How to Start NEMT Billing: Complete Setup Guide for New Providers (2026)
Table of Contents
Starting an NEMT billing operation feels overwhelming when you’re staring at a blank slate. You’ve got vehicles, drivers, and patients ready to transport—but the money won’t flow until claims start getting paid. And that process? It’s where most new providers stumble.
The typical NEMT provider spends 90 to 180 days getting their billing infrastructure operational. Some stretch past a year because they didn’t understand what was required upfront. Meanwhile, completed trips sit unbilled, cash reserves drain, and frustration mounts.
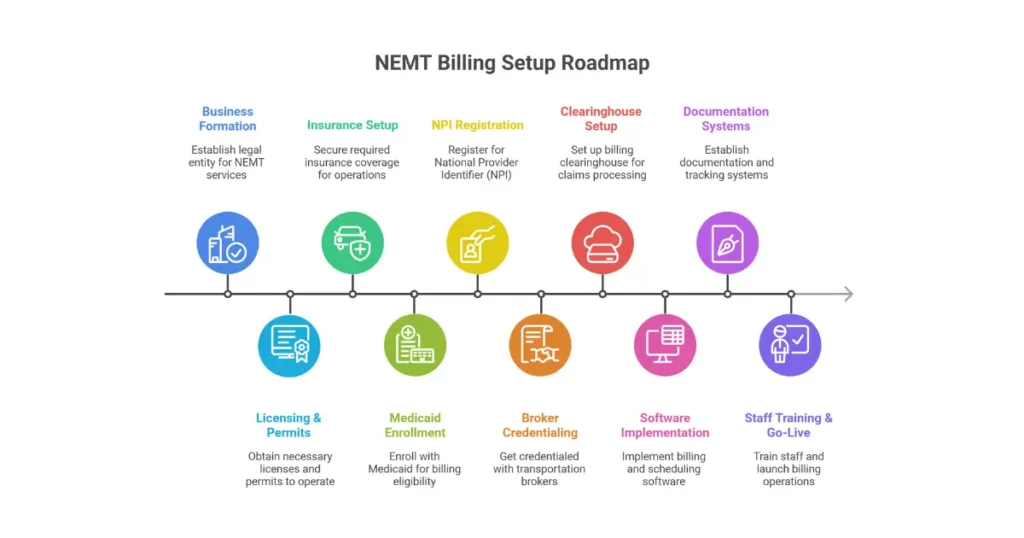
This guide walks through every step of NEMT billing setup—from forming your business entity through submitting your first clean claim. We’ve structured it around the actual sequence you’ll follow, with realistic timelines and costs at each phase. Whether you’re launching a single-van operation or scaling a multi-state fleet, you’ll find the specifics you need here.
For providers already billing but struggling with rejections, our NEMT denial codes guide covers resolution strategies in detail. This article focuses on getting your foundation right from day one.
Understanding NEMT Billing {#understanding-nemt-billing}
Before diving into setup steps, let’s clarify what NEMT billing actually involves and how it differs from what you might expect.
What Is NEMT Billing?
NEMT billing is the process of converting completed non-emergency medical transportation trips into compliant claims for reimbursement. Unlike standard medical billing that focuses on clinical diagnoses and procedures, NEMT billing centers entirely on transportation logistics and trip validation.
The billing cycle includes eligibility verification, prior authorization management, trip documentation, HCPCS coding, electronic claim submission through EDI 837P transactions, adjudication monitoring, payment posting, and denial management. Every trip generates a potential claim—but only properly documented, correctly coded, timely-filed claims actually get paid.
Covered services typically include ambulatory transport (patients who can walk), wheelchair van transport, stretcher transport, and mobility-assisted transport for scheduled medical appointments. Reimbursement depends on loaded mileage, trip type, vehicle classification, and documented medical necessity—not clinical treatment outcomes.
How NEMT Billing Differs from Medical Billing
The distinction matters because providers who approach NEMT billing like traditional medical billing run into problems immediately.
Focus and documentation diverge significantly. Medical billing relies on clinical notes, physician documentation, and diagnosis codes tied to treatment. NEMT billing requires GPS logs, timestamps, mileage verification, driver attestation, vehicle identification, and patient signatures. Your documentation proves the trip happened as claimed—nothing clinical about it.
Coding systems differ too. Medical billing uses CPT codes for procedures and ICD-10 codes for diagnoses. NEMT uses HCPCS Level II transport codes (A0130, A0425, S0215) paired with origin and destination modifiers. Get the modifier wrong, and the claim denies regardless of trip completion.
Risk profiles vary considerably. NEMT claims fail without medical necessity proof or timely submission even when the trip actually occurred. The service is non-clinical, but compliance requirements rival clinical billing in complexity.
How Do NEMT Companies Get Paid?
Revenue flows through four primary channels, each with distinct payment timelines and requirements:
Medicaid Fee-for-Service pays directly from state Medicaid agencies. You submit claims via EDI 837P after trip completion, with reimbursement based on base rate plus loaded mileage. Payment typically arrives within 30 to 90 days, with strict timely filing limits ranging from 90 to 365 days depending on state. Check our state-by-state Medicaid NEMT rates guide for specific reimbursement amounts.
Broker-Managed Medicaid routes through intermediaries like ModivCare, MTM, Veyo, and Access2Care. These brokers contract with states to manage transportation benefits, then subcontract with providers like you. Claims go through broker portals after GPS and electronic proof of delivery verification, with payment typically arriving in 15 to 30 days—faster than direct Medicaid. High-volume providers can negotiate rates 10 to 25 percent above standard schedules.
Medicare Advantage covers NEMT as a supplemental benefit under Part C plans. Coverage varies by plan, county, and annual trip limits. Traditional Medicare does not routinely cover NEMT, making this channel plan-specific. Payment arrives within 14 to 30 days when coverage applies.
Private Pay involves direct billing to patients, families, dialysis centers, nursing homes, and facilities. No prior authorization required, payment methods include credit card, ACH, cash, and checks, and rates run 2 to 3 times higher than Medicaid. Payment timeline ranges from same-day to seven days.
Timeline and Cost Overview
Setting realistic expectations prevents the cash-flow crises that sink new operations.
Total setup time ranges from 90 days minimum to 12 months maximum. Broker-friendly states with parallel processing can hit the low end. States with complex Medicaid enrollment like California can stretch toward a year. The 2025-2026 CMS PAVE screening updates added 30 to 60 days to most state reviews.
CMS mandates “high-risk” screening for NEMT providers, meaning more documentation and longer review periods than lower-risk provider categories. The 2025-2026 PAVE (Provider Application and Validation for Enrollment) updates added screening layers that extend timelines. For official enrollment requirements and screening protocols, refer to the CMS Provider Enrollment and Certification guidelines.
Billing-focused startup costs run $5,000 to $25,000 excluding vehicles, fleet equipment, and insurance. Small single-state operations land around $5,000 to $15,000. Multi-broker, multi-state setups push $15,000 to $25,000. These figures cover enrollment fees, credentialing costs, software implementation, clearinghouse setup, and initial staff training—not ongoing operational expenses.
| Setup Phase | Timeline | Cost Range |
|---|---|---|
| Business formation | 1-2 weeks | $50-$500 |
| Medicaid enrollment | 60-180 days | $2,500-$5,500 |
| Broker credentialing | 30-90 days per broker | $500-$2,000 per broker |
| Clearinghouse/EDI setup | 1-4 weeks | $500-$2,000 |
| Software implementation | 4-12 weeks | $1,000-$10,000 |
Prerequisites Before You Start {#prerequisites}
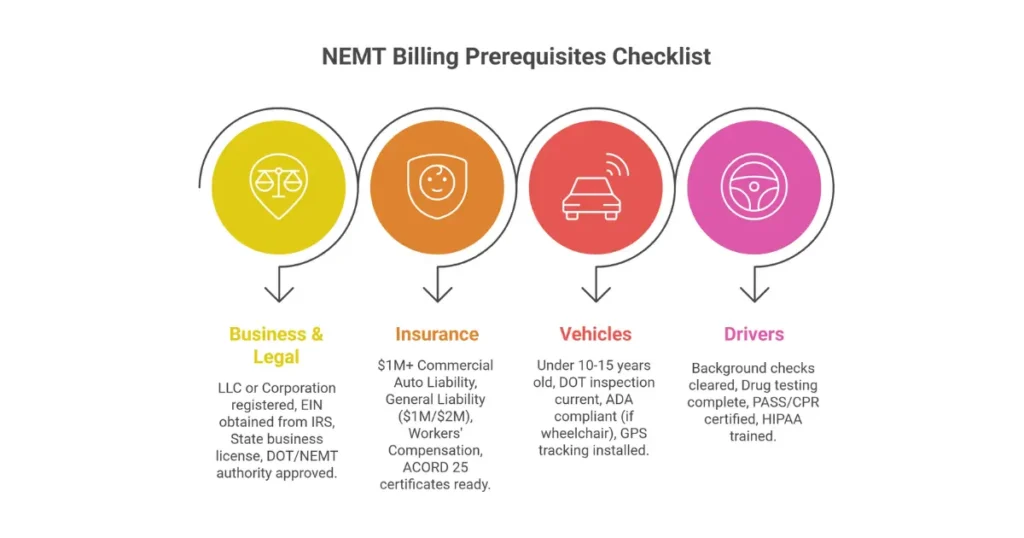
Rushing into Medicaid enrollment without prerequisites in place guarantees rejection. State agencies and brokers verify compliance before approving providers—missing any requirement delays everything.
Business Entity Requirements
LLC (Limited Liability Company) is the recommended structure for NEMT providers, chosen by approximately 80 percent of new operations. The preference stems from personal asset protection against passenger injury and accident lawsuits, pass-through taxation simplicity, and lower administrative burden than corporations.
| Entity Type | NEMT Advantages | Key Limitations | Setup Timeline |
|---|---|---|---|
| Sole Proprietorship | Fast, no formation cost | Unlimited personal liability | 1 day |
| LLC | Liability shield, tax flexibility | $100-$800 state fees | 1-2 weeks |
| Corporation (S/C) | Investor-ready, credibility | Annual filings, higher costs | 2-4 weeks |
Mandatory registrations include:
- EIN (Employer Identification Number) from IRS—free, instant, required for banking, payroll, Medicaid enrollment, and broker credentialing
- State business registration through Secretary of State
- Local business licenses varying by county and city
NEMT Licensing by State
State-level licensing requirements vary dramatically. Plan for these timelines:
| State | Licensing Authority | Fee | Timeline |
|---|---|---|---|
| California | CPUC PSC Permit | $1,500+ | 90-180 days |
| Texas | TxDMV Carrier Authority | $200 | 30-60 days |
| New York | TLC Medallion/Para-Transit | $500+ | 60-120 days |
| Florida | HSMV Carrier Permit | $300 | ~45 days |
| Illinois | IDOT Vehicle Base Permit | $500 | 30-90 days |
Most states require DOT authority (federal and/or intrastate) before NEMT licensing approval. Operating permits tie to vehicle class and service level. California’s CPUC requirement alone can add six months to your timeline.
Insurance Requirements
Brokers and Medicaid agencies verify insurance before credentialing approval. Minimum coverage levels for 2025-2026:
| Coverage Type | Minimum Required | Typical Annual Cost |
|---|---|---|
| Commercial Auto Liability | $1M CSL (CA requires $1.5M+) | $8,000-$20,000 per vehicle |
| General Liability | $1M per occurrence / $2M aggregate | $1,500-$4,000 per fleet |
| Workers’ Compensation | State-mandated | $3,000-$10,000 (3-5 drivers) |
| Professional Liability (E&O) | $1M recommended | $800-$2,500 |
| Umbrella/Excess | $1M-$5M | $2,000-$6,000 |
ACORD 25 certificates must name the Medicaid agency and each broker (ModivCare, MTM, etc.) as additional insured with 30-day cancellation notice required.
Vehicle Specifications
Medicaid and broker standards for vehicles include:
- Model year within 10-15 years
- Mileage under 150,000-200,000 miles
- Annual DOT safety inspection current
- Exterior vehicle marking indicating NEMT service
ADA accessibility requirements for wheelchair units:
- 30-inch minimum aisle width
- Hydraulic lift rated 800+ pounds
- 4-point wheelchair securement system
- Lap and shoulder belts for passengers
Required equipment across all vehicles:
- Fire extinguisher
- First aid and biohazard spill kit
- Wheelchair tie-down straps (if applicable)
- Emergency triangles
- Backup alarms (where required)
- GPS tracking system with real-time capability
- Electronic proof of delivery capability
Driver Qualifications
Driver credentials undergo verification during enrollment and credentialing:
Licensing requirements:
- Minimum Class D license
- CDL required for 9+ passenger vehicles or vehicles with air brakes
- Clean 3-5 year motor vehicle record
- No DUIs, reckless driving, or violent offenses
Background and testing:
- FBI-level criminal background check
- Sex offender registry clearance
- DOT drug and alcohol testing (pre-employment plus random)
- DOT Clearinghouse enrollment
Training certifications:
- PASS Certification (Passenger Assistance Safety and Sensitivity)
- CPR and First Aid
- HIPAA compliance training
- Defensive driving course
- Annual refresher training (8-16 hours)
Step 1: Medicaid Provider Enrollment {#medicaid-enrollment}
Medicaid enrollment establishes your legal ability to bill for NEMT services in a specific state. Without an active Provider Transaction Access Number (PTAN), claims cannot be processed.
What Medicaid Enrollment Involves
Every state maintains a Medicaid enrollment portal where providers submit applications, documentation, and undergo screening. The process involves identity verification, background checks against exclusion lists, compliance verification, and site visits in some states.
CMS mandates “high-risk” screening for NEMT providers, meaning more documentation and longer review periods than lower-risk provider categories. The 2025-2026 PAVE (Provider Application and Validation for Enrollment) updates added screening layers that extend timelines.
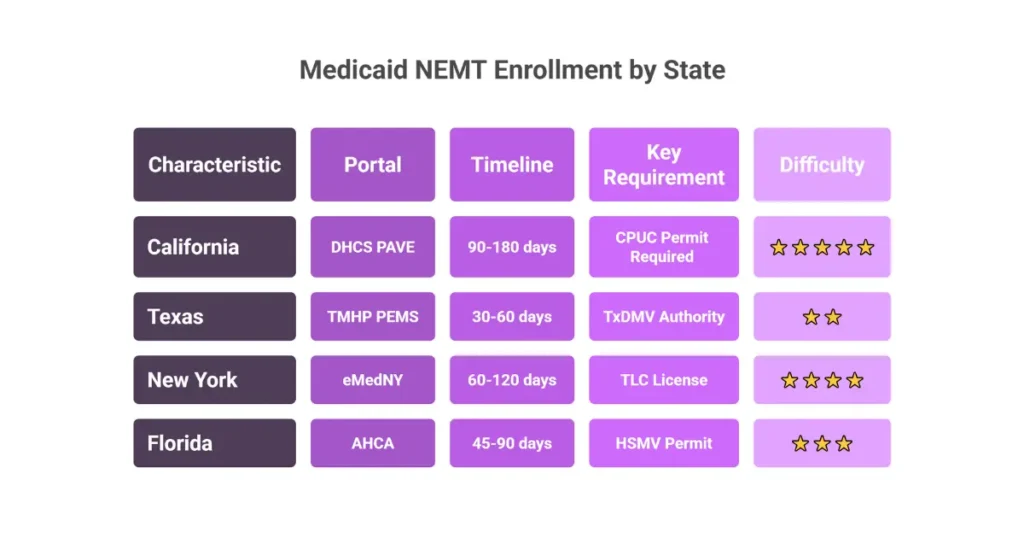
California (Medi-Cal) NEMT Enrollment
Enrollment System: DHCS PAVE Portal (Provider Application and Validation for Enrollment) Governing Body: California Department of Health Care Services (DHCS)
Process Flow:
- Form LLC, obtain EIN and Type 2 NPI
- Apply for CPUC Passenger Stage Corporation (PSC) Permit—mandatory before Medi-Cal billing
- Register and submit application in PAVE portal
- Upload compliance documents for DHCS review
- Receive PTAN upon approval
- Enroll with Managed Care Plans and brokers (ModivCare, Access2Care)
Timeline: 90-180 days Key Requirement: CPUC PSC permit must be approved before Medi-Cal enrollment proceeds
Texas Medicaid NEMT Enrollment
Enrollment System: PEMS (Provider Enrollment and Management System) Administrator: TMHP (Texas Medicaid and Healthcare Partnership)
Process Flow:
- Obtain EIN, NPI, TxDMV carrier authority
- Create PEMS account
- Submit Medicaid enrollment with NEMT taxonomy code 343900000X
- TMHP review and approval
- Receive PTAN
- Enroll with brokers (Zypp, AMR)
Timeline: 30-60 days (fastest major state)
New York Medicaid NEMT Enrollment
Enrollment Systems: eMedNY (Medicaid), MAS (Medical Answering Services—broker)
Process Flow:
- Secure TLC/DMV paratransit license
- Submit enrollment via eMedNY portal
- Apply to MAS broker portal separately
- Document review and approval
- Test claims after PTAN issuance
Timeline: 60-120 days
Florida Medicaid NEMT Enrollment
Enrollment System: AHCA (Agency for Health Care Administration) Provider Portal
Process Flow:
- Obtain HSMV carrier permit
- Register EIN/NPI in AHCA portal
- Submit Medicaid application
- AHCA adjudication
- Enroll with broker (Logisticare)
Timeline: 45-90 days
Required Documents for Medicaid Enrollment
Regardless of state, prepare these documents before starting:
Business Documentation:
- Articles of Organization/Incorporation
- State business license
- EIN verification (CP575, 147C, or W-9)
- Ownership disclosure (5%+ controlling interest)
- Type 2 NPI with taxonomy code 343900000X
Insurance Documentation:
- ACORD 25 Certificate of Insurance
- Commercial auto liability ($1M CSL minimum)
- General liability ($1M/$2M aggregate)
- Workers’ compensation (if applicable)
- Medicaid agency listed as additional insured
Vehicle Documentation:
- Registration and title (business name)
- Annual DOT/safety inspection reports
- VIN-matched insurance binders
- Lift and securement certifications (wheelchair vehicles)
Driver/Owner Documentation:
- FBI-level background checks
- OIG exclusion clearance
- MVRs (3-year clean record)
- Drug and alcohol testing results
- PASS/CPR/First Aid certificates
Common Enrollment Mistakes
Applications get rejected for these preventable errors:
- Missing or incomplete CPUC filings (California)
- Incorrect or missing taxonomy code
- Insurance limits below Medicaid/broker minimums
- Vehicle age or inspection violations
- OIG exclusion matches on any owner or driver
- Missing driver physicals or drug screens
- Address mismatches across IRS, NPI, and Medicaid records
- Late ownership disclosures (can trigger 6-month bans)
Tips for Faster Approval
- Submit CPUC and Medicaid applications in parallel where possible
- Use a Medicaid credentialing service ($2,000-$5,000) to save approximately 60 days
- Pre-audit documents using DHCS or state checklists
- Ensure 100 percent document naming consistency across all submissions
- Run mock compliance audits using NEMT software before submission
- Monitor application status weekly and escalate via portal support emails
Step 2: NPI Registration {#npi-registration}
The National Provider Identifier (NPI) is your 10-digit identification number issued by CMS. Without an NPI, you cannot submit electronic claims to any payer.
Type 1 vs Type 2 NPI
Understanding which type you need prevents common delays:
Type 1 (Individual): Assigned to specific persons, such as a solo driver operating as a sole proprietor. Even with an EIN, sole proprietors typically receive Type 1 NPIs.
Type 2 (Organization): Assigned to business entities—LLCs, Corporations, Partnerships. Most NEMT companies should apply for Type 2 NPI, allowing billing under the business name with multiple drivers and vehicles linked to a single billing entity.
HIPAA mandates this standard identifier to improve efficiency of electronic health information transmission. Every payer requires it.
NPPES Registration Process
The National Plan and Provider Enumeration System (NPPES) is the only official portal for NPI registration. All NEMT providers must register through this CMS-managed system to receive their 10-digit identifier required for electronic claim submission.
Step-by-Step:
- Create I&A Account: Before applying for NPI, create a user account on the Identity & Access Management (I&A) System. This becomes your NPPES login.
- Login to NPPES: Select “Apply for an NPI for an Organization” (for Type 2).
- Enter Business Details:
- Legal Business Name (must match IRS records exactly)
- Employer Identification Number (required for Type 2)
- Business address (physical practice location and mailing address)
- Identify Authorized Official: The person legally responsible for the business (owner, CEO). SSN required for verification.
- Submit and Wait: Electronic applications process within 10 business days typically.
NEMT Taxonomy Codes
Taxonomy codes classify your service type. Wrong code selection causes claim denials.
| Taxonomy Code | Classification | When to Use |
|---|---|---|
| 343900000X | Non-Emergency Medical Transport (Van) | Primary choice—standard code for most NEMT services |
| 343800000X | Secured Medical Transport (Van) | Specialized secure transport (psychiatric, high-risk patients) |
| 344600000X | Taxi | Only if fleet is registered specifically as taxi service |
| 347E00000X | Transportation Broker | Only if managing other providers, not driving |
Most NEMT software and Medicaid portals expect 343900000X. You can add multiple codes, but ensure the van code is marked as primary.
Post-Registration Steps
- Save the NPI Enumerator email and attached PDF—this is your official proof
- Verify your entry in the NPI Registry for correct business name and taxonomy code
- Update NPPES within 30 days of any change to business address, phone, or authorized official
- Enable Multi-Factor Authentication on your I&A account
Step 3: Broker Credentialing {#broker-credentialing}
Here’s what trips up most new providers: Medicaid enrollment alone does not generate trips. You must credential separately with transportation brokers to receive ride assignments and bill for completed trips.
What Broker Credentialing Involves
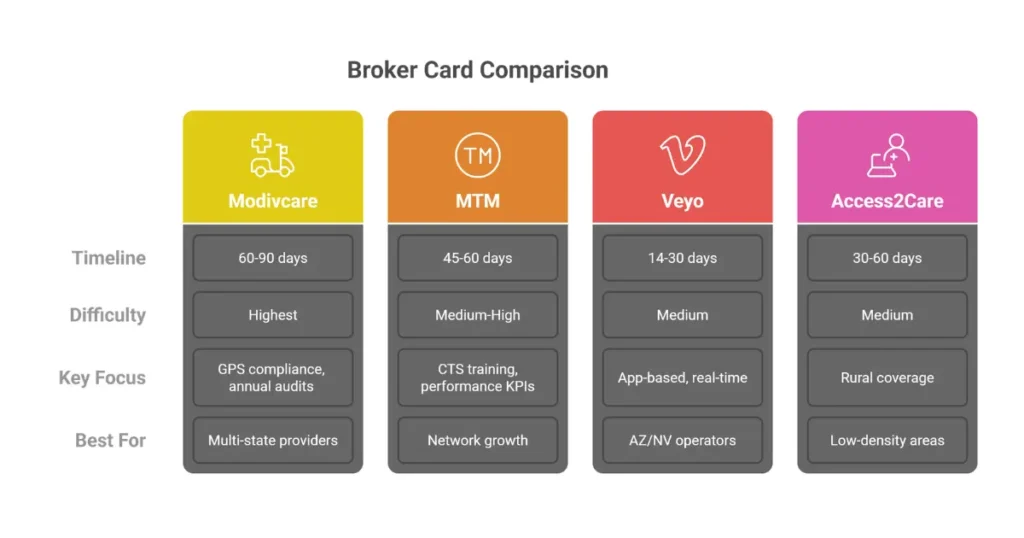
Brokers like ModivCare, MTM, Veyo, and Access2Care contract with state Medicaid agencies to manage transportation benefits. They subcontract with providers, verify compliance, assign trips, and process payments.
Credentialing confirms your business, vehicles, drivers, insurance, and compliance meet broker standards. Each broker has its own portal, requirements, and timeline.
ModivCare Credentialing
Portal: Complicore / WellRyde Prerequisite: Active Medicaid enrollment + Type 2 NPI
Requirements:
- $1M auto liability (ACORD 25 with ModivCare as additional insured)
- Complete fleet and driver uploads
- HIPAA and annual compliance attestations
- GPS-enabled dispatch software
Unique Focus: Compliance audits, GPS tracking verification, annual re-attestation Timeline: 60-90 days Best For: High-volume, multi-state providers
MTM Credentialing
Portal: MTM Provider Portal (mtm-inc.net/providers)
Requirements:
- W-9, insurance, vehicle inspections
- Driver PASS, CPR, MVRs, drug screens
- CTS (Customer Transportation Specialist) training
- MTM Connect app (GPS and ePOD mandatory)
Unique Focus: Network adequacy and performance KPIs Timeline: 45-60 days
Veyo Credentialing
Portal: Veyo Provider Portal
Requirements:
- Medicaid enrollment prerequisite
- $1M liability insurance
- Vehicles under 10 years old
- Driver background (under 4 MVR points)
- Wheelchair competency test (if applicable)
Unique Focus: App-based dispatch, real-time response requirements Timeline: 14-30 days (fastest broker) Best For: Arizona and Nevada operators
Access2Care Credentialing
Portal: Access2Care Vendor Portal
Requirements:
- EIN, NPI, insurance binders
- DOT inspections current
- Driver physicals, drug screens, OIG checks
Unique Focus: Rural coverage, stretcher transport options Timeline: 30-60 days Advantage: Faster approvals in low-density counties
Broker Timeline Comparison
| Broker | Average Credentialing Time | Notes |
|---|---|---|
| Veyo | 14-30 days | Fastest, tech-driven |
| Access2Care | 30-60 days | Faster in rural areas |
| MTM | 45-60 days | Training-heavy |
| ModivCare | 60-90 days | Highest compliance requirements |
Universal Credentialing Documents
Regardless of broker, prepare:
Business Credentials:
- State/local business license
- W-9 (current, signed)
- ACORD 25 COI with broker as additional insured
- $1M CSL auto liability minimum
- General liability ($1M/$2M aggregate)
- Surety bond ($5,000-$50,000, broker/state dependent)
- Active Type 2 NPI (343900000X)
- SAM.gov registration
Vehicle Credentials:
- Registration and title (business name)
- Annual DOT safety inspections
- Vehicle age compliance (10-15 years max)
- ADA-compliant ramps/lifts (800 lb capacity)
- Interior/exterior photos
- Required equipment (fire extinguisher, first aid kit, backup alarm, spill kit)
Driver Credentials:
- Background checks (7-10 years)
- Clean MVR (under 6 points in 3 years)
- Valid license (CDL if required)
- PASS certification
- CPR/First Aid
- DOT 5-panel drug and alcohol screening
- Physical exam (where required)
Common Credentialing Mistakes
- Address mismatches between insurance, NPI, and license
- Missing broker as additional insured on COI
- Documents expiring within 30 days of submission
- Unsigned contract pages
- Vehicle registrations in personal name instead of business
- Missing GPS or dispatch system proof
- Driver credentials lapsing mid-contract
Any credential lapse makes trips non-billable and may trigger clawbacks.
Maintaining Credentials
Credentialing isn’t one-and-done:
- Annual full recredentialing (all documents)
- Quarterly driver re-checks (MVR, drug tests)
- Monthly audits for insurance and vehicle status
- Immediate suspension for expired credentials
- Full broker re-onboarding every 2-3 years
Use automated document tracking with 90/60/30-day expiration alerts.
Step 4: Clearinghouse and EDI Setup {#clearinghouse-setup}
A clearinghouse sits between your billing system and payers, standardizing and validating claims before submission. Skipping this step means manual portal entry for every claim—unsustainable at any volume.
What a Clearinghouse Does
Healthcare clearinghouses convert your trip data into HIPAA-compliant ANSI X12 5010A1 format, scrub claims for errors before submission, route clean claims to Medicaid and broker systems, and return electronic remittance files for payment posting.
The business impact is significant: clearinghouse-processed claims reduce denials by 20-30 percent and cut average accounts receivable from 90+ days to 15-45 days. Bulk submission replaces manual portal entry.
Top Clearinghouses for NEMT
| Clearinghouse | Best For | NEMT Strength | Cost Model |
|---|---|---|---|
| Availity | Multi-broker NEMT | Strong ModivCare/MTM connectivity | $0.10-$0.25 per claim (often payer-sponsored) |
| Change Healthcare | High-volume fleets | Broadest payer network | $0.15-$0.40 per claim |
| Trizetto (Cognizant) | Enterprise NEMT | Government EDI reliability | $75-$500/month subscription |
| Office Ally | Startups | Free entry-level access | Free basic tier |
| Waystar | Large fleets | Analytics + denial management | $150-$300+/month |
Recommendations:
- Multi-state/broker-heavy operations: Availity
- Single-state startups: Office Ally
- Enterprise fleets: Trizetto or Change Healthcare
EDI Transaction Types
NEMT billing requires these electronic transactions:
| Transaction | Purpose |
|---|---|
| 837P | Professional claim submission (HCPCS A0100-A0999, mileage codes) |
| 999 | Claim receipt acknowledgement |
| 270/271 | Real-time eligibility verification |
| 835 | Electronic Remittance Advice for auto-posting payments |
Brokers also validate GPS and ePOD metadata alongside standard EDI files.
Clearinghouse Setup Process
Prerequisites:
- Type 2 NPI (343900000X)
- Medicaid PTAN/Provider ID
- Broker credentialing completed
Steps:
- Select Clearinghouse: Confirm direct integration with your NEMT software (RouteGenie, TobiCloud, etc.)
- Vendor Enrollment: Submit EIN, W-9, NPI. Sign clearinghouse agreement.
- Payer and Broker EDI Enrollment: Complete state Medicaid EDI forms (PEMS, PAVE). Sign Trading Partner Agreements. Add broker payer IDs (e.g., ModivCare 68068).
- Integration and Testing: Software integration via API/SFTP (1-2 weeks). Submit 10-25 test claims. Achieve 90%+ acceptance rate.
- Go-Live: Production billing enabled. 30-day monitoring period targeting 95% clean-claim rate.
Clearinghouse Costs
| Cost Type | Typical Range |
|---|---|
| Setup fee | $0-$500 |
| Per-claim fee | $0.08-$0.40 |
| Monthly minimum | $25-$200 |
| Subscription (enterprise) | $75-$500/month |
Example: 500 trips/month × $0.15/claim = approximately $900/year. Bundling ERA and eligibility checks reduces costs by approximately 15%.
Timeline
| Phase | Duration |
|---|---|
| Clearinghouse enrollment | ~1 week |
| State/broker trading partner agreements | 1-2 weeks |
| Testing and certification | 2-3 weeks |
| Go-live | Immediate after approval |
Total: 4-8 weeks post-PTAN
Run clearinghouse and broker EDI enrollment in parallel to save approximately 2 weeks.
Common Clearinghouse Errors
- Invalid or missing payer IDs (40% of rejections)
- Missing service facility NPI
- Taxonomy mismatch (343900000X required)
- HCPCS/modifier errors
- GPS/ePOD attachment failures
- Eligibility not checked (270/271 skipped)
Step 5: Billing Software Selection {#software-selection}
The right NEMT software reduces billing errors by up to 25 percent, cuts AR by 30-60 days, and typically breaks even at just 100-200 trips per month. The wrong choice creates manual workarounds that consume staff time and increase denials.
Software Pricing Models
Per-Vehicle Pricing: $40-$150 per vehicle/month. Best for predictable budgeting and growing fleets.
Per-Trip Pricing: $0.25-$0.75 per trip. Aligns cost with revenue but fluctuates seasonally.
Flat Subscription: $250-$1,500/month. Bundled dispatch and billing regardless of volume.
Enterprise/Custom API: $2,000+/month. For 50+ vehicles, multi-broker integration, advanced analytics.
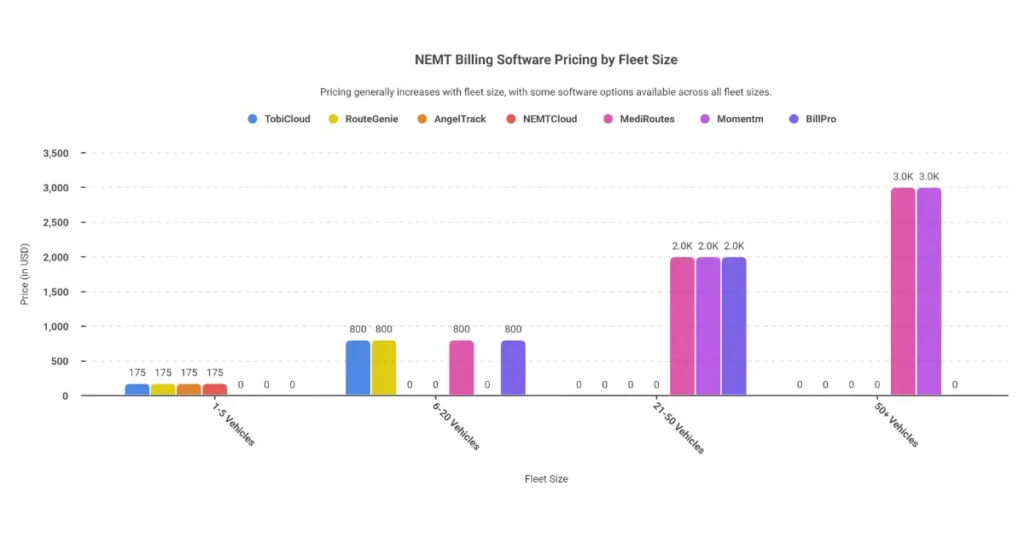
Monthly Cost by Fleet Size
| Fleet Size | Monthly Range | Notes |
|---|---|---|
| 1-5 vehicles | $50-$300 | Entry-level SaaS, limited automation |
| 6-20 vehicles | $400-$1,200 | Volume discounts typically apply |
| 21-50 vehicles | $1,000-$3,000 | Dedicated support common |
| 50+ vehicles | $3,000+ | Custom API and broker SLAs |
Hidden Costs to Watch
- Setup/implementation: $0-$5,000
- Custom integrations: $2,000-$10,000
- Overage fees: ~$0.50 per excess trip
- Premium support: $100-$300/month
- GPS hardware: ~$50 per vehicle
- Clearinghouse pass-through: ~$0.15 per claim
- Annual increases: 10-15%
Top NEMT Software Options
TobiCloud
- Best for: 1-20 vehicles
- Key features: Trip attestation, broker EDI, AR tracking
- Pricing: ~$50/vehicle + $0.10/trip
- Integrations: MTM Connect, Availity, GPS telematics
RouteGenie
- Best for: Small to mid-size fleets
- Key features: Route optimization, ePOD, analytics
- Pricing: ~$50/vehicle (volume discounts)
- Integrations: Veyo, Change Healthcare, Power BI
MediRoutes
- Best for: Multi-state Medicaid operations
- Key features: Multi-payer billing, GPS validation
- Pricing: Custom (~$75/vehicle)
- Integrations: Trizetto, state Medicaid portals
AngelTrack
- Best for: Tech-savvy startups
- Key features: Open-source base, HIPAA billing
- Pricing: $99-$299/month flat
- Integrations: Office Ally, custom EDI
Momentm (NovusMED)
- Best for: 20+ vehicle fleets
- Key features: AI scheduling, safety analytics
- Pricing: $100-$250/vehicle
- Integrations: All major brokers
BillPro
- Best for: Billing-heavy operations
- Key features: Denial management, ERA auto-posting
- Pricing: $200-$500/month
- Integrations: Availity, Medicaid FFS
Essential Software Features
Must-have capabilities:
- EDI 837P/835/270-271 support
- Broker API integrations (MTM, ModivCare, Veyo)
- GPS tracking with ePOD signatures
- HCPCS claim scrubbing (A0100-A0999, S0215)
- ERA auto-posting
- HIPAA and 5010A1 compliance
- Driver mobile apps (offline capable)
Impact by feature:
| Feature | Business Impact |
|---|---|
| GPS + ePOD | 25-40% denial reduction |
| Claim scrubbing | 20-30% cleaner claims |
| Eligibility checks | Prevents ~30% avoidable denials |
| Broker APIs | Eliminates double entry, saves 15 days cash flow |
| Denial analytics | Recovers 20-35% rejected revenue |
Implementation Timeline
| Phase | Duration |
|---|---|
| Vendor demos and selection | Week 1 |
| Configuration and EDI mapping | Weeks 2-3 |
| Driver training and dry runs | Week 4 |
| Go-live (limited volume) | Week 5 |
| Full operational rollout | Week 6 |
Total: 4-6 weeks typical, 2-3 weeks accelerated for SaaS
Step 6: Documentation Systems {#documentation-systems}
Documentation makes or breaks NEMT billing. Missing any required element can result in 80-100% claim denial—even when the trip actually occurred.
Required Trip Documentation
Every completed trip needs these elements captured:
Patient Information:
- Full legal name (exact Medicaid match)
- Date of birth
- Medicaid/Insurance ID number
Trip Details:
- Pickup and drop-off addresses (suite/unit specific)
- Service date
- Appointment purpose and time
- Loaded mileage (GPS and odometer aligned)
Five Mandatory Timestamps:
- Dispatch
- Arrive pickup
- Depart pickup
- Arrive destination
- Depart destination
Dual Electronic Signatures:
- Driver attestation
- Patient/guardian ePOD (electronic proof of delivery)
Driver Documentation:
- Full name
- Valid driver’s license number
- Pre-trip and post-trip vehicle inspection logs
- Patient interaction notes (mobility needs, condition)
Vehicle Documentation:
- Make/model/year
- VIN and license plate
- Current registration
Authorization Documentation:
- Prior authorization number
- Authorized service type and limits
- Broker Trip ID
- Assignment confirmation
GPS Tracking Requirements
100% GPS coverage is mandatory for all major brokers. ModivCare, MTM, and Veyo all require GPS verification.
Standards:
- Pickup/drop-off validation within 0.1 miles
- Loaded mileage must match GPS route
- Route deviation alerts enabled
- Five GPS-synced timestamps per trip
Audit trail requirements:
- GPS device ID
- Date/time stamp
- Latitude/longitude (WGS84 format)
- Speed and heading
- Device-to-claim chain of custody
Without GPS breadcrumb data, claims face automatic denial.
Recommended GPS systems:
- Samsara: $25-$40/vehicle/month
- Verizon Connect: ~$30/vehicle/month
- Native GPS via NEMT software (TobiCloud, RouteGenie)
Electronic Signature Requirements
Patient/Guardian Signatures:
- HIPAA-compliant digital signatures only
- Wet-ink signatures increasingly rejected post-2025
- Proxy signatures require documented authority
- Optional photo verification (privacy-compliant)
Driver Attestation:
- Separate electronic confirmation of trip completion
- Patient condition observed
- Accommodations provided (wheelchair, oxygen)
- Time-synced with GPS location
Compliance Rules:
- Signatures must be unalterable
- Pixel data, timestamp, and device ID locked on capture
- Signature required to close trip in software
Physician Certification Statement (PCS)
When PCS is required:
- Wheelchair transport
- Stretcher transport
- Non-ambulatory Medicaid members
PCS must include:
- Diagnosed condition requiring NEMT
- Reason patient cannot use public/personal transport
- Authorized frequency and duration
- Physician signature and date
Renewal: Typically quarterly. Missing or expired PCS triggers immediate claim denial.
Document Retention Requirements
Retention periods:
- Federal minimum: 7 years
- California/New York: 10 years
- Broker access: 90-day immediate portal availability
Storage standards:
- HIPAA-compliant encrypted cloud storage
- AES-256 encryption
- Access logs retained 6+ years
- Paper backups recommended for disputes
Audit readiness: Ability to produce complete trip file within 5 minutes, organized by Year → Month → Patient → Trip ID.
Step 7: HCPCS Codes and Billing Requirements {#hcpcs-codes}
HCPCS coding errors are among the top reasons NEMT claims deny. Understanding which codes to use and how modifiers work prevents preventable revenue loss.
For detailed information on denial codes and resolution, see our NEMT denial codes guide.
NEMT HCPCS Codes
Base Trip Codes:
| Code | Description | Typical Use |
|---|---|---|
| A0080 | Taxi transport, non-emergency | Low-cost taxi-based NEMT |
| A0090 | Per diem taxi charges | Multiple trips in one day |
| A0100 | Non-emergency taxi, single trip | Ambulatory curb-to-curb |
| A0120 | Wheelchair van (no lift required) | Ambulatory patient, wheelchair-accessible vehicle |
| A0130 | Wheelchair van with lift and securement | Most common NEMT wheelchair code |
| A0140 | Wheelchair van with attendant | Mobility or safety assistance needed |
Mileage Codes (Loaded Miles Only):
| Code | Description | Notes |
|---|---|---|
| A0425 | Ground mileage, per mile | Loaded miles only; GPS required |
| S0215 | Ground mileage, per statute mile | Required by some states (e.g., California) |
Specialized/State-Specific Codes:
| Code | Description |
|---|---|
| S0209 | Wheelchair mileage (short-haul) |
| T2001 | Transport, wheelchair—base + mileage |
| T2002 | Wheelchair transport with attendant |
| T2003 | Litter vehicle with attendant |
| T2004 | Stretcher vehicle transport |
| T2005 | Air transport (rare) |
| A0170 | Ancillary services (tolls, parking) |
Origin and Destination Modifiers
Two-character modifiers must be appended to every base and mileage line. First letter indicates origin, second letter indicates destination.
| Letter | Location Type |
|---|---|
| R | Residence/Home |
| H | Hospital |
| P | Physician office/clinic |
| N | Skilled nursing facility (SNF) |
| D | Diagnostic/therapeutic site |
| E | Residential care facility |
| G | Hospital-based dialysis |
| J | Non-hospital dialysis |
| S | Scene |
| I | Site of transfer |
| X | Intermediate stop |
Common Modifier Pairs:
| Pair | Meaning |
|---|---|
| RH | Residence → Hospital |
| HR | Hospital → Residence |
| RP / PR | Residence ↔ Physician |
| RN / NR | Residence ↔ SNF |
| RG / GR | Residence ↔ Hospital dialysis |
| RJ / JR | Residence ↔ Free-standing dialysis |
Missing or mismatched modifiers are a top cause of CO-96 and PR-16 denials.
Reimbursement Rate Ranges
Rates vary significantly by state. See our state-by-state Medicaid NEMT rates guide for specific amounts.
| Code | Description | Base Rate Range | Mileage |
|---|---|---|---|
| A0130 | Wheelchair van w/lift | $25-$75/trip | $2-$10/mi |
| A0120 | Wheelchair van no lift | $20-$50/trip | A0425 |
| A0100 | Taxi NEMT | $10-$25/trip | A0425 |
| A0425 | Ground mileage | N/A | $1.10-$10/mi |
High-paying states: California, New York ($50-$120/trip) Low-paying states: Mississippi, Indiana ($12-$25/trip)
CMS-1500 Form Key Fields
| Box | Content |
|---|---|
| 21 | Diagnosis (commonly Z75.3 or patient condition) |
| 24D | HCPCS code + two-letter modifier (e.g., A0130 RH) |
| 24G | Units: Base = 1, Mileage = total loaded miles |
| 32 | Drop-off facility address |
| 33 | Billing provider NPI and address |
Critical Rules:
- Base and mileage lines must carry matching modifiers
- Mileage units must match GPS and trip logs
- Prior authorization required for stretcher and specialty codes
Common Coding Errors
- CO-96: Wrong vehicle type billed
- CO-45: Missing authorization
- PR-16: Mileage mismatch (billed unloaded miles)
- Modifier mismatch: Base modifier ≠ mileage modifier
- Invalid origin/destination pairs
Step 8: Staff Training {#staff-training}
Billing staff competency directly impacts clean-claim rates and denial recovery. Untrained part-time staff handling billing typically results in 10-20% lost collections.
Staff Roles and Requirements
Intake and Eligibility Specialist: Verifies Medicaid coverage, trip eligibility, PCS/prior authorizations before transport.
Billing Specialist/Clerk: Converts trip data into claims, submits via clearinghouse, posts payments, resolves rejections.
Denial Management/AR Specialist: Analyzes EOB/ERA codes, corrects errors, manages appeals, tracks denial trends.
Billing Lead/RCM Analyst: Oversees workflows, KPIs, payer performance, complex appeals.
Compliance Officer: Conducts audits, ensures HIPAA and Medicaid compliance, updates training based on rule changes.
Baseline Qualifications:
- Prior healthcare or Medicaid billing experience (NEMT preferred but not required)
- Proficiency with Excel, EMRs, dispatch systems, clearinghouses
- Understanding of HCPCS coding, EDI (837/835), payer manuals
- High attention to detail and ability to follow SOPs
- For leadership: 2-3 years billing experience plus NEMT operations familiarity
Training Curriculum
NEMT Foundations:
- Medicaid NEMT benefit overview and eligibility rules
- Differences between NEMT, ambulance, and rideshare billing
- End-to-end trip lifecycle: eligibility → auth → trip → documentation → claim → payment
Coding and Modifiers:
- HCPCS transport codes (A0100, A0120, A0130, A0425, S0215, T2001-T2005)
- Origin/destination modifiers (RH, HR, RP, PR)
- State-specific modifiers (U1-U9, TT, HQ)
- Coding scenarios: dialysis, repetitive trips, shared rides
Medicaid and State Rules:
- Federal Medicaid NEMT requirements
- Reading and interpreting state Medicaid NEMT manuals
- Timely filing, documentation retention, overpayment rules
Broker-Specific Training:
- ModivCare, MTM, Veyo, Access2Care workflows
- Portal navigation, trip closure, GPS/ePOD requirements
- Broker billing IDs, file formats, submission timelines
Denial and AR Management:
- Common denial codes (CO-16, CO-4, CO-96, CO-109)
- Root cause analysis and prevention
- Appeal documentation and workflows
- Weekly denial reviews and monthly retraining
Compliance and HIPAA:
- HIPAA privacy and security standards
- Fraud, Waste, and Abuse (FWA) awareness
- Audit readiness and record-keeping
Certification Options
General Billing and Coding:
- Certified Professional Biller (CPB—AAPC)
- Certified Professional Coder (CPC—AAPC)
- Certified Medical Reimbursement Specialist (CMRS)
NEMT/Transportation-Specific:
- NEMTAC certifications (operations, compliance, billing modules)
- NEMTAC Certified Transport Specialist (CTS)
- CTAA training programs
- NAAC Certified Ambulance Coder (CAC)—respected crossover credential
Best practice: At least one formal billing credential plus one NEMT-specific certification per team.
In-House vs Outsourced Billing {#in-house-vs-outsourced}
The build-or-buy decision significantly impacts cash flow, control, and scalability. Neither option is universally superior—your fleet size, growth trajectory, and management bandwidth determine the right choice.
In-House Billing Costs
Primary cost components:
| Component | Annual Cost |
|---|---|
| Billing specialist salary | $45,000-$60,000 |
| Billing manager/RCM lead | $65,000-$85,000 |
| Benefits and payroll taxes | 20-30% of salary |
| Fully loaded cost per biller | ~$66,000-$71,500 |
Additional costs:
- NEMT software: $50-$200 per vehicle/month
- Training and onboarding: $1,000-$3,000 per hire
- Overhead (office, IT, compliance): 15-25% of salary
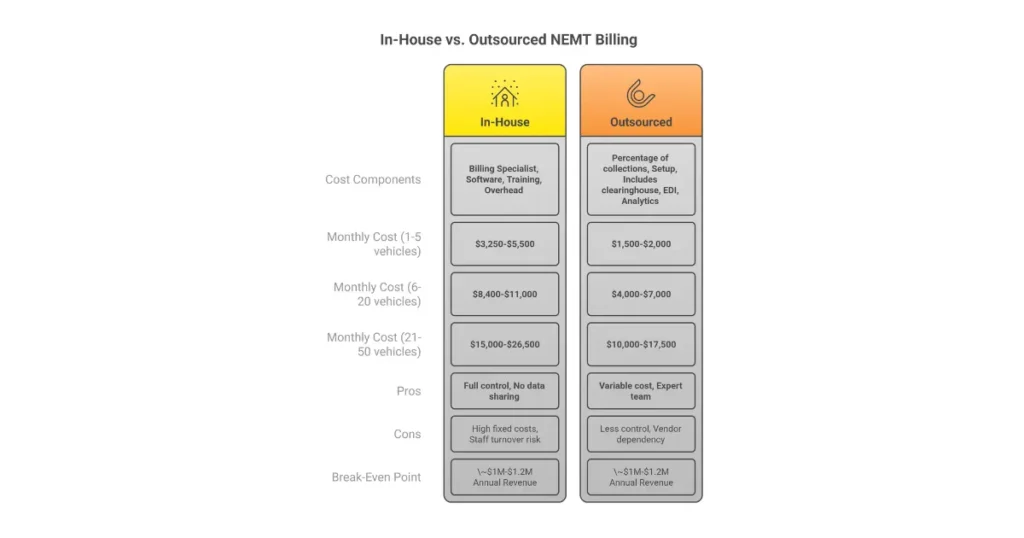
Monthly cost by fleet size:
| Fleet Size | Monthly In-House Cost |
|---|---|
| 1-5 vehicles | $3,250-$5,500 |
| 6-20 vehicles | $8,400-$11,000 |
| 21-50 vehicles | $15,000-$26,500 |
| 50+ vehicles | $28,000-$50,000+ |
Outsourced Billing Costs
Common pricing models:
Percentage of collections: 4-8% of collected revenue. Smaller fleets or complex AR push toward 7-8%. Larger, cleaner operations get 4-6%.
Flat fee/minimums: $750-$2,000/month for low volume, plus per-claim fees.
One-time setup: $1,000-$5,000 for onboarding, integrations, credentialing support.
Monthly cost by fleet size:
| Fleet Size | Monthly Outsourced Cost |
|---|---|
| 1-5 vehicles | $1,500-$2,000 |
| 6-20 vehicles | $4,000-$7,000 |
| 21-50 vehicles | $10,000-$17,500 |
| 50+ vehicles | $18,000-$25,000 (negotiated) |
Outsourced fees typically include clearinghouse, EDI, and basic analytics.
Pros and Cons Comparison
In-House Billing:
| Pros | Cons |
|---|---|
| Full operational and reporting control | High fixed costs regardless of volume |
| Immediate coordination with dispatch | Staff turnover risk disrupts cash flow |
| No third-party data handling | Management time required |
| Custom workflows and payer strategies | Slower scalability during growth |
Outsourced Billing:
| Pros | Cons |
|---|---|
| Variable, performance-based cost | Percentage fees increase with revenue |
| Faster implementation and scalability | Potential visibility gaps without strong SLAs |
| Lower denial rates, stronger appeal expertise | Vendor dependency risk |
| Reduced HR, training, IT burden | May not prioritize marginal, low-dollar appeals |
Break-Even Analysis
Calculate your effective costs:
In-house cost percentage = (Billing staff + software + overhead) ÷ monthly collections
Outsourced cost percentage = Contracted percentage of collections
Typical outcomes:
- Small fleets (1-10 vehicles): In-house cost often 10-15%+. Outsourced cost 4-8%. Outsourcing usually cheaper.
- Mid-sized fleets (10-30 vehicles): Costs converge. Decision depends on collection performance and denial rates.
- Larger fleets (30+ vehicles): In-house can be cost-effective if net collections ≥95% and AR is well-managed.
Rule of thumb: Break-even typically occurs around $1.0-$1.2M annual revenue, assuming competent internal management.
Decision Factors
Consider:
- Fleet size and revenue stability
- Monthly collections vs. fully loaded cost of a biller
- Current denial rate and AR performance
- Internal expertise in Medicaid, brokers, NEMT coding
- Multi-state or multi-broker complexity
- Leadership bandwidth for compliance and analytics
- Need for customization vs. speed to cash
Hybrid models (shared responsibility) are common at mid-scale—keeping dispatch-billing coordination in-house while outsourcing denial management or credentialing.
For providers who want expert handling of their billing operations, our NEMT billing services team manages everything from enrollment through collections.
Common Mistakes and FAQ {#mistakes-faq}
Most NEMT revenue loss occurs before the first claim is ever submitted. These mistakes and their prevention strategies come from patterns we see repeatedly.
Top 15 NEMT Billing Mistakes
Pre-Launch Mistakes:
1. Launching trips before payer enrollment is complete Prevention: Do not accept Medicaid/broker trips until provider IDs, contracts, and EDI testing are fully approved. Use a go-live checklist. Cost impact: 1-3 months of unrecoverable revenue.
2. Underestimating Medicaid and broker setup timelines Prevention: Plan for 90-180 days to first consistent payment. Maintain minimum 3-month operating cash reserve. Cost impact: Severe cash-flow gaps; early business failure risk.
3. No documentation workflow before first trip Prevention: Standardize trip logs and train drivers before launch. Cost impact: Early denials and permanent write-offs.
Credentialing Mistakes:
4. Submitting enrollment with incomplete insurance or licensing Prevention: Use payer-specific credentialing checklists. Review packets before submission. Cost impact: 1-3 months delayed revenue.
5. Using wrong NPI type or taxonomy Prevention: Enroll with Type 2 (organizational) NPI and correct NEMT taxonomy. Keep EIN and legal name consistent. Cost impact: 30-90 days avoidable delay.
6. Ignoring recredentialing and document expirations Prevention: Track COIs, licenses, inspections, driver certs with 90/60/30-day alerts. Cost impact: Trip suspensions and payment holds.
Documentation and Coding Mistakes:
7. Incomplete trip documentation Prevention: Configure software to block trip completion without required fields and signatures. Audit weekly. Cost impact: 10-30% denial rates and audit exposure.
8. Incorrect base codes or missing mileage pairing Prevention: Embed code-selection rules. Maintain internal coding grid. Cost impact: Repeated denials; fraud scrutiny if systemic.
9. Mismatched or missing origin/destination modifiers Prevention: Auto-inherit modifiers from base codes to mileage lines. Cost impact: High preventable denial volume.
Compliance Mistakes:
10. Skipping HIPAA and FWA training Prevention: Mandatory onboarding and annual training. Document attendance. Cost impact: Regulatory penalties and contract termination risk.
11. Treating all states and brokers the same Prevention: Maintain state- and broker-specific billing rules. Update when manuals change. Cost impact: Chronic denials and underpayments.
Technology Mistakes:
12. Using dispatch software without billing integration Prevention: Adopt NEMT-specific platforms with dispatch, billing, GPS, and ePOD integration. Cost impact: Errors, missed trips, slower cash flow.
13. No claim scrubbing or rejection monitoring Prevention: Enable pre-submission edits. Work clearinghouse rejections daily. Cost impact: Missed timely filing and inflated staffing costs.
Staffing and Process Mistakes:
14. Assigning billing to untrained part-time staff Prevention: Designate dedicated RCM role or outsource to NEMT-experienced partner. Cost impact: 10-20% lost collections.
15. No billing KPIs or review cadence Prevention: Track clean-claim rate, denial rate, days in AR, write-offs monthly. Cost impact: 5-15% silent annual revenue leakage.
Frequently Asked Questions
-
How to bill Medicaid for NEMT?
Billing Medicaid for NEMT requires completing provider enrollment to receive a PTAN, verifying patient eligibility before each trip, documenting trips with GPS timestamps and electronic signatures, coding claims with appropriate HCPCS codes (A0130, A0425) and origin/destination modifiers, and submitting electronically through your clearinghouse within state timely filing limits. Most states also require broker credentialing for trip assignments. Our complete NEMT billing guide covers the full process.
-
How do NEMT companies get paid?
NEMT companies receive payment through four channels: Medicaid fee-for-service (30-90 day payment), broker-managed Medicaid through ModivCare, MTM, or Veyo (15-30 day payment), Medicare Advantage supplemental benefits (14-30 day payment), and direct private pay from patients or facilities (same day to 7 days). Most providers rely primarily on broker-managed Medicaid, which offers faster payment but requires separate credentialing.
-
How much does NEMT software cost?
NEMT billing software costs $50-$300/month for 1-5 vehicles, $400-$1,200/month for 6-20 vehicles, and $1,000-$3,000+/month for larger fleets. Pricing models include per-vehicle ($40-$150/vehicle), per-trip ($0.25-$0.75), or flat subscription. Setup fees range from free to $5,000. Hidden costs include custom integrations, GPS hardware, and clearinghouse pass-through fees.
-
How long does NEMT credentialing take?
Total NEMT credentialing takes 90-180 days on average. Medicaid enrollment ranges from 30 days (Texas) to 180 days (California). Broker credentialing adds 14-90 days depending on the broker—Veyo is fastest at 14-30 days, ModivCare slowest at 60-90 days. Parallel processing and using credentialing services can compress timelines by 30-60 days.
-
Is NEMT profitable?
Yes, NEMT is profitable when utilization, documentation, and billing are well-managed. Profit margins scale with trip volume—small denial improvements of 5-10% materially impact profitability. Providers who maintain clean-claim rates above 95% and days in AR under 45 typically achieve healthy margins. For detailed profitability analysis, see our article on whether NEMT is a good business.
-
Can I bill Medicaid without being credentialed?
No. Medicaid does not reimburse NEMT services unless the provider is fully enrolled and authorized on the date of service. Trips completed before your effective enrollment date are non-reimbursable and increase compliance risk. Similarly, broker trips require active credentialing—completing trips before approval means working for free.
-
What’s the difference between a rejection and a denial?
Rejections occur at the clearinghouse level before payer review—they’re technical errors like invalid member ID or missing fields. Fix and resubmit immediately. Denials occur after payer adjudication—they’re coverage or policy decisions requiring appeals. Rejections are faster to resolve but must be caught quickly to avoid timely filing issues.
-
How long does it take to get paid for NEMT trips?
Payment timelines vary by payer: brokers typically pay in 14-21 days via EFT, while state Medicaid may take 30-60 days depending on fiscal cycles and clean-claim rates. Private pay collects same-day to 7 days. Factors affecting speed include documentation completeness, coding accuracy, and denial rates.
Conclusion
Setting up NEMT billing requires patience, attention to detail, and realistic timeline expectations. The 90-180 day setup window tests new providers, but those who follow proper sequencing—business formation, Medicaid enrollment, broker credentialing, clearinghouse setup, software implementation, documentation systems—emerge with billing infrastructure that generates consistent cash flow.
The providers who struggle are those who rush trips before enrollment completes, skip documentation standards, or treat billing as an afterthought. The providers who thrive invest upfront in proper setup, train staff on NEMT-specific requirements, and build systems that prevent denials rather than just appealing them.
Key takeaways:
- Plan for 90-180 days from business formation to first paid claim
- Budget $5,000-$25,000 for billing-specific startup costs
- Complete Medicaid enrollment AND broker credentialing—both are required
- GPS documentation and electronic signatures are non-negotiable
- Track clean-claim rate, denial rate, and days in AR from day one
For providers who want expert guidance through the setup process or prefer to outsource billing entirely, our NEMT billing specialists handle everything from enrollment through collections.
Need a custom NEMT website to support your growing operation? Our NEMT website development services create professional online presence tailored to transportation providers.

