
Here is the reality: outpatient wound care billing carries a CERT audit error rate near 25%, nearly triple the Medicare Part B average. That number is not an accident. It is the result of practices treating wound care billing like basic office billing—same rules, same codes, same casual documentation habits. This guide exists because that approach fails, and it fails expensively.
What you are about to read covers every element of outpatient wound care billing for 2026—Place of Service restrictions that determine which codes even pay, the full CPT code reference from 97597 through 15271, the ICD-10 depth logic that auditors cross-reference against your procedure codes, and the January 2026 $127.14 per square centimeter flat rate for skin substitutes that changed the economics of graft billing overnight. We also cover the denials that are quietly bleeding most practices dry, and the documentation that makes the difference between a paid claim and a 120-day appeals cycle. This is written by people who have submitted these claims and sat through MAC audits—not consultants who read the policies and summarized them.
Table of Contents
What Is Outpatient Wound Care Billing — And Why the Setting Changes Everything
The Place of Service code on your CMS-1500 claim form is not an administrative formality. It is the master key that determines which CPT codes are payable, what your reimbursement rate will be, and whether your patient’s care is even eligible for Part B coverage.
Outpatient wound care billing refers to the billing of wound management services—debridement, negative pressure wound therapy, skin substitutes, compression, and related procedures—performed outside of an inpatient hospital stay. That definition sounds simple, but the payment logic underneath it is not. Medicare pays differently depending on whether your patient is sitting in your private office, a hospital-based wound clinic, or a skilled nursing facility. The CPT codes stay the same. The POS code changes everything else.
Understanding this distinction is particularly important in 2026 because the convergence of the new skin substitute flat rate, updated documentation requirements for compression codes, and ongoing OIG focus on wound care upcoding means that a billing error in the wrong setting can trigger recoupment, TPE review, and in serious cases, False Claims Act exposure. The setting is not just a billing question—it is a compliance question.
POS 11, POS 22, and POS 31 — What Changes With Each Setting
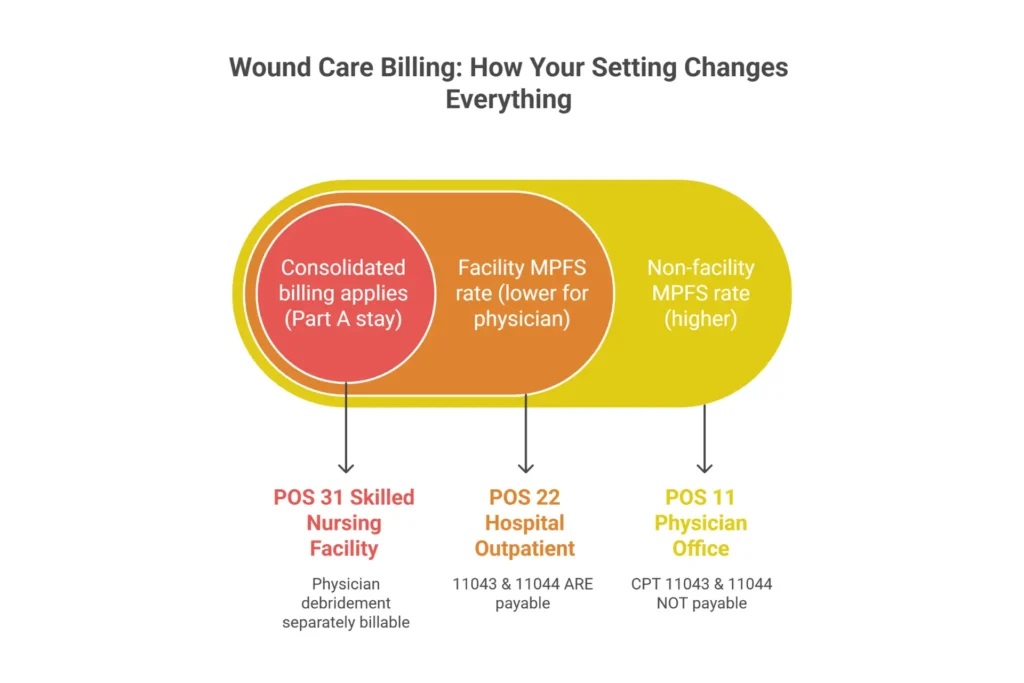
In POS 11 (physician office), you bill under the Medicare Physician Fee Schedule at the non-facility rate. That rate is higher than the facility rate because it is meant to account for overhead—your equipment, your staff, your supplies. It is a more favorable rate for many debridement codes. But the trade-off is that several CPT codes are simply not payable here. CPT 11043 (muscle and fascia debridement) and CPT 11044 (bone debridement) are facility-restricted. Bill them with POS 11 and you will receive a denial. Worse, if your EHR auto-populates POS 11 and your providers routinely document bone or muscle involvement, you have a systematic upcoding exposure that a RAC contractor will eventually find.
In POS 22 (hospital outpatient department, HOPD), the billing splits between two claims. The physician submits a professional claim on the CMS-1500 at the facility rate (which is lower than the non-facility rate). The hospital submits a facility fee claim on a UB-04 under the Outpatient Prospective Payment System (OPPS) using Ambulatory Payment Classification (APC) logic and revenue codes such as 0361 (minor surgery) or 0510 (general clinic). The combined payment from both claims is typically higher than what the physician would have received alone in POS 11—which is why hospital outpatient departments generate more total revenue per wound care encounter. Critically, the facility overhead in POS 22 makes 11043 and 11044 payable, because the hospital facility fee accounts for the operating room and sterile field resources those codes require.
In POS 31 (skilled nursing facility), the billing rules shift again. If the patient is in a covered Medicare Part A stay, consolidated billing applies—routine wound care services are bundled into the SNF’s daily Part A rate and cannot be billed separately by the physician. However, certain physician services—including surgical debridement performed by an independent physician—are separately billable under Part B, as long as the claim is submitted correctly and documentation clearly supports physician involvement rather than facility staff care. Getting this wrong is one of the most common SNF billing errors we see.
⚠️ The 97602 Status B Trap — Paying $0.00 in Your Own Office
CPT 97602 (non-selective debridement—wet-to-dry, enzymatic) carries a Status B indicator on the Medicare Physician Fee Schedule. In plain English: it pays zero dollars in POS 11. The claim processes, it shows $0.00 paid, and unless you are tracking paid amounts by CPT code, you will never notice. If your providers are performing debridement in the office and billing 97602, they are working for free on every one of those claims.
The fix is clinical documentation: if the debridement involved a scalpel, scissors, curette, or forceps to selectively remove devitalized tissue while preserving viable dermis, that is CPT 97597—selective debridement—which is separately payable in POS 11. Your note must describe the technique, tissue type removed, and wound measurements. If the debridement was truly non-selective (mechanical wet-to-dry removal, enzymatic creams), 97602 is the accurate code—but that service is only separately reimbursable in a facility setting under OPPS. Run a report on your paid claims by CPT code. If 97602 appears in POS 11 with $0.00 reimbursed, act on it now.
Understanding the MPFS vs. APC Payment Difference
Providers who run wound clinics in both office-based and hospital-based settings often ask why the same service pays differently depending on the setting. The answer is in the payment system. In POS 11, you are paid under the Medicare Physician Fee Schedule (MPFS), which calculates payment from Relative Value Units (RVUs) and a conversion factor. In POS 22, the physician is paid the lower facility MPFS rate, and the hospital collects the APC facility payment on top of it. This is why the “where” is not just administrative detail—it is reimbursement strategy. For practices considering whether to affiliate with a hospital outpatient department, the financial modeling of professional vs. facility revenue is a real RCM analysis, not a trivial one. Our wound care RCM guide covers setting-specific revenue optimization in detail.
CPT Codes for Outpatient Wound Care: Full 2026 Reference
Every wound care CPT code has a depth rule, an NCCI bundling profile, a setting restriction, and a documentation requirement. If you do not know all four for the codes you bill, you are guessing—and Medicare’s automated edits are not guessing.
This section covers the complete outpatient wound care CPT list for 2026. Our dedicated wound care billing codes reference goes deeper on each code family if you need the granular detail. Here, we focus on the billing logic that actually determines whether your claim pays.
Active Wound Care Management — 97597, 97598, and the 97602 Trap
CPT 97597 covers selective debridement of the first 20 square centimeters. Selective means you are using clinical technique—scalpel, scissors, curette, or forceps—to remove devitalized tissue (slough, fibrin, biofilm) while preserving viable tissue underneath. Your documentation must include the tissue type removed (percentage of slough, eschar, fibrin), wound measurements in centimeters, and confirmation of the technique used. The 2026 non-facility rate sits in the $110–$140 range, and the MUE limit is 4 units per claim date. This is the code you want to be billing in your office when providers perform clinical debridement.
CPT 97598 is the add-on code for each additional 20 sq cm of selective debridement beyond the first unit. Never bill 97598 without a primary 97597 unit—add-on codes cannot stand alone. The MUE for 97598 is 12 units, which gives you substantial room for larger wounds, but documentation must account for each 20 sq cm increment clearly.
CPT 97602 is non-selective debridement—wet-to-dry mechanical removal, enzymatic agents, or autolytic methods. As detailed in the callout above, this is Status B in POS 11. It pays $0.00. Do not bill it in the office. The only appropriate setting for separately-payable 97602 billing is a facility context under OPPS.
Surgical Debridement — 11042 Through 11047, and the Depth Rule That Determines Everything
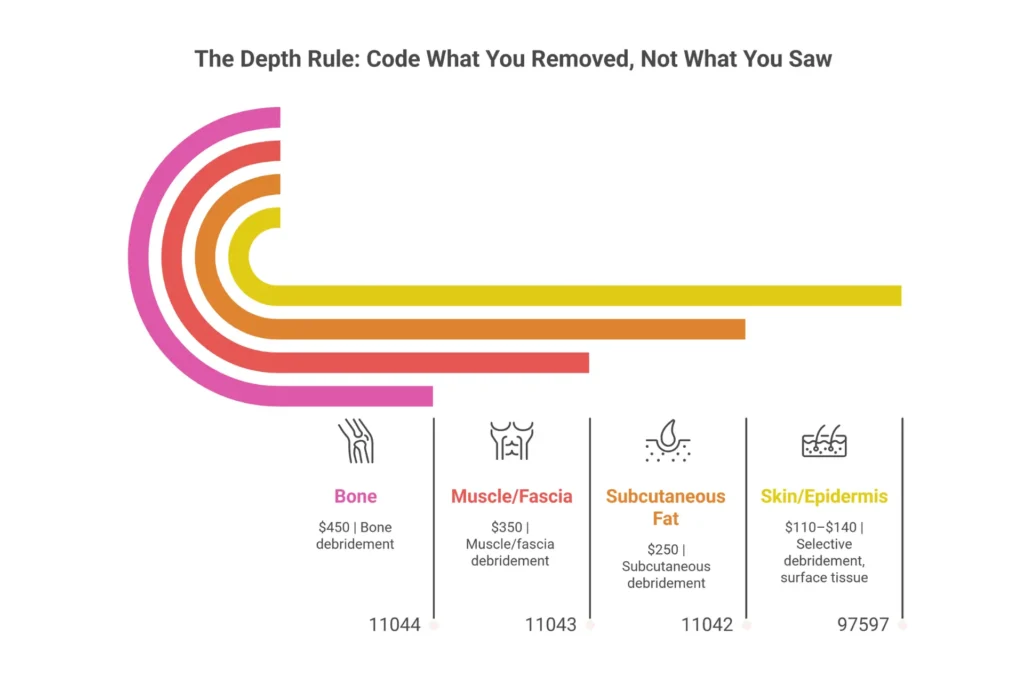
The surgical debridement codes operate on one principle that sounds simple but is widely misapplied: you code by the deepest tissue layer actually removed, not by what you can see in the wound. Bone visible in the wound base is not the same as bone debrided. Muscle exposed to view is not the same as muscle excised. OIG Work Plan audits for 2025–2026 specifically target CPT 11044 (bone debridement) claims where documentation does not support actual bone removal—it is one of the highest-dollar audit triggers in wound care.
CPT 11042 covers subcutaneous tissue debridement for the first 20 sq cm. The note must describe excision of non-viable subcutaneous adipose to bleeding margins—exact language matters. The 2026 non-facility rate is approximately $250. This is payable in POS 11 and POS 22.
CPT 11043 covers muscle and fascia debridement. Facility-only. Do not bill in POS 11. Approximately $350 at the facility rate. Requires documentation of muscle fascia involvement—naming the specific muscle or fascia layer debrided, depth reached, and excisional technique.
CPT 11044 covers bone debridement. Facility-only. Approximately $450 at the facility rate. Documentation must describe tangible bone removal: “cortical bone debridement performed with rongeur, non-viable cortical fragments removed to healthy bleeding margins.” “Bone visible” is not sufficient and will be flagged in an ADR review.
CPT 11045, 11046, 11047 are add-ons for each additional 20 sq cm at the subcutaneous, muscle, and bone levels respectively. Same depth matching rules apply—sequence the primary code first, then the add-on at the same depth level.
When treating multiple wounds, sum the areas of wounds at the same depth and bill a single primary code plus the appropriate add-ons. Do not bill one 11042 per wound—aggregate same-depth wounds and use the add-on structure.
NPWT Codes — What Is the Difference Between 97606 and 97608?
The most common question we get about NPWT billing is the 97606 vs. 97608 distinction. The answer is simpler than most people think: the device type determines the code, not the wound type.
CPT 97605 and 97606 are for durable (reusable) negative pressure wound therapy pumps. 97605 covers wounds up to 50 sq cm; 97606 covers wounds larger than 50 sq cm. Under these codes, the clinic bills only for the professional service component. The DME supplier—not the physician—bills for the pump and supplies (A6550 for canisters, A7000 for dressing kits, E2402 for the pump itself) through a separate DME claim.
CPT 97607 and 97608 are for disposable (single-use) NPWT devices. 97607 covers wounds up to 50 sq cm; 97608 covers wounds over 50 sq cm. These are all-inclusive codes. The payment covers both the professional service and the disposable device. Do not bill A6550, A7000, or any other supply code alongside 97607 or 97608—that constitutes unbundling and triggers automatic denial plus audit exposure. The 2026 non-facility rate for 97607 is approximately $300; for 97608, approximately $400.
Compression Codes — 29580, 29581, and the 2026 Documentation Change
CPT 29580 (Unna boot) and CPT 29581 (multilayer compression bandage) both received updated descriptor language effective January 1, 2026 that introduces a physician-directed application requirement. This means the note can no longer simply state that compression was applied—it must document clinical direction and the vascular assessment (ABI or distal pulse documentation) that justifies compression. Applying high-gradient compression to a patient with arterial insufficiency carries clinical and liability risk, and CMS updated these descriptors to formalize the oversight requirement. Without the vascular assessment notation, expect denials or ADR requests.
E/M Codes and Modifier 25 in Wound Care
You can bill an evaluation and management service on the same day as a procedure—but only when the E/M involves significant, separately identifiable work above and beyond the pre-procedural examination of the wound you are about to debride. The pre-procedure check does not count. If your provider assessed new cellulitis spreading beyond the wound margin, adjusted antibiotic therapy, reviewed cultures, or managed an unrelated complication, that is a legitimate modifier 25 E/M. If the note essentially describes assessing the wound and performing debridement, modifier 25 will not survive an audit. The OIG currently estimates that 35–40% of modifier 25 wound care claims are insufficiently documented.
| CPT Code | Description | Setting | 2026 Rate (Non-Fac) | MUE |
|---|---|---|---|---|
| 97597 | Selective debridement, first 20 sq cm | Office / HOPD | ~$110–$140 | 4 |
| 97598 | Selective debridement, add-on per 20 sq cm | Office / HOPD | Add-on | 12 |
| 97602 | Non-selective debridement (Status B — POS 11) | ⚠ NOT POS 11 | $0 in office | — |
| 11042 | Subcutaneous debridement, first 20 sq cm | Office / HOPD | ~$250 | — |
| 11043 | Muscle/fascia debridement | Facility Only | ~$350 | — |
| 11044 | Bone debridement | Facility Only | ~$450 | — |
| 97605 | NPWT durable pump, ≤50 sq cm | Any | ~$150 | — |
| 97606 | NPWT durable pump, >50 sq cm | Any | ~$200 | — |
| 97607 | NPWT disposable (all-inclusive), ≤50 sq cm | Any | ~$300 | — |
| 97608 | NPWT disposable (all-inclusive), >50 sq cm | Any | ~$400 | — |
| 29580 | Unna boot application (vascular assessment req.) | Any | ~$80 | — |
| 29581 | Multilayer compression bandage | Any | ~$90 | — |
Billing for Wound Care Supplies in the Outpatient Setting
The most expensive supply billing mistake is not using the wrong A-code—it is billing A-codes for supplies you handed to the patient after their office procedure. Those are bundled. The only separately-billable supplies under Medicare Part B are items you send home with the patient for self-care.
This distinction—in-office vs. take-home—is where the majority of supply billing denials originate. Supplies used during debridement, applied after a skin substitute, or used to dress a wound immediately post-procedure are included in the payment for that procedure. Medicare does not separately reimburse for those materials. Billing HCPCS A-codes for supplies consumed during an in-office procedure constitutes unbundling and will trigger a CO-16 or CO-97 denial. Our full wound care billing guidelines cover supply documentation in depth.
Standard Written Order — What Medicare Actually Requires
Before a single take-home supply claim can be submitted, a Standard Written Order (SWO) must exist. This is not optional, and missing or incomplete SWOs are the primary driver of CO-96 denials in wound supply billing. Per CMS documentation requirements, the SWO must include the beneficiary’s name and Medicare Beneficiary Identifier (MBI), the order date, a specific item description with the HCPCS code (not just “wound dressings”), the quantity to be dispensed, the frequency of dressing changes, and the prescriber’s name, NPI, and signature.
The SWO must be completed before the supplies are delivered—backdating is not permitted and will be identified in audit. Renew the SWO every 90 days or whenever the clinical plan changes. A frequency change alone (say, from daily to twice-daily for increased exudate) requires an updated SWO. Missing the renewal date is the single most common reason for supply recoupment in TPE reviews.
HCPCS A-Code Selection — Matching the Dressing to the Wound
Selecting the correct A-code is not arbitrary—it is clinical decision-making that must be documented in the patient chart. The HCPCS Level II A-code selection depends on dressing type, sterility, and pad size (not wound size—a distinction auditors check consistently). For Medicare, dressings may not exceed three times the wound area in size. Here is the selection logic for the most commonly billed codes:
| HCPCS Code(s) | Dressing Type | Clinical Indication | Exudate Level |
|---|---|---|---|
| A6222–A6224 | Impregnated gauze (non-water based) | Infected or contaminated wounds | Scant–Moderate |
| A6225–A6227 | Impregnated gauze (water/saline) | Clean wounds requiring moisture | Scant–Moderate |
| A6234–A6235 | Hydrocolloid wafers (by size) | Stage 2 pressure injuries, low exudate wounds | Scant–Moderate |
| A6209–A6211 | Foam dressings (sterile) | Granulating wounds, moderate exudate | Moderate |
| A6200–A6202 | Composite dressings | Wounds needing absorption + non-stick layer | Moderate–Heavy |
| A6196–A6198 | Alginate / fiber dressings | Heavily exuding wounds, cavity wounds | Heavy |
| A6550 | NPWT wound cover (canister) | Durable NPWT only (97605/97606) | Via pump |
The clinical documentation must align with the HCPCS selection. If you are billing A6196 (alginate), your note must describe heavy exudate with documented measurement. If Medicare’s automated systems see alginate billed consistently for wounds with documented scant drainage, recoupment is likely. This is not about gaming codes—it is about ensuring the clinical documentation actually matches the product you are using, which it should if the product selection is clinically appropriate.
Bundled vs. Separately Billable — Getting This Right
The rule: supplies applied in the clinic immediately during or following a procedure are bundled. Supplies dispensed to the patient to take home for self-care are separately billable through the DME benefit. This is what CMS Article A55818 from Palmetto GBA refers to when it describes the bundling principle for physician-billed services. You cannot bill A6222 for the dressing you applied before the patient walked out the door—that is the global service. You can bill A6222 for the box of dressings you send home with the patient for daily self-care changes. The documentation must clearly reflect this distinction.
There is also a separate pathway confusion worth addressing: if the patient qualifies for home health services, wound care supplies may be provided through a home health agency as part of the 30-day episode payment, not through Part B DME. Billing DME A-codes when the patient is in an active home health episode is an audit trigger. Verify patient status before billing home supplies.
What About Disposable NPWT Supply Codes?
One supply bundling trap that catches practices regularly: when billing CPT 97607 or 97608 (disposable NPWT), the payment is all-inclusive. Do not separately bill A6550, A7000, or E2402 alongside these codes. Those supplies are embedded in the disposable NPWT payment. Billing them separately is a textbook unbundling violation. Conversely, when billing durable NPWT codes (97605/97606), A-codes for canisters and dressing kits are appropriately billed—but through the DME MAC, not on the same professional claim.
Is Your Practice Losing Revenue on Supply Billing?
Most wound care practices have at least one supply billing gap they haven’t found yet — whether it’s bundled claims that should be separate, missing SWOs, or A-code mismatches. Our billing team identifies exactly where your revenue is leaking.
ICD-10 Coding for Outpatient Wound Claims
ICD-10 coding in wound care is a logic puzzle with real financial consequences. The diagnosis code must mirror the depth of the procedure code, comply with the etiology-first sequencing rule, and appear on your MAC’s LCD Group 1 list—or the claim denies automatically, regardless of how accurate your CPT code was.
Noridian’s LCD L38902 and CMS Article A58565 (Rev 11) together define which diagnosis codes are covered for wound care services. Noridian’s covered list includes over 1,173 diagnosis codes across wound types. Palmetto GBA’s Article A55818 adds additional coding guidance specific to its jurisdiction. Claims with valid ICD-10 codes that do not appear on the MAC’s Group 1 list deny as CO-50 (not medically necessary)—not because the code is wrong, but because it is not covered. This is a critical distinction when building appeals. For a complete ICD-10 to CPT crosswalk, see our wound care billing codes resource.
Diabetic Foot Ulcer — The Mandatory Dual-Code Sequence
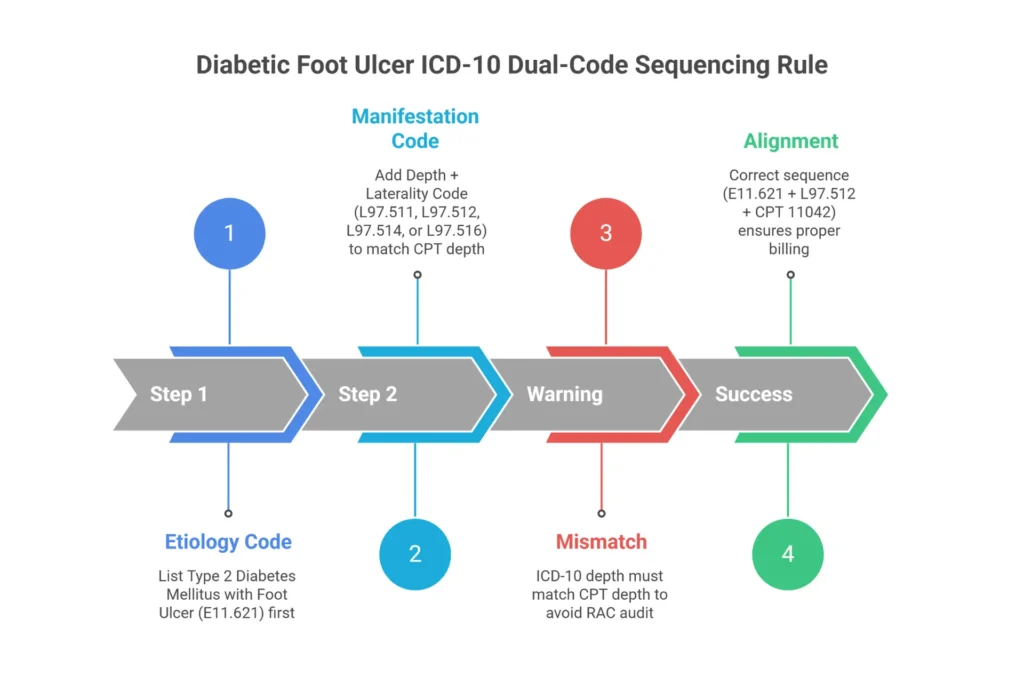
Billing E11.621 (Type 2 diabetes with foot ulcer) alone generates a 40% denial rate in wound care claim audits. E11.621 is the etiology—it tells the payer what caused the wound. It does not specify depth, laterality, or tissue involvement. You must also bill a code from the L97.5xx series to provide that information.
The L97 depth extension system uses a 6th character to describe the tissue layer involved: L97.511 is skin breakdown only; L97.512 is fat layer exposed; L97.513 is fat layer necrosis; L97.514 is bone necrosis; L97.516 is bone involvement without necrosis. The 5th character adds laterality (1 = right foot, 2 = left foot, 3 = right toe, 4 = left toe). This matters because the ICD-10 depth must be consistent with the CPT depth. If L97.512 (fat layer) is on your claim, billing 11044 (bone debridement) creates a conflict that automated systems will flag. The diagnosis says fat layer, the procedure says bone removal—that combination invites a RAC audit and a CO-97 denial.
Correct sequencing: always list E11.621 first (etiology), then the appropriate L97.5xx code (manifestation). Reversing the order is technically incorrect per ICD-10 Official Guidelines and may also trigger denials.
Pressure Injuries — Stage Matters More Than Most Providers Realize
Stage 1 pressure injuries (L89.91x) are not covered for debridement. Stage 1 involves non-blanchable erythema of intact skin—there is no devitalized tissue to debride, so debridement cannot be medically necessary. Billing debridement with a Stage 1 diagnosis will deny as CO-50.
Stages 2 through 4, unstageable injuries, and deep tissue injuries (L89.92x through L89.96x) are covered when properly documented. The ICD-10 code must include the specific anatomic site and laterality—the correct 4th and 5th characters. L89.153 (Stage 3 pressure injury, right sacral area) is very different from L89.91x. Auditors specifically look for mismatched staging, particularly for sacral, hip, and buttock wounds where Stage 2 is frequently documented but debridement codes suggesting deeper tissue involvement are billed.
Post-Surgical Dehiscence — T81.32XA Is Deleted (Critical 2024 Update)
Effective October 1, 2024, ICD-10 code T81.32XA was deleted. Claims submitted with this code after the deletion date auto-reject with a CO-146 denial—not a soft edit, but an automatic rejection. If your EHR still maps post-surgical wound dehiscence to T81.32XA, fix it immediately. The replacement codes are:
- T81.320A — Disruption of wound, deep incisional
- T81.321A — Disruption of wound, superficial incisional
- T81.322A — Disruption of abdominal wound
- T81.329A — Disruption of wound, unspecified
The 7th character A means initial encounter. D is subsequent encounter; S is sequela. Using A on every visit regardless of care phase is also an audit trigger—ensure your encounter designator is accurate.
The Excludes1 Gangrene Trap — I96 vs. Combination Codes
ICD-10 code I96 (gangrene, not elsewhere classified) carries an Excludes1 note that creates a hard-stop denial when billed alongside certain combination codes. If a patient has diabetic gangrene, the correct code is E11.52 (Type 2 DM with diabetic peripheral angiopathy with gangrene)—not E11.621 plus I96. The Excludes1 rule means these codes cannot coexist because the gangrene is already captured in the combination code. Billing both generates a CO-97 denial that many practices attribute to documentation issues when it is actually a coding logic error.
Documentation That Makes Outpatient Wound Claims Pay
If it is not documented with clinical precision, it did not happen—and it will not be paid. CMS Section 1833(e) is explicit: no payment shall be made for services that are not adequately documented. That rule does not bend for clinical complexity, provider tenure, or good intentions.
Wound care documentation failures are the leading cause of CO-97 denials and ADR (Additional Documentation Request) reviews. The CERT program’s ongoing surveillance shows a 25% error rate for wound care specifically, meaning one in four audited claims has a documentation problem serious enough to generate a finding. The OIG Work Plan for 2025–2026 has explicitly identified CPT 11044 (bone debridement) and skin substitute claims as Tier 1 audit targets. This is not the environment in which to be cavalier about note quality.
The 5 Pillars of Wound Documentation
Every wound care note—regardless of complexity, setting, or provider type—must include five core elements that we refer to as the documentation pillars. These are not just good practice; they are what LCD L38902 requires, and they are what MAC reviewers check first during ADR review.
- Location and Laterality: Not “right foot” but “plantar surface, 1st metatarsal head, right foot.” The ICD-10 7th character requires this level of specificity, and auditors cross-reference location against the diagnosis code.
- Measurements: Length × Width × Depth in centimeters. Undermining and tunneling described by the clock method (e.g., “3 cm undermining, 9 to 11 o’clock position”). Surface area calculation in square centimeters to support CPT code selection.
- Tissue Type: Percentage breakdown of granulation, slough, fibrin, and eschar. “Some slough” fails the specificity test. “40% yellow adherent fibrin, 30% friable granulation, 30% periwound hyperkeratosis” passes.
- Exudate: Type (serous, sanguineous, serosanguineous, purulent), amount (scant, small, moderate, large), and color. Exudate documentation also drives HCPCS A-code selection for take-home supplies.
- Periwound Assessment: Erythema, maceration, induration, callus formation, wound edge attachment. This documentation supports medical necessity and vascular assessment for compression coding.
CPT-Specific Documentation Language That Actually Survives Audits
Beyond the 5 pillars, each CPT code requires specific language that demonstrates the service was actually performed at the complexity level being billed. Here are the phrases that matter:
For CPT 97597: “Selective debridement performed via sharp technique using #15 scalpel and tissue forceps. Adherent fibrin and devitalized epidermis removed from 15 sq cm wound surface. Viable tissue margins preserved. Bleeding base confirmed post-debridement.”
For CPT 11042: “Sharp excision of non-viable subcutaneous adipose tissue performed to bleeding margins. 12 sq cm of subcutaneous fat debrided. Non-viable fat identified by dusky color and loss of structural integrity on palpation.”
For CPT 11044: “Cortical bone exposed at wound base. Bone debridement performed with rongeur—non-viable cortical fragments removed to healthy bleeding margins. 8 sq cm bone surface area debrided.” Note: “bone visible” as the only description is insufficient. Auditors are specifically trained to look for whether the note describes bone removal, not just bone exposure.
The 30-Day Rule — Documenting When Healing Stalls
LCD L38902 requires documented evidence of healing progress—specifically, at least 20% wound size reduction or measurable improvement in tissue quality—every 30 days. If your patient is not progressing, the burden falls on documentation to explain why treatment is still medically necessary. “Continued same plan” is the phrase that flags a denial in MAC review.
When healing stalls, the note must demonstrate clinical reasoning: etiology reassessment (was a vascular evaluation performed? is there underlying osteomyelitis?), infection status review, offloading compliance evaluation, or a documented rationale for changing the treatment modality. If you are transitioning a patient to NPWT because debridement alone is not achieving adequate granulation, say exactly that. This narrative is what transforms a stalled-wound note from a denial into a paid claim.
Template cloning—copying the same note forward—is one of the highest-risk documentation practices in wound care. CERT auditors are specifically trained to identify cloned documentation, and pattern-matching software used by RAC contractors flags it algorithmically. Every note should reflect what you actually found on that date, with measurements that differ from the prior visit. Our team offers a wound care billing and coding audit service that includes documentation review before an ADR arrives.
Outpatient Billing Modifiers — The Rules That Prevent Denials
Modifiers are the steering wheel that keeps your claim from crashing into NCCI bundling edits. Miss a required modifier and you get a CO-4 denial. Use the wrong modifier without documentation to back it up and you get a CO-97 denial and an audit flag.
The NCCI (National Correct Coding Initiative) Chapter 4G governs the integumentary system, and its bundling rules for wound care are specific and unforgiving. As of Version 28.3 effective January 1, 2026, the procedure-to-procedure (PTP) edits for wound care include several Indicator 0 pairs (mutually exclusive—never separately billable) and Indicator 1 pairs (separately billable with appropriate modifier and documentation). Knowing which is which prevents the majority of preventable wound care denials. Our complete guide to wound care billing codes includes the full NCCI edit matrix for common code pairs.
Modifier 25 — When Same-Day E/M Is Separately Billable
The OIG estimates that 35–40% of wound care modifier 25 claims are insufficiently documented. That is not a small problem when you consider that modifier 25 likely appears on a substantial portion of your wound care claims. The standard is clear: modifier 25 is for a significant, separately identifiable evaluation and management service above and beyond the pre-procedural assessment of the wound being treated. If the only reason you evaluated the patient was to assess the wound before debridement, modifier 25 does not apply—that assessment is inherent to the procedure.
Where modifier 25 is legitimate: the provider assessed spreading cellulitis and adjusted antibiotic therapy; the provider managed uncontrolled diabetes complicating wound healing with medication changes; the provider reviewed new lab results showing worsening renal function relevant to a systemic infection. These are separately identifiable E/M services. The note must document the MDM or time for that E/M portion independently from the procedure documentation.
Can 29580 and 11042 Be Billed Together?
No—not on the same limb. NCCI Chapter 4G treats the compression wrap (CPT 29580, Unna boot) as the dressing for the debridement when both are performed on the same extremity on the same day. The Indicator 1 edit means they could theoretically be separated with a modifier, but the documentation must support that the services were performed on different anatomic structures—not just different locations on the same leg. The practical rule: if you debrided the right foot and applied an Unna boot to the right ankle on the same visit, 29580 will deny with CO-97. If you debrided the right foot and applied an Unna boot to the left ankle during the same encounter, use modifier XS (separate structure) to identify the different laterality. Same-limb compression and debridement are bundled. Cross-limb is separately billable with XS.
Can You Bill 11043 and 97605 Together?
Yes—these represent sequential services on the same wound and NCCI does not bundle them. CPT 11043 (muscle/fascia debridement) prepares the wound bed; CPT 97605 (NPWT application, ≤50 sq cm) promotes healing afterward. The NCCI Indicator is 1, meaning separate billing is allowed, and in most cases no modifier is required as long as documentation clearly describes both the debridement and the NPWT as distinct clinical interventions. Your note should state: “Post-debridement, NPWT initiated at 125 mmHg continuous pressure, 50cc canister drainage” or similar language that makes the sequential nature of the treatment explicit. Document the initiation parameters for NPWT separately from the debridement narrative.
X-Modifiers, Modifier 59, RT/LT, and Digit Codes
CMS introduced the X-modifier family to replace the overuse of modifier 59, which became the modifier of last resort in wound care billing. The hierarchy is: use XS (separate structure) when the services are on different anatomic sites; XE (separate encounter) when services occurred at different times during the day; XP (separate practitioner) when the services were rendered by different providers; XU (unusual non-overlapping service) for scenarios that don’t fit the other three categories. Only use modifier 59 when none of the four X-modifiers accurately describes the situation. Excessive modifier 59 use is itself an audit flag.
For laterality, RT and LT modifiers are required on every limb-based procedure. Missing RT or LT on a code like 11042 generates a CO-16 denial for missing information—an easily preventable error. For toe-specific procedures, the digit modifiers T1 through T9 (and TA for the great toe) must be used to identify the specific digit treated. Payers will not accept a claim for bilateral toe debridement without digit-level specificity.
Does Medicare Cover Outpatient Wound Care? Rules, Limits, and Supplies
Yes—Medicare Part B covers outpatient wound care when it is medically necessary. But “medically necessary” in Medicare means meeting specific documented criteria, not simply that your patient has a wound that needs treatment.
This distinction matters because practices routinely assume that if a wound exists and care is provided, Medicare will pay. That assumption creates most of the CO-97 denials in wound care billing. Coverage exists within a framework of rules—a 30-day conservative care trial, measurable improvement benchmarks, frequency limits, and diagnosis requirements. Understanding those rules is the difference between a paid claim and an 18-month appeals cycle. For deeper Medicare-specific guidance, see our dedicated Medicare wound care billing guide.
Part B Coverage — What Pays and What Doesn’t
Medicare Part B covers debridement (when properly documented), NPWT, skin substitutes (up to 8 applications per 16-week period), compression therapy for venous ulcers with documented I87.31x diagnoses, and hyperbaric oxygen therapy for Wagner Grade 3 or higher diabetic foot ulcers under NCD 20.29. Medicare pays 80% of the approved amount after the annual Part B deductible ($257 in 2026). Your patient is responsible for 20% coinsurance.
What Medicare does not cover: non-selective debridement in the physician office (97602, Status B), Stage 1 pressure injuries (no devitalized tissue), routine wound care during a global surgical period, supplies used during an office procedure (bundled), and skin substitutes applied before a 30-day trial of standard care failure is documented. These are not gray areas—they are hard coverage exclusions, and billing them creates both denial exposure and potential overpayment liability.
The 12/360 Rule and ABN Requirements
Medicare limits specialized surgical debridement (CPT codes 11042–11047) to 12 sessions per rolling 360-day period. This is a frequency hard stop, not a soft limit. When a patient reaches their 13th session, that claim denies automatically. If the 13th debridement is clinically necessary—documented exceptional circumstances, wound not responsive to standard frequency—you have two obligations: document the exceptional circumstances clearly in the note and append modifier KX to signal to Medicare that the requirements are met but the frequency limit is exceeded.
Equally important: if you believe Medicare is likely to deny a claim, you must issue an Advance Beneficiary Notice (ABN) using Form CMS-R-131 before the service. Without a signed ABN on file, you cannot bill the patient when Medicare denies. The modifier GA indicates an ABN is on file; GZ indicates you expect a denial but do not have an ABN (meaning you cannot bill the patient—a significant financial exposure). GY indicates the service is statutorily non-covered and the patient can be billed only with a signed ABN.
Does Medicare Cover Wound Care Supplies at Home?
Yes—home wound care supplies are covered under the Part B DME benefit at 80% after the deductible. Dressings, gauze, hydrocolloids, foam, alginate, and NPWT equipment for home use are all coverable with a valid Standard Written Order and appropriate documentation of wound size and exudate level. Simple dressing changes at home for stable wounds without a skilled need are considered self-care and are not covered as nursing services—they are supplies-only claims through a DME supplier, not skilled visits. This distinction matters particularly for patients on home health orders who may have supply coverage through the home health benefit rather than DME Part B.
Outpatient Graft Billing — Skin Substitutes Under the 2026 CMS Flat Rate
The era of profit-by-product-selection ended January 1, 2026. CMS finalized a flat rate of $127.14 per square centimeter for most outpatient skin substitutes in the CY 2026 Physician Fee Schedule Final Rule, and the financial math has fundamentally changed for every practice that uses grafts.
Before this change, skin substitute reimbursement was calculated as ASP+6% (Average Sales Price plus 6%)—a model that directly incentivized the use of expensive products because higher-cost grafts generated higher reimbursement. CMS’s OIG Data Brief (OEI-03-23-00460) identified this as a driver of $19.6 billion in projected unnecessary spending, and the flat rate eliminates that dynamic entirely. Under the new model, whether you use a $50/sq cm synthetic or a $400/sq cm amniotic membrane product, Medicare pays the same $127.14 per sq cm applied. The only exception: Section 351 licensed biologics under PHSA retain the ASP+6% model.

What the $127.14 Flat Rate Means for Your Practice in Practice
The math is direct: if your acquisition cost exceeds $127.14 per sq cm, you lose money on every application. Many premium amniotic membrane allografts (361 HCT/P products) that previously generated substantial revenue under ASP+6% now represent a net loss unless renegotiated to acquisition costs below the flat rate threshold. 510(k) cleared synthetic matrices and PMA-approved products that already had low acquisition costs are now margin-positive. Formulary selection is no longer a clinical preference alone—it is a revenue cycle decision.
Additionally, the flat rate applies only to the administered portion. Discarded graft material is not reimbursable. This creates a practical incentive toward smaller, more precisely-sized grafts and careful pre-application measurement. Documenting the exact square centimeters applied—separate from the total graft size—is critical for both reimbursement accuracy and audit defense.
Q41xx Codes and the CPT 15271–15278 Billing Workflow
Skin substitute claims require two code types on the same claim: the product-specific HCPCS Q41xx code identifying the graft product, and the application CPT code (15271–15278) reflecting the anatomic site and square centimeters applied. CPT 15271 is the primary code for trunk, arms, and legs, first 100 sq cm in adults; 15272 is the add-on for each additional 100 sq cm. 15275 covers face, scalp, neck, and ears; pediatric codes 15273/15274 and 15277/15278 apply to patients under 10 years old. Pair the exact Q41xx code for the product you used (e.g., Q4100 for Dermagraft, Q4116 for Alloderm) with the appropriate anatomic application code. For newly authorized products without a specific Q-code, Q4431–Q4433 are the 2026 unlisted codes.
Prior Authorization and Q-Code Mismatch Prevention
Medicare Advantage plans require prior authorization for approximately 90% of skin substitute applications. Submit prior authorization requests with a 30-day history of conservative care failure, Wagner Grade documentation for DFU, ABI or TCOM vascular study results, and offloading compliance records. For traditional Medicare, the documentation requirements are the same—they just do not require pre-authorization before the service.
Q-code mismatch is the #1 RAC audit trigger in 2026 skin substitute billing. When the Q-code on the claim does not match the FDA classification of the product documented in the chart—or when the chart does not document which specific product was used—the result is a PR-96 denial and a chart request. The Order-to-Vial-to-Claim verification workflow eliminates this risk: document the exact product lot number in the note, confirm the corresponding Q-code before claim submission, and retain the product verification documentation in the patient file.
Elite Med Financials Verified Graft Program
We built our Verified Graft Program specifically for the 2026 flat-rate environment. Every product in our formulary is priced for margin-positive reimbursement below the $127.14/sq cm threshold, and we source authorized DermaBind TL and FM products through NovaMed — synthetic matrices designed for the new payment model.
Our 3-Step IVR Verification confirms Q-code accuracy before any claim goes out — eliminating the mismatch risk that triggers RAC review. If you are currently using expensive amniotics under the flat rate and losing money per application, this is worth a conversation.
Explore Verified Graft Products →Why Outpatient Wound Care Claims Get Denied — And How to Fix Each One
Wound care denial rates run 2–3 times higher than average Medicare Part B services. That gap is not random—it is the predictable result of code-specific complexity meeting documentation gaps. Here are the denial patterns we see most and exactly how to address them.
Before diving into specific denial codes, understand the financial context: the CERT error rate for wound care is approximately 25%, and the average administrative cost to work a single denied claim has risen to about $25–$30 in 2026 with increased documentation complexity. Multiply that by denial volume across a busy wound clinic and the ROI of denial prevention over denial management becomes clear. Our wound care billing FAQ covers common denial questions in detail, and our denial management service is available through our RCM services page.
CO-97 — Medical Necessity Documentation Failures
CO-97 accounts for 35–40% of all wound care denials and indicates that the service was not considered medically necessary based on the documentation submitted. Common root causes: billing debridement without a complete 5-pillar note, submitting E11.621 without the companion L97.5xx depth code, cloned notes that do not show clinical progression between visits, and failure to document the 30-day conservative care failure that justifies advanced wound care.
The fix for an existing CO-97 denial is a Level 1 Redetermination submitted within 120 days of the denial date. Compile a complete bundle: all clinical notes from the current episode of care with serial wound measurements, photographs showing wound progression, the original diagnosis documentation, and a cover letter that explicitly cites LCD L38902 Group 1 ICD codes and documents the 30-day standard care failure. Level 1 Redeterminations with a complete documentation bundle succeed at a 60–70% rate with MAC contractors. Do not submit a bare appeal letter—the bundle is what wins.
The 97602 Status B Error — A Silent Revenue Killer
Pull a report from your practice management system: filter claims by CPT 97602, POS 11, and paid amount $0.00. If you see results—and in most practices that bill wound care, you will—those are paid claims where your providers worked for free. The 97602 Status B issue is invisible in day-to-day operations because the claim processes, the EOB shows $0 reimbursed, and nobody catches it unless someone is specifically looking.
The fix is education, not appeals. You cannot appeal a Status B denial for 97602 in POS 11—the policy is clear. The solution is clinical documentation training: providers need to understand that if they performed selective debridement (any technique involving scalpel, scissors, curette, or forceps to target specific tissue), that should be documented as 97597, not 97602. If the debridement was truly non-selective, the service either accepts the bundling or is performed in a facility setting.
NCCI Bundling Violations — Indicator 0 vs. Indicator 1
Billing CPT 97597 and 11042 on the same wound on the same day is an NCCI Indicator 0 edit—these codes are mutually exclusive. You chose the technique: selective active wound management (97597) or surgical subcutaneous excision (11042). Bill the one that matches the depth and technique documented. Billing 97597 and 97598 for selective debridement alongside 11042 for the same wound results in denial of both and a potential unbundling audit flag.
The 29580 and 11042 same-limb bundling is an Indicator 1 edit—separately payable with documentation of different anatomic sites and modifier XS. Same limb, same day, without XS: 29580 denies with CO-97. Different limbs with XS documented: both pay. The solution is systematic: build the XS-on-compression rule into your billing workflow so it applies automatically when different-limb scenarios occur.
Frequency Limit Exceedances — The 12/360 Hard Stop
The 13th debridement in a 360-day rolling period is an automatic denial. Track your debridement counts by patient. If a wound is not healing at the expected rate, that is a clinical signal—assess for osteomyelitis, vascular insufficiency, or inadequate offloading. If the 13th visit is genuinely necessary, document the exceptional circumstances, append modifier KX, and have a signed ABN on file with modifier GA on the claim. Without the ABN, you cannot collect from the patient when Medicare denies, making that service a complete write-off.
🗂️ 10-Point Pre-Submission Wound Care Billing Checklist
Check every item before submitting any outpatient wound care claim.
- POS code verified — Confirm POS 11/22/31 matches actual care setting. CPT 11043 and 11044 require facility (POS 22) — billing in POS 11 generates automatic denial.
- 97602 not billed in POS 11 — CPT 97602 is Status B in office setting = $0.00 reimbursed. If selective technique was used, bill 97597 with documentation of sharp debridement.
- 5 Pillars documented — Location with laterality, measurements (L×W×D cm), tissue type percentages, exudate type/amount, periwound condition — all present in the clinical note.
- ICD-10 dual-code sequence correct — E11.621 paired with appropriate L97.5xx depth code; etiology (E11.621) listed FIRST, manifestation (L97.5xx) second. Solo E11.621 = 40% denial rate.
- Diagnosis on LCD L38902 Group 1 list — Confirm ICD-10 code appears on your MAC’s Group 1 covered diagnoses. Valid codes not on the list deny as CO-50 (not medically necessary).
- RT/LT modifier on all limb codes — Every extremity-based procedure requires a laterality modifier. Missing RT or LT triggers CO-16 denial — one of the most preventable errors in wound care billing.
- NCCI bundling check completed — Verified 29580 and 11042 are NOT on same limb without XS modifier. Confirmed 97597 and 11042 are NOT billed on the same wound (Indicator 0 = mutually exclusive).
- 12/360 debridement count verified — Confirm this is not the 13th debridement in a 360-day rolling period. If it is: ABN signed (CMS-R-131), modifier KX appended, exceptional circumstances documented.
- Skin substitute: Q-code matches product in chart — Product lot number documented in the note. HCPCS Q41xx code confirmed against the exact product used. Q-code mismatch = #1 RAC audit trigger in 2026.
- Modifier 25 documentation is separate — If billing E/M with a procedure, the note documents a separately identifiable MDM beyond the wound assessment that preceded the procedure.
📋 Source: Elite Med Financials — Wound Care Billing Guidelines 2026
Voice Search Q&A — Wound Care Billing Questions Answered Simply
The following questions represent the most common voice and natural-language searches about outpatient wound care billing. We’ve structured each answer to be clear, direct, and complete for both conversational searches and AI assistant queries.
Why is my 97602 showing $0.00 paid even though the claim processed?
CPT 97602 carries a Status B indicator on the Medicare Physician Fee Schedule. In Place of Service 11 (physician office), Status B means the code is bundled into the evaluation and management service and pays zero dollars. The claim processes—it is not rejected—but Medicare considers the non-selective debridement to be included in the office visit payment. The fix: if the debridement used sharp selective technique (scalpel, scissors, forceps), document it as such and bill CPT 97597 instead. If it was truly non-selective (wet-to-dry, enzymatic), the service only generates separate payment in a facility setting.
Why can’t I bill CPT 11043 in my private practice office?
CPT 11043 (muscle and fascia debridement) is a facility-only code. Billing it with Place of Service 11 generates a denial because Medicare’s Physician Fee Schedule does not support payment for this code in a non-facility setting. The clinical rationale: muscle and fascia debridement requires the infrastructure, sterile field, and infection control resources of a hospital outpatient department or ambulatory surgical center. To bill 11043 and be paid, the procedure must occur in POS 22 (hospital outpatient) or equivalent facility setting, where the hospital also collects a facility fee that covers those overhead requirements.
Can I bill for wound care dressings and gauze I used during a procedure?
No. Supplies used during a wound care procedure in your office—dressings applied post-debridement, gauze used during the procedure itself, topicals applied at the time of the visit—are bundled into the CPT code payment. Medicare does not separately reimburse for those supplies. What you can bill separately are take-home supplies dispensed to the patient for self-care between visits. Those are billable under the Part B DME benefit using the appropriate HCPCS A-codes, with a signed Standard Written Order on file and documentation of wound size, exudate level, and change frequency.
How does the 2026 skin substitute flat rate change what my practice needs to do?
Effective January 1, 2026, most outpatient skin substitutes reimburse at a flat rate of $127.14 per square centimeter, regardless of the product’s actual cost. Previously, reimbursement was based on Average Sales Price plus 6%, which meant expensive products generated higher payments. Under the flat rate, if your acquisition cost exceeds $127.14 per sq cm, you lose money on every application. The change requires practices to audit their current graft formulary, renegotiate supplier pricing or switch products, and verify that Q-codes on claims precisely match the products documented in the patient chart. Formulary selection is now an RCM decision, not just a clinical preference.
What happens when a patient hits 12 debridements in 360 days — is the 13th automatically denied?
Yes — Medicare’s 12/360 rule limits specialized debridement (CPT 11042–11047) to 12 sessions per rolling 360-day period. The 13th session denies automatically as exceeding frequency limits. However, if the additional debridement is medically necessary, you have options: document exceptional clinical circumstances in the note, append modifier KX to the claim to signal that the frequency limit is exceeded but the service is medically necessary, and have a signed Advance Beneficiary Notice (ABN using Form CMS-R-131) on file with modifier GA on the claim. Without the ABN, you cannot bill the patient when Medicare denies.
My EHR still maps post-surgical wound dehiscence to T81.32XA — is that causing my claims to reject?
Yes. ICD-10 code T81.32XA was deleted effective October 1, 2024. Claims submitted with the old code after that date automatically reject with a CO-146 denial. The replacement codes are T81.320A (deep incisional disruption), T81.321A (superficial incisional disruption), T81.322A (abdominal wound disruption), and T81.329A (unspecified disruption). Update your EHR code mapping immediately. Any claims rejected since October 2024 for this reason should be corrected and resubmitted—the denials are reversible once the correct code is applied, within your payer’s resubmission timelines.
How specific does my wound documentation need to be to pass a MAC audit?
Significantly more specific than most providers document in their standard notes. MAC auditors during ADR review specifically look for five elements: a precise wound location with laterality (not “right foot” but “plantar surface, 1st metatarsal head, right foot”); measurements in centimeters (L×W×D); tissue type percentages (percentage of granulation, slough, fibrin, eschar); exudate characterization (type, amount, color); and periwound assessment. Beyond those pillars, the note must include language that demonstrates the specific procedure performed—”excisional debridement to bleeding subcutaneous margins” for 11042, or “tangential bone debridement with rongeur” for 11044. Generic language like “wound cleansed and debrided” does not support procedure-level billing.
Frequently Asked Questions About Outpatient Wound Care Billing
How do you bill for wound care services?
Billing for wound care services requires a precise three-step process. First, document the five clinical pillars — location with laterality, wound measurements in centimeters, tissue type percentages, exudate characteristics, and periwound condition — to establish medical necessity. Second, select the correct CPT code based on the deepest tissue removed: CPT 97597 for selective debridement of surface tissue, 11042 for subcutaneous tissue, 11043 for muscle/fascia (facility only), and 11044 for bone (facility only). Third, apply the appropriate modifiers — RT/LT for all limb procedures, XS for multiple wounds, and modifier 25 only if a separately identifiable E/M service was performed beyond the pre-procedure wound assessment. Always pair debridement codes with an ICD-10 code that specifies wound depth and etiology, and confirm the diagnosis appears on your MAC’s LCD covered list.
Is wound care considered outpatient?
Yes, wound care is primarily classified as an outpatient service when performed in a physician’s office (POS 11), hospital outpatient department (POS 22), or skilled nursing facility (POS 31). Outpatient wound care encompasses chronic wound management — diabetic foot ulcers, venous stasis ulcers, pressure injuries, and post-surgical dehiscence — that does not require an overnight inpatient stay. The distinction is based on patient status, not the setting itself: observation status patients are still considered outpatient even if they are in a hospital bed. Outpatient services bill under Medicare Part B using either the Physician Fee Schedule or OPPS, while inpatient wound care during a hospitalization is bundled into the DRG payment and not separately billable by the physician.
What is the difference between CPT 97606 and 97608?
The difference between CPT 97606 and 97608 is the equipment type, not the wound type. CPT 97606 is for durable (reusable) NPWT pumps applied to wounds larger than 50 square centimeters — under this code, the clinic bills only for the professional service component, and a DME supplier separately bills for the pump and supplies. CPT 97608 is for disposable (single-use) NPWT devices on wounds larger than 50 square centimeters — this is an all-inclusive code covering both the professional service and the device. Do not bill separate supply codes such as A6550 or A7000 alongside 97607 or 97608, as this constitutes unbundling and triggers automatic audit. The 2026 reimbursement for 97607 is approximately $300; for 97608, approximately $400.
Can you bill 11043 and 97605 together?
Yes — CPT 11043 (muscle and fascia debridement) and CPT 97605 (NPWT application, up to 50 sq cm) can be billed together on the same wound on the same day. NCCI does not bundle these codes because they represent two distinct sequential treatments: debridement prepares the wound bed, and NPWT promotes healing afterward. No modifier is typically required, as NCCI assigns these codes Indicator 1, meaning separate billing is allowed when documentation supports separate services. The clinical note must clearly describe both interventions independently — the debridement including depth reached and tissue excised, and the NPWT initiation including device type, pressure setting such as 125 mmHg continuous, and canister placement. Sequential documentation is what protects this code combination from audit.
Are wound care supplies covered by Medicare?
Medicare Part B covers wound care supplies under two distinct pathways with very different rules. Supplies dispensed to patients for home self-care are covered at 80% after the annual deductible through the DME benefit, using HCPCS A-codes in the A6196 through A6235 range for dressings, with a valid Standard Written Order. However, supplies used during an in-office wound care procedure are bundled into the CPT code payment and not separately reimbursable — billing A-codes for in-office procedural supplies constitutes unbundling. Skin substitutes are covered under a separate framework, now at a flat rate of $127.14 per square centimeter for most products effective January 2026. The Standard Written Order must specify the exact HCPCS code, quantity, and change frequency before supplies are dispensed to the patient.
How to get wound care supplies covered by insurance?
To get wound care supplies covered, follow three steps. Step one: obtain a Standard Written Order signed by the treating physician specifying the patient’s name, Medicare ID, the exact HCPCS code such as A6222 for impregnated gauze, quantity, change frequency, and the prescriber’s NPI and signature. The SWO must exist before supplies are dispensed — backdating is not permitted. Step two: document medical necessity in the clinical note including wound measurements in centimeters, exudate level, and tissue type, and select a dressing type that clinically matches the wound’s drainage needs. Step three: submit the claim through a licensed DME supplier using the HCPCS A-code on a CMS-1500 form. Medicare pays 80% after the deductible. For Medicare Advantage plans, verify prior authorization requirements before dispensing. Without a complete SWO, the claim receives a CO-96 denial that cannot be appealed without first obtaining the order.
What are the five rules of wound care billing?
The five foundational rules of wound care billing are as follows. Rule one: document the deepest tissue layer actually removed, not what was visible — if subcutaneous fat was excised, bill 11042; if bone was removed in a facility, bill 11044. Rule two: bill the deepest wound first when treating multiple wounds on the same day, sequencing by complexity. Rule three: sum the square centimeters of wounds at the same tissue depth and use add-on codes rather than billing a separate primary code per wound. Rule four: use RT/LT modifiers on every limb procedure and XS for separate anatomic sites to prevent CO-16 and NCCI bundling denials. Rule five: always link diagnosis etiology to manifestation — pair E11.621 for diabetes with L97.5xx for the specific depth of the foot ulcer, and always sequence the etiology code first.
How much does outpatient wound care cost with Medicare?
For Medicare beneficiaries, outpatient wound care costs approximately 20% of the Medicare-approved amount after the 2026 annual Part B deductible of $257. A subcutaneous debridement session using CPT 11042 with an approved amount of approximately $250 would cost the patient around $50 in coinsurance. For skin substitutes under the 2026 flat rate of $127.14 per square centimeter, the patient’s coinsurance share is approximately $25.43 per square centimeter applied. NPWT sessions range from approximately $150 to $400 in approved amounts, placing patient coinsurance at $30 to $80 per session. Patients with Medicare Supplement or Medigap plans typically have their 20% coinsurance covered. Medicare Advantage plans may have different cost-sharing structures and may require prior authorization, which can affect both timing and patient out-of-pocket costs.
Conclusion: What 2026 Actually Requires From Your Billing Operation
Outpatient wound care billing in 2026 is not harder than it used to be—it is more precisely defined. CMS has not made the rules more complex so much as it has made the enforcement more systematic. Automated edits catch POS violations. RAC contractors run pattern analysis on depth documentation vs. CPT code selection. The flat-rate skin substitute model has eliminated the margin for error on formulary selection. And the CERT program continues to identify documentation failures at nearly three times the Medicare average.
What this means practically: the practices that do well in 2026 are those with disciplined claim workflows, CPT-specific documentation language, and a clear understanding of which codes pay in which settings. They are not necessarily the practices with the most complex clinical protocols—they are the ones whose billing operation is as systematic as their clinical care. The 97602 Status B error, the T81.32XA deletion, the 12/360 frequency cap—these are all correctable problems. The question is whether you find them on your own terms or on an auditor’s.
If you are seeing denial rates above 10%, zero-dollar paid claims on debridement codes, or inconsistency between your ICD-10 codes and CPT depth documentation, those are signals worth acting on. Our team specializes in exactly these scenarios. We do not offer generic billing services—we offer wound care billing specifically, and we understand the difference between a 97597 note that pays and one that triggers an ADR.
Ready to Fix Your Outpatient Wound Care Billing?
Our wound care billing team has submitted these exact claims, survived these audits, and built the workflows that prevent the denials in this guide. We specialize in wound care billing specifically — not general billing that happens to include wound codes. Let us do that for your practice so you can focus on patients, not paperwork.

