You’ve narrowed your shortlist. You’ve watched at least two demos. Now you need the one thing every OTP EMR vendor makes hardest to get before a call: real pricing.
If you are comparing methadone clinic software pricing in 2026, the hardest part is not finding vendors — it is understanding what each quote actually includes. This guide is the price-discovery worksheet we wish more clinic owners had before signing. We’ll show you the public pricing signals for the seven OTP/MAT platforms most clinics shortlist in 2026, the line items vendors typically don’t volunteer (implementation, pump validation, EPCS, clearinghouse, exit fees), a working 3-year total cost of ownership model, an ROI worked example with real OTP billing math, and a candid breakdown of MASE’s Growth Bridge program — including who qualifies, who doesn’t, and why it’s not a loan.
Important: Every OTP EMR vendor quotes custom pricing based on patient census, provider count, modules, integrations, and contract term. Numbers in this guide are public signals from vendor pages, Capterra, GetApp, Software Advice, G2, and analyst databases as of May 2026. Use them to set expectations and to negotiate — not as final quotes. Get a written proposal before you sign.

TL;DR — Methadone clinic software pricing in 2026
In 2026, methadone clinic software commonly ranges from several hundred dollars per month to $1,500+/month per provider for enterprise platforms. Most dedicated OTPs spend $400–$900 per provider per month for the EMR subscription alone, plus 3–8% of collections if billing is included, plus a one-time implementation fee of $5,000–$50,000+ depending on platform complexity and pump validation requirements. Some eligible OTPs may qualify for MASE Growth Bridge, which can reduce or cover the EMR subscription when paired with EliteMed billing at 2.85% of collections.
The cheapest EMR is almost never the cheapest total cost. The platforms that look inexpensive on the subscription line often charge separately for implementation, pump integration, EPCS, PDMP, clearinghouse, training, and support — and the highest “hidden cost” most clinics underestimate is billing leakage from denials, missed bundle billing, and underpaid take-homes.
If your clinic is shopping price, the right comparison is 3-year TCO including billing, not monthly subscription.
If you want software plus billing handled together, see our complete OTP clinic software solution.
Table of Contents
Who this pricing guide is for
This guide is for OTP owners, methadone clinic administrators, MAT program directors, billing managers, compliance officers, and behavioral health executives comparing software costs before booking demos.
It is especially useful if you are opening a new OTP clinic, replacing AZZLY, Kipu, Methasoft, or paper workflows, comparing EMR + billing options, trying to understand Growth Bridge eligibility, calculating 3-year EMR and billing cost, or reviewing quotes from multiple OTP EMR vendors.
This guide is not written for patients looking for methadone treatment pricing. It is written for clinic decision-makers evaluating software and billing systems.
Methadone clinic software pricing models explained
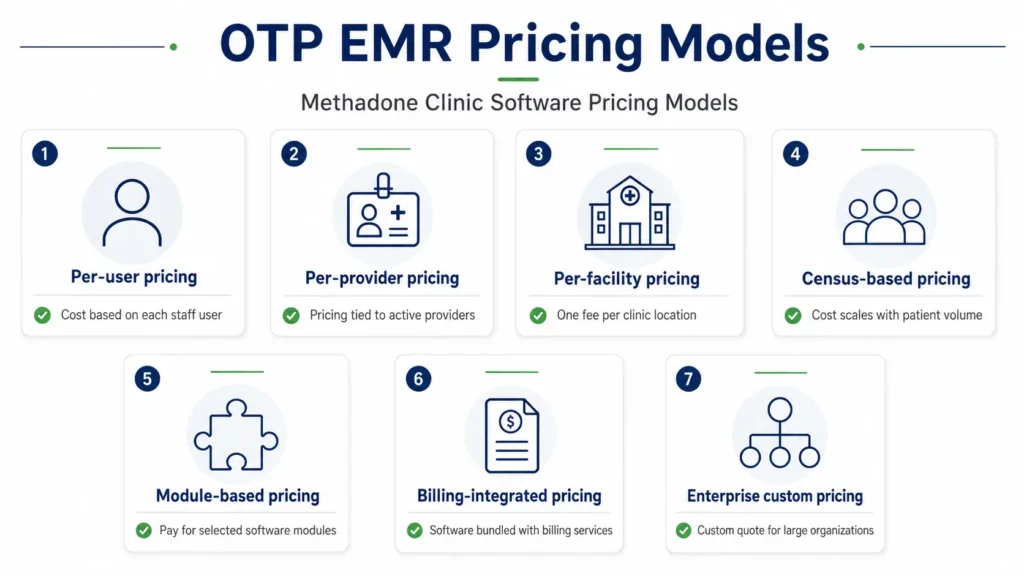
Most OTP EMR vendors use one of seven pricing models: per-user, per-provider, per-facility, census-based, module-based, billing-integrated, or enterprise custom pricing. The model matters because two vendors can quote the same monthly number but produce completely different three-year costs.
| Pricing Model | How It Works | Best Fit | Watch Out For |
|---|---|---|---|
| Per-user | You pay for each staff login | Small clinics with stable teams | Costs rise with nurses, counselors, billers, and admins |
| Per-provider | You pay for prescribers or licensed providers | Provider-led clinics | Ask whether counselors or part-time providers count |
| Per-facility | One monthly fee per location | Dedicated OTPs | Multi-site expansion can trigger new fees |
| Census-based | Cost scales with active patient count | Growing OTPs | Success can increase software cost |
| Module-based | Base EMR plus add-ons | Clinics that want phased rollout | Base price may exclude OTP-critical features |
| Billing-integrated | Software cost tied to RCM/billing | Clinics wanting EMR + billing together | Verify collection percentage and contract terms |
| Enterprise custom | Negotiated contract | Large multi-site networks | Less transparent and often higher implementation cost |
The most common combination in dedicated OTPs is per-provider subscription + billing-integrated pricing — which is also why methadone clinic software cost per provider and OTP EMR total cost of ownership are the two questions every buyer should bring to a demo.
What is included in methadone clinic software pricing?
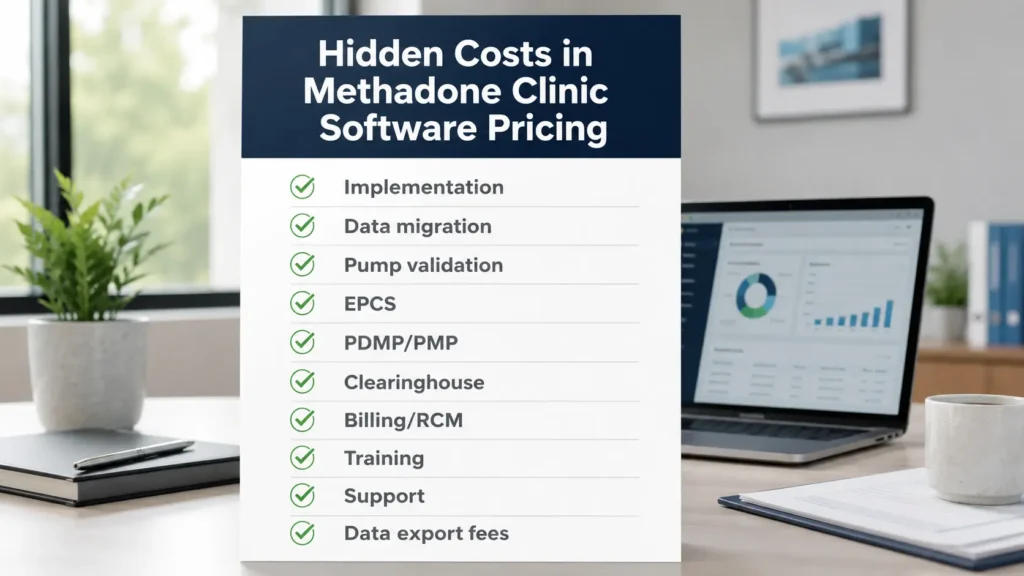
Before comparing vendor quotes, name the line items. Every OTP EMR contract has some combination of these — and the ones a vendor doesn’t list on their website are usually the ones that move the total cost by 20–40%.
1. Monthly subscription — Charged per user, per provider, per active patient, per location, or as a flat platform license. Per-provider is most common for OTPs; per-active-patient is the most punitive structure if your census grows.
2. Implementation fee — One-time. Covers project management, data migration, configuration, training, testing, and go-live support. Typical range: $5,000–$50,000+ for OTPs depending on pump validation, multi-site rollout, and data complexity.
3. Pump validation — OTP-specific. Charged when the EMR integrates with MethaSpense, SciLog, or IVEK pumps. Includes hardware verification, dose-to-chart testing, and FDA-compliant validation documentation. Often $2,500–$10,000+ per site. For clinics evaluating dosing, MethaSpense/SciLog sync, and compliance workflows, see the full OTP Methadone EMR overview.
4. EPCS / e-prescribing — Required for Schedule II buprenorphine and naltrexone prescribing. Some platforms include EPCS; others charge $50–$150 per provider per month.
5. State PDMP / PMP / MAPS integration — May be native, API-based, or a paid add-on. Some clinics pay $100–$500 per month per integrated state.
6. Clearinghouse / billing setup — If the EMR includes billing, the clearinghouse may be bundled or charged separately at $100–$400/month.
7. Patient portal / patient app — Often a separate per-patient or flat monthly fee. $50–$500/month.
8. Training — Initial training is usually included in implementation. Refresher training, new-hire training, and certification programs may be extra at $500–$5,000 per session.
9. Support tier — Standard support is included. Premium 24/7 support, dedicated account manager, and SLA guarantees usually cost more.
10. RCM / billing services — If the EMR vendor also handles billing, expect 4–10% of collections. Specialized OTP billing services (like EliteMed’s OTP billing services) typically run lower — around 2.85% of collections — because OTP-specialized billing has higher clean-claim rates.
11. Custom integrations — Lab interfaces, accounting integrations (QuickBooks, Sage), HR systems. $1,000–$10,000 per integration.
12. Annual price increases — Most multi-year contracts include 3–7% annual escalators. Read this clause carefully.
13. Exit / data export fees — Some vendors charge thousands to export your data when you leave. Get this in writing before signing.
OTP EMR pricing comparison 2026 — seven platforms
This table shows the public pricing signals for the seven OTP/MAT platforms most methadone clinics shortlist. Every number requires verification with the vendor; OTP pricing is custom in nearly every case. The “Pricing Confidence” column reflects how reliable each signal is — vendors with custom enterprise quotes and no published rates have low pricing confidence, while vendors who publish rates publicly or disclose them during the demo have higher confidence.
| Platform | Subscription model | Public price signal (per provider/month) | Implementation fee | Billing model | Pricing Confidence |
|---|---|---|---|---|---|
| MASE OTP EMR | Custom + Growth Bridge (eligible OTPs may qualify for reduced or covered subscription) | $0 (Growth Bridge) – $600 | Flat fee, disclosed on demo | EliteMed billing at 2.85% of collections (optional, OTP-specialized) | Medium — disclosed during demo |
| AZZLY Rize | Per-provider subscription | Quote-based, not published | Quote-based | Built-in RCM, % of collections varies | Low — not publicly listed |
| Kipu Health | Tiered enterprise license | $300–$1,500+ (per signals, varies by tier) | Custom, often $10,000+ | Integrated RCM, fee % varies | Medium-low — third-party signals |
| Behave Health | Bundled CRM/EHR/RCM/ERP | Quote-based, not published | Quote-based | Unified RCM included | Low — not publicly listed |
| ClinicTracker | Per-user, transparent | ~$70/user/month (public signal) | Custom | Built-in billing | Medium — public signals |
| Alleva | Quote-based | Premium tier, quote-based | Custom | Integrated RCM | Low — not publicly listed |
| Netsmart / Methasoft | Enterprise license | Custom, often $1,000+ per provider equivalent | Often $25,000+ | Plexus RCM | Low — not publicly listed |
How to read this table: Subscription is only one of 13 cost lines. A $70/user platform with $500/month in add-ons, separate billing, and a high denial rate can cost more than a $600/provider platform that bundles everything. Always evaluate 3-year TCO and 3-year revenue impact, not just subscription.
For deeper feature-by-feature comparison, see our best OTP EMR software guide. For a detailed AZZLY Rize alternative analysis specifically, see our dedicated post.
Comparing quotes from MASE, AZZLY, Kipu, Methasoft, or Behave?
Ask for a written 3-year TCO breakdown before you sign. EliteMed can help you compare EMR + billing costs side by side.
The hidden costs vendors don’t advertise
Most OTP buyers underestimate three categories. These are where pricing surprises happen.
1. OTP-specific implementation costs
OTP implementation is more expensive than general behavioral health implementation for three reasons. Pump validation requires FDA-compliant testing of the EMR-to-pump bidirectional sync. Inventory migration from your bulk methadone records to digital DEA Form 222 workflows takes time and audit verification. And 42 CFR Part 2 consent mapping (re-papering existing patients into the new system’s consent architecture) is mandatory and often labor-intensive.
A pure behavioral health EMR may go live in 30–60 days for $10,000. An OTP EMR with full pump validation, DEA workflow setup, take-home configuration, and 42 CFR Part 2 segmentation can take 60–120 days and cost $25,000–$75,000+ before subscription begins.
Ask every vendor: Is pump validation included in implementation? Who pays for FDA validation documentation? What’s the timeline before billing turns on?
2. Billing leakage
This is the largest hidden cost in OTP software — and it’s almost never on the vendor proposal.
A 200-patient methadone clinic billing Medicare bundle code G2067 at roughly $230/week per patient generates approximately $2.39 million/year in gross charges. Even a 5% denial-and-rework rate on this base equals ~$120,000/year in unrecovered revenue. A 10% denial rate plus unbilled take-home add-ons (G2078) can leak $200,000–$350,000/year.
If your EMR’s billing layer can’t validate clean claims at submission, automatically roll seven daily doses into one weekly OTP bundle, attach the right modifiers for commercial take-homes, and track prior auth on Sublocade/Vivitrol — you’re paying for that gap whether or not it appears on a contract line.
This is why OTP-specialized billing (like EliteMed’s OTP revenue cycle management) often pays for itself in the first 90 days even at 2.85% of collections — the clean-claim rate is higher than generic RCM.
See CMS OTP billing and payment rules for the official Medicare bundle definitions. Verify your software handles the current code set.
3. Compliance and audit-related cost
The third hidden cost is what your software does not do for compliance. If your platform can’t generate a clean DEA Form 222 reconciliation report on demand, can’t produce an audit-ready 42 CFR Part 2 consent log, or can’t show callback history when a state regulator asks — you’ll spend $5,000–$50,000+ on consulting, remediation, or in extreme cases lost SAMHSA certification.
Refer to SAMHSA OTP certification and regulatory guidance for current accreditation requirements. The software you choose is responsible for keeping these workflows audit-ready every day, not just at survey time.
MASE Growth Bridge — what it is, who qualifies, what it isn’t
Growth Bridge is the most-asked-about line item in MASE pricing conversations, and the one most often misunderstood. Here is the honest version.
What it is: A commercial program designed for eligible OTPs where MASE may reduce or cover the monthly EMR subscription cost for an initial period, in exchange for the clinic adopting EliteMed Financials’ OTP billing services at 2.85% of collections.
Why it exists: OTPs that can’t justify a $400–$900/month per-provider EMR fee tend to stay on outdated systems — which costs them more in compliance risk, denials, and operational drag than the EMR itself ever would. Growth Bridge removes the software cost barrier so the clinic can modernize without a large upfront subscription line. It is designed for clinics evaluating an OTP EMR and billing solution together, not just standalone software.
It is not a loan. There is no principal, no interest, no repayment schedule, and no debt obligation. It is a commercial arrangement where the EMR subscription cost is offset by the value of the billing partnership.
Who typically qualifies: Standalone methadone clinics. New OTPs in their first 24 months of operation. Existing OTPs migrating from outdated or unsupported systems. Clinics adopting MASE EMR and EliteMed billing as a bundled solution. Multi-site organizations may qualify with a custom structure.
Who typically does not qualify: Clinics that already use a competing billing service and want to keep it. Programs where MASE EMR is not a workflow fit (e.g., pure residential treatment with no methadone). Clinics that want EMR-only with no billing partnership.
What you should ask during your demo:
- What’s the eligibility criteria for my clinic’s census and structure?
- What’s the term length of the Growth Bridge agreement?
- What happens if I decide to switch billing providers mid-term?
- What’s the standard subscription rate I’d return to after Growth Bridge ends, if it ends?
- Is the offer documented in writing in the master service agreement?
If a vendor program ever sounds too good to be true, the right response is to read the contract carefully — not to walk away. Growth Bridge is structured, conditional, and disclosed in writing. Ask for the terms before you sign.
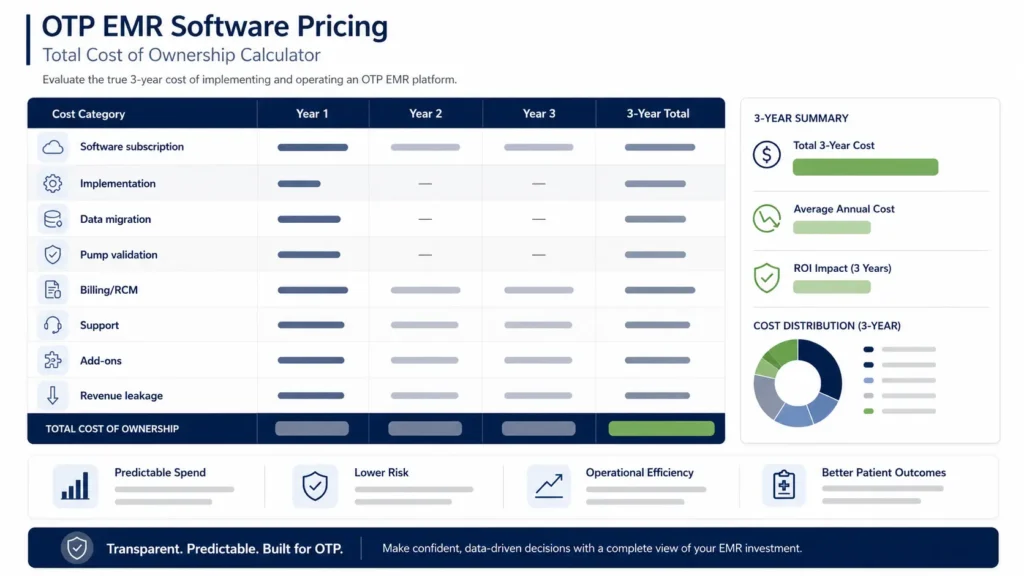
3-year total cost of ownership — worked example
Let’s model a representative methadone clinic and run the math.
Clinic profile:
- 200 active patients
- 3 prescribers (1 MD, 2 NP/PA equivalents)
- 1 dispensing site
- Medicare + Medicaid + 3 commercial payers
- ~$2.4M annual gross OTP billing
- Migrating from a legacy system
Scenario A: Generic Behavioral Health EMR + Outsourced Billing
| Cost Line | Year 1 | Year 2 | Year 3 | 3-Year Total |
|---|---|---|---|---|
| EMR subscription (per provider, $500/mo × 3) | $18,000 | $18,540 | $19,096 | $55,636 |
| Implementation + pump validation | $35,000 | – | – | $35,000 |
| EPCS / PDMP / clearinghouse | $4,800 | $4,944 | $5,092 | $14,836 |
| Patient portal + integrations | $3,600 | $3,708 | $3,819 | $11,127 |
| Training (refresher + new hires) | $1,500 | $2,000 | $2,000 | $5,500 |
| Outsourced billing at 6.5% of $2.4M | $156,000 | $160,680 | $165,500 | $482,180 |
| Estimated billing leakage at 7% denial/under-billing | $168,000 | $173,040 | $178,231 | $519,271 |
| 3-Year Total Cost | $386,900 | $362,912 | $373,738 | $1,123,550 |
Scenario B: MASE EMR + EliteMed Billing (with Growth Bridge eligibility)
| Cost Line | Year 1 | Year 2 | Year 3 | 3-Year Total |
|---|---|---|---|---|
| EMR subscription (Growth Bridge offset, illustrative) | $0–$7,200 | $14,400+ | $14,832+ | $29,232–$36,432+ |
| Implementation + pump validation (flat) | $18,000–$25,000 | – | – | $18,000–$25,000 |
| EPCS / PDMP / native integrations | Included | Included | Included | Included |
| Patient portal + integrations | Included | Included | Included | Included |
| Training | Included in implementation | $1,000 | $1,000 | $2,000+ |
| EliteMed billing at 2.85% of $2.4M | $68,400 | $70,452 | $72,566 | $211,418 |
| Estimated billing leakage at 2% (OTP-specialized billing) | $48,000 | $49,440 | $50,923 | $148,363 |
| 3-Year Total Cost | $134,400–$148,600 | $135,292+ | $139,321+ | $408,013–$423,213+ |
In this illustrative scenario, the difference between the two models exceeds $700,000 over three years. Your actual savings may be higher, lower, or nonexistent depending on payer mix, denial rate, billing performance, implementation cost, and Growth Bridge eligibility. The savings come less from the subscription difference and more from the billing leakage gap — the difference between specialized OTP billing and generic RCM.
Important caveats: Every clinic’s economics are different. Denial rates depend on payer mix, documentation quality, and prior auth processes. Implementation cost depends on pump count, site count, and migration complexity. Growth Bridge eligibility is determined per clinic. Use this model as a structure to plug your own numbers into — not as a quote.
Quick OTP EMR cost calculator
Use this simple formula before comparing vendors:
3-Year Cost = Software subscription
- implementation
- data migration
- pump validation
- EPCS / PDMP / clearinghouse
- support / training
- billing fees (or RCM percentage of collections)
- estimated revenue leakage from denials and missed bundle billing
- exit or data export fees
Then compare that number against the revenue improvement you expect from cleaner claims, faster workflows, fewer missed take-home charges, and lower compliance risk. If the revenue improvement on $2M+ annual billing exceeds the 3-year cost difference between two vendors, the more expensive subscription is often the cheaper total decision.
ROI math: when does new software pay for itself?
For most methadone clinics shopping between EMRs, the dominant ROI lever is not subscription — it’s clean claim rate × payer mix × patient census.
Here’s a simplified ROI worksheet:
Step 1: Calculate your current weekly methadone revenue. Active patients × average weekly bundle rate. For a 200-patient clinic billing primarily Medicare/Medicaid OTP bundles, this is roughly $45,000–$52,000/week.
Step 2: Estimate your current denial/under-billing rate. Pull 90 days of remits. Divide unrecovered/denied/under-billed amount by total billed. Most clinics on generic billing run 6–12%; OTP-specialized billing typically runs 2–5%.
Step 3: Calculate the recovery delta. If your denial rate drops from 8% to 3%, that’s a 5% revenue lift. On $2.4M annual billing, that’s $120,000/year in newly captured revenue.
Step 4: Subtract the cost of the change. New EMR subscription delta + new billing service delta + implementation amortized over 36 months.
For most OTPs in the 150–350-patient range, the breakeven on switching to OTP-specialized software + billing is somewhere between month 4 and month 9. After that, the entire revenue lift is contribution margin.
This is why pricing alone is the wrong lens. 3-year revenue impact is the right one.

Want a real ROI estimate for your clinic?
Book a 15-minute MASE pricing discussion · Review software cost, billing model, implementation, and revenue-cycle opportunity
Pricing red flags — what to push back on before signing
Use this checklist when reviewing any OTP EMR proposal. Any of these warrant a conversation before you sign.
1. Per-active-patient pricing without a cap. If your census grows from 200 to 350 patients, your subscription cost should not grow proportionally. Negotiate a cap or move to per-provider pricing.
2. Implementation fees that aren’t fixed. “Time and materials” implementation contracts almost always exceed the initial estimate by 30–80%. Demand a fixed-fee implementation with a defined scope.
3. Pump validation as a billable extra. OTP-specific software should treat pump validation as a core capability, not an upcharge per pump model.
4. EPCS, PDMP, or clearinghouse as separate line items. These are not “premium features” for an OTP — they’re table-stakes. They should be in the base subscription.
5. Annual price escalators above 5%. Negotiate down. CPI + 2% is reasonable. 7%+ compounds aggressively over three years.
6. Exit / data export fees. Get these in writing. Some vendors charge $5,000–$15,000 to export your patient data when you leave. This is anti-competitive but legal.
7. Multi-year lock-ins without performance SLAs. If you’re committing to a three-year term, the vendor should commit to uptime, support response time, and clean-claim rate. Reciprocity matters.
8. Vague “custom pricing” with no written quote. If the salesperson won’t put pricing in writing after a demo, you haven’t seen pricing. Walk away or escalate.
9. Bundle pricing that hides the components. Demand a line-item breakdown: subscription, implementation, integrations, billing, support. If they can’t break it down, they don’t want you to compare.
10. Billing services without OTP specialization. A general medical biller charging 5% of $2.4M ($120,000/year) with a 10% denial rate is more expensive than an OTP-specialized biller at 2.85% with a 3% denial rate. Math wins.
FAQ: OTP EMR pricing in 2026
How much does OTP EMR software cost on average?
Most dedicated OTPs spend $400–$900 per provider per month on EMR subscription, plus $5,000–$50,000+ one-time implementation, plus 3–8% of collections for billing if outsourced. A 200-patient, 3-prescriber clinic typically runs $250,000–$400,000+ over three years for software and billing combined. Specialized solutions with Growth Bridge eligibility can substantially reduce the subscription line.
Is MASE Growth Bridge a loan or financing program?
No. Growth Bridge is not a loan. There is no principal, interest, or repayment schedule. It is a commercial program where the EMR subscription cost may be reduced or covered for eligible OTPs that adopt EliteMed Financials’ OTP billing services at 2.85% of collections. The arrangement is documented in the master service agreement before signing.
What hidden fees should I watch for in an OTP EMR contract?
Watch for implementation overages, pump validation upcharges, separate EPCS and PDMP fees, clearinghouse charges, training fees beyond initial setup, multi-year price escalators above 5%, exit/data export fees, and per-active-patient pricing without caps. Always demand a line-item proposal and a written 3-year TCO before signing.
How does pricing compare between MASE, AZZLY Rize, Kipu, and Methasoft?
MASE offers the most transparent pricing structure with a flat implementation fee, optional Growth Bridge eligibility, and EliteMed billing at 2.85% of collections. AZZLY Rize, Kipu, and Methasoft all use quote-based custom pricing without published rates — typical signals range from $300/provider/month entry to $1,500+/provider/month for enterprise tiers. Implementation for legacy enterprise platforms can exceed $25,000–$75,000+ for larger OTPs.
Does billing cost more than the EMR itself?
For most OTPs, yes — by a wide margin. A clinic billing $2.4M annually at a 6.5% billing fee pays $156,000/year just in billing service charges, compared to $18,000–$36,000/year in EMR subscription. This is why OTP-specialized billing at 2.85% (saving roughly $87,000/year) often pays for the entire EMR program by itself.
Can I negotiate OTP EMR pricing, or is it fixed?
Pricing is almost always negotiable. Subscription rate, implementation fee, training, annual escalator percentage, contract term, exit clauses, and bundled add-ons are all commonly negotiated. The strongest leverage points are committing to a longer term in exchange for a lower rate, bundling EMR + billing with one vendor, and asking for multi-site discounts if you operate more than one location. Get every concession in writing.
Is OTP EMR pricing usually per user, provider, facility, or patient census?
OTP EMR pricing can use any of these models. Smaller behavioral health tools often use per-user pricing, medical systems may use per-provider pricing, dedicated OTP systems may use per-facility or census-based pricing, and enterprise vendors usually quote custom contracts. Ask every vendor how they define users, providers, active patients, and locations before comparing quotes — two vendors can quote the same monthly number using different definitions and produce wildly different invoices in year two.
What is the cheapest OTP EMR software?
The cheapest OTP EMR is not always the lowest-cost option. A low monthly subscription can become expensive if dosing, pump integration, billing, support, implementation, EPCS, PDMP, or data export are charged separately. ClinicTracker publishes around $70/user/month, which is among the more transparent low-end signals, but full OTP compliance often requires modules and add-ons that are not in the base price. Clinics should compare three-year total cost of ownership and billing impact, not only the starting subscription.
Bottom line
Methadone clinic software pricing in 2026 ranges from $0 (with Growth Bridge eligibility) to $1,500+/month per provider. But the right comparison is never subscription alone — it’s 3-year total cost of ownership including billing impact and avoided revenue leakage.
The biggest dollar lever in OTP software is not the EMR line — it’s the clean claim rate on $2M+ in annual billing. A 5-point swing in denial rate is worth more than the entire EMR subscription, every year.
If your clinic is comparing quotes, demand a line-item proposal, run a 3-year TCO with your actual billing volume, and ask every vendor for their OTP-specific clean claim rate before signing. That single question filters out most of the noise.
For clinics where MASE EMR + EliteMed billing is a workflow fit, Growth Bridge eligibility is worth confirming as part of the conversation. If the structure works, the math typically works.
Reviewed by: EliteMed Financials Revenue Cycle Team
Why trust this guide: EliteMed Financials works with behavioral health and OTP billing workflows and partners with MASE Behavioral Health EMR. This guide discloses that partnership and uses publicly available vendor pricing signals where competitor costs are discussed. All TCO and ROI examples are illustrative models — your clinic’s actual numbers will differ based on census, payer mix, denial rate, and contract terms.
Last updated: May 2026 · Next scheduled review: November 2026
Sources cited: CMS OTP billing and payment rules; SAMHSA OTP certification and regulatory guidance; Capterra, G2, GetApp, Software Advice public pricing signals; vendor product and pricing pages; analyst databases as of May 2026.
EliteMed Financials LLC is the billing partner for MASE Behavioral Health EMR. Pricing signals in this article are publicly available estimates as of May 2026 and require verification with each vendor. Numbers are not quotes. Growth Bridge eligibility is determined per clinic and disclosed in writing during the demo and proposal process. This article does not constitute legal, financial, billing, or compliance advice.

