Why OTP clinics need a different type of EMR in 2026
If you run a methadone clinic, you already know: your EMR decision is not the same decision a therapist’s office or a residential treatment center makes.
Every morning, your clinic dispenses Schedule II controlled substances through calibrated pumps to hundreds of patients in a 4-hour dosing window. You manage take-home medications under the 2024 SAMHSA Final Rule’s expanded flexibility tiers. You run random callbacks tied to a Diversion Control Plan. You track serialized bottles. You reconcile DEA Form 222 inventory against bulk tank levels. You document care under 42 CFR Part 2 privacy rules that are stricter than HIPAA. And you bill weekly OTP bundles that most billers have never seen.
A behavioral health EMR can chart the visit. An OTP EMR needs to run the operation.
This buyer’s guide compares the leading OTP EMR platforms in 2026 across the capabilities that actually matter for methadone clinics: dosing-window workflows, pump integration, take-home tracking, diversion controls, DEA/SAMHSA compliance, billing, AI documentation, pricing, and implementation. We rank by OTP-specific depth — not generic feature lists.
What this guide covers: We review MASE Behavioral Health EMR, Behave Health, Kipu Health, AZZLY Rize, ClinicTracker, Alleva, ZenCharts, Netsmart/Netalytics/Methasoft, and Sunwave/Lightning Step. Every claim is based on publicly available product documentation, review platforms, and our workflow analysis as of May 2026. Where we could not verify a capability, we say so.
That is why many searches for “best addiction treatment EMR” or “substance abuse EMR software” do not fully answer the needs of a dedicated OTP. Methadone clinics need a more specialized opioid treatment program software category — and this guide covers it.

Who this guide is for
This guide is for OTP owners, executive directors, medical directors, compliance officers, nursing directors, billing managers, and operations leaders comparing EMR software for methadone or MAT programs.
It is especially useful for startup methadone clinics choosing their first EMR, established OTPs switching from outdated systems, clinics adding MAT/OTP workflows to behavioral health programs, and operators comparing MASE, AZZLY Rize, Kipu, Behave Health, ClinicTracker, Alleva, ZenCharts, Netsmart/Methasoft, and Sunwave/Lightning Step.
This guide is not for patients looking for a methadone clinic near them. It is written for clinic decision-makers evaluating software.
How we ranked the best OTP EMR software
We scored platforms across seven evaluation factors weighted by their impact on daily methadone clinic operations. This is not a generic feature-count ranking — it is weighted toward the workflows that carry the highest operational and regulatory risk for OTPs.
| Evaluation Factor | Weight |
|---|---|
| OTP dosing and dispensing workflows | 25% |
| Compliance and controlled-substance workflows | 20% |
| Billing / RCM integration | 15% |
| Implementation and migration support | 15% |
| AI, reporting, and operational visibility | 10% |
| Pricing transparency and total cost | 10% |
| Public proof / market validation | 5% |
Platforms with native OTP dispensing, pump integration, and compliance automation score highest. Platforms that require workarounds, bolt-on modules, or manual processes for core OTP workflows score lower — regardless of how strong their general behavioral health features are.
All competitor claims in this guide are based on publicly available vendor documentation, review platforms, and market research. Where we could not verify a capability from public sources, we note “in the public materials we analyzed, we did not find clear documentation of…” rather than stating the feature is absent. Buyers should verify all claims directly during vendor demos.
What is the best OTP EMR software in 2026?
There is no single best OTP EMR for every clinic. The right choice depends on your daily census, pump hardware, level-of-care mix, billing complexity, and tolerance for implementation downtime.
For dedicated methadone clinics, MASE Behavioral Health EMR earns our top recommendation because it combines native MethaSpense/SciLog pump synchronization, facial biometric verification with geofencing, digital callback automation, serialized bottle tracking with QR verification, real-time DEA Form 222 workflows, 42 CFR Part 2 native architecture, and optional EliteMed billing at 2.85% of collections — in one connected system built for OTP from day one.
For broader MAT programs, Behave Health and AZZLY Rize offer strong all-in-one platforms. For enterprise networks, Kipu Health and Netsmart/Methasoft provide scale. For AI documentation, Alleva leads. For residential treatment, ZenCharts and Kipu are strongest.
The best OTP EMR is the one that protects your dosing window, automates your compliance workflows, and supports the controlled-substance accountability your DEA registration depends on. Book demos with your shortlisted vendors, bring your compliance officer, and test with your actual pumps.
If you are looking for software plus billing support together, see our complete OTP clinic software solution.
What is an OTP EMR?
An OTP EMR is specialized software built for Opioid Treatment Programs — the federally regulated clinics that dispense methadone and other medications for opioid use disorder. It is a specialized form of addiction treatment EHR or MAT EHR software, but it goes deeper into methadone dispensing, take-home management, and controlled-substance accountability than broader SUD EMR or substance abuse EMR software categories. Unlike a general behavioral health EMR or a MAT EHR designed for office-based buprenorphine prescribing, an OTP EMR manages clinical documentation and medication dispensing operations, controlled-substance inventory, diversion controls, and OTP-specific billing in one platform.
The distinction matters because methadone clinics are not documentation-first businesses. They are dispensing-first businesses with documentation requirements. The dosing window is the operational bottleneck. If the software cannot manage the pump, track the bottles, automate the callbacks, reconcile the inventory, and generate an audit-ready DEA package — it is probably not a true OTP EMR. It is a behavioral health EMR with a methadone module bolted on.
OTP EMR vs MAT EHR vs behavioral health EMR:
- OTP EMR = narrowest and most regulated. Manages on-site liquid methadone dispensing, pump integration, controlled-substance inventory, take-home tracking, callbacks, DEA Form 222, and 42 CFR Part 2. Built for daily observed dosing clinics.
- MAT EHR = broader. Often supports buprenorphine prescribing, naltrexone, and office-based opioid treatment (OBOT). Prescriptions are typically filled at pharmacies, not dispensed on-site. Less daily structure required.
- Behavioral health EMR = broadest. Covers residential, outpatient, PHP/IOP, counseling, group therapy, and general SUD treatment. May include MAT modules. Rarely includes native pump integration or methadone-specific dispensing workflows.
If your clinic physically dispenses methadone daily, you need an OTP EMR — not a behavioral health EMR with SUD features.
What methadone clinics should look for in OTP EMR software
Before comparing vendors, define your non-negotiables. These are the 10 capabilities that separate purpose-built OTP software from general behavioral health platforms.
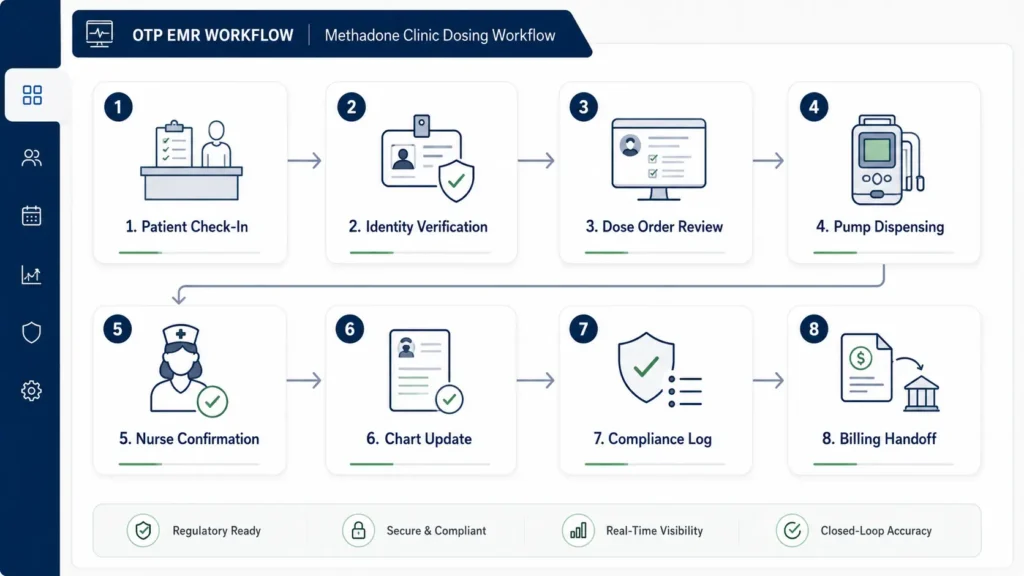
1. Dosing-window workflow
The morning dosing line is the critical path. The software should handle patient check-in, identity verification, vital signs, dose order review, pump-assisted dispensing, immediate chart logging with nurse signature and timestamp, and exception handling — all without double entry. Ask vendors: “Walk me through a full morning dosing line for 200 patients.”
2. Pump integration (MethaSpense / SciLog)
The EMR should communicate directly with IVEK MethaSpense and SciLog dispensing pumps. Real-time bidirectional sync means the clinical order goes to the pump, the pump pours, and the chart records the exact dose — no manual typing. Ask: “Does your software send the exact dose to my pump, or do I have to type it twice?”
3. Take-home tracking and bottle serialization
The 2024 SAMHSA Final Rule (89 FR 7528, effective April 2, 2024) expanded take-home flexibility: up to 7 days in the first 14 days of treatment, 14 days from day 15, and 28 days from day 31 per updated 42 CFR § 8.12(i). Software should automate take-home eligibility based on clinical milestones, generate serialized bottle labels (QR or barcode), track bottle returns, and log missed-dose logic. Ask: “How does the system handle bottle logic when a patient misses a dose?”
4. Guest dosing
Guest dosing — when a patient from another OTP doses at your clinic temporarily — should be a single workflow, not a faxed paper packet. Secure verification, dose confirmation, logging, and return reporting to the home clinic should all happen inside the EMR.
5. Diversion controls and callbacks
SAMHSA’s 42 CFR Part 8 requires OTPs to maintain a Diversion Control Plan. Software should automate random callback selection, SMS notification, bottle-count scheduling, result logging, and missed-callback alerts. Facial biometric verification and geofencing at the dosing window add an identity layer beyond passwords. Ask: “How do you prevent a patient from using someone else’s ID during a 5 AM rush?”
6. DEA Form 222 and controlled-substance inventory
The EMR should track Schedule II methadone ordering via DEA Form 222 (digital or paper, with CSOS as the electronic ordering option), reconcile received inventory against bulk tank levels, and generate a bulk-to-dose report for DEA audits. Ask: “Can I reconcile my bulk inventory receipt directly into the system using a Form 222 log?”
7. PMP/PDMP/MAPS integration
State Prescription Drug Monitoring Program checks should be in-chart — not a separate browser tab. Verify whether integration is native, API-based, or a paid add-on, and whether it covers your specific state(s).
8. 42 CFR Part 2 privacy architecture
42 CFR Part 2 governs the confidentiality of substance use disorder treatment records and is stricter than standard HIPAA. The EMR should enforce consent management, record segmentation, redisclosure controls, audit trails, and role-based access as a platform foundation — not a checkbox setting.
9. OTP billing and RCM
OTP billing is not standard CPT billing. Medicare uses weekly bundle codes (G2067 for methadone episodes of care, G2078 for take-home methadone add-ons). Medicaid varies by state. Commercial payers use H0020 and H0033. The EMR should automatically roll daily dosing, counseling, and labs into clean weekly claims. Ask: “Does the system automatically roll daily dosing and counseling into a weekly claim?”
10. AI documentation and clinical guidance
AI in OTP EMR ranges from post-visit note scribing (Alleva’s TravisAI, Kipu AI Scribe, Lightning Step’s LIA) to real-time clinical guidance during the encounter (MASE). Verify whether AI understands MAT-specific terminology like induction, withdrawal symptoms, take-home eligibility, and QTc risk — not just generic medical language. <!– 📸 IMAGE: Buyer checklist infographic — “10 Things Methadone Clinics Should Verify Before Choosing an OTP EMR.” Alt: “OTP EMR buyer checklist for methadone clinics — 10 features to verify” –>
Regulatory note: OTP regulations, DEA guidance, SAMHSA accreditation standards, CMS billing rules, and state Medicaid policies can change. Always verify current SAMHSA, DEA, CMS, state Medicaid, and state OTP requirements with the relevant agency before making software or billing decisions. This guide does not constitute regulatory, clinical, or billing advice.

Best OTP EMR software in 2026: top platforms reviewed
We reviewed nine platforms that serve OTP/methadone clinics. Each review covers the platform’s OTP-specific strengths, documented weaknesses, best-fit buyer, and what to verify during the demo. Platforms are presented in order of OTP-native depth for dedicated methadone clinics.
1. MASE Behavioral Health EMR — Best Overall for Dedicated Methadone Clinics
What it is: A purpose-built OTP EMR designed from day one for opioid treatment programs and methadone clinics — not adapted from a behavioral health platform.
OTP-specific strengths: Native real-time MethaSpense + SciLog pump synchronization (dose-to-chart with no double entry), facial biometric verification combined with geofencing at the dosing window, digital callback policy automation (SMS + scheduling + chart logging), serialized bottle tracking with QR verification, diversion risk scoring that combines callbacks, bottles, toxicology, and dosing patterns, real-time digital DEA Form 222 workflows with inventory reconciliation, PMP/MAPS integration, 42 CFR Part 2 native architecture, and AI clinical guidance during the encounter (not just post-visit notes).
Billing: Pairs with EliteMed Financials’ OTP billing services at 2.85% of collections — H0020/H0033 weekly bundle billing, Medicare G-codes (G2067–G2080), Sublocade/Vivitrol prior auth, and 50-state Medicaid coverage.
Pricing: MASE pricing is structured around clinic size, provider count, implementation scope, and pump configuration. Eligible OTPs may qualify for Growth Bridge support that can reduce or cover the EMR subscription for an initial period. EliteMed billing is available at 2.85% of collections. Request a written quote for monthly software, implementation, migration, pump validation, support, and billing fees.
Implementation: 14–30 days for standard OTP configurations. Includes pump validation, data migration, staff training, parallel run, and onsite go-live support.
Weaknesses to verify: Newer entrant with limited third-party review volume. Enterprise scale for very large networks (50+ sites) should be confirmed. Detailed EPCS and state-by-state PDMP connectivity should be verified during demo.
Best for: Standalone methadone clinics, small-to-mid-size dedicated OTPs, high-compliance programs, clinics needing pump/dosing automation, clinics exploring Growth Bridge eligibility.
2. Behave Health — Best All-in-One MAT/OBOT Platform
What it is: Modern all-in-one CRM + EHR + RCM + ERP platform for behavioral health and addiction treatment. Cloud-native with strong operational tooling.
OTP-specific strengths: Unified CRM/EHR/RCM/ERP in one platform, DrFirst EPCS integration, medication administration records (eMAR), take-home tracking, dosing schedules, insurance verification, case management, staff performance dashboards, and SmartNotes clinical observation tools.
Weaknesses to verify: In the public materials we analyzed, we did not find clear documentation of native MethaSpense/SciLog pump synchronization. OTP-native features are not highlighted as core differentiators. Serialized bottle depth and digital DEA Form 222 workflows require verification during demo.
Best for: MAT/OBOT clinics prioritizing consolidated operations, mixed-level-of-care programs, digital-first clinics wanting unified CRM + billing + clinical in one vendor.
3. AZZLY Rize — Best Known Addiction Treatment EMR with MAT Support
What it is: Cloud-based EHR/PM/RCM on Microsoft Azure, purpose-built for behavioral health and addiction treatment. ONC-certified. 3.9/5 across 69+ reviews. Customer support rated 4.2/5.
OTP-specific strengths: Medication Outpatient Records (MORs) for MAT workflows, methadone/buprenorphine/naltrexone tracking, configurable templates, rules-based auto-coding, built-in clearinghouse integration, patient portal, and integrated RCM. Strong customer support reputation.
Weaknesses to verify: In the public materials and review pages we analyzed, we did not find clear documentation of native MethaSpense/SciLog synchronization, facial biometric verification, digital callback automation, or serialized bottle tracking. Performance complaints (slow loading, dated UI) appear in Capterra/Software Advice reviews. Buyers should verify these OTP-specific workflows directly during a demo. For a detailed AZZLY Rize alternative comparison, see our dedicated analysis.
Best for: Mid-size outpatient addiction treatment programs, clinics adding MAT to existing behavioral health operations, organizations valuing strong customer support and billing integration.
4. Kipu Health — Best for Large Behavioral Health Networks
What it is: One of the largest addiction-treatment-specific EMR platforms. Originally residential-first, now includes dedicated MAT modules with Pump Konnectors for SciLog/IVEK pump support.
OTP-specific strengths: Kipu Messenger for patient engagement, ASAM CONTINUUM assessments, dedicated MAT module, Kipu references pump connector-style integrations for SciLog/IVEK in some materials (buyers should verify supported pump models, bidirectionality, and real-time dose-to-chart workflow during the demo), configurable diversion controls with SMS callbacks, Kipu AI Scribe for documentation, e-prescribing with EPCS, and deeply integrated RCM.
Weaknesses to verify: Residential-first heritage may add configuration overhead for pure OTP clinics. Can be expensive for solo OTPs. Implementation complexity should be assessed. OTP-native dispensing details are not always consistently documented across all public sources.
Best for: Multi-site addiction treatment organizations running residential + detox + MAT + OTP across multiple levels of care. High-growth SUD organizations scaling rapidly.
5. Netsmart / Netalytics / Methasoft — Best Legacy OTP / Enterprise Option
What it is: The legacy OTP specialist. Netsmart acquired Netalytics (Methasoft + SMART platforms) in 2023, bringing them into the Netsmart CareFabric ecosystem. Methasoft has decades of methadone-clinic-specific deployment.
OTP-specific strengths: Established methadone dispensing workflows, dosing pump integration (legacy MethaSpense/SciLog support through Methasoft heritage), fingerprint and iris biometric verification, liquid inventory reconciliation, enterprise reporting and interoperability, Red Flag diversion system, population health analytics, and Plexus RCM.
Weaknesses to verify: UI can feel clinical rather than modern (myAvatar performance concerns in reviews). Implementation can be lengthy and expensive for smaller clinics. Detailed 42 CFR Part 2 segmentation architecture and DEA Form 222 digital automation depth should be verified. Pricing is enterprise-custom with low transparency.
Best for: Large OTP chains (5+ locations), multi-state enterprises, high-volume networks where legacy depth and interoperability outweigh modern UX.
6. ClinicTracker — Best Budget-Conscious MAT Workflow Option
What it is: Customizable behavioral health EHR with strong EPCS focus, practice management, and billing tools. Publicly signals pricing around ~$70/user/month — more transparent than most competitors.
OTP-specific strengths: EPCS with PDMP integration, lab integration, MAT medication tracking, customizable workflows, custom form builders, voice recognition, billing management with complex contract/grants billing, ClinicTracker Connect for unsigned document reminders.
Weaknesses to verify: Not clearly an OTP/methadone specialist. In the public materials we analyzed, we did not find clear documentation of native pump sync. Advanced accountability features (biometrics, callbacks, bottle tracking) require confirmation. Windows heritage in older reviews; cloud functionality at OTP scale should be verified.
Best for: Smaller substance-abuse clinics, budget-conscious MAT programs prioritizing EPCS and practice management, power-user administrators who want deep workflow customization.
7. Alleva — Best for AI Documentation and Patient Engagement
What it is: AI-focused addiction treatment EMR with TravisAI (AI-generated notes), Echo (ambient AI), Alleva Insights (data visualization), and strong patient engagement tools.
OTP-specific strengths: Strongest marketed AI documentation suite among reviewed platforms, deep data visualization with recovery metrics, alumni engagement, mobile app for patient engagement, medication reconciliation, e-prescribing, integrated EMR/CRM/RCM.
Weaknesses to verify: More focused on general SUD/behavioral health than pure methadone dosing. In the public materials we analyzed, OTP-specific workflows, pump integration, biometrics, callbacks, and bottle tracking are not emphasized. AI helps notes but doesn’t necessarily automate dosing operations.
Best for: Premium recovery centers, addiction treatment programs where documentation burden is the top pain point, programs prioritizing patient engagement and long-term outcomes tracking.
8. ZenCharts — Best for Residential Treatment Programs
What it is: Cloud-based EHR built by clinical directors for residential treatment, detox, and SUD programs. Known for intuitive charting, ease of use, and strong customer support.
OTP-specific strengths: Intuitive clinical charting with note-first workflows, real-time Compliance Engine with missing-signature flags, EPCS, CRM + billing tools, faster reimbursements.
Weaknesses to verify: Residential orientation dominant. In the public materials we analyzed, pump integration, advanced diversion automation, and high-volume methadone dispensing workflows are not clearly documented. May not scale for daily OTP volume at high-census clinics.
Best for: Residential addiction treatment programs, mixed addiction programs with simpler MAT, clinics prioritizing ease-of-use and clinician satisfaction over deep OTP automation.
9. Sunwave / Lightning Step — Best SUD Continuum Option
What it is: Post-2025 merger creating a unified CRM/EMR/RCM platform for behavioral health and addiction treatment. Single-database architecture with AI-powered workflows through LIA (Lightning Intelligent Assistant).
OTP-specific strengths: LIA automated charting and AI documentation, medication management, lab and pharmacy integrations, medication administration records, single-database architecture eliminating data silos, unified CRM/EMR/RCM, and documented focus on reducing provider burnout and charting time.
Weaknesses to verify: In the public materials we analyzed, deep OTP pump-specific workflows (MethaSpense/SciLog synchronization) are not clearly documented. Merged product maturity is still evolving. Advanced OTP accountability features (biometrics, callbacks, serialized bottle tracking) should be verified. Invoicing module may be less robust for massive enterprise-scale billing.
Best for: Addiction treatment centers where staff burnout and charting speed are top pain points, broader BH/SUD programs with unified operations needs, organizations where AI-powered documentation is a primary selection criterion.
OTP EMR comparison matrix
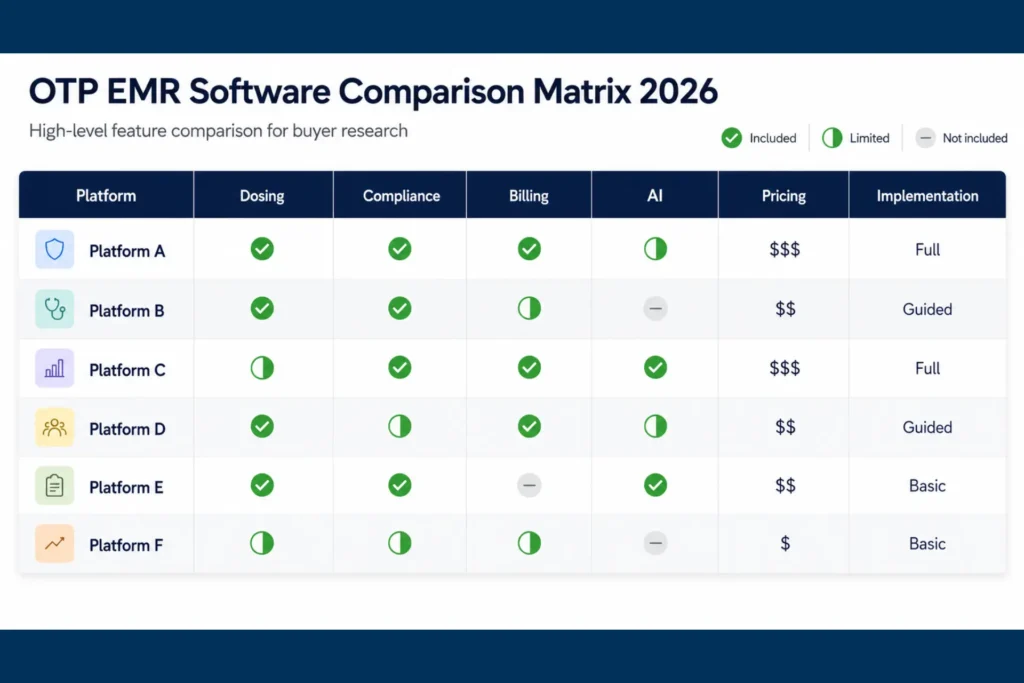
Use this OTP EMR comparison and methadone clinic software comparison to shortlist platforms before booking demos. Then bring it to vendor demos and ask for proof, not promises. <!– TABLE — Create as WordPress Table block. Bold MASE column. –>
| Capability | MASE | Netsmart/Methasoft | Kipu Health | AZZLY Rize | Behave Health | ClinicTracker | Alleva | ZenCharts | Sunwave/Lightning Step |
|---|---|---|---|---|---|---|---|---|---|
| Built for OTP from day one | ✅ OTP-first | ✅ Legacy OTP | ◐ Residential-first + MAT | ◐ BH-first + MAT | ◐ All-in-one BH | ◐ General BH | ◐ AI/SUD-first | ◐ Residential-first | ◐ Merged BH/SUD |
| MethaSpense/SciLog pump sync | ✅ Native real-time | ✅ Legacy support | ◐ Konnectors | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented |
| Facial biometric verification | ✅ Yes | ◐ Fingerprint/iris | ◐ Face/Touch ID | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented |
| Geofencing | ✅ Yes | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented |
| Digital callback automation | ✅ SMS + scheduling | ◐ Limited | ✅ SMS callbacks | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented |
| Serialized bottle/QR tracking | ✅ Yes | ◐ Inventory-level | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented |
| Diversion risk scoring | ✅ Yes | ◐ Red Flag system | ◐ Configurable | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented |
| DEA Form 222 digital | ✅ Yes | ✅ Yes | ◐ EPCS + DEA reporting | ◐ Limited | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented | ❓ Not documented |
| 42 CFR Part 2 native | ✅ Platform foundation | ✅ Yes | ✅ Yes | ✅ Yes | ✅ Yes | ◐ Standard | ✅ Yes | ◐ Standard | ◐ Standard |
| AI documentation | ✅ Clinical guidance | ◐ Limited | ✅ Kipu AI Scribe | ◐ DAX Copilot | ◐ SmartNotes | ◐ Limited | ✅ TravisAI + Echo | ◐ Limited | ✅ LIA |
| Integrated OTP billing | ✅ EliteMed 2.85% | ✅ Plexus RCM | ✅ Integrated/modular | ✅ Rules-based RCM | ✅ Unified RCM | ✅ Built-in | ✅ Integrated | ✅ Included | ✅ Unified |
| Growth Bridge option | ✅ Yes | ❌ No | ❌ No | ❌ No | ❌ No | ❌ No | ❌ No | ❌ No | ❌ No |
| Implementation timeline | 14–30 days | Custom (lengthy) | Custom | Custom | Custom | Custom | Custom | Custom | Custom |
Legend: ✅ = Clearly stated or verified · ◐ = Partial, configurable, or limited detail · ❓ = Not clearly stated in public materials · ❌ = Not offered
Want to test this matrix against your actual workflows?
15-min MASE demo · Bring your pump model numbers · Bring your compliance officer
Feature support is based on public vendor materials and available market research as of May 2026. “Not documented” does not always mean the feature is absent — it means the vendor did not clearly describe it in reviewed materials. No matrix can replace a live demo. Verify pump compatibility, dosing-window speed, DEA workflows, take-home tracking, and billing logic using your own pumps, census, and compliance requirements.
OTP EMR pricing in 2026: what methadone clinics should expect to pay
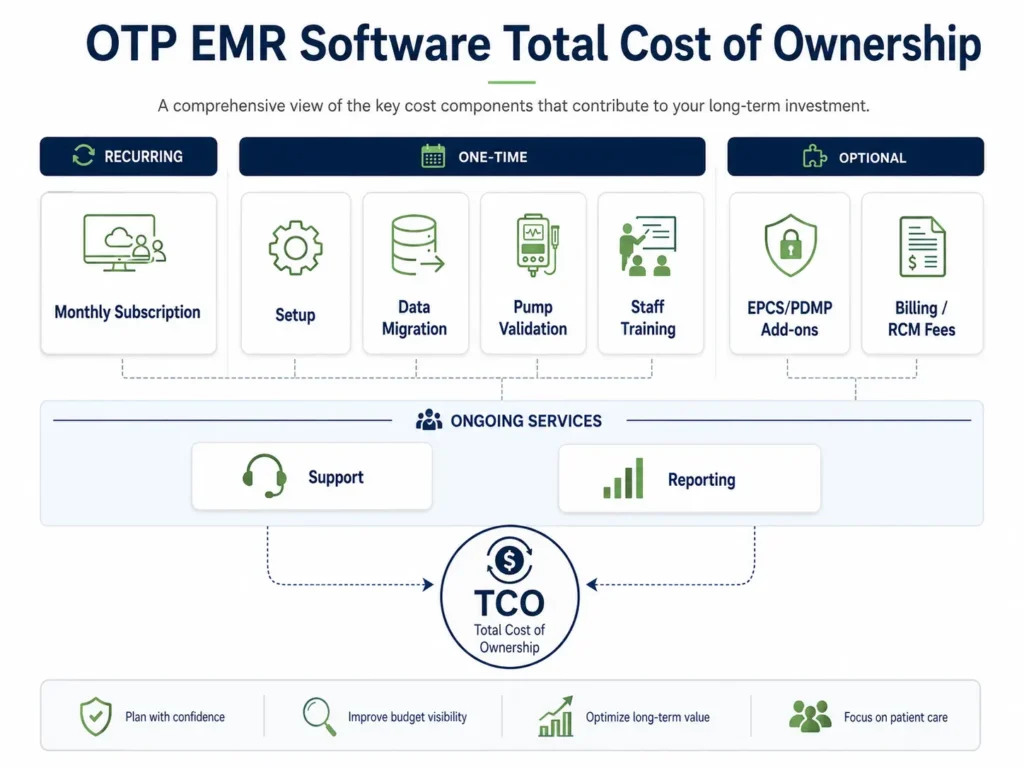
OTP EMR pricing is almost universally quote-based. Direct price comparison is difficult because vendors rarely publish pricing, and the sticker price is often a distraction from the real cost.
What drives the real cost: Integration depth (pump validation, EPCS setup, PDMP connections), implementation and data migration, staff training, support tiers, clearinghouse fees, and RCM/billing fees. A $500/month EMR that requires $50,000 in custom pump integration work is not cheaper than a $1,200/month EMR with native pump sync included.
Pricing signals by vendor (May 2026)
| Vendor | Pricing Model | Public Signals | Implementation | Billing/RCM |
|---|---|---|---|---|
| MASE | Custom subscription + Growth Bridge (eligible OTPs may qualify for reduced/covered subscription) | 2.85% of collections (EliteMed billing) | Flat fee, disclosed on demo | Optional EliteMed 2.85% |
| Netsmart/Methasoft | Enterprise custom | $500–$2,000+/mo signals for small-medium; high implementation | $20k–$300k+ for larger deployments | Plexus RCM or integrated |
| Kipu Health | Custom/enterprise | $200–$600/mo range cited; starts ~$600/mo in some listings | Contact for quote | Integrated or modular |
| AZZLY Rize | Custom per-provider | ~$799+/mo cited in third-party comparisons (unverified) | $5,000–$25,000+ cited | Integrated RCM |
| Behave Health | Custom | No public per-provider numbers | Contact for quote | Included in all-in-one |
| ClinicTracker | Per-user/subscription | ~$70/user/month (most transparent) | Not clearly public | Built-in |
| Alleva | Custom/contract | No public pricing found | Contact for quote | Integrated |
| ZenCharts | Quote-based | $25–$40/mo entry signals (older listings, verify) | Contact for quote | Included |
| Sunwave/Lightning Step | Custom/platform | ~$49/mo all-in-one signals (older listings, verify) | Contact for quote | Unified CRM/EMR/RCM |
Pricing signals are from third-party comparison sites and may be outdated. Request a written quote including total year-one and three-year TCO before committing.
The TCO question every methadone clinic should ask
Before signing, request a line-item breakdown that includes: monthly subscription, implementation/setup fee, data migration, pump validation, EPCS identity proofing, PDMP/PMP connections, clearinghouse fees, RCM/billing percentage, AI modules, reporting add-ons, support tiers, training, and data-export/termination fees. Compare first-year and three-year totals.
A cheap EMR with missing native features can cost more in manual workarounds, denied claims, staff overtime, and audit exposure than a higher-subscription platform that handles those workflows natively.
When to choose each OTP EMR
Not every methadone clinic is the same. Here’s how to match the platform to your operational reality.
Startup methadone clinic (first EMR)
Priority: Fast implementation, low upfront cost, pump validation before first dosing day, scalable compliance tools.
Best fit: MASE (Growth Bridge $0/mo + OTP-native workflows), Behave Health (cloud-native all-in-one), AZZLY Rize (fast cloud deployment + strong billing).
Avoid: Enterprise systems with 6-month implementations and $50k+ setup fees before your first patient.
Established OTP switching systems
Priority: Migration of dosing history, DEA logs, take-home records, pump re-validation, minimal double-entry during cutover.
Best fit: MASE (OTP-native pump sync + structured migration), Netsmart/Methasoft (legacy migration engine + DEA log continuity), Kipu (configurable diversion tools + broader scale).
Avoid: Vendors that cannot demonstrate dosing-history migration or pump re-validation in the demo.
Multi-site OTP network (3+ locations)
Priority: Centralized compliance, enterprise reporting, cross-site guest dosing, corporate templates, multi-site licensing.
Best fit: Kipu (enterprise configurability + multi-site dashboards), Netsmart/Methasoft (legacy OTP depth at scale), Behave Health (unified CRM/EHR/RCM/ERP).
MAT/OBOT clinic (buprenorphine-focused, not daily methadone)
Priority: EPCS, PDMP, patient engagement, mobile app, prescription workflows — not daily pump-assisted dosing.
Best fit: Behave Health, AZZLY Rize, Alleva, ClinicTracker. These handle prescription-based MAT without the cost of pump-heavy OTP features.
Avoid: Overbuying a legacy OTP system if you don’t dispense methadone on-site.
Billing-heavy clinic (high denial rates, aging A/R)
Priority: Clean-claim automation, OTP bundle billing, denial management, RCM integration.
Best fit: AZZLY Rize (billing-first architecture), Behave Health (unified RCM), MASE + EliteMed billing (OTP-specialized RCM at 2.85%).
Compliance-heavy clinic (DEA scrutiny, high-audit state)
Priority: DEA Form 222 automation, controlled-substance inventory reconciliation, 42 CFR Part 2 segmentation, audit-ready exports, diversion accountability.
Best fit: MASE (strongest public OTP-specific compliance depth), Netsmart/Methasoft (legacy regulatory brand trust), Kipu (enterprise compliance monitoring).
AI/documentation-heavy clinic (staff burnout, note backlog)
Priority: Documentation time reduction, ambient scribing, clinician productivity.
Best fit: Alleva (TravisAI + Echo), Kipu (AI Scribe), Sunwave/Lightning Step (LIA).
Important: AI documentation does not replace dosing controls. If your highest-risk workflow is the morning dosing line, choose dosing depth first, AI second.
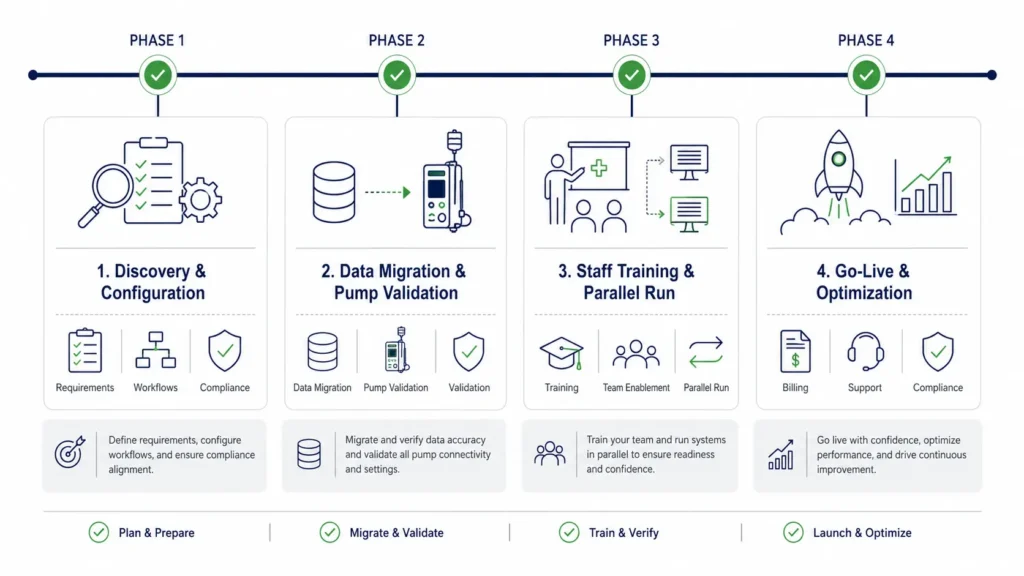
Implementation and migration: what to plan before switching OTP EMRs
Switching OTP EMRs is not just a software migration. It is a dosing-window, compliance, inventory, consent, billing, and patient-safety cutover. Plan accordingly.
Data migration checklist
Migrate these before go-live:
- Patient demographics (name, DOB, MRN, insurance, contact)
- Current dosing levels (active daily milligram amount for every active patient)
- Dosing history (30–90 days minimum of daily logs: dose, date, time, nurse, pump data)
- Phase/tier status (take-home eligibility, step level)
- Take-home records (bottle issuance logs, return verifications, callback results)
- Toxicology history (last 6 months of UDS results)
- Treatment plans (ASAM assessments, goals, timelines, signatures)
- 42 CFR Part 2 consents (consent forms, revocations, expiration dates, version history)
- DEA inventory logs (Form 222 records, bulk tank balance)
- Financial balances (open authorizations, unpaid patient balances, payer contracts)
Older closed charts can move to a read-only archive rather than cluttering the new system.
Dosing window: the critical path
Treat the dosing window as the highest-risk workflow during migration.
- Test pump integration before go-live: run 50 dummy pours using test patients.
- Verify hold logic: the system should fail to pour when an account is on hold.
- Reconcile the bulk tank at noon on Day 1: compare new EMR starting balance, physical tank count, and old system closing balance. Match to the decimal point.
- Keep the legacy system view-only for 48 hours after cutover.
- Require dual-nurse verification for the first dose poured on the new system.
- Prepare downtime dosing paper backup in case of system failure.
Standard implementation timeline
| Clinic type | Typical timeline |
|---|---|
| Small single-site OTP (MASE-specific) | 14–30 days |
| Standard OTP (general vendors) | 8–16 weeks |
| Multi-site network | 12–20+ weeks |
| Large enterprise (Netsmart-scale) | 6+ months |
Most delays occur during pump validation and 42 CFR Part 2 consent mapping. Budget time for both.
Planning a migration? Start with a demo that shows your exact workflows.
Pump validation · Data migration · Staff training · Onsite go-live support · Most OTPs live in 14–30 days
Questions to ask before choosing an OTP EMR
Bring these 12 questions to every vendor demo. The answers will tell you more than any feature list.
- Can you show a real dosing-window workflow from patient check-in to pump pour to chart entry — for 200 patients?
- Is MethaSpense/SciLog integration native, bidirectional, and real-time — or does it require manual entry at any point?
- How does your system manage guest dosing from another OTP?
- How are take-home bottles labeled, tracked, returned, and reconciled?
- Can the system automate random callbacks per our Diversion Control Plan?
- How does the system support DEA Form 222 ordering, receipts, and bulk-to-dose reconciliation?
- Does the platform support state PMP/PDMP/MAPS checks inside the patient chart — not a separate browser tab?
- How does the system enforce 42 CFR Part 2 consent, segmentation, and redisclosure rules?
- Can billing automatically roll seven daily doses into one weekly OTP bundle claim?
- What happens during system downtime at the dosing window?
- How long does implementation take for a clinic with our census and our pumps?
- What is the full three-year total cost of ownership — including implementation, migration, pump validation, training, EPCS, PDMP, clearinghouse, RCM, support, and exit fees?

Shortlist recommendation by clinic need
Use this table to narrow your vendor shortlist before booking demos.
| If your clinic needs… | Shortlist these vendors |
|---|---|
| OTP-specific dosing and pump sync | MASE, Netsmart/Methasoft, Kipu |
| EMR + billing + lower RCM fee | MASE + EliteMed, Behave Health, AZZLY Rize |
| Large enterprise deployment | Kipu, Netsmart/Methasoft, Behave Health |
| AI documentation | Alleva, Kipu, Sunwave/Lightning Step |
| Residential treatment | ZenCharts, Kipu, Alleva |
| Budget-friendly MAT workflows | ClinicTracker, MASE (Growth Bridge) |
| Unified CRM + EHR + RCM + ERP | Behave Health, Sunwave/Lightning Step |
| Staff burnout / charting speed | Alleva, Sunwave/Lightning Step, Kipu |
Final recommendation: the best OTP EMR for methadone clinics in 2026
There is no universal best OTP EMR. The right choice depends on your daily census, pump hardware, level-of-care mix, billing complexity, and tolerance for implementation downtime.
That said — for dedicated methadone clinics whose primary operations revolve around on-site liquid methadone dispensing, high-stakes compliance, and pump-connected workflows, MASE Behavioral Health EMR earns our top recommendation.
Here’s why:
Integrated dosing and hardware. MASE connects the clinical order to the physical pour through native real-time MethaSpense and SciLog pump synchronization — no third-party bolt-ons, no manual workarounds.
Compliance as a core feature. Digital DEA Form 222 tracking, 42 CFR Part 2 native privacy architecture, PMP/MAPS integration, automated callback policy, serialized bottle tracking, biometric verification, geofencing, and diversion risk scoring. The software supports controlled-substance compliance and reduces avoidable audit risk.
Specialized billing. OTP weekly bundle billing paired with EliteMed’s OTP-specialized RCM — reducing the administrative burden of daily claim reconciliation.
Growth Bridge. Eligible OTPs may qualify for Growth Bridge support that can reduce or cover the EMR subscription for an initial period — removing the software-license barrier that keeps smaller clinics on outdated systems.
Implementation built around dosing continuity. Pump validation, data migration, parallel run, and inventory integrity from day one — because a dosing window cannot stay closed.
When to evaluate other platforms
- Netsmart/Methasoft remains a powerhouse for massive networks where legacy OTP depth and enterprise-grade controls outweigh modern UX.
- Kipu Health is the strongest enterprise addiction-treatment option when residential + MAT + multi-site scalability matters more than pure OTP-native depth.
- Behave Health leads when unified CRM/EHR/RCM/ERP and end-to-end revenue operations matter more than OTP-specific dispensing workflows.
- AZZLY Rize fits outpatient MAT and broader addiction treatment programs where billing integration and customer support are top priorities.
- Alleva is the strongest AI documentation option when reducing note-writing burden is the primary pain point.
- ZenCharts fits residential programs that need ease of use and clinical satisfaction over deep OTP automation.
- ClinicTracker is the budget-sensitive value option with transparent per-user pricing for smaller SUD clinics.
- Sunwave/Lightning Step is worth evaluating when staff burnout, charting speed, and unified CRM/EMR/RCM operations are the primary selection criteria.
The honest answer: Book demos with your top 2–3 vendors. Bring your compliance officer. Test with your actual pumps. Request references from similar-volume OTPs. Compare three-year TCO, not sticker price. And choose the software that helps protect the workflows your DEA registration depends on — your dosing window, your compliance records, and your patients.
FAQ: OTP EMR software for methadone clinics
What is an OTP EMR, and how is it different from a behavioral health EMR?
An OTP EMR is specialized software for Opioid Treatment Programs that manages methadone dosing, take-home medication, compliance, billing, and clinical records. Unlike a general behavioral health EMR, it must support daily observed dosing, controlled-substance inventory, DEA workflows, pump integration, and 42 CFR Part 2 privacy — not just clinical notes and scheduling.
What is the best OTP EMR software for methadone clinics in 2026?
For dedicated methadone clinics, MASE Behavioral Health EMR is our top recommendation because it combines OTP-native dosing, pump sync, DEA Form 222 tracking, diversion monitoring, and optional EliteMed billing in one connected system. For broader MAT programs, Behave Health and AZZLY Rize offer strong all-in-one platforms. For enterprise networks, Kipu and Netsmart/Methasoft provide scale.
What features are most important in methadone clinic software?
Dosing-window workflows, MethaSpense/SciLog pump integration, take-home tracking with bottle serialization, guest dosing, DEA Form 222 support, PMP/PDMP checks, 42 CFR Part 2 consent controls, OTP weekly bundle billing, diversion controls with callbacks, and audit-ready reporting.
How much does OTP EMR software cost in 2026?
Pricing is mostly custom/quote-based. Vendors charge per user, per provider, per active patient, percentage of collections, or enterprise license. MASE offers Growth Bridge for eligible OTPs plus 2.85% of collections. ClinicTracker signals ~$70/user/month. Others require demos for pricing. Always compare total cost of ownership including implementation, migration, pump validation, training, and RCM fees.
Which OTP EMR supports MethaSpense and SciLog pump integration?
MASE offers native real-time bidirectional pump sync. Netsmart/Methasoft has legacy pump support. Kipu references pump connector-style integrations for SciLog/IVEK in some materials. In the public materials we analyzed for other platforms (AZZLY Rize, Behave Health, ClinicTracker, Alleva, ZenCharts), we did not find clear documentation of MethaSpense or SciLog integration — verify during demo.
What is 42 CFR Part 2, and why does it matter for OTP EMR software?
42 CFR Part 2 protects substance use disorder treatment records with privacy rules stricter than HIPAA. OTP EMR software should enforce consent management, record segmentation, redisclosure controls, and audit trails as a platform foundation — not a generic settings checkbox. See the current eCFR Part 2 text.
How does OTP EMR software support DEA Form 222 and inventory reconciliation?
Stronger OTP EMRs connect DEA Form 222 workflows to bulk inventory, pump dispensing, take-home bottles, and controlled-substance reports. The system should track Schedule II ordering, receiving, reconciliation, and generate a bulk-to-dose audit package. The DEA also offers CSOS electronic ordering as an alternative to paper Form 222.
Does OTP software integrate with PMP, PDMP, or MAPS systems?
Most OTP and MAT platforms support some PMP/PDMP workflow, but buyers should verify state-specific coverage, consent requirements under 42 CFR Part 2, in-chart lookup, reporting workflows, and whether access is native, API-based, or a paid add-on.
How long does OTP EMR implementation take?
MASE standard configurations: 14–30 days. General OTP vendors: 8–16 weeks. Multi-site networks: 12–20+ weeks. Large enterprises (Netsmart-scale): 6+ months. Most delays occur during pump validation and 42 CFR Part 2 consent mapping.
What should methadone clinics verify before booking an OTP EMR demo?
Bring your pump hardware model numbers, daily census, take-home eligibility volume, state PMP/PDMP requirements, current billing denial rate, and your compliance officer. Test dosing-window speed, pump integration, take-home bottle tracking, callback automation, DEA Form 222 workflows, and billing bundle logic with your actual data — not a generic demo.
Is OTP EMR software the same as methadone dispensing software?
Not exactly. Methadone dispensing software typically focuses on the pump-to-dose workflow and liquid inventory. A full OTP EMR adds clinical documentation, treatment planning, compliance management, billing/RCM, take-home tracking, callbacks, DEA Form 222 workflows, 42 CFR Part 2 consent controls, and reporting — covering the entire clinic operation, not just the dispensing window.
What is the best addiction treatment EMR for OTP clinics?
For clinics where on-site methadone dispensing is the core workflow, a purpose-built OTP EMR like MASE is a stronger fit than a broader addiction treatment EMR. For OTP clinics that also run residential, PHP/IOP, or outpatient SUD programs, Kipu, Behave Health, or AZZLY Rize may provide the multi-level-of-care coverage needed — but buyers should verify OTP-specific dosing and pump capabilities during demos.
Can an OTP EMR help reduce billing denials?
Yes — when the EMR ties clinical documentation directly to billing rules, validates payer requirements, automates OTP weekly bundle logic (H0020, G2067, G2078), tracks authorizations, and flags missing documentation before claims are submitted. Most clinics that switch from manual or generic billing to OTP-specialized billing recover 15–30% in previously denied or underbilled revenue within the first 90 days.
Related resources
- MASE OTP/Methadone EMR — Full Product Page
- OTP Billing Services by EliteMed Financials
- OTP Clinic Software — Complete Solution
- AZZLY Rize Alternative for Methadone Clinics
- Contact EliteMed Financials
Reviewed by: EliteMed Financials Revenue Cycle Team
Clinical / compliance review: Reviewed with input from OTP billing, behavioral health compliance, and methadone clinic operations specialists.
Why trust this guide: EliteMed Financials works with behavioral health and OTP billing workflows and partners with MASE Behavioral Health EMR. This guide clearly discloses that partnership and uses publicly available vendor information where competitor capabilities are discussed. If you can improve this guide, we welcome your feedback via our contact page.
Last updated: May 2026 · Next scheduled review: November 2026
Sources cited: SAMHSA 42 CFR Part 8 Final Rule (89 FR 7528); 42 CFR Part 2 (eCFR); CMS OTP Billing; DEA Form 222; DEA CSOS; IVEK Corporation (MethaSpense); Capterra, G2, GetApp, and Software Advice reviews; vendor product pages and documentation.
EliteMed Financials LLC is the billing partner for MASE Behavioral Health EMR. This article compares OTP EMR platforms based on publicly available product documentation, review platforms, and our workflow analysis as of May 2026. “Not documented” indicates the capability is not described in publicly accessible vendor materials at the time of publication and does not necessarily mean the capability is absent. We have no undisclosed financial relationships with any vendor named in this comparison other than our partnership with MASE. Always verify vendor capabilities, pricing, and regulatory compliance directly before any purchase decision. This article does not constitute clinical, legal, billing, or compliance advice.

