Published by Elite Med Financials | Updated March 2026 | Estimated Read: 18 minutes

Let’s start with an uncomfortable number: the average behavioral health practice loses between $18,000 and $45,000 every year to billing code errors. Not fraud. Not malpractice. Just wrong codes, missing modifiers, and documentation that doesn’t hold up when a payer’s audit algorithm flags it.
I’ve spent years working inside mental health revenue cycles, and the pattern is almost always the same — a brilliant clinician who understands trauma, anxiety, and personality disorders better than anyone, but who had to learn billing from a 2019 YouTube video. In 2026, with AI-driven claim scrubbing, permanent telehealth rules, and LPC/LMFT Medicare expansion now fully active, that 2019 knowledge is genuinely costing you money.
This guide covers everything: the three code systems that tell your patient’s story to payers, the 2026 Medicare rates for every therapy CPT code, the state-by-state Medicaid rules nobody puts in one place, and the specific errors that trigger Recovery Audit Contractor (RAC) reviews. We’ve written it for therapists, practice managers, and billing staff who want to actually understand what they’re submitting — not just copy and paste codes.
Featured Snippet Answer — What Are Mental Health Billing Codes? Mental health billing codes are standardized alphanumeric identifiers used to document and bill behavioral health services to insurance payers. CPT codes (e.g., 90837) describe the service provided, ICD-10-CM codes (e.g., F41.1) establish medical necessity through diagnosis, and HCPCS Level II codes (e.g., H0004) cover supplemental services, particularly in Medicaid. All three systems must work together on a compliant claim.
Table of Contents
What Are Mental Health Billing Codes? CPT vs ICD-10 vs HCPCS Explained
Every claim you submit tells a story in code. The problem is, most providers are writing that story in at least two languages simultaneously — and when one doesn’t match the other, payers reject the entire claim.
There are three distinct coding systems in behavioral health billing:
CPT Codes (Current Procedural Terminology) — The American Medical Association publishes these annually. In mental health, CPT codes describe the service delivered: individual therapy for 45 minutes (90834), a psychiatric diagnostic evaluation (90791), or crisis psychotherapy (90839). These are the “what did you do?” codes.
ICD-10-CM Codes (International Classification of Diseases) — Maintained by the World Health Organization and implemented by CMS, these are your diagnosis codes. F41.1 for generalized anxiety disorder, F32.1 for moderate major depressive disorder. These answer the fundamental payer question: why does this patient need treatment? Without a valid ICD-10 code supporting medical necessity, no CPT code gets paid.
HCPCS Level II Codes — CMS manages these, and they cover services that CPT doesn’t capture well. In mental health, they’re mostly relevant for Medicaid — H0004 for behavioral health counseling in 15-minute units, H2011 for crisis stabilization, T1019 for personal care services. Think of HCPCS as the “extras” catalog.
| Feature | CPT | ICD-10-CM | HCPCS Level II |
|---|---|---|---|
| Maintained By | American Medical Association | WHO/CMS | CMS |
| Codes | What you did (procedure) | Why it was needed (diagnosis) | Supplemental services |
| Example | 90837 — Psychotherapy, 60 min | F41.1 — GAD | H0004 — BH counseling, 15 min |
| Used On | CMS-1500 Box 24D | CMS-1500 Box 21 | UB-04 or CMS-1500 |
| Who Needs It | All providers | All providers | Medicaid providers primarily |
How they link on a claim: On a CMS-1500 form, Box 21 holds your ICD-10 codes (A, B, C…), Box 24B holds the Place of Service code, Box 24D holds the CPT code plus any modifiers, and Box 24E contains the “diagnosis pointer” — the letter that connects the specific diagnosis to the specific procedure. If Box 21 has F41.1 as “A” and Box 24E for 90837 shows “A,” you’ve told the payer: generalized anxiety disorder justifies this 60-minute therapy session. That linkage is what creates medical necessity.
The billing golden rule every provider must internalize: your ICD-10 code must clinically justify your CPT code’s intensity. Billing 90837 (60-minute therapy) for a patient diagnosed only with F32.0 (mild depression) may get paid once, but it will eventually trigger a utilization review. The diagnosis needs to match the care level.
If your team is still learning the difference between these systems or if you’re seeing unexplained denials, our medical coding services are built specifically for behavioral health practices navigating exactly this complexity.
Complete List of Mental Health CPT Billing Codes 2026
Here’s the thing about mental health CPT codes that trips up providers constantly: almost all of them are time-based. Unlike a surgeon billing for an appendectomy (fixed procedure = fixed code), therapists bill for minutes of face-to-face clinical work. That means time documentation isn’t a nice-to-have — it’s the literal foundation of your claim.
The 2026 Medicare Physician Fee Schedule (PFS) maintains the same core psychotherapy structure with updated reimbursement rates. Here’s the full picture:
Individual Psychotherapy (The Core Codes)
| CPT Code | Description | Face-to-Face Time | 90785 Add-On OK? | Telehealth OK? | 2026 Medicare Non-Facility Rate | Most Denied For |
|---|---|---|---|---|---|---|
| 90832 | Psychotherapy, 30 min | 16–37 min | Yes | Yes | ~$86 | Session under 16 min |
| 90834 | Psychotherapy, 45 min | 38–52 min | Yes | Yes | ~$114 | Billing 90837 for 52 min sessions |
| 90837 | Psychotherapy, 60 min | 53+ min | Yes | Yes | ~$167 | Missing start/stop times |
| 90791 | Psychiatric diagnostic eval (no medical) | N/A | Yes | Yes | ~$173 | Billing more than once per 6 months |
| 90792 | Psychiatric eval with medical services | N/A | Yes | Yes | ~$202 | Used by non-prescribers |
The 53-Minute Rule — Memorize This
Billing 90837 requires documented face-to-face time of 53 minutes or more. Not 52. Not “about an hour.” The midpoint between 90834 (which maxes at 52 minutes) and 90837 falls at 52.5 minutes — which rounds up to 53. A 52-minute session documented as 90837 is upcoding under CMS guidelines. Do it once and you’ll probably get paid. Do it consistently and a RAC audit will eventually recover those payments — with interest, over a six-year lookback period.
What counts as face-to-face time? Only direct therapeutic interaction. Not writing your notes afterward. Not reviewing records before the client walks in. Not coordinating with another provider. Just the actual therapy time.
Add-On Codes (Can’t Bill Alone)
| CPT Code | Description | Time | Goes With | 2026 Medicare Rate | Common Error |
|---|---|---|---|---|---|
| 90785 | Interactive complexity | N/A | 90832/34/37, 90791/92 | ~$45 | Not documenting which of 4 criteria was met |
| 90833 | Psychotherapy add-on, 30 min | 16–37 min | E/M codes | ~$70 | Billed as standalone code |
| 90836 | Psychotherapy add-on, 45 min | 38–52 min | E/M codes | ~$86 | Mismatched time to E/M duration |
| 90838 | Psychotherapy add-on, 60 min | 53+ min | E/M codes | ~$125 | Confused with 90836 |
The 90785 interactive complexity add-on is legitimate and often underused — but only when one of four specific criteria is present: (1) maladaptive communication between patient and caregiver that disrupts the session; (2) caregiver actively interfering with or blocking treatment; (3) a sentinel event during or just before the session that requires mandated reporting; or (4) communication barriers requiring additional equipment or interpreter services. “This patient was really difficult today” does not meet criteria. Document the specific criterion.
Crisis, Family, and Group Codes
| CPT Code | Description | Time | Notes |
|---|---|---|---|
| 90839 | Crisis psychotherapy, first 60 min | 30–74 min | Requires documented crisis event, not routine high-acuity |
| 90840 | Crisis psychotherapy, each add’l 30 min | Per 30 min over 74 min | Rarely needed; requires extraordinary circumstances |
| 90846 | Family therapy without patient | ~50 min | Document how session benefits the identified patient |
| 90847 | Family therapy with patient present | ~50 min | Cannot bill if identified patient not present |
| 90853 | Group psychotherapy | N/A | Requires per-patient individualized documentation |
Psychiatric E/M and BHI Codes (Prescribers and Integration Specialists)
| CPT Code | Description | Who Bills | Notes |
|---|---|---|---|
| 99213 | Office visit, low complexity established pt | MD, DO, NP, PA | Medication check, simple |
| 99214 | Office visit, moderate complexity | MD, DO, NP, PA | Standard med management |
| 99215 | Office visit, high complexity | MD, DO, NP, PA | Complex psychiatric presentation |
| 99484 | General BHI, 20+ min/month | Care managers | Monthly aggregate billing |
| G0568–G0570 | Collaborative Care Model (CoCM) | Psychiatric consultants | Replaced 99492–99494 in 2026 |
The CoCM transition from 99492–99494 to G0568–G0570 in 2026 catches many practices off guard. If your Collaborative Care program is still billing the old codes, those claims will deny. Update your charge capture templates immediately.
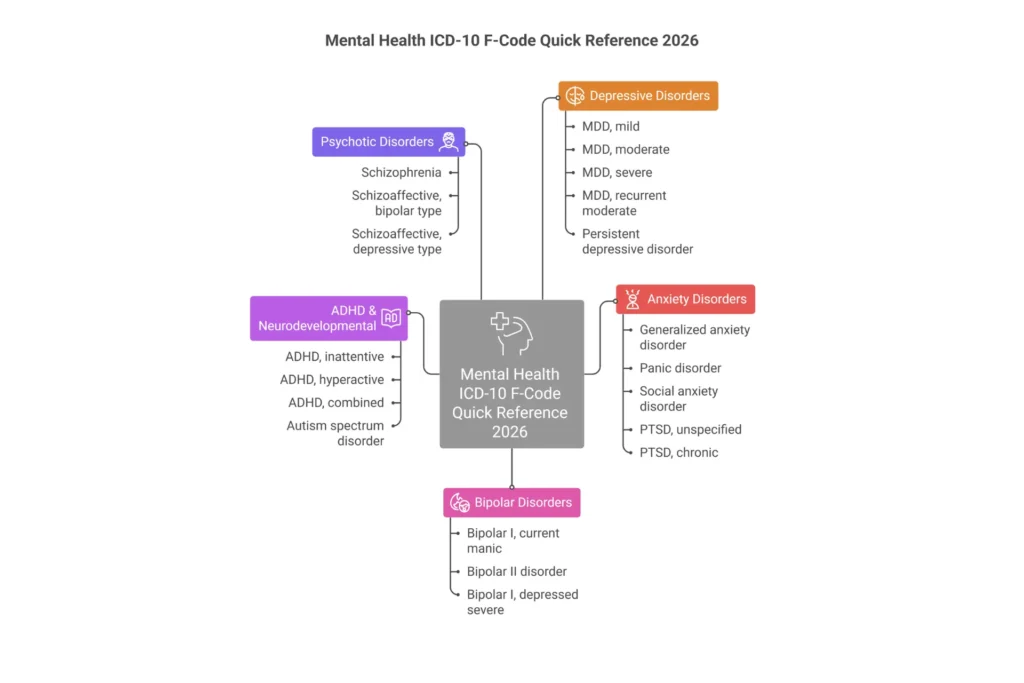
ICD-10 Diagnosis Codes for Mental Health — Complete F-Code Reference
Every ICD-10 mental health code lives in the F01–F99 range. DSM-5 gives us our diagnostic criteria; ICD-10-CM translates those clinical judgments into the alphanumeric codes that insurance companies actually process. The two systems don’t map perfectly, which is where most documentation problems originate.
The Specificity Problem That’s Costing You Money
Payers in 2026 are flagging providers who rely on unspecified codes past the first 1–2 visits. F32.9 (major depressive disorder, unspecified) is fine for an initial intake. By the third session, you need to specify severity. By visit six, if you’re still using F32.9 for a patient you’ve been treating for moderate-to-severe depression, some payer systems will automatically trigger a records request.
The PHQ-9 is your best friend for ICD-10 justification. Score 5–9 supports F32.0 (mild). Score 10–14 supports F32.1 (moderate). Score 15–19 supports F32.2 (severe without psychotic features). Score 20+ supports F32.2 with attention to psychotic features. Document the score in every session note and the specificity takes care of itself.
Top 30 Mental Health ICD-10 Codes for 2026
| ICD-10 Code | DSM-5 Diagnosis | Severity/Specifier | Common CPT Pair | Key Documentation Requirement |
|---|---|---|---|---|
| F32.0 | MDD, single episode, mild | PHQ-9 5–9 | 90832, 90834 | Specifier required by visit 3 |
| F32.1 | MDD, single episode, moderate | PHQ-9 10–14 | 90834, 90837 | Functional impairment documentation |
| F32.2 | MDD, single episode, severe w/o psychosis | PHQ-9 15+ | 90837 | Safety planning note recommended |
| F32.3 | MDD, single episode, severe with psychosis | PHQ-9 20+ | 90837, 90792 | Document psychotic features explicitly |
| F32.9 | MDD, unspecified | N/A | 90832, 90834 | Acceptable for intake only |
| F33.0 | MDD, recurrent, mild | Prior episode documented | 90834 | Note prior episode in assessment |
| F33.1 | MDD, recurrent, moderate | 2+ episodes | 90834, 90837 | Justify recurrent with episode history |
| F33.2 | MDD, recurrent, severe w/o psychosis | 2+ episodes | 90837 | Significant functional impairment |
| F33.9 | MDD, recurrent, unspecified | N/A | 90834 | Specify by visit 2 |
| F41.0 | Panic disorder | With/without agoraphobia | 90834, 90837 | Panic attack frequency in notes |
| F41.1 | Generalized anxiety disorder | 6+ months required | 90834, 90837 | Document chronicity of worry |
| F41.9 | Anxiety disorder, unspecified | N/A | 90832, 90834 | Refine within 2 visits |
| F43.10 | PTSD, unspecified | N/A | 90837 | Duration determines acute vs chronic |
| F43.11 | PTSD, acute | <3 months post-trauma | 90837 | Note exposure and onset date |
| F43.12 | PTSD, chronic | >3 months post-trauma | 90837 | Confirm timeline |
| F43.21 | Adjustment disorder with depressed mood | Identifiable stressor | 90834 | Document specific stressor |
| F43.23 | Adjustment disorder with mixed anxiety/depression | Identifiable stressor | 90834 | Both anxiety and depressive symptoms present |
| F90.0 | ADHD, inattentive type | Inattention only | 90834, 90837 | No significant hyperactivity |
| F90.1 | ADHD, hyperactive-impulsive | No inattention | 90834 | Rare in clinical presentation |
| F90.2 | ADHD, combined type | Both presentations | 90834, 90837 | Most common ADHD code |
| F31.32 | Bipolar I, current episode depressed, moderate | Moderate severity | 90834, 90837 | Document prior manic episode |
| F31.9 | Bipolar disorder, unspecified | N/A | 90837 | Specify episode type ASAP |
| F60.3 | Borderline personality disorder | N/A | 90837 | Requires longitudinal documentation |
| F10.10 | Alcohol use disorder, mild (abuse) | DSM-5 mild AUD | 90834 | 2–3 criteria in 12 months |
| F10.20 | Alcohol use disorder, moderate-severe (dependence) | DSM-5 mod/severe | 90834, H0004 | 4+ criteria in 12 months |
| F50.01 | Anorexia nervosa, restricting type | N/A | 90837, 90847 | BMI tracking recommended |
| F84.0 | Autism spectrum disorder | Severity level 1–3 | 90837, 90834 | Level of support required |
| F34.1 | Persistent depressive disorder (dysthymia) | 2+ years | 90834 | Duration must be documented |
| F20.9 | Schizophrenia, unspecified | N/A | 90837, 90792 | Coordinate with prescriber |
| F42 | OCD | With/without insight | 90837 | Y-BOCS score supports intensity |
Z-Codes: Supporting Context, Not a Primary Diagnosis
Z-codes describe social determinants of health and life circumstances. They add essential context but cannot stand alone as the reason for treatment:
- Z63.0 — Relationship problems with spouse/partner
- Z63.8 — Other problems with primary support group
- Z91.5 — Personal history of self-harm
- Z59.5 — Extreme poverty
- Z13.31 — Screening for depression (only when no treatment is being provided)
Using Z63.0 as a primary diagnosis for ongoing 90837 sessions will result in PR-49 denials (“service not medically necessary”) from most payers. Always lead with an F-code. Add the Z-code as a secondary code to provide clinical context.
CMS Article A57480 is the Medicare Local Coverage Determination that explicitly governs what diagnoses support medical necessity for psychotherapy. F32.x, F33.x, F41.x, F43.x, F31.x, F60.x — these are your workhorses. F99 (unspecified mental disorder) is effectively unbillable. Don’t use it.
Worried about your ICD-10 coding accuracy? Our insurance eligibility and medical coding team audits diagnosis linkage before claims go out the door.
Modifier Codes for Mental Health Billing — 2026 Complete Guide

Modifiers are two-character codes appended to CPT codes that clarify the circumstances of a service. They tell payers: this was telehealth, this provider is a master’s-level clinician, these were two genuinely separate services on the same day. In behavioral health, modifiers are often the difference between getting paid and getting denied.
The Modifiers Every Mental Health Biller Must Know
Telehealth Modifiers
- -95: Synchronous audio-video telehealth. The standard modifier for video therapy sessions. Required by Medicare (with POS 02 or 10), required by BCBS, Aetna, Cigna, UHC. Append it to any CPT code delivered via video: 90837-95, 90791-95, 90839-95.
- -93: Synchronous audio-only telehealth. Permanent for Medicare mental health as of 2024. Use when the patient cannot or chooses not to use video. Document the reason: “Patient declined video due to privacy concerns in shared living space.” Without that documentation, audio-only claims are vulnerable to denial.
- -FQ: Audio-only for FQHC/RHC settings only. Rural health clinics use this instead of -93. Non-FQHC providers should not use -FQ.
- -GT: Legacy telehealth modifier. Some older Medicare Advantage plans still accept it, but for traditional Medicare, use -95. If you’re still routinely appending -GT to Medicare claims and getting paid, it’s working by exception — don’t count on it continuing.
E/M and Procedural Modifiers
- -25: This goes on E/M codes only (like 99214) when a psychiatrist performs both medication management and a separate, distinct therapy session on the same day. The documentation must show two separate services — not a medication check that happened to include some supportive listening, but a genuinely distinct therapeutic intervention. Without -25, the E/M and the therapy add-on (90833, 90836, or 90838) will bundle and you’ll only get paid for one.
- -59: Distinct procedural service. Used on procedure codes (not E/M) when you provide two genuinely separate services on the same day — like an individual therapy session in the morning and a group session in the afternoon. This is not a magic unbundling modifier; there must be a real clinical reason the services were provided separately.
Provider Level Modifiers (Medicaid Critical)
- HO: Master’s level clinician (LCSW, LPC, LMFT). Required by California Medi-Cal, Texas Medicaid, Florida Medicaid, New York Medicaid, and Illinois Medicaid on every claim. Missing HO in these states = automatic denial.
- HN: Bachelor’s level clinician. Used for case managers, peer support specialists, paraprofessionals billing H-codes.
- HP: Doctoral level psychologist (PhD/PsyD). Required by some state Medicaid programs.
- AJ: Clinical social worker. Required by Medicare for LCSWs billing certain codes.
- HQ: Group setting. Required by TX and FL Medicaid when billing 90853 or group H-codes.
- HF: Substance abuse program. Required for SUD-specific services in TX, GA, FL Medicaid.
Modifier Sequencing Rule Nobody Tells You
Modifiers must appear in a specific order on Box 24D of the CMS-1500: pricing modifiers first, informational modifiers second.
Pricing modifiers that affect payment (-25, -59) go before informational modifiers (HO, -95). So for a master’s-level LCSW delivering telehealth in California Medicaid: 90837-HO-95, not 90837-95-HO.
Get the sequence wrong and you may get paid, but you’ve created a compliance vulnerability that post-payment auditors look for.
Modifier Combinations: What Works and What Doesn’t
| Combination | Valid? | Correct Order | Use Case |
|---|---|---|---|
| HO + 95 | YES | HO first | Master’s level telehealth |
| 25 + AJ | YES | 25 first | LCSW E/M + therapy same day |
| 59 + HQ | YES | 59 first | Group as distinct second service |
| 95 + GT | NO | N/A | Can’t use both telehealth modifiers |
| HO + HP | NO | N/A | Provider can’t be both master’s and doctoral |
| 93 + 95 | NO | N/A | Audio-only and video on same line |
| 25 + 59 | CAUTION | 25 first | Rare; needs extensive documentation |
Our denial management team sees modifier errors as the #1 cause of preventable denials in behavioral health practices. If you’re not sure whether your modifier setup is correct, that’s worth fixing before the next claim submission.
Mental Health Billing Codes by Payer — Medicare, Medicaid, and Commercial
The same CPT code — say, 90837 — pays differently, requires different modifiers, and has different prior authorization rules depending on who’s actually paying the claim. Treating all three payers the same is one of the most expensive mistakes a behavioral health practice can make.

The Three-Payer Comparison Table
| Criteria | Medicare | Medicaid (FFS Average) | Commercial (BCBS/Aetna/UHC/Cigna) |
|---|---|---|---|
| CPT Coverage | All psychotherapy, evals, crisis, testing, BHI, G-codes | All CPT + H/T-codes (H0004, H2011, T1019) | Core CPT coverage; some require auth |
| Prior Authorization | None for routine outpatient therapy | Varies by state; often triggers >12–20 visits | Frequent for 90837, testing, IOP/PHP |
| Session Limits | None (parity) | 20–52 visits/year state-specific | 20–50 visits, parity-based |
| Telehealth Modifiers | -95 or -93 permanent, POS 10/02 | State-specific (+HO required in many states) | -95 required; POS varies by payer |
| Provider Types | MD/DO, PhD, LCSW, LPC, LMFT (from 2024) | LCSW/LPC/PhD; state licensure governs | Same as Medicare; paneled required |
| ICD-10 Specificity | F-codes required; unspecified flagged after initial | F-codes + Z-codes; unspecified ok initial | Highest specificity; Cigna flags F41.9 after 2 claims |
| Timely Filing | 12 months from DOS | 90–365 days (state-dependent) | 90–180 days; UHC = 90 days strict |
| Reimbursement (90837) | ~$167 baseline non-facility | 70–90% of Medicare | 110–150% of Medicare |
The Medicare Provider Expansion: What It Means for LPCs and LMFTs
Starting January 1, 2024, Licensed Professional Counselors (LPCs) and Licensed Marriage and Family Therapists (LMFTs) became recognized Medicare Part B providers. By 2026, this expansion is fully implemented.
Enrollment requires completing a CMS-855I form (or PECOS online application) and completing a Medicare credentialing process that typically takes 60–120 days. Once enrolled, LPCs and LMFTs bill at 75% of the Medicare Physician Fee Schedule — the same rate as Clinical Social Workers.
The key limitation: “incident-to” billing still requires physician supervision in specific configurations, and LPCs/LMFTs cannot bill codes that require medical services (90792, E/M codes like 99214).
T1019 vs T1020: The Medicaid Confusion Everyone Asks About
T1019 and T1020 are HCPCS codes that appear in Medicaid behavioral health billing but are not psychotherapy codes. They serve a different purpose entirely:
T1019 is billed per 15-minute unit for personal care services — things like ADL assistance (grooming, meal prep) and brief respite support that help a patient with serious mental illness maintain stability in the community. It’s not therapy. Don’t substitute it for 90834.
T1020 is a per-diem code for a full day of structured personal care or 24-hour respite. Used in Medicaid waiver programs for individuals with SMI who need round-the-clock community support.
Both are Medicaid waiver codes, primarily used by community-based service providers. If you’re a clinical therapist billing 90834 and 90837 for sessions, you’ll encounter T1019 and T1020 when a patient’s comprehensive Medicaid waiver plan includes personal care alongside their therapy.
MHPAEA Parity: Your Commercial Denial Appeal Weapon
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires commercial health plans to cover mental health services at the same level as medical/surgical services. In practical terms:
- A plan that covers unlimited ER visits cannot impose a 20-visit annual limit on therapy
- Copays for therapy cannot exceed copays for specialist medical visits
- Prior authorization requirements for mental health cannot be more restrictive than for comparable medical services
When a commercial payer denies a claim for exceeding visit limits or applies more restrictive auth requirements than they apply to medical care, you have a parity violation. Cite 29 CFR Part 2590, Subpart C in your appeal. This works.
Need help navigating commercial payer denials? Our AR follow-up services specialize in the appeals process for behavioral health, including parity-based appeals.
Medicaid Mental Health Billing Codes — State-by-State Guide
Medicaid is not one payer. It’s 50 different programs, each with different codes, different modifiers, different session limits, and different prior authorization triggers. What gets paid in California gets denied in Florida.
The 3-Month Retroactive Eligibility Rule
Before diving into state specifics: Medicaid provides retroactive coverage for up to 3 months prior to an application date when the patient would have been eligible during that period. If a patient applies in March and is approved, you can submit claims for services back to December — but only after eligibility is confirmed, and only within the state’s timely filing window.
Some states have waived retroactive eligibility, reducing it to 1 month or eliminating it entirely. Always verify a patient’s retroactive eligibility date before submitting backdated claims.
State-by-State Medicaid Mental Health Reference (Top 10 States)
| State | Program | Core CPTs | Key HCPCS | Telehealth Modifier | Session Cap (Adults) | PA Threshold | Notable Rules |
|---|---|---|---|---|---|---|---|
| California | Medi-Cal | 90832–90837, 90791 | H0001–H2021, T1019/T1020 | HO+95 | None (>20 auth) | >20 visits | MHSA-funded peer support H0038 |
| Texas | TMHP/CHIP | 90832–90837, 90791 | H0004–H0036, H2011 | HO/HN+95 | 52/year | >16 visits | HF for SUD; HQ for group |
| New York | Medicaid | 90832–90837, 90791 | H0015–H2021, T1023 | HO+95 | Clinic-determined | Clinic-specific | OMH/OPWDD carve-outs; separate rules |
| Florida | Florida Medicaid | 90832–90837, 90791/92 | H0001–H0031, H0004 | HO/HN+95 | 52/year FFS | >8 visits (very strict) | MCO auth stricter than FFS |
| Illinois | Illinois Medicaid | 90832–90837, 90791 | H2011–H2021, T1019 | HO+95 | None with auth | >12 visits | Peer support H0038 available |
| Pennsylvania | PA HealthShare | 90832–90834, 90837 | H0004–H2019 | 95/-93 | 20/year initial | All evals require auth | CHC H2021 community-based |
| Ohio | Ohio Medicaid | 90832–90837, 90791 | H0015–H0036 | HO+95 | 104/year (generous) | >26 visits | T1020 for SUD respite |
| Michigan | MI Health Link | 90832–90837, 90847, 90853 | H0001–H2025 | 95/FQ | None | MCO-determined | IMD waiver H0040 supported housing |
| Georgia | Georgia Medicaid | 90832–90837, 90791 | H0005–H0034, HF | HO+95 | 24/year adults | >12 visits | HF modifier heavy for SUD programs |
| New Jersey | NJ FamilyCare | 90832–90837, 90791/92 | H2011–H2021 | 95/-93 | None | >20 visits | H0031 for MH assessment by non-MD |
H-Codes: The Medicaid-Specific Behavioral Health Codes
| H-Code | Description | Billing Unit | Primary Use States |
|---|---|---|---|
| H0004 | Behavioral health counseling and therapy | Per 15 minutes | All |
| H0031 | Mental health assessment by non-physician | Per session | CA, TX, NJ |
| H0036 | Community psychiatric supportive treatment | Per 15 minutes | TX, OH, GA |
| H0038 | Self-help/peer services | Per 15 minutes | CA, IL |
| H2011 | Crisis intervention mental health | Per 15 minutes | All |
| H2019 | Therapeutic behavioral services | Per 15 minutes | CA, TX |
| H2021 | Community-based wrap-around services | Per day | PA, OH |
EPSDT: The Override for Medicaid Patients Under 21
If you serve children or adolescents on Medicaid and you’re running into session limit denials, this is the rule you need to know: EPSDT (Early and Periodic Screening, Diagnostic, and Treatment) requires every state Medicaid program to cover all medically necessary services for patients under 21, regardless of state-imposed session limits.
If a 16-year-old with severe MDD needs 40 sessions per year and your state has a 24-visit annual cap, EPSDT overrides that cap. Appeal language to cite: “Under 42 U.S.C. § 1396d(r), EPSDT mandates coverage of all medically necessary services for this patient. Session limits do not apply.”
Our mental health billing services team has successfully appealed dozens of Medicaid session limit denials using EPSDT. If you’re seeing these denials for your pediatric patients, it’s worth a call.
Telehealth Mental Health Billing Codes and Modifiers 2026
The Consolidated Appropriations Act, 2026 extended Medicare telehealth flexibilities through December 31, 2027. For behavioral health specifically: all psychotherapy codes remain on the telehealth-approved list permanently, geographic restrictions don’t apply, patients can receive care at home (POS 10), and audio-only sessions (modifier -93) are permanently covered for mental health.
Permanent doesn’t mean automatic. Telehealth claims fail at a higher rate than in-person claims — and the most common reason is a two-digit code entered incorrectly.
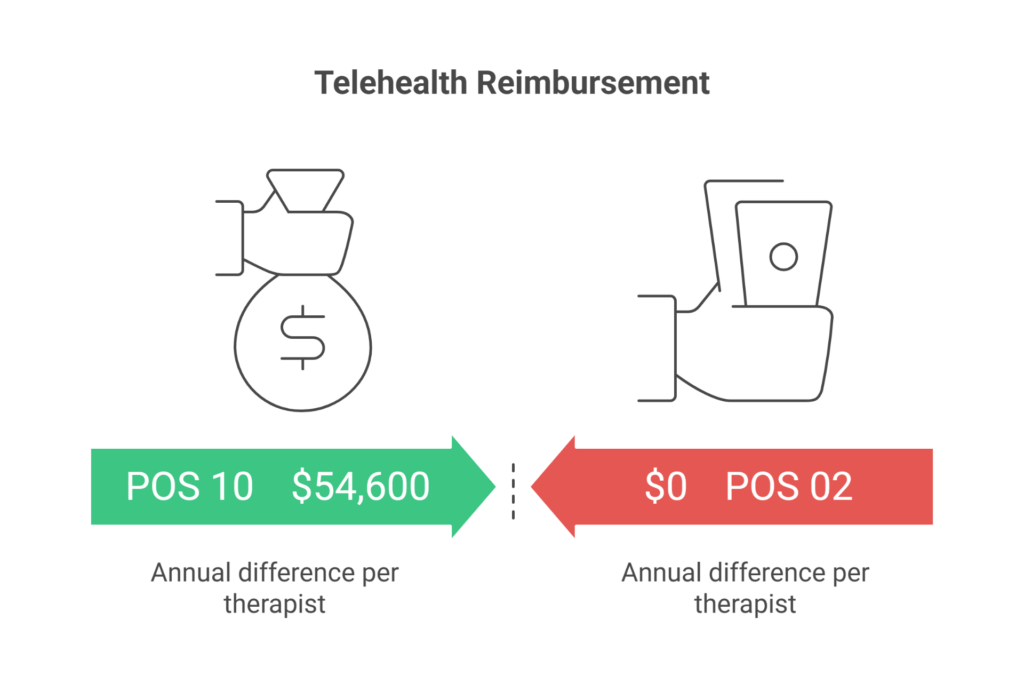
POS 02 vs POS 10: Where $54,600 Hides
This is the single most expensive mistake in telehealth billing, and it’s invisible unless you’re looking for it.
POS 10 (Telehealth Provided in Patient’s Home): Patient is in their private residence. Reimburses at the non-facility rate — same as an in-person office visit.
POS 02 (Telehealth Provided Other than Patient’s Home): Patient is at a clinic, school, workplace, or any location other than their home. Reimburses at the lower facility rate.
The financial difference for 90837 in 2026 Medicare: POS 10 pays approximately $167. POS 02 pays approximately $125. That’s $42 per session.
For a therapist seeing 25 patients per week through telehealth, and most of them are at home: using POS 02 when POS 10 is correct costs $42 × 25 sessions × 52 weeks = $54,600 per year. In lost revenue. From one two-digit code.
Decision logic: Ask yourself one question — where is the patient physically located during this session?
- At home/private residence → POS 10
- At a clinic, school, or any healthcare facility → POS 02
- At their workplace (non-healthcare) → POS 02
Telehealth Modifier Matrix by Payer (2026)
| Payer | Video Modifier | Audio-Only Modifier | POS Required | Notes |
|---|---|---|---|---|
| Medicare | -95 | -93 | 10 or 02 | -93 requires documentation of why video not used |
| BCBS (most states) | -95 | Varies by plan | 02 or 10 | Check alpha prefix for home plan rules |
| Aetna | -95 | Limited (select plans) | 10 required for home | POS 10 strictly required |
| UHC/Optum | -95 or -GT legacy | -93 (select plans) | 02 or 10 | -GT being phased out |
| Cigna/Evernorth | -95 | Not covered | 10 | Strict video requirement; no audio-only |
| TRICARE | -95 | -93 (rural/barriers) | 02 or 10 | Prime requires referral first |
| CA Medi-Cal | -95 + HO | -93 + HO | 10 | HO modifier required on every claim |
| TX Medicaid | -95 + HO/HN | -93 + HO/HN | 02 or 10 | Both HO and 95 required |
Audio-Only Documentation (Modifier -93)
Medicare permanently covers audio-only mental health services. But you must document:
- That audio-video was available to both parties
- The specific reason video wasn’t used (“patient declined for privacy reasons” or “insufficient bandwidth at patient’s location”)
- Patient identity was verbally confirmed
- Patient’s physical location was confirmed
- Patient provided verbal consent for audio-only format
Sample language: “Audio-video capability was available. Audio-only utilized per patient preference due to privacy concerns in shared residence. Patient identity confirmed via date of birth and last four of SSN. Patient located at [address]. Verbal consent obtained for audio-only telehealth.”
Without that documentation, -93 claims are vulnerable on post-payment review — even though the code is permanently covered.
Outpatient vs Inpatient Mental Health Billing Codes
When a patient moves from your outpatient practice to a hospital or residential program, the billing world changes completely. You shift from the CMS-1500 form and CPT codes to the UB-04 form, revenue codes, and DRGs. Many outpatient providers aren’t aware of how to bill if they’re seeing patients in hospital settings.
Level of Care Billing at a Glance
| Level of Care | Form | Primary Codes | Revenue Codes | Prior Auth |
|---|---|---|---|---|
| Outpatient individual | CMS-1500 | 90834, 90837 | 0914 | Rarely |
| Outpatient group | CMS-1500 | 90853 | 0915 | Rarely |
| Intensive Outpatient (IOP) | UB-04 | H0015, S9480, 90853 | 0904, 0906 | Yes (>20 sessions) |
| Partial Hospitalization (PHP) | UB-04 | G0410, G0411 | 0905, 0912/0913 | Always |
| Crisis Stabilization | UB-04 | H2011, S9484 | 0169 | Retrospective |
| Inpatient Psychiatric | UB-04 | DRG assignment | 0114, 0124 | Always |
| Residential Treatment | UB-04 | H0017, H0018, T1023 | 1001, 1002 | Always |
IOP requires: Minimum 9 hours per week of structured programming. Condition Code 92 on UB-04. Revenue code 0904. Per-component billing for Medicare, per-diem (S9480) for commercial.
PHP requires: Minimum 20 hours per week. Physician certification that the patient would otherwise require inpatient care. Revenue codes 0905 (PHP general), 0912 (half-day, under 6 hours), 0913 (full-day, 6+ hours). Condition Code 41 on UB-04.
Inpatient Psychiatric DRG Reference
When a patient is admitted to a psychiatric unit, the facility gets paid by Diagnosis-Related Group:
| MS-DRG | Diagnoses | Average LOS | Approximate Base Payment |
|---|---|---|---|
| 876 | Depressive/adjustment disorders | 3–5 days | $5,500–$7,500 |
| 885 | Psychoses (schizophrenia, bipolar acute) | 7–14 days | $8,500–$12,000 |
| 886 | Behavioral/developmental disorders | 5–10 days | $6,500–$9,500 |
| 887 | Other mental disorders | 4–8 days | $5,800–$8,000 |
An important distinction: when a patient is in an inpatient psychiatric unit, the hospital submits a UB-04 for room, board, nursing, and program costs, while the attending psychiatrist submits a separate CMS-1500 for their daily E/M visits (99221 for admission, 99231/99232/99233 for subsequent days). Both claims are necessary; neither covers the other.
BCBS and Commercial Payer Mental Health Billing Rules 2026
Blue Cross Blue Shield isn’t one company. There are 33 independent BCBS plans operating under a national licensing agreement — which means the rules for a BCBS patient in Illinois are genuinely different from a BCBS patient in Texas.
The BlueCard Program: Why Your Local Plan Isn’t Always the Decision-Maker
When an out-of-state BCBS patient sees you, their claim travels through a system called BlueCard:
- You bill your local BCBS plan (wherever you’re located)
- The claim routes to the patient’s home plan using a three-character alpha prefix on the member ID card
- The home plan determines medical policy and prior authorization requirements
- The local plan determines your contracted reimbursement rate
This creates a genuinely confusing situation where you might get denied by Illinois BCBS rules when you’re a Texas provider seeing an Illinois BCBS patient. Always verify benefits using Availity and specifically look up which plan’s rules govern prior authorization.
Commercial Payer Prior Authorization Triggers (2026)
| CPT Code | BCBS | Cigna | Aetna | UHC | TRICARE |
|---|---|---|---|---|---|
| 90837 (standard 60-min) | Varies by plan | Auth required | Auth after 12 | Auth required | None (<8 visits) |
| 90791 (initial eval) | Usually exempt | Usually exempt | Usually exempt | Usually exempt | None (<8 visits) |
| 96130 (psych testing) | Always | Always | Always | Always | Always |
| H0015 (IOP) | Always | Always | Always | Always | Always |
| 99484 (BHI) | Varies | Required | Varies | Varies | Usually not covered |
TRICARE Mental Health Billing
TRICARE Prime requires a referral from the patient’s Primary Care Manager (PCM) for all mental health services, including initial evaluations. TRICARE Select allows self-referral for the first 8 outpatient therapy visits per year without a referral.
After 8 visits in TRICARE Select or any visit in TRICARE Prime, prior authorization is required for continued outpatient care. Inpatient, IOP, and PHP services always require authorization under both plans. TRICARE reimbursement rates mirror Medicare rates — helpful for your financial modeling.
TRICARE service regions matter for which company administers benefits: Health Net Federal Services administers TRICARE East, while Humana Military administers TRICARE West.
Place of Service Codes for Mental Health Billing
Every CMS-1500 claim has a Box 24B that many providers treat as an afterthought. It’s not. The POS code tells payers where the patient was located, which determines whether you receive facility or non-facility rates.
Complete Mental Health POS Code Reference
| POS | Setting | Reimbursement | Common CPTs | Notes |
|---|---|---|---|---|
| 02 | Telehealth — not patient’s home | Facility rate (lower) | 90834-95, 90791-95 | Patient at clinic, school, work |
| 03 | School | Non-facility | 90834, H0004 | Private space documentation required |
| 10 | Telehealth — patient’s home | Non-facility (highest) | 90837-95, 90791-95 | Most common telehealth POS |
| 11 | Office | Non-facility (highest) | 90834, 90837 | Standard in-person therapy |
| 12 | Patient’s home (in-person) | Non-facility | 90834, 90837 | Requires travel documentation |
| 21 | Inpatient hospital | Facility | 99221–99233 | Psychiatrist daily rounding |
| 22 | On-campus outpatient hospital | Facility | 90834, 90791 | Hospital-based psych clinic |
| 23 | Emergency room | Facility | 99281–99285, 90839 | Psychiatric emergency evaluation |
| 52 | Partial hospitalization | APC bundled | G0410, G0411 | Facility billing only |
| 53 | Community mental health center | Non-facility | 90853, H0015 | CMHC-based services |
The revenue difference between POS 10 (non-facility) and POS 02 (facility) for a single 90837 session is approximately $42 in 2026 Medicare rates. For a practice with 20 telehealth sessions daily, ensuring POS 10 is used for home-based patients represents over $200,000 in annual revenue protection. Get this right.
Common Mental Health Billing Code Errors and How to Avoid Them
Behavioral health has the highest claim denial rate in healthcare — 15–25% compared to 5–10% for medical/surgical claims. After reviewing thousands of behavioral health claims, the same errors appear again and again.
Top 10 Mental Health Billing Errors (Ranked by Annual Revenue Impact)
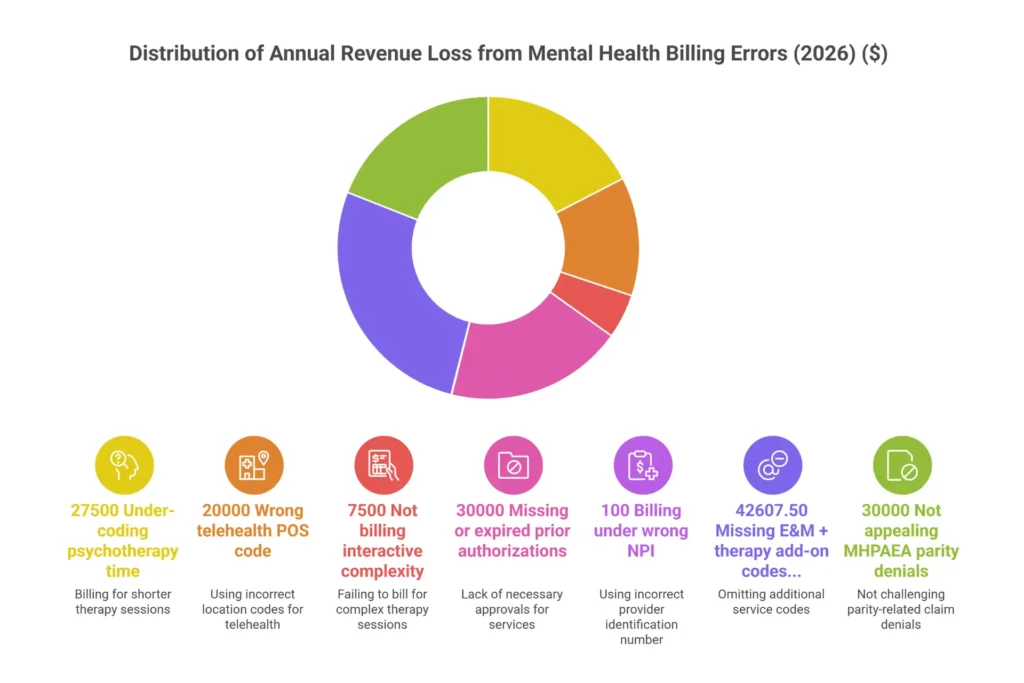
Error #1: Billing 90837 for 52-minute sessions (Upcoding) The midpoint rule means 90837 requires 53 minutes minimum. Practices that round every 50–52 minute session to 90837 get flagged by statistical outlier analysis. Annual impact: $20,000+ in potential recoupment. Fix: Use EHR timers, document exact start/stop times.
Error #2: Missing -95 modifier on telehealth claims Most billing systems won’t automatically add -95. It must be deliberately appended. A video session without -95 denies on CO-4 (modifier inconsistency). Annual impact: $15,000+ in denied claims. Fix: Build a charge capture alert that flags any 90832–90837 without a POS of 11 or a modifier.
Error #3: Wrong time code on edge sessions (52-minute as 90837) Slightly different from Error #1 — this is the accidental 52-minute session billed as 90837. Not pattern-based; just a one-time error. Annual impact: $10,000+ across a practice. Fix: EHR start/stop time capture, not estimation.
Error #4: Using F32.9 indefinitely Unspecified codes flag utilization management reviews after 2–3 uses for the same patient. Annual impact: $8,000+ in medical necessity denials. Fix: Implement a “diagnosis escalation” policy — review and update specificity by the 3rd session.
Error #5: Z-codes as primary diagnosis Z63.0 (relationship problems) as the only diagnosis code for 90837 will deny on PR-49 from every major payer. Annual impact: $7,000+. Fix: Always lead with an F-code; use Z-codes only as secondaries.
Error #6: Bundling 90791 and 90837 on the same date NCCI edits bundle the initial evaluation and therapy when billed together without a valid modifier and clear documentation of medical necessity for both. Annual impact: $12,000+ in bundled denials. Fix: One code per date policy, or use modifier 59 with thorough documentation if clinically justified.
Error #7: Missing -25 on psychiatrist’s E/M + therapy add-on Without modifier 25 on the 99214, the E/M bundles with 90833 and you collect for one. Annual impact: $5,000+. Fix: Psychiatrist charge entry template with -25 pre-populated for any session with both codes.
Error #8: Missing HO/HN in Medicaid states In California, Texas, Florida, and New York, every claim without the appropriate provider level modifier denies on CO-16. Annual impact: $8,000+ depending on Medicaid panel size. Fix: State-specific modifier rules in your billing system by payer.
Error #9: POS 02 when POS 10 is correct (telehealth) This one doesn’t trigger a denial — it just underpays you. Annual impact: $42 per session × volume. Fix: Verify patient location at the start of every telehealth session and document it.
Error #10: 90785 add-on without criteria documentation Interactive complexity denies without specific criteria documentation. Annual impact: $4,000+ in add-on denials. Fix: Create a 90785 criteria checklist in your EHR template.
Pre-Claim Submission Checklist
Before any claim goes out, run through these:
- Time documented (start and stop) for all 90832/90834/90837
- Correct time code matches exact minutes (53+ for 90837)
- ICD-10 F-code present and specific (not just Z-codes)
- Diagnosis pointer linking ICD-10 to CPT is correct
- Telehealth modifier present if telehealth (95 or 93)
- POS 10 for home-based telehealth (not 02 or 11)
- State Medicaid modifiers (HO/HN) present where required
- -25 on E/M codes when therapy add-on is also billed
- -59 or appropriate X-subset when two procedures same day
- 90785 criteria documented in the note before billing the add-on
Consistent billing errors cost behavioral health practices an average of $25,000–$45,000 annually. Our charge entry and claim submission services catch these before they become denials.
🧮 Mental Health Billing Revenue Leak Calculator
Find out how much unbilled, under-billed, or denied revenue your practice may be losing annually.
Estimated Annual Revenue Leakage
Estimates are based on average error rates observed across behavioral health practices. Actual revenue impact varies by practice size, payer mix, and current billing processes. Not a guarantee of recoverable revenue.
Documentation Requirements for Mental Health Billing Compliance

Your clinical note is not separate from your revenue cycle. It is your revenue cycle. The documentation you write (or don’t write) within 72 hours of a session determines whether you get paid, get audited, or get recouped.
What CMS Article A57480 Actually Requires
CMS Article A57480 is the Medicare Local Coverage Determination governing psychotherapy medical necessity. What providers actually need to document:
- Date of service and patient identifier
- Provider credentials (license type and number)
- Chief complaint or reason for visit
- Specific interventions used (CBT, DBT, motivational interviewing — not just “therapy”)
- Patient response to the intervention within the session
- Progress toward treatment goals (referenced by number or name)
- Plan for next session
- Provider signature with credentials
For time-based codes: exact start and stop times are required. “Approximately 60 minutes” is not compliant. “50-minute session” is not compliant. “Start 10:05 AM, end 11:02 AM (57 minutes)” is compliant.
Documentation Requirements by CPT Code
| CPT Code | Minimum Note Content | Time Documentation | Common Audit Flag |
|---|---|---|---|
| 90832 | 2+ interventions, patient response | Start/stop times required | Total time under 16 minutes |
| 90834 | Same + progress toward goals | Start/stop times required | “Good session” — no specifics |
| 90837 | Same + barriers addressed, risk screened | Start/stop, 53+ min | Time note says “1 hour” not exact |
| 90791 | Full MSE (all 9 elements), history, safety | N/A | Incomplete MSE |
| 90839 | Crisis event, risk assessment, specific interventions, disposition | 30+ min start/stop | No documented crisis trigger |
| 90785 | Which of 4 criteria, specific example | N/A | Criteria not stated explicitly |
| 90853 | Per-patient response noted individually | N/A | Identical notes across group members |
The Mental Status Exam Elements (Required for 90791/90792)
Your initial evaluation note must document all MSE components: appearance, behavior, speech, mood (patient’s subjective report), affect (your observation), thought process, thought content, cognition, insight, and judgment. Missing even one element creates an audit vulnerability for 90791.
HIPAA: Psychotherapy Notes vs Progress Notes
This distinction trips up many providers, especially those from training programs that taught process-oriented documentation:
Progress notes are the clinical records used for billing. They document what service was provided, to whom, when, for how long, what interventions were used, and patient response. These must be shared with payers upon request and with patients upon request.
Psychotherapy notes are the therapist’s personal process notes — raw session observations, hypotheses, countertransference reactions. HIPAA gives these special protection. They don’t need to be shared with payers or other providers without specific patient authorization.
The practical problem: some providers keep only psychotherapy notes and use them to justify billing. You can’t bill from psychotherapy notes. You need compliant progress notes that meet CMS requirements and are separate from your personal process documentation.
Practices that want patient documentation services or a documentation audit — reviewing whether current notes would survive payer scrutiny — can reach out to our compliance team.
✅ Mental Health Billing Error Prevention Checklist 2026
Check each item your practice has covered. Click a button below to download directly as a PDF file — no print dialog, no page selection.
Found gaps in your billing process? Our mental health billing specialists handle everything so you can focus on patients, not paperwork.
Get a Free Audit →Voice Search Questions: Quick Answers for Mental Health Billing
What are the CPT codes for mental health billing? The core mental health CPT codes are 90832 (30-minute therapy), 90834 (45-minute therapy), 90837 (60-minute therapy), 90791 (psychiatric diagnostic evaluation), and 90839 (crisis psychotherapy). Add-on codes include 90785 for interactive complexity and 90833/90836/90838 for therapy delivered alongside E/M services.
What is the difference between CPT codes 90832, 90834, and 90837? All three are time-based individual psychotherapy codes. The difference is session duration: 90832 covers 16–37 minutes, 90834 covers 38–52 minutes, and 90837 covers 53 minutes or longer. Document exact start and stop times — billing 90837 for a 52-minute session is considered upcoding.
Does Medicaid cover mental health therapy sessions? Yes. Medicaid covers psychotherapy (90832–90837), psychiatric evaluations (90791/90792), and crisis services (90839) in all 50 states. Many states also reimburse HCPCS H-codes like H0004 for community-based behavioral health services. Session limits, prior authorization thresholds, and required modifiers vary significantly by state.
What is the 3-month rule in mental health billing? The 3-month rule refers to Medicaid’s retroactive eligibility provision. When a patient is approved for Medicaid, coverage can be applied back up to 3 months before the application date, provided the patient would have met eligibility criteria during that period. Providers can bill for services rendered during that retroactive window after eligibility is confirmed.
What modifier is used for telehealth mental health services? Modifier -95 indicates synchronous (real-time) audio-video telehealth. Modifier -93 indicates synchronous audio-only telehealth when video isn’t available or the patient declines video. Both must be paired with the correct Place of Service code: POS 10 for sessions where the patient is at home, POS 02 for any other patient location.
What is the difference between POS 02 and POS 10 for telehealth? POS 10 is used when the patient is in their private home during a telehealth session — it reimburses at the higher non-facility rate. POS 02 is used when the patient is at any other location (clinic, school, workplace) — it reimburses at the lower facility rate. For a 90837 session in 2026 Medicare, the difference is approximately $42 per session.
Can LPCs and LCSWs bill Medicare for mental health services? Yes. Licensed Clinical Social Workers (LCSWs) have been Medicare providers for years, and Licensed Professional Counselors (LPCs) and Licensed Marriage and Family Therapists (LMFTs) became eligible Medicare providers starting January 1, 2024. LPCs and LMFTs are reimbursed at 75% of the Medicare Physician Fee Schedule rate and must be enrolled via PECOS or CMS-855I.
What is the billing code for mental health crisis services? CPT 90839 covers crisis psychotherapy for the first 60 minutes (minimum 30 minutes) when a patient is in acute distress or at imminent risk of harm. CPT 90840 is the add-on for each additional 30 minutes beyond 74 total minutes. For Medicaid mobile crisis teams, H2011 is billed in 15-minute units. Facility-based crisis stabilization typically uses HCPCS S9484 on a UB-04 claim.
Frequently Asked Questions About Mental Health Billing Codes
What are the most common mental health billing codes?
The highest-volume mental health CPT codes are 90834 (45-minute psychotherapy), 90837 (60-minute psychotherapy), 90791 (psychiatric diagnostic evaluation), and 90853 (group therapy). For Medicaid practices, H0004 (behavioral health counseling, per 15 minutes) and H2011 (crisis intervention) also appear frequently. The specific codes a practice relies on depend heavily on provider type, treatment modality, and payer mix.
What is the difference between CPT 90832, 90834, and 90837?
These codes represent the same service — individual psychotherapy — at different time thresholds. 90832 is for sessions lasting 16–37 minutes, 90834 is for 38–52 minutes, and 90837 is for 53 minutes or longer. The 53-minute minimum for 90837 comes from the midpoint rule between the 52-minute maximum of 90834 and the 60-minute benchmark. Billing 90837 for 52 minutes is upcoding and triggers statistical audit flags when it appears as a pattern.
What ICD-10 codes are used for mental health billing?
The most commonly billed mental health ICD-10 codes are F41.1 (generalized anxiety disorder), F32.1 (major depressive disorder, moderate), F33.1 (recurrent MDD, moderate), F43.10 (PTSD, unspecified), and F90.2 (ADHD, combined type). Unspecified codes like F32.9 and F41.9 are acceptable for the first 1–2 visits but should be replaced with more specific codes as the clinical picture clarifies. Z-codes (like Z63.0 for relationship problems) can only be used as secondary diagnoses alongside a primary F-code.
What modifier codes are required for mental health billing?
For telehealth sessions, modifier -95 (audio-video) or -93 (audio-only) is required by Medicare and most commercial payers. Modifier -25 is required on E/M codes (like 99214) when a psychiatrist also provides a separate therapy add-on on the same day. Modifier -59 is needed when two distinct procedures are performed on the same date. For Medicaid in California, Texas, Florida, New York, and Illinois, provider level modifiers (HO for master’s level, HN for bachelor’s level) are required on every claim.
How do I bill Medicaid for mental health services?
Medicaid mental health billing typically requires standard CPT codes (90832–90837 for therapy, 90791 for evaluations) plus state-specific provider modifiers (HO/HN in most states) and any applicable telehealth modifiers. Many states also use HCPCS H-codes for community-based services that don’t fit CPT descriptions. Prior authorization requirements range from never (rare) to after 8 visits (Florida). Always verify session limits, modifier requirements, and PA thresholds for your specific state’s program and any managed care organizations in your patient’s plan.
What mental health billing codes does Medicare cover in 2026?
Medicare Part B covers all time-based psychotherapy codes (90832–90837), diagnostic evaluations (90791/90792), crisis codes (90839/90840), family therapy (90846/90847), group therapy (90853), psychological testing (96130–96139), and general behavioral health integration (99484). The CoCM codes G0568–G0570 replaced the previous 99492–99494 codes in 2026. LPCs and LMFTs are now covered providers, reimbursed at 75% of the Physician Fee Schedule. Telehealth is permanently covered for all these services.
What is the difference between T1019 and T1020 in mental health billing?
T1019 and T1020 are HCPCS codes for personal care services in Medicaid waiver programs — not psychotherapy codes. T1019 is billed per 15 minutes for hands-on personal care assistance (ADLs, brief respite) that supports mental health stability in the community. T1020 is billed per diem for a full day (24 hours) of structured personal care or respite. Neither code should be used for therapy sessions; use 90834 or 90837 for clinical psychotherapy.
What is the 3-month rule in mental health billing?
The 3-month rule refers to Medicaid’s retroactive eligibility provision: if a patient is approved for Medicaid, the coverage period can be backdated up to 3 months before the application date if the patient would have been eligible during that window. This allows providers to bill for services already rendered — but only after eligibility is confirmed, and only within the state’s timely filing window. Some states have reduced or eliminated retroactive eligibility through state plan waivers.
Can I bill 90785 (interactive complexity) alongside any therapy code?
No. 90785 is a specific add-on code requiring one of four documented criteria: maladaptive communication between patient and caregiver that disrupts the session; a caregiver interfering with or blocking treatment; a sentinel event requiring mandated reporting; or communication barriers requiring special equipment or interpreter services. It can only be billed alongside 90791/90792, 90832/90834/90837, 90839/90840, or 90846/90847. The criteria must be explicitly documented in the note — stating that a session was “complex” is insufficient.
What CPT codes can LCSWs and LPCs bill to insurance?
LCSWs and LPCs can bill all time-based psychotherapy codes (90832, 90834, 90837), the diagnostic evaluation without medical services (90791), crisis codes (90839/90840), family therapy (90846/90847), group therapy (90853), interactive complexity add-on (90785), and general BHI (99484). They cannot bill codes requiring medical services: 90792 (eval with medical), 99202–99215 (E/M codes), or the therapy add-ons 90833/90836/90838 (which require an E/M code from a prescriber). Medicare enrollment for LPCs and LMFTs requires PECOS enrollment and yields 75% of the physician fee schedule rate.
What is the billing code for mental health crisis services?
CPT 90839 covers the first 60 minutes of crisis psychotherapy (minimum 30 minutes) — for acute situations involving imminent risk or severe decompensation. CPT 90840 covers each additional 30-minute increment beyond 74 total minutes. Documentation must describe the crisis event specifically, not just note “high acuity.” For Medicaid community-based crisis teams, H2011 is billed per 15-minute unit. Hospital-based crisis stabilization units typically bill S9484 (per diem) or H0039 on UB-04 claims.
Is CPT 99214 used in mental health billing?
Yes. CPT 99214 is an Evaluation and Management code used by psychiatrists, psychiatric nurse practitioners, and physician assistants for medication management visits of moderate complexity. It is not a psychotherapy code — it covers the medical decision-making involved in prescribing and monitoring psychiatric medications. When a prescriber provides medication management (99214) and also delivers separate, documented psychotherapy on the same day, they bill 99214 with modifier -25 plus the appropriate therapy add-on code (90833, 90836, or 90838). Both services must be documented separately.
Conclusion: Stop Losing Revenue to Codes
Mental health billing codes aren’t obstacles between you and your patients — they’re the financial infrastructure that keeps your practice running. Get them right, and you collect what your work is worth. Get them wrong, and you fund your payers’ profits with your own uncollected revenue.
The three most important things to take away from this guide:
First, document time precisely. Start and stop times, exact minutes, specific interventions — not estimates, not approximations. The difference between 52 minutes and 53 minutes is the difference between 90834 and 90837. That difference matters in a RAC audit.
Second, know your payer rules. Medicaid in Florida operates nothing like Medicaid in California. Medicare has different rules than Cigna. The modifier that gets you paid in Texas Medicaid will cause a denial on a New York Medicaid claim. Payer rules aren’t static — they change, and your billing system needs to reflect those changes.
Third, treat ICD-10 as a clinical narrative, not an administrative checkbox. Payers read your diagnosis codes as evidence of medical necessity. An unspecified code after the fourth session tells them you haven’t done a thorough assessment. A specific, severity-coded diagnosis tells them this patient genuinely needs skilled behavioral health intervention.
If you’re seeing denial rates above 8%, billing the wrong POS for telehealth, getting Medicaid claims rejected for missing modifiers, or just not sure whether your documentation would hold up to an audit — that’s worth fixing before it compounds.
Elite Med Financials specializes in behavioral health revenue cycle management. We understand the specific challenges of mental health billing: the parity law disputes, the state Medicaid variation, the telehealth POS confusion, the documentation compliance requirements. Our team reviews your top 50 claims at no cost and shows you exactly where revenue is leaking — with a specific, actionable plan to stop it.
Get Your Free Behavioral Health Billing Audit →
Or explore how our full RCM services for healthcare providers can support your practice from credentialing through collections.
Sources: CMS Medicare Physician Fee Schedule CY 2026, CMS Article A57480, AMA CPT® 2026 Professional Edition, CMS Consolidated Appropriations Act Telehealth Guidance, CMS Medicaid State Plan Data. All reimbursement rates are approximate national averages; actual payment varies by geographic GPCI adjustment, provider type, and payer-specific contracted rates.
Internal Resources: What Is Mental Health Billing? | Mental Health CPT Codes Guide | How to Choose a Mental Health Billing Service | Revenue Cycle Management Guide | Healthcare Revenue Cycle Overview

