-only models that don’t include denial management — which is where most of the value actually is.
What is the difference between in-house and outsourced mental health billing?
In-house billing gives you direct oversight and familiarity, but carries fixed overhead costs of $58,000 to $97,500 per year regardless of performance, 15% to 33% annual turnover risk, and typical performance metrics of 80% to 90% clean claims and 45 to 60 days-in-AR. Outsourced billing converts that to a variable cost tied to your actual collections, delivers 92% to 98% clean claims and 25 to 35 days-in-AR, and comes with team redundancy, specialized expertise, and performance accountability through service level agreements.
Is outsourcing medical billing a good idea for therapy practices?
Yes, with the caveat that the benefit scales with practice size and insurance complexity. Solo therapists with five or more insurance panels typically see strong ROI even at $150,000 in annual revenue. Small groups from two to five providers almost always benefit. The primary exception is cash-pay only or very small solo practices where the fee doesn’t justify the overhead of a vendor relationship.
How long does it take to transition to outsourced billing?
Eight to twelve weeks for a standard transition. Practices with complex legacy AR, multiple state Medicaid enrollments, or incomplete credentialing may take ten to sixteen weeks. The cash flow disruption that people fear rarely materializes when the transition includes a proper parallel processing phase. Most practices see collections improvement by month two and are fully stabilized by month three.
What should I look for in an outsourced mental health billing company?
Five non-negotiable criteria: behavioral health represents at least 75% of their billing portfolio; verified clean claim rate of 95% or higher; direct EHR integration (not manual exports); HIPAA Business Associate Agreement signed before data sharing; and month-to-month contracts available after the initial ramp period. Beyond the basics, look for dedicated account management (not a shared queue), real-time dashboard access, and the ability to answer the behavioral health specialization test questions confidently.
Are outsourced mental health billing companies HIPAA compliant?
Reputable companies are — and they should be able to prove it. Look for SOC 2 Type II or HITRUST certification, multi-factor authentication for all system access, encrypted data at rest and in transit, and a Business Associate Agreement as standard practice. For practices with substance use disorder clients, also verify 42 CFR Part 2 compliance specifically. If a vendor can’t describe their security certification program in detail, that’s a deal breaker.
Can outsourcing mental health billing reduce my denial rate?
Substantially. In-house mental health billing averages denial rates of 10% to 20%. Specialized outsourced teams bring this down to 2% to 8% by combining payer-specific coding rules, systematic pre-authorization management, and dedicated denial appeal workflows. More importantly, they recover 80% to 90% of denials through appeal — compared with the 35% to 50% recovery rate typical of in-house teams and the 50% to 65% that in-house teams simply abandon.
Will I lose control of my billing if I outsource?
You gain more visible control than you currently have. Most practice owners with in-house billing know only what their biller reports to them verbally. Outsourced billing comes with a real-time dashboard showing AR aging, denial trends, and payer-level collections data available 24/7. Instead of walking down the hall to ask “how are we doing?”, you open a portal and see every metric updated daily. The trade is hands-on management for data-driven oversight — most practice owners find the trade very much in their favor.
Should I outsource mental health billing to a company in India?
Use caution. The 4% to 6% fee looks attractive compared to 7% to 9% for US-based services. But mental health billing requires compliance with US-specific regulations (MHPAEA, 42 CFR Part 2, state Medicaid programs) that change frequently, payer follow-up during US business hours that a 12-hour time zone gap makes impractical, and HIPAA compliance that is jurisdictionally difficult to enforce offshore. US-based behavioral health specialists consistently outperform offshore options on clean claim rates and denial recovery — the fee savings typically cost more than they save.
How do outsourced billing services handle denied claims?
A quality service handles denials in four steps: immediate flagging within 24 hours of ERA posting; categorization as administrative or clinical error; rapid appeal filed within 48 hours with supporting documentation; and a feedback loop to the practice to prevent the same denial pattern recurring. Elite vendors achieve 85% or higher first-pass success on appeals and maintain denial trend logs that identify systemic issues — like a specific payer’s unusual interpretation of a documentation requirement — and address them at the source rather than claim by claim.
Conclusion: The Math Is Clear. The Transition Is Manageable. The Opportunity Is Now.
Three things worth carrying away from this guide:
First, the true cost of in-house billing is almost certainly higher than your current estimate. Once you add benefits, payroll taxes, turnover risk, software, and the revenue lost to abandoned denials, most three-provider practices are spending $85,000 to $140,000 per year on a function that outsourced specialists handle better for $30,000 to $50,000.
Second, the performance gap between in-house and outsourced mental health billing is real and measurable. Clean claim rates, denial rates, days-in-AR — outsourced behavioral health specialists consistently outperform in-house teams on every metric that translates directly into revenue collected. The 10% to 15% net collections improvement isn’t marketing language; it’s the mathematical result of specialized expertise applied at scale.
Third, the transition is far less disruptive than it looks. A parallel processing approach keeps your cash flow at 95%+ of normal throughout the changeover. Most practices reach full stabilization and measurable improvement within 90 days.
TAKE THE NEXT STEP
Ready to Eliminate Billing Headaches — and Recover Revenue You’re Currently Losing?
Elite Med Financials specializes exclusively in behavioral health revenue cycle management. Our free Practice Revenue Audit analyzes your last 90 days of claims, identifies every denial pattern and underpayment, and shows you exactly what outsourcing would mean for your practice — in real numbers, not estimates.
No obligation. No pressure. Practices we audit typically discover $30,000 to $95,000 in recoverable annual revenue they didn’t know existed.
Serving mental health practices in Florida, Texas, Connecticut, Virginia, Ohio, Massachusetts, Delaware, Michigan, and all 50 states.
Elite Med Financials specializes exclusively in behavioral health revenue cycle management. We serve mental health practices across the United States — including Florida, Texas, Connecticut, Virginia, Ohio, Massachusetts, Delaware, Michigan, and all 50 states.
External References: MGMA 2024 DataDive Provider Compensation, AAPC Medical Billing Certification Resources, Bureau of Labor Statistics Occupational Outlook Handbook (Medical Records Specialists), KFF 2024 Employer Health Benefits Survey

