The Complete Guide to NEMT Billing: Process, Codes, Compliance & Revenue Optimization (2026)
Table of Contents
What Is NEMT Billing?
NEMT billing is the process of submitting claims and collecting payment for non-emergency medical transportation services. Unlike standard medical billing, NEMT billing requires navigating multiple payer systems—Medicaid, Medicare Advantage, private insurance, and transportation brokers—each with distinct requirements for eligibility verification, trip documentation, coding, and claims submission.
The stakes are significant. The NEMT market reached $10.8 billion in 2024 and is projected to grow to $19.9 billion by 2034, driven by aging populations and increasing recognition that transportation barriers prevent patients from accessing healthcare. An estimated 4-5% of Medicaid beneficiaries rely on NEMT services annually, translating to over $1.5 billion in annual Medicaid NEMT spending across states.
For NEMT providers, mastering the billing process directly determines business viability. The difference between a 95% clean claim rate and an 80% clean claim rate represents tens of thousands of dollars in annual revenue—money that either flows into your business or disappears into denied claims, rework costs, and missed timely filing deadlines.
Why NEMT Billing Differs from Standard Medical Billing
Standard medical billing follows relatively predictable patterns—verify insurance, submit claims, receive payment. NEMT billing introduces complications that trip up even experienced billers:
Multiple payer relationships require different workflows. Medicaid programs operate through state agencies or contracted brokers like ModivCare, MTM (Medical Transportation Management), Access2Care, and Veyo. Each broker maintains separate portals, credentialing requirements, and payment timelines. Medicare Advantage plans vary coverage by insurer and geography. Private insurance coverage is rare and inconsistent.
Trip-based documentation creates unique audit exposure. Every billable trip requires timestamps, signatures, GPS-verified mileage, and proof connecting the transport to a covered medical appointment. Missing a single element on a single trip log can trigger denial—or worse, flag patterns that invite broader audit scrutiny.
Geographic fragmentation means no universal rules. A provider operating across state lines faces different Medicaid fee schedules, documentation requirements, timely filing limits, and broker relationships in each state. What works in New York fails in Texas.
The Cost of Getting NEMT Billing Wrong
Industry benchmarks reveal the gap between optimized and struggling operations:
| Metric | Top Performers | Industry Average | Struggling Ops |
| Clean Claim Rate | 95%+ | 85-90% | Below 80% |
| Denial Rate | Under 5% | 10-15% | 20%+ |
| Days in A/R | Under 30 | 45-60 | 90+ |
| Collection Rate | 95%+ | 85-90% | Below 80% |
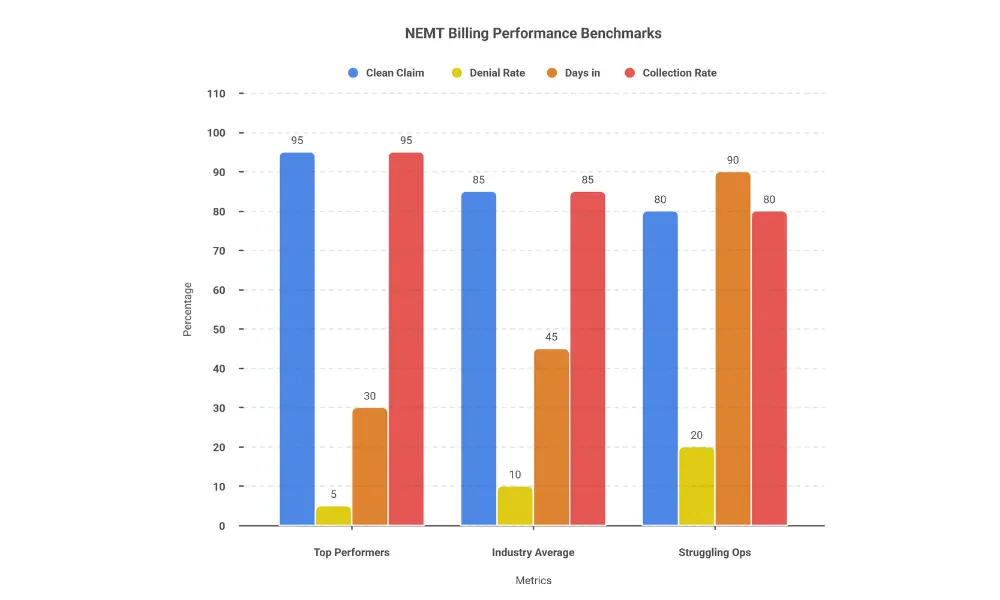
A provider with $1 million in annual billings and a 15% denial rate loses $150,000 before accounting for the staff time spent on rework and appeals. Reduce that denial rate to 5%, and you recover $100,000 annually—often the single highest-ROI improvement available to NEMT businesses.
This guide covers every aspect of NEMT billing—from the step-by-step process to payer-specific requirements to compliance frameworks—giving you the knowledge to achieve top-performer benchmarks. Whether you manage billing in-house or evaluate professional NEMT billing services, understanding these fundamentals is essential.
The NEMT Billing Process: 7 Steps to Clean Claims
Successful NEMT billing follows a systematic process from eligibility verification through payment posting. Each step builds on the previous one—shortcuts or gaps at any stage create problems that compound downstream, resulting in denials, delayed payments, and compliance exposure.
Here’s the complete NEMT billing process broken down into seven actionable steps.
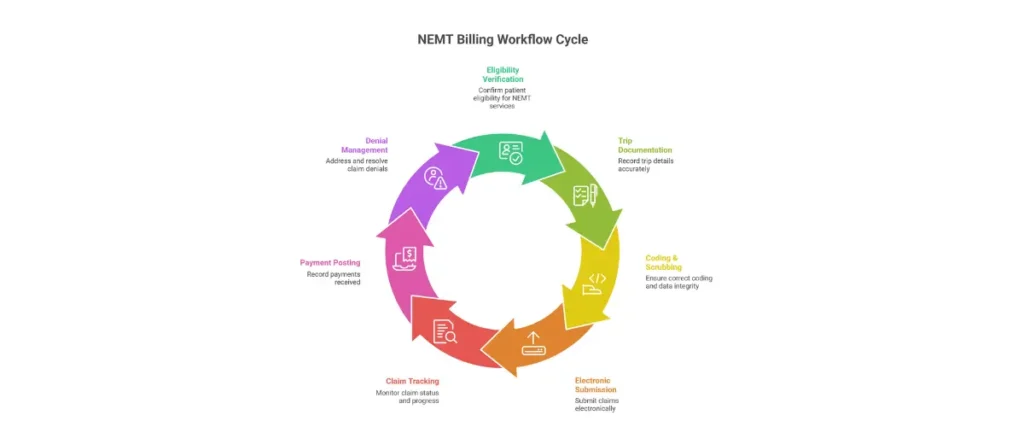
Step 1: Eligibility Verification
Eligibility verification confirms the patient has active coverage for NEMT services before you dispatch a vehicle. This single step prevents more denials than any other intervention.
Best practice: Verify eligibility 24-48 hours before scheduled trips using electronic EDI 270/271 transactions. Real-time eligibility checks through your billing software or clearinghouse confirm:
- Active Medicaid/Medicare/insurance enrollment
- NEMT benefit inclusion in the patient’s plan
- Any prior authorization requirements
- Applicable copays or cost-sharing
Why this matters: Medicaid eligibility can change monthly based on income verification, premium payments, or administrative processing. A patient eligible last week may not be eligible today. Billing for ineligible patients results in automatic denial with zero appeal success—you’ve provided free transportation.
For broker-assigned trips, the broker typically handles initial eligibility. However, smart providers verify independently before high-value trips (wheelchair, stretcher) where denial costs exceed verification effort.
Step 2: Trip Documentation
Complete trip documentation provides the evidentiary foundation for every claim. Think of documentation as your audit defense—if it isn’t documented, it didn’t happen, and you can’t bill for it.
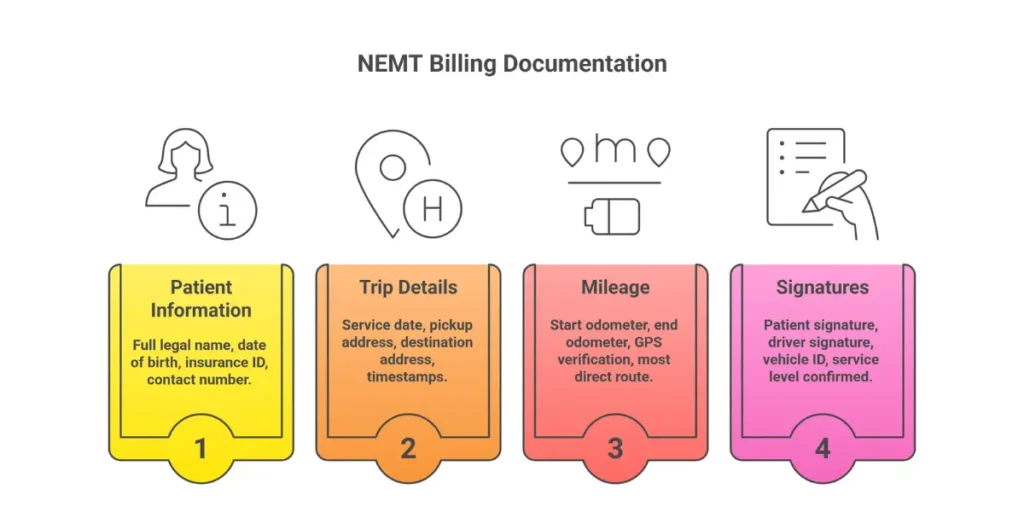
Required documentation elements:
Patient Information:
- Full legal name matching insurance records
- Date of birth
- Medicaid/Medicare/Insurance ID number
Trip Details:
- Service date
- Pickup address (complete with unit/suite numbers)
- Destination address
- Appointment time and purpose
- Facility or provider name
Service Verification:
- Driver name and credentials
- Vehicle identification
- Service level provided (ambulatory, wheelchair, stretcher)
Mileage Documentation:
- Starting odometer reading
- Ending odometer reading
- GPS-verified route
- Total loaded miles (patient in vehicle)
Attestation:
- Patient or representative signature confirming service receipt
- Driver signature attesting to service delivery
- Timestamps for pickup and drop-off
Digital documentation systems using tablets or mobile apps capture this information in real-time with GPS integration, eliminating the manual errors and missing fields that plague paper-based systems. Electronic proof of delivery (ePOD) creates tamper-evident records that withstand audit scrutiny.
Step 3: Coding and Claim Scrubbing
Accurate coding translates your service into the standardized language payers require for processing. NEMT billing uses HCPCS Level II codes combined with origin/destination modifiers and supporting ICD-10 diagnosis codes.
Common NEMT HCPCS codes:
| Code | Description | Billing Unit |
| A0080 | Wheelchair transport | Per mile |
| A0090 | Ambulette/taxi | Per trip |
| A0130 | Wheelchair van | Per mile |
| T2001 | Non-emergency transport | Per trip |
| T2002 | Wheelchair van with driver | Per trip |
| T2003 | Wheelchair van mileage | Per mile |
Modifier codes indicate origin and destination:
- R = Residence
- H = Hospital
- P = Physician office
- N = Skilled nursing facility
Example: A trip from home to doctor’s office uses modifier RP (Residence to Physician).
Claim scrubbing validates claims before submission, checking for:
- Correct HCPCS code for service level
- Matching modifiers on base and mileage codes
- Valid ICD-10 diagnosis supporting medical necessity
- Complete required fields
- Duplicate claim detection
AI-powered claim scrubbing catches errors that rule-based systems miss, pushing clean claim rates above 95%. Manual review cannot match the consistency and speed of automated scrubbing at scale.
Step 4: Electronic Claim Submission
Claims submission transmits your validated claims to payers using EDI 837P (Professional) format—the healthcare industry standard for electronic claims.
Submission pathways vary by payer:
- State Medicaid: Direct portal submission or through approved clearinghouse
- Brokers (ModivCare, MTM): Broker-specific portals or API integration
- Medicare Advantage: Through the plan’s designated clearinghouse
- Private insurance: CMS-1500 form or EDI through clearinghouse
Timing matters. Submit claims within 24-48 hours of service completion to maximize cash flow and ensure compliance with timely filing limits. Batch processing daily keeps claims current; weekly submission creates unnecessary A/R aging.
Timely filing limits vary by payer:
- Medicaid: 90-365 days (state-dependent)
- Medicare Advantage: 90-365 days (plan-dependent)
- Brokers: 30-90 days (contract-dependent)
Missing timely filing deadlines results in permanent, non-appealable denial. There are no exceptions for “we forgot” or “our biller quit.”
Step 5: Claim Tracking and Adjudication
After submission, claims enter the payer’s adjudication process. Proactive tracking identifies problems early while correction remains possible.
Monitor claim status using:
- EDI 277 claim status responses
- EDI 999 acknowledgment reports confirming receipt
- Payer portal dashboards
- Clearinghouse tracking tools
Follow-up cadence: Check claim status at 14-day intervals for claims not yet adjudicated. Payers have processing backlogs; proactive follow-up keeps your claims from getting lost.
Common adjudication outcomes:
- Paid: Claim accepted, payment issued
- Denied: Claim rejected (requires appeal or correction)
- Pended: Additional information requested
- Partial payment: Claim paid at reduced amount (requires review)
Track adjudication patterns to identify systematic issues. If 30% of claims from a specific payer pend for the same reason, you have a documentation or coding problem to address at the source.
Step 6: Payment Posting and Reconciliation
Payment posting records received payments against submitted claims, identifying discrepancies requiring follow-up.
ERA 835 (Electronic Remittance Advice) provides detailed payment information:
- Paid amount per claim
- Adjustment reason codes explaining any variance
- Patient responsibility amounts
- Denial codes for rejected line items
Best practice: Post payments daily as ERAs arrive. Automated ERA posting through integrated billing software eliminates manual data entry errors and accelerates reconciliation.
Reconciliation checks:
- Payment matches expected reimbursement rate
- All submitted claims have corresponding payment or denial
- Adjustment codes are reviewed and addressed
- Underpayments flagged for follow-up
Payment variances require investigation. A claim paid at 80% of expected rate may indicate coding issues, contract misunderstanding, or payer error requiring correction.
Step 7: Denial Management and Appeals
Denials are inevitable—even optimized operations experience 3-5% denial rates. The difference between good and great revenue performance lies in systematic denial management.
Common denial codes:
- CO-16: Claim lacks prior authorization
- CO-29: Timely filing limit exceeded
- CO-15: Authorization missing/invalid
- CO-18: Duplicate claim
- CO-197: Missing/incomplete documentation
Denial management workflow:
- Categorize denials by reason code to identify patterns
- Prioritize high-dollar and easily correctable denials
- Gather supporting documentation for appeals
- Submit appeals within payer-specific deadlines (typically 60-90 days)
- Track appeal outcomes to measure success rates
- Analyze root causes to prevent future denials
Critical insight: Industry data shows 65% of denied claims are never appealed—representing massive recoverable revenue left on the table. Even with 50% appeal success rates, systematic denial management recovers significant revenue that passive operations forfeit.
A/R aging reports should trigger escalation:
- 30 days: Standard follow-up
- 60 days: Supervisor review
- 90 days: Executive escalation
Claims approaching timely filing limits require immediate action regardless of other priorities.
NEMT Billing Requirements by Payer Type
Different payers operate under different rules, and mastering these variations determines whether claims get paid or denied. Medicaid, Medicare Advantage, private insurance, and transportation brokers each maintain unique billing codes, documentation requirements, prior authorization rules, and reimbursement timelines that providers must navigate successfully.
Understanding payer-specific requirements isn’t optional—it’s the foundation of sustainable NEMT revenue.
How to Bill Medicaid for NEMT
Medicaid represents 60-70% of NEMT billing volume for most providers, making mastery of state-specific requirements essential for business survival. Under federal regulation 42 CFR § 431.53—officially titled ‘Assurance of Transportation’ and published in the Electronic Code of Federal Regulations—all state Medicaid programs must provide transportation to covered medical services.
However, Medicaid NEMT billing varies dramatically by state—from program structure to reimbursement rates to documentation requirements.
Understanding Your State’s NEMT Program Structure
States organize Medicaid NEMT through three primary models:
Broker-based models dominate the landscape. Most states contract with transportation brokers—ModivCare, MTM (Medical Transportation Management), Access2Care, Veyo, or Verida—to manage NEMT benefits. You bill the broker rather than the state Medicaid agency directly. The broker verifies eligibility, assigns trips, sets provider rates, and processes payments. States using statewide broker models include Connecticut, New Jersey, and New York, while Arizona, Kansas, and Texas use regional broker arrangements.
Fee-for-service (FFS) states allow direct billing to the state Medicaid agency. This model provides potentially higher reimbursement but requires managing state-specific billing portals, claim formats, and documentation standards. Alabama, Alaska, and Maryland operate primarily FFS programs.
Managed Care Organization (MCO) integration embeds NEMT within broader Medicaid managed care contracts. Each MCO may maintain different billing procedures, rates, and authorization requirements—even within the same state. Providers must credential separately with each MCO serving their region.
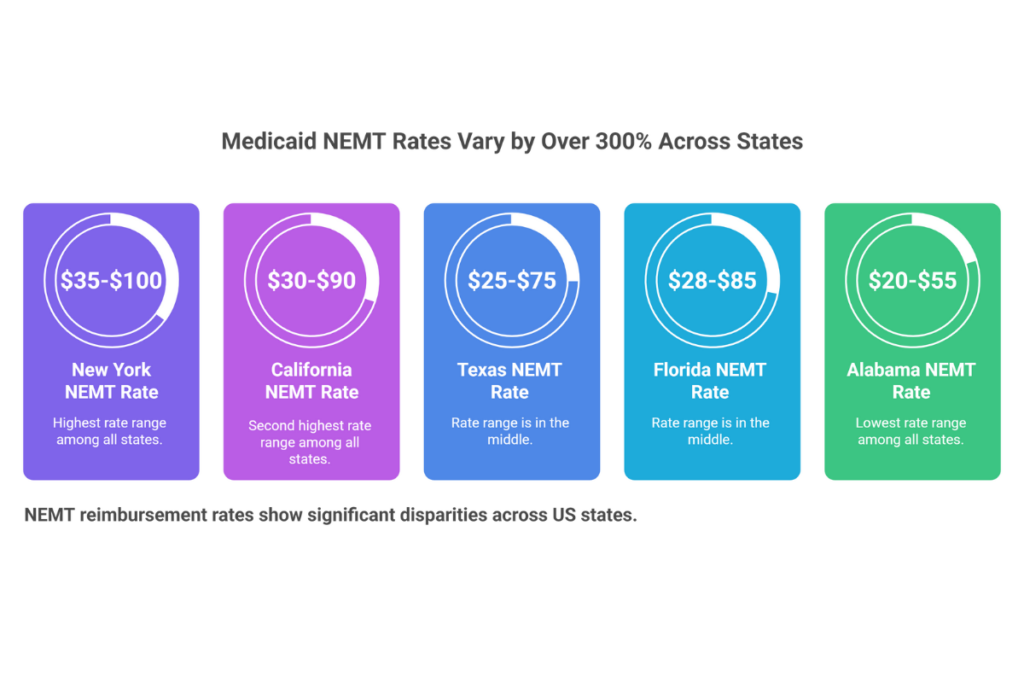
State-by-State Medicaid NEMT Rates
Medicaid reimbursement rates vary by over 300% between the highest and lowest-paying states for identical services. This geographic disparity fundamentally shapes business viability before you complete a single trip.
These state rate variations directly impact your billing strategy and revenue potential. For a complete understanding of how to optimize your NEMT billing process across different states and payers, see our comprehensive NEMT Billing Guide state by state which covers the complete 7-step billing workflow.
| State | Ambulatory (per trip) | Wheelchair (per trip) | Mileage Rate |
| New York | $35-$50 | $60-$100 | $2.50-$4.00/mi |
| California | $30-$45 | $50-$90 | $2.00-$3.50/mi |
| Texas | $25-$40 | $45-$75 | $2.00-$3.00/mi |
| Florida | $28-$42 | $50-$85 | $2.25-$3.25/mi |
| Pennsylvania | $30-$45 | $55-$90 | $2.50-$4.00/mi |
| Illinois | $28-$40 | $50-$80 | $2.00-$3.00/mi |
| Ohio | $25-$38 | $45-$75 | $2.00-$2.75/mi |
| Georgia | $22-$35 | $40-$70 | $1.75-$2.50/mi |
| Tennessee | $20-$32 | $35-$60 | $1.50-$2.25/mi |
| Alabama | $20-$30 | $35-$55 | $1.50-$2.00/mi |
Rates vary by broker contract, MCO agreement, and service region within each state. Verify current rates with your state Medicaid agency or broker.
Medicaid Provider Enrollment Process
Before billing Medicaid, complete provider enrollment through your state’s process:
- Apply through your state Medicaid provider enrollment portal with required documentation (business license, insurance certificates, vehicle inspections, driver credentials)
- Complete broker credentialing if your state uses ModivCare, MTM, Access2Care, or other brokers—each broker maintains separate credentialing requirements
- Obtain your Medicaid provider number enabling electronic claim submission
- Set up EDI 837P connectivity through your state portal or approved clearinghouse
Provider enrollment typically requires 60-90 days from application to approval. Plan accordingly before expecting Medicaid revenue—this timeline creates cash flow challenges for startups without adequate working capital.
Medicaid Documentation Requirements
State Medicaid programs specify documentation requirements for NEMT claims:
Physician Certification Statement (PCS) requirements vary by state and service level. Many states require PCS forms for wheelchair and stretcher transport, documenting medical necessity through physician attestation. PCS forms must include diagnosis, mobility limitation description, and certification that the patient cannot safely use other transportation.
Trip logs with GPS verification provide proof of service that withstands audit scrutiny. Required elements include timestamps, addresses, mileage, patient signatures, and driver identification.
Medical necessity documentation connects each trip to Medicaid-covered healthcare services—routine appointments, dialysis, therapy, mental health treatment, and other covered benefits.
Will Medicare Pay for NEMT?
According to the Medicare Coverage Database maintained by CMS, traditional Medicare (Parts A and B) does not cover routine non-emergency medical transportation—only emergency ambulance services when medically necessary. This official guidance is documented in the Medicare Benefit Policy Manual, Chapter 10.
Medicare ambulance coverage requires that transport by any other means would endanger the patient’s health and that the destination is the nearest appropriate facility. For routine doctor visits, dialysis appointments, therapy sessions, or other non-emergency care, Original Medicare provides no transportation benefit.
Medicare Advantage NEMT Benefits
Medicare Advantage (Part C) plans frequently include NEMT as a supplemental benefit, making this payer segment increasingly important for providers seeking revenue diversification beyond Medicaid.
Coverage varies significantly by plan and insurer:
| Insurer | Typical NEMT Benefit | Copay Range | Trip Limits |
| UnitedHealthcare | Included in most MA plans | $0-$15 | 24-48 trips/year |
| Humana | Many plans include | $0-$20 | 12-36 trips/year |
| Aetna | Select plans | $5-$20 | 20-40 trips/year |
| Cigna | Limited plans | $10-$20 | 12-24 trips/year |
| Kaiser Permanente | Regional variation | $0-$15 | Varies by region |
Benefits vary by specific plan, county, and year. Verify coverage before providing service.
How to Bill Medicare Advantage for NEMT
- Verify the specific plan includes NEMT benefits through eligibility inquiry or member services contact
- Confirm your company is in the plan’s provider network—out-of-network claims may be denied or reduced
- Obtain prior authorization if required by the specific MA plan
- Submit claims using EDI 837P through the plan’s designated clearinghouse or portal
- Track payment within the plan’s timeline (typically 14-30 days, faster than Medicaid)
Dual-Eligible Beneficiary Billing
Patients enrolled in both Medicare and Medicaid (dual-eligibles) receive NEMT coverage through Medicaid as the primary payer. Medicare does not cover routine NEMT even for dual-eligible beneficiaries—Medicaid’s transportation assurance requirement under 42 CFR § 431.53 provides the coverage. Bill Medicaid using standard Medicaid procedures; do not submit NEMT claims to Medicare for dual-eligible patients unless emergency ambulance services are provided.
Is NEMT Covered by Private Insurance?
Private insurance NEMT coverage varies dramatically by plan and is not federally mandated. Unlike Medicaid’s guaranteed transportation benefit, commercial health plans treat NEMT as an optional supplemental benefit that most plans exclude.
Which Private Insurance Plans Cover NEMT?
Coverage is most common in:
- Employer-sponsored plans with chronic disease management programs covering dialysis, chemotherapy, and rehabilitation transport
- Plans in states requiring NEMT coverage (limited mandates exist in California and New York)
- High-premium comprehensive health plans marketed to elderly or disabled populations
- Workers’ compensation insurance covering transportation to treatment for work-related injuries
Private Insurance Billing Process
Step 1: Verify coverage by contacting the insurer’s provider services line with patient policy details, specific HCPCS codes you plan to bill, and questions about prior authorization requirements.
Step 2: Obtain prior authorization before providing services. Most private insurers require pre-approval including physician’s order for medical transportation, detailed medical necessity documentation, and treatment plan demonstrating ongoing appointment needs.
Step 3: Submit claims with complete documentation using CMS-1500 or UB-04 forms as preferred by the insurer, including authorization numbers and supporting medical records.
Step 4: Follow up aggressively on private insurance claims—payment timelines of 30-90 days and higher denial rates require persistent attention.
Private Pay Rates
When insurance doesn’t cover NEMT, patients may pay directly at market rates:
- Ambulatory: $30-$75 base plus $2-$5 per mile
- Wheelchair: $50-$150 base plus $3-$6 per mile
- Stretcher: $200-$400 base plus $5-$10 per mile
Private pay offers faster payment (same-day to 7 days), eliminates payer complexity, and commands premium rates—making it a valuable revenue diversification strategy for profitable NEMT operations.
NEMT Broker Billing
Transportation brokers serve as intermediaries between state Medicaid agencies and NEMT providers, managing trip assignment, rate setting, and payment processing for the majority of Medicaid NEMT volume nationwide.
Major NEMT Brokers
| Broker | States Served | Provider Portal | Payment Timeline |
| ModivCare | 31+ states | modivcare.com | Net 15-30 days |
| MTM | 28+ states | mtm-inc.net | Net 15-30 days |
| Access2Care | 20+ states | access2care.net | Net 15-30 days |
| Veyo | AZ, CA, CO, ID, NV, VA | veyo.com | Net 15-30 days |
| Verida | Regional markets | verida.com | Net 15-30 days |
How Broker Billing Works
Brokers don’t pay you directly—they manage Medicaid NEMT benefits on behalf of state agencies. The workflow operates as follows:
- Credentialing: Complete broker enrollment with required documentation, insurance verification, and vehicle inspections
- Trip assignment: Brokers assign trips through provider portals or APIs based on availability, location, and performance metrics
- Service delivery: Complete assigned trips with required documentation
- Claim submission: Submit completed trip data through broker portals or integrated software
- Payment processing: Brokers process claims and issue payment within their payment cycle (typically Net 15-30 days—faster than direct Medicaid billing)
Maximizing Broker Relationships
Broker systems track provider scorecards measuring on-time performance, complaint rates, turn-back rates (declined trip assignments), and documentation compliance. High-performing providers receive:
- Priority trip assignments
- Access to premium service categories
- Potential rate negotiations
- Fewer audits and compliance reviews
Maintaining 95%+ on-time performance and under 2% complaint rates positions your company as a preferred provider—the key to sustainable broker-based revenue.
Professional NEMT billing services help providers navigate multi-broker credentialing, optimize claim submission across different portals, and maximize reimbursement from each payer relationship.
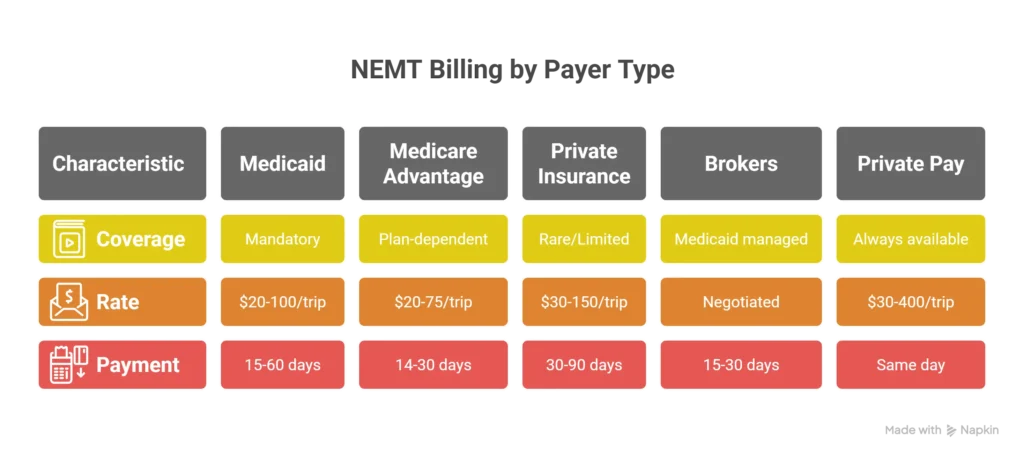
Payer Type Comparison Summary:
| Payer | Coverage | Typical Rate | Payment Time | Complexity |
| Medicaid | Mandatory (42 CFR § 431.53) | $20-$100/trip | 15-60 days | High |
| Medicare Traditional | Emergency only | N/A for NEMT | N/A | N/A |
| Medicare Advantage | Plan-dependent | $20-$75/trip | 14-30 days | Medium |
| Private Insurance | Rare/limited | $30-$150/trip | 30-90 days | High |
| Brokers | Medicaid managed | Negotiated | 15-30 days | Medium |
| Private Pay | Always available | $30-$400/trip | Same day-7 days | Low |
NEMT Billing Codes: Complete Reference Guide
Accurate coding determines whether claims get paid or denied. Using the wrong HCPCS code for the service level provided, mismatching modifiers, or failing to link appropriate diagnosis codes triggers automatic rejections that waste time and jeopardize timely filing compliance.
This reference guide covers every code you need for NEMT billing success.
HCPCS Codes for NEMT Services
The Healthcare Common Procedure Coding System (HCPCS) Level II—the official code set maintained by CMS for reporting medical procedures and services—provides standardized codes for NEMT services. The complete code set, including annual updates to transportation codes, is available through the CMS HCPCS resource center.
Primary NEMT Transportation Codes
| HCPCS Code | Description | Service Type | Billing Unit | Rate Range |
| A0080 | Wheelchair transport | Wheelchair | Per mile | $2-$5/mi |
| A0090 | Taxi/ambulette transport | Ambulette | Per trip | $20-$50 |
| A0100 | Taxi transport | Ambulatory | Per trip | $15-$40 |
| A0120 | Minivan transport | Ambulatory | Per mile | $2-$4/mi |
| A0130 | Wheelchair van transport | Wheelchair | Per mile | $3-$6/mi |
| A0140 | Ambulatory van (walkers) | Ambulatory | Per mile | $2-$5/mi |
| A0160 | Stretcher/litter transport | Stretcher | Per trip | $50-$150 |
| A0170 | Wheelchair/stretcher combo | Mixed | Per trip | $75-$200 |
| A0172 | Dialysis taxi transport | Dialysis | Per trip | $25-$60 |
| A0180 | Non-emergency wheelchair | Wheelchair | Per mile | $3-$7/mi |
T-Codes for NEMT Services
| HCPCS Code | Description | Service Type | Billing Unit | Rate Range |
| T2001 | Commercial NEMT transport | Ambulatory/WC | Per trip | $20-$45 |
| T2002 | Wheelchair van with driver | Wheelchair | Per trip | $40-$100 |
| T2003 | Wheelchair van mileage | Wheelchair | Per mile | $3-$6/mi |
| T2004 | Minivan mileage | Ambulatory | Per mile | $2-$5/mi |
| T2005 | Stretcher van with driver | Stretcher | Per trip | $100-$300 |
| T2007 | NEMT waiting time | Add-on | 30-min units | State-based |
Mileage Add-On Codes
| HCPCS Code | Description | Use Case | Rate Range |
| S0209 | Wheelchair mileage | Short-haul WC transport | $2-$5/mi |
| S0215 | Ground mileage | All ground transport | $2-$10/mi |
| A0425 | Ground mileage | Ambulance/NEMT mileage | State-based |
Critical Rule: Mileage codes (A0425, T2003, S0209, S0215) must carry the same modifiers as the base transport code. Modifier mismatch between base and mileage codes triggers automatic denial.
Modifier Codes for NEMT Billing
Modifiers indicate trip origin and destination, providing payers with context essential for proper adjudication. NEMT claims require two-position modifier combinations—origin first, destination second.
Origin/Destination Modifiers
| Modifier | Location Type | Common Use |
| D | Diagnostic facility | Lab, imaging center |
| E | Residential/custodial facility | Assisted living, group home |
| G | Hospital-based dialysis | Dialysis center in hospital |
| H | Hospital | Inpatient/outpatient hospital |
| I | Independent pickup | Site of illness or injury |
| J | Freestanding dialysis | Independent dialysis center |
| N | Skilled nursing facility | SNF, nursing home |
| P | Physician office | Doctor’s office, clinic |
| R | Residence | Patient’s home |
| S | Scene of accident | Accident/emergency scene |
| X | Destination unknown | Intermediate transport |
Example Modifier Usage:
- RH = Residence to Hospital
- HR = Hospital to Residence
- RJ = Residence to Freestanding Dialysis
- NP = Nursing Facility to Physician Office
ICD-10 Diagnosis Codes for Medical Necessity
Linking appropriate ICD-10 diagnosis codes to NEMT claims establishes medical necessity—the clinical justification for why the patient requires specialized transportation rather than standard transit options.
| ICD-10 Code | Description | Transport Justification |
| Z51.11 | Chemotherapy encounter | Wheelchair/stretcher required |
| Z51.81 | Renal dialysis encounter | Dialysis transport codes |
| Z99.89 | Ventilator dependence | Non-ambulatory transport |
| E11.9 | Type 2 diabetes | Fatigue, mobility limitations |
| I50.9 | Heart failure | Limited physical capacity |
| R53.83 | Chronic fatigue | Ambulatory restrictions |
| M79.1 | Myalgia | Pain-related mobility limits |
Required Documentation for NEMT Billing
Complete documentation protects against audits and prevents denials. Every billable trip requires specific data elements captured at the time of service—not reconstructed hours later from memory.
The “Big 5” Audit-Critical Fields
Every NEMT claim must include these five elements that auditors verify first:
- Patient full legal name matching insurance records exactly
- Medicaid/Insurance ID number verified as active on service date
- Complete pickup and drop-off addresses including suite/unit numbers
- Sequential timestamp documentation (dispatch, arrival, departure, destination)
- Dual signatures (driver attestation + patient/representative acknowledgment)
Complete Documentation Checklist
Patient Information: ☐ Full legal name ☐ Date of birth ☐ Medicaid/Medicare/Insurance ID ☐ Contact phone number
Trip Details: ☐ Service date ☐ Dispatch time ☐ Arrival at pickup time ☐ Loaded departure time ☐ Arrival at destination time ☐ Complete pickup address ☐ Complete destination address
Mileage Documentation: ☐ Starting odometer reading ☐ Ending odometer reading ☐ Total loaded miles ☐ GPS route verification ☐ Most direct route confirmation
Medical Information: ☐ Facility/provider name ☐ Appointment purpose ☐ Level of service justification ☐ Linked ICD-10 diagnosis code
Attestation: ☐ Driver signature with credentials ☐ Patient/representative signature ☐ Vehicle identification ☐ Service level confirmation
Physician Certification Statement (PCS) Requirements
A Physician Certification Statement documents medical necessity through physician attestation and is required in most states for wheelchair and stretcher transport.
When PCS Is Required
- Wheelchair transport in most state Medicaid programs
- Stretcher/gurney transport in all state programs
- Recurring transport for ongoing treatment (dialysis, chemotherapy)
- Out-of-area transport exceeding standard mileage thresholds
PCS Required Elements
A valid PCS must include:
- Patient name and date of birth
- Diagnosis requiring specialized transport
- Mobility limitation description
- Certification that patient cannot safely use other transportation
- Physician signature with credentials and NPI
- Validity period (typically 30-180 days depending on state)
State-specific PCS validity periods:
- California: 60 days standard, 180 days for chronic conditions
- New York: 90 days for wheelchair, 60 days for stretcher
- Texas: 60 days standard
- Florida: 90 days for recurring dialysis transport
Electronic vs Paper Documentation
Digital trip capture eliminates the documentation errors that cause 15-20% of NEMT denials. Modern NEMT billing software with driver mobile apps provides advantages paper systems cannot match.
Digital Documentation Benefits
GPS-verified mileage provides indisputable proof of distance traveled via the most direct route, eliminating mileage disputes and audit flags for “perfect mileage patterns” that suggest fabrication.
Electronic signatures captured on tablets meet HIPAA security requirements, create tamper-evident records, and eliminate missing signature denials.
Sequential timestamps recorded automatically prevent post-dated trip logs and ensure audit trail integrity.
EVV (Electronic Visit Verification) compliance, increasingly required by state Medicaid programs, integrates with digital trip capture systems.
Documentation Retention Requirements
NEMT billing records must be retained for 7-10 years depending on state requirements and payer contracts. Digital storage with proper backup systems ensures compliance while enabling rapid retrieval during audits.
Investing in professional NEMT website development with integrated dispatch and documentation systems pays for itself through reduced denials and eliminated compliance risk.
Common Coding Errors to Avoid:
| Error Type | Problem | Consequence |
| Wrong base code | Ambulatory code for wheelchair patient | Automatic denial |
| Mileage without base | Billing mileage alone | Incomplete claim rejection |
| Modifier mismatch | Different modifiers on base vs mileage | Denial + audit flag |
| Missing ICD-10 | No diagnosis code linked | Medical necessity denial |
| Duplicate billing | Same trip submitted twice | Fraud investigation |
Best NEMT Billing Software: Comparison Guide
Choosing the right NEMT billing software directly impacts clean claim rates, denial management efficiency, and days in accounts receivable. The best platform for your operation depends on fleet size, payer mix, integration requirements, and budget constraints.
This comparison covers the leading platforms across different market segments.
Top NEMT Billing Software Platforms
The NEMT software market ranges from all-in-one platforms handling dispatch through payment posting to specialized billing-focused solutions. Understanding each platform’s strengths helps match technology to operational needs.
| Platform | Best For | Core Strength | Pricing Model |
| Bambi NEMT | Small-mid fleets | AI-powered all-in-one | Per-vehicle/month |
| RouteGenie | Growing fleets | Routing + billing integration | Tiered subscription |
| TripMaster | Enterprise/paratransit | Multi-fleet management | Custom enterprise |
| MediRoutes | Billing-focused ops | Claims processing depth | Per-vehicle/month |
| AngelTrack | Dispatch-heavy ops | Dispatch + billing combo | Per-vehicle/month |
| Tobi Cloud | AR management | Billing + A/R automation | Subscription |
| CTS Software | EDI-heavy operations | Fleet + EDI strength | Custom pricing |
| Ecolane | Large enterprise | Enterprise-scale systems | Enterprise contract |
Essential NEMT Billing Software Features
When evaluating NEMT billing software, prioritize features that directly impact revenue cycle performance rather than flashy add-ons with minimal ROI.
Must-Have Billing Features
EDI 837P claim submission enables electronic claim filing to Medicaid, Medicare Advantage, brokers, and commercial payers. Manual claim submission is no longer viable at scale—EDI connectivity is table stakes.
Eligibility verification (EDI 270/271) automates real-time insurance verification before trips occur, preventing eligibility-related denials that waste service delivery resources.
Claim scrubbing identifies coding errors, modifier mismatches, and documentation gaps before submission. AI-powered claim scrubbing in platforms like Bambi NEMT catches errors that rule-based systems miss, pushing clean claim rates above 95%.
ERA auto-posting (EDI 835) automatically records payments and identifies underpayments, eliminating manual payment posting that delays revenue recognition and introduces errors.
Denial tracking and management provides systematic workflows for identifying denial patterns, managing appeals within timely filing limits, and recovering revenue that would otherwise be written off.
A/R aging reports surface claims approaching timely filing deadlines and highlight chronic slow-pay patterns requiring escalation.
Integration Requirements
Broker portal integration matters most for Medicaid-heavy operations. Direct API connections with ModivCare, MTM, Access2Care, and other brokers streamline trip assignment acceptance and claim submission.
Accounting software integration with QuickBooks or Xero eliminates duplicate data entry and ensures billing records reconcile with financial statements.
GPS and EVV compliance integration provides audit-proof mileage documentation and satisfies Electronic Visit Verification requirements increasingly mandated by state Medicaid programs.
NEMT Software Comparison by Fleet Size
Fleet size determines which platform category delivers optimal value. Overpaying for enterprise features or underinvesting in scalable infrastructure both hurt long-term profitability.
Small Fleets (1-10 Vehicles)
Priority: Ease of use, affordable pricing, all-in-one functionality
Best options: Bambi NEMT, RouteGenie, MediRoutes
Small fleet operators need platforms that handle dispatch, billing, and basic reporting without requiring dedicated administrative staff. Cloud-based solutions with per-vehicle pricing keep costs proportional to operation size. Avoid enterprise platforms with minimum seat requirements or complex implementation fees that don’t scale down.
Growing Fleets (10-50 Vehicles)
Priority: Scalability, multi-payer support, automation depth
Best options: RouteGenie, Tobi Cloud, AngelTrack
Growing operations face increasing complexity—multiple payer relationships, higher claim volumes, and growing denial management workload. Platforms with robust automation, strong broker integrations, and flexible reporting become essential. The billing complexity at this stage often exceeds what software alone can efficiently handle.
Enterprise Operations (50+ Vehicles)
Priority: Enterprise integration, custom workflows, dedicated support
Best options: TripMaster, Ecolane, CTS Software
Large-scale operations require enterprise-grade platforms with custom implementations, dedicated account management, and integration capabilities matching complex IT environments. Implementation timelines extend to 3-6 months with significant upfront investment.
Software Costs vs. Billing Service ROI
NEMT billing software typically costs $50-$200 per vehicle monthly depending on platform and feature tier. For a 20-vehicle fleet, annual software costs range from $12,000-$48,000 before accounting for staff time managing the billing function.
Beyond software licensing, in-house billing requires:
- Dedicated billing staff ($35,000-$55,000 annually per FTE)
- Ongoing training on payer rule changes
- Clearinghouse and EDI gateway fees
- Compliance monitoring and audit preparation
- Denial management time investment
The hidden cost calculation: A 20-vehicle fleet generating $1M in annual revenue with a 15% denial rate leaves $150,000 on the table. If software and staff recover half that amount, the investment pays off. But professional billing services routinely achieve 5-8% denial rates—recovering an additional $70,000-$100,000 annually while eliminating staffing overhead.
For many operators, particularly those scaling from 10-50 vehicles, professional NEMT billing services deliver better ROI than software-plus-staff approaches—recovering more revenue at lower total cost while freeing owners to focus on operations and growth.
Software Selection Checklist
Before committing to any platform, verify these requirements:
☐ Payer compatibility — Does the software support your specific state Medicaid program, brokers, and MA plans?
☐ Broker integrations — Are ModivCare, MTM, Access2Care, or your regional brokers directly integrated?
☐ Clean claim rate track record — What clean claim rates do similar-sized users achieve?
☐ Implementation timeline — How long until fully operational? What training is included?
☐ Contract terms — Monthly vs. annual commitment? Cancellation terms?
☐ Support quality — Response times? Dedicated account manager availability?
☐ Scalability — Will the platform grow with your fleet without requiring migration?
Request demos from at least three platforms, run parallel trials if possible, and speak with current users in similar-sized operations before committing.
Common NEMT Billing Errors That Cause Denials
Most NEMT claim denials stem from preventable errors—mistakes that systematic processes eliminate before claims ever reach payers. Understanding the most frequent denial triggers and implementing targeted prevention strategies pushes clean claim rates above 95% while recovering revenue that less disciplined operations write off.
Eligibility Verification Failures
Denial Code: PR-19 (Coverage not in effect)
The Problem: Billing for patients whose Medicaid coverage lapsed, expired, or was never active on the service date causes automatic denials with zero appeal success. Eligibility changes occur constantly—job changes, missed premium payments, annual recertification failures—and yesterday’s active coverage guarantees nothing about today.
The Solution: Verify eligibility within 24-48 hours before every scheduled trip using EDI 270/271 real-time eligibility checks. Recheck coverage for recurring patients weekly, not just at initial booking. Eligibility verification costs pennies per check; eligibility denials cost the entire trip revenue plus rework time.
HCPCS Coding Errors
Denial Code: CO-96 (Non-covered service based on coding)
The Problem: Using incorrect HCPCS codes for the service level provided—billing wheelchair transport codes for ambulatory patients, applying wrong mileage codes, or mismatching modifiers between base and mileage codes—triggers immediate rejection. Upcoding violations carry penalties reaching $10,000 per false claim plus potential fraud investigation.
The Solution: Implement automated claim scrubbing with payer-specific coding rules that catch errors before submission. Train dispatchers to document mobility level accurately at booking. Never change codes after service completion without documented justification and supervisor approval.
Documentation Gaps
Denial Code: CO-197 (Missing/incomplete documentation)
The Problem: Missing trip logs, unsigned attestations, incomplete Physician Certification Statements, or timestamp mismatches create documentation gaps that auditors flag immediately. Documentation errors cause 25-30% of initial denials and often result in permanent revenue loss when records cannot be reconstructed.
The Solution: Capture documentation electronically at point of service using mobile apps with required field validation that prevents incomplete submissions. Implement same-day documentation audits catching gaps while trips remain fresh. Store all records in audit-ready format with 7-10 year retention.
Authorization Failures
Denial Code: CO-16 (Claim lacks prior authorization)
The Problem: Providing service without required prior authorization—whether from brokers, Medicare Advantage plans, or Medicaid MCOs—results in non-payment regardless of medical necessity or service quality. Authorization requirements vary by payer, service level, and geography.
The Solution: Build authorization verification into pre-trip workflows. Integrate with broker portals to confirm trip assignments include valid authorization. For Medicare Advantage, verify authorization requirements before each trip—assumptions based on past patterns fail when plan rules change.
Mileage Discrepancies
Denial Code: Variable (audit-triggered)
The Problem: Mileage billing that doesn’t match GPS records, deviates from most-direct-route requirements, or shows patterns suggesting inflation (perfectly round numbers, identical distances across different routes) triggers fraud investigations. Mileage fraud penalties reach $10,000 per claim plus potential criminal prosecution.
The Solution: Use GPS-integrated mileage tracking with automated distance calculation via mapping APIs. Bill loaded miles only using the most direct route—never odometer readings alone. Review mileage patterns monthly for anomalies suggesting driver gaming or system errors.
Timely Filing Violations
Denial Code: CO-29 (Timely filing limit exceeded)
The Problem: Missing payer-specific filing deadlines results in permanent, non-appealable denials. Timely filing limits range from 90 days to one year depending on payer—and most providers underestimate how quickly deadlines arrive when billing backlogs accumulate.
The Solution: Implement claim aging reports with automated alerts at 30, 60, and 90 days. Prioritize oldest claims first during daily billing workflows. Never let claims age beyond 50% of the applicable timely filing limit without escalation.
Duplicate Claim Submissions
Denial Code: CO-18 (Duplicate claim)
The Problem: Submitting the same trip twice—whether through system errors, manual rework confusion, or inadequate tracking—triggers duplicate denials and potential overpayment recovery audits.
The Solution: Assign unique trip IDs at dispatch that carry through the entire billing lifecycle. Implement duplicate detection rules in billing software that flag potential duplicates before submission. Track claim status to prevent resubmission of claims already in adjudication.
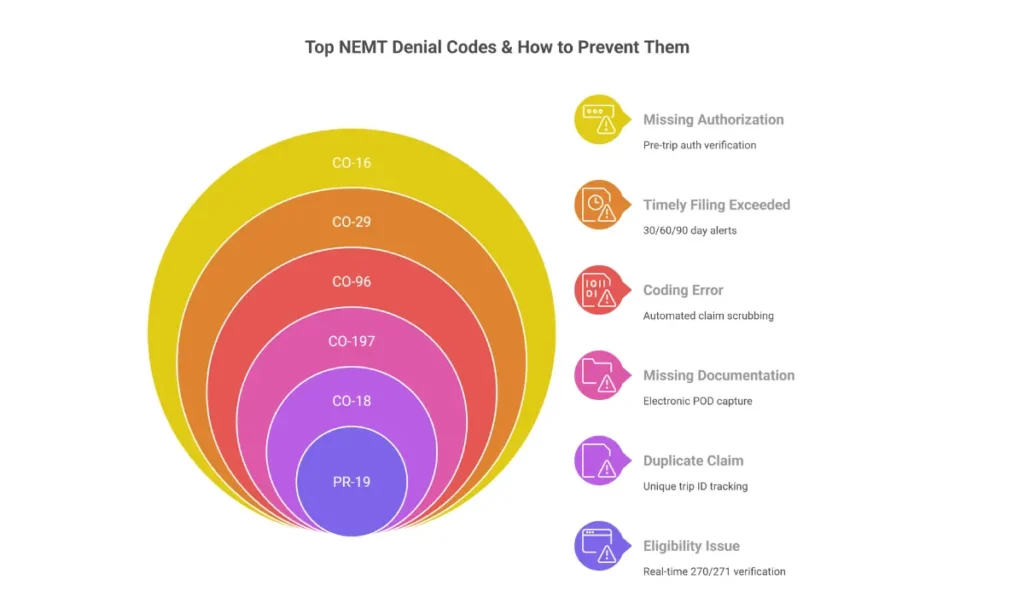
Denial Prevention Summary:
| Error Type | Prevention Method | Denial Code |
| Eligibility | EDI 270/271 real-time verification | PR-19 |
| Coding | Automated claim scrubbing | CO-96 |
| Documentation | Electronic POD with required fields | CO-197 |
| Authorization | Pre-trip auth verification workflow | CO-16 |
| Mileage | GPS-integrated tracking | Audit-triggered |
| Timely Filing | Aging reports with 30/60/90 alerts | CO-29 |
| Duplicates | Unique trip ID tracking | CO-18 |
NEMT Billing Compliance Requirements
NEMT providers operate under overlapping federal, state, and payer-specific compliance frameworks. Violations trigger penalties ranging from claim recoupment to program exclusion to criminal prosecution—consequences that can end businesses overnight.
Understanding compliance requirements isn’t about checking boxes. It’s about building systems that prevent violations before they occur.
HIPAA Requirements for NEMT Providers
NEMT providers are HIPAA-covered entities handling Protected Health Information (PHI) including patient names, Medicaid IDs, diagnoses, medical appointments, pickup/drop-off locations, and Physician Certification Statements. The HIPAA Privacy Rule (45 CFR § 164.500) and Security Rule (45 CFR § 164.308) impose specific obligations.
PHI Protection Requirements
Electronic PHI (ePHI) security requires encryption on all devices storing patient data—dispatch computers, billing systems, driver tablets, and mobile apps. Unencrypted devices containing ePHI create breach exposure with penalties reaching $1.9 million per violation category annually.
Access controls limit PHI access to workforce members with legitimate need. Drivers access only their assigned trips. Billing staff access only billing-relevant data. Unique user IDs and audit logs track all PHI access for investigation purposes.
Business Associate Agreements (BAAs) must be executed with every vendor handling PHI—billing software providers, dispatch platforms, clearinghouses, and third-party billing services. Without signed BAAs, PHI sharing with these vendors violates HIPAA regardless of actual security practices.
HIPAA Compliance Checklist
☐ Signed BAAs with all software and billing vendors ☐ Encrypted tablets and driver mobile devices ☐ Annual HIPAA training with documented completion ☐ Written HIPAA risk assessment (updated annually) ☐ Breach notification policy and incident response plan ☐ Minimum necessary access controls implemented
Federal Compliance Framework
Beyond HIPAA, NEMT providers face federal healthcare compliance requirements with severe penalties for violations.
The False Claims Act (31 U.S.C. § 3729) imposes liability for submitting false or fraudulent claims to government healthcare programs. Penalties range from $11,000-$22,000 per false claim plus treble damages—meaning providers pay three times the overpayment amount. Qui tam provisions allow whistleblowers to file lawsuits on behalf of the government, receiving 15-30% of recovered amounts.
The Anti-Kickback Statute prohibits offering, paying, soliciting, or receiving anything of value to induce referrals for services paid by federal healthcare programs. NEMT providers cannot pay facilities, social workers, or discharge planners for patient referrals—even informal arrangements trigger violations.
CMS Program Integrity requirements (42 CFR § 455) mandate self-reporting of identified overpayments within 60 days. Failure to report and refund overpayments constitutes False Claims Act violation independent of the original billing error.
OIG Exclusion Screening requires monthly verification that no employee or contractor appears on the List of Excluded Individuals/Entities (LEIE). Employing excluded individuals while billing federal programs violates law regardless of the individual’s role.
Audit Preparedness
Medicaid audits—whether from state agencies, brokers, or federal contractors—examine documentation, billing patterns, and compliance systems. Audit triggers include high denial rates, mileage outliers, duplicate claim patterns, and rapid service-level growth that suggests upcoding.
What Auditors Examine
- Trip documentation completeness — timestamps, signatures, addresses, mileage
- Medical necessity proof — PCS forms, diagnosis codes, appointment verification
- Mileage accuracy — GPS records matching billed distances via most direct route
- Service level justification — documentation supporting wheelchair/stretcher billing
- Billing pattern analysis — statistical outliers suggesting fraud indicators
Audit Response Requirements
Most audits require response within 30 days of findings notification. Responses must include supporting documentation for every questioned claim, corrective action plans for identified deficiencies, and refund calculations for confirmed overpayments.
Lookback periods extend 3-6 years depending on state and audit type. A single documentation deficiency pattern can trigger recoupment across thousands of historical claims.
Fraud Prevention Controls
NEMT fraud schemes that trigger criminal investigation and program exclusion include:
Ghost trips — billing for transportation never provided Signature falsification — forging patient signatures on trip logs Mileage inflation — billing distances exceeding actual travel Upcoding — billing wheelchair rates for ambulatory patients Kickback arrangements — paying for patient referrals
Fraud Prevention Checklist
☐ GPS verification for all mileage billing ☐ Electronic signature capture with timestamp validation ☐ Service level documentation matching mobility assessment ☐ Anti-kickback policy prohibiting referral payments ☐ Anonymous compliance hotline for employee reporting ☐ Monthly billing pattern analysis for statistical outliers
Record Retention Requirements
NEMT billing records must be retained for 7-10 years depending on state requirements and payer contracts—longer than many providers expect. Required records include:
- Trip logs with signatures and timestamps
- GPS route data and mileage verification
- Physician Certification Statements
- Eligibility verification records
- Claim submission and payment records
- Driver credentials and training documentation
- Vehicle inspection and maintenance records
Digital storage with secure backup ensures records remain accessible throughout retention periods while enabling rapid retrieval during audits.
Providers lacking internal compliance expertise benefit from professional billing services that maintain compliance programs, conduct internal audits, and ensure billing practices meet evolving regulatory requirements.
In-House vs Outsourced NEMT Billing: Which Delivers Better ROI?
The decision to manage billing internally or partner with a professional NEMT billing company affects revenue, compliance risk, and operational focus. Neither approach works universally—the right choice depends on fleet size, revenue volume, and growth trajectory.
Understanding the true cost comparison helps you make an informed decision.
True Cost of In-House NEMT Billing
In-house billing appears cheaper on paper—until you calculate total cost of ownership including salary, benefits, software, training, and hidden overhead.
Direct staffing costs:
- Experienced NEMT biller salary: $55,000-$85,000 annually
- Benefits and payroll taxes: 25-30% additional ($14,000-$25,000)
- Total per biller: $69,000-$110,000 annually
Operational costs:
- Billing software licensing: $6,000-$24,000 annually
- Clearinghouse and EDI fees: $1,200-$3,600 annually
- Continuing education and training: $1,000-$2,500 annually
- Compliance program maintenance: $2,000-$5,000 annually
Hidden costs:
- Hiring and onboarding (3-6 months to full productivity)
- Turnover replacement (average billing staff tenure: 2-3 years)
- Management oversight time
- Denial rework from inexperienced staff
- Compliance gaps during staff transitions
Total in-house cost for one biller: $80,000-$145,000 annually
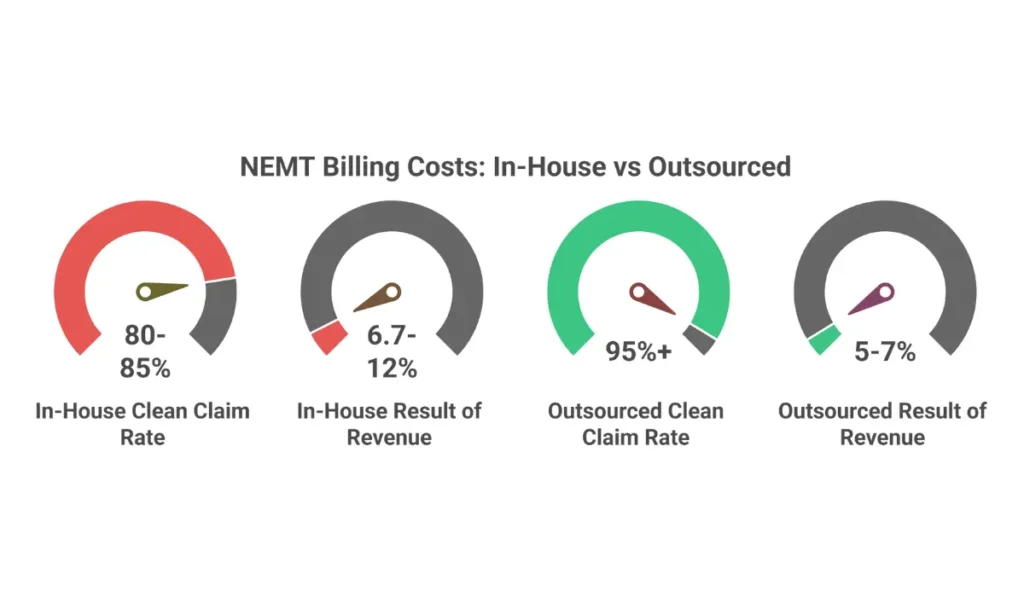
For a 20-vehicle fleet generating $1.2M revenue, in-house billing consumes 6.7-12% of gross revenue—before accounting for revenue lost to higher denial rates and slower collections.
Outsourced NEMT Billing Costs
Professional NEMT billing services typically charge 4-7% of collections—you pay only on revenue actually received, not on billed amounts or denied claims.
For the same 20-vehicle, $1.2M revenue fleet:
- At 5% of collections: $60,000 annually
- At 7% of collections: $84,000 annually
What’s included in professional billing fees:
- Eligibility verification (EDI 270/271)
- Claim scrubbing and submission
- ERA posting and reconciliation
- Denial management and appeals
- A/R follow-up and collections
- Compliance monitoring
- Reporting and analytics
- Staff training and turnover absorbed by provider
The cost advantage compounds because professional billing services achieve higher collection rates (95%+ clean claim rates vs. 80-85% typical in-house), faster reimbursement (reducing A/R days from 60-90 to 30-45), and lower denial rates (5-8% vs. 15-20%).
Decision Framework by Fleet Size
Small fleets (1-10 vehicles): Outsourcing almost always wins. Revenue volume doesn’t justify dedicated billing staff, and owner time spent on billing subtracts from growth activities. A 5-vehicle operation generating $300K annually pays approximately $15,000-$21,000 for professional billing—less than a part-time biller’s salary.
Growing fleets (10-30 vehicles): The critical decision zone. Operations at this size often attempt in-house billing, discover complexity exceeds expectations, and experience revenue leakage from denials and compliance gaps. Professional NEMT billing services deliver superior ROI while freeing ownership to focus on fleet expansion and operational excellence.
Large fleets (30+ vehicles): Hybrid models become viable. Large operations may employ internal billing coordinators handling day-to-day tasks while outsourcing complex denial management, appeals, and compliance monitoring to specialists.
When to Outsource NEMT Billing
Consider outsourcing when:
☐ Denial rates exceed 10% consistently ☐ Days in A/R exceed 60 days ☐ Staff turnover disrupts billing continuity ☐ Compliance requirements overwhelm internal capacity ☐ Growth plans require owner focus on operations, not billing ☐ Multi-state or multi-broker complexity increases ☐ Clean claim rates fall below 90%
The question isn’t whether you can bill internally—it’s whether internal billing delivers the best return on your time and capital compared to professional alternatives.
For most NEMT operators, outsourced billing services recover more revenue at lower total cost while eliminating compliance risk and freeing ownership for higher-value activities.
How to Optimize NEMT Billing Revenue
Revenue optimization extends beyond simply submitting claims. It requires systematic measurement, strategic payer management, and continuous process improvement that compounds over time. Providers tracking the right KPIs and implementing proven optimization strategies consistently outperform competitors by 20-40% on key financial metrics.
Essential NEMT Billing KPIs
You can’t optimize what you don’t measure. These key performance indicators reveal billing health and identify improvement opportunities.
| KPI | Target | Average | Poor |
| Clean Claim Rate | 95%+ | 85-90% | <80% |
| Denial Rate | <5% | 10-15% | >20% |
| Days in A/R | <30 days | 45-60 days | >90 days |
| Collection Rate | >95% | 85-90% | <80% |
| First-Pass Pay Rate | >90% | 75-85% | <70% |
| Cost Per Claim | <$5 | $8-$12 | >$15 |
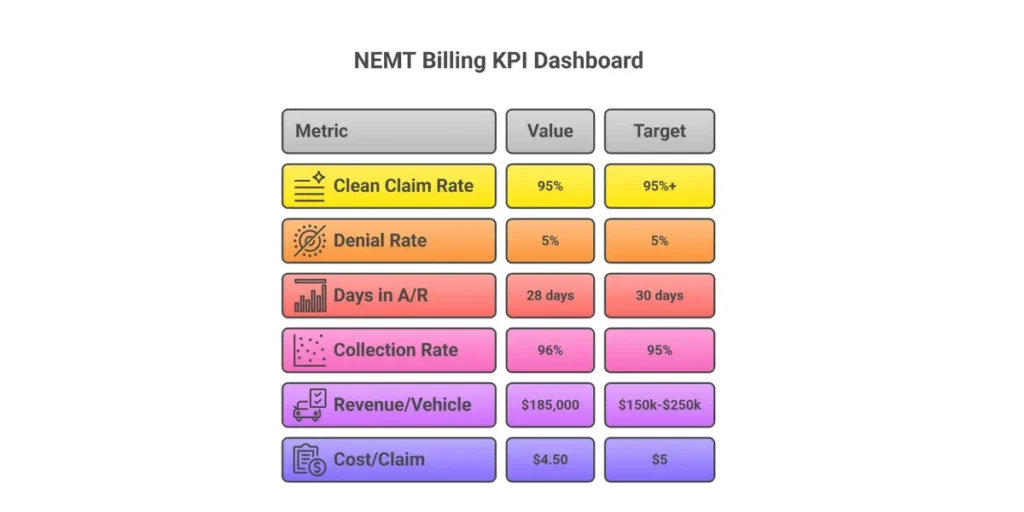
Revenue per vehicle benchmarks help contextualize overall performance. Well-optimized NEMT operations generate $150,000-$250,000 annually per vehicle—operations falling significantly below this range likely have billing inefficiencies, unfavorable payer mix, or operational issues limiting trip volume.
Revenue Optimization Strategies
Reduce Denial Rates
Every denied claim represents revenue at risk. With average denial rates of 10-15% and appeal success rates of 50-65%, providers leave significant money on the table.
High-impact denial reduction tactics:
- Implement real-time eligibility verification eliminating coverage-related denials
- Deploy AI-powered claim scrubbing catching coding errors before submission
- Standardize documentation workflows preventing incomplete claim submissions
- Track denial patterns by code and payer to address root causes systematically
Reducing denial rates from 15% to 5% on $1M revenue recovers $100,000 annually—often the single highest-ROI improvement available.
Accelerate Cash Flow
Days in A/R directly impacts working capital and growth capacity. Reducing A/R from 60 days to 30 days effectively doubles cash velocity without increasing revenue.
Cash flow acceleration tactics:
- Submit claims within 24-48 hours of service completion
- Implement automated ERA posting eliminating payment reconciliation delays
- Establish systematic follow-up at 14, 30, and 45-day intervals
- Prioritize high-dollar aged claims for immediate attention
Optimize Payer Mix
Not all payers deliver equal value. Private pay and Medicare Advantage typically offer higher reimbursement and faster payment than Medicaid, while broker relationships provide volume stability with moderate rates.
Payer mix optimization approach:
- Analyze revenue and margin by payer to identify most profitable relationships
- Pursue Medicare Advantage network participation for higher-margin trips
- Develop private pay marketing for premium service offerings
- Negotiate broker rate increases based on performance metrics and capacity
Shifting payer mix from 90% Medicaid to a diversified portfolio (55% Medicaid, 25% broker, 15% MA, 5% private) can increase average revenue per trip by 15-25%.
Capture Revenue Leakage
Revenue leakage occurs when billable services go unbilled—missed trips, incorrect coding, documentation gaps, and timely filing failures.
Leakage prevention tactics:
- Audit trip logs against billing records weekly to identify unbilled services
- Implement dispatch-to-billing integration eliminating manual handoff errors
- Review write-offs monthly for patterns indicating systemic issues
- Track timely filing compliance preventing deadline-related losses
Measuring Optimization ROI
Track improvement over 90-day cycles to measure optimization initiative effectiveness:
Baseline metrics (Day 1):
- Current clean claim rate, denial rate, days in A/R
- Revenue per vehicle, collection rate
- Cost per claim
Progress metrics (Day 90):
- Same KPIs measured against baseline
- Dollar value of improvements calculated
- ROI on optimization investments quantified
Providers implementing systematic optimization—whether through internal process improvement or professional billing partnerships—typically see measurable improvement within 90 days, with full optimization benefits realized over 6-12 months.
Frequently Asked Questions About NEMT Billing
What Is NEMT Billing?
NEMT billing is the process of submitting claims to Medicaid, Medicare Advantage, brokers, and private insurers for non-emergency medical transportation services. It includes eligibility verification, trip documentation, HCPCS coding, electronic claim submission via EDI 837P, payment posting, and denial management. Professional NEMT billing requires understanding payer-specific rules, compliance requirements, and revenue cycle optimization.
How Do You Bill for NEMT Services?
NEMT billing follows a seven-step process: (1) verify patient eligibility 24-48 hours before service, (2) document trips with GPS mileage, timestamps, and signatures, (3) assign correct HCPCS codes and modifiers, (4) scrub claims for errors, (5) submit via EDI 837P within timely filing limits, (6) post payments and reconcile ERAs, (7) manage denials and appeals. Automation increases clean claim rates above 92% and reduces denials by up to 20%.
How Do You Bill Medicaid for NEMT?
To bill Medicaid for NEMT, providers must enroll with their state Medicaid program or contracted broker (ModivCare, MTM, Access2Care), verify patient eligibility before each trip, obtain required authorizations, document services with GPS-verified mileage and signatures, and submit EDI 837P claims using state-specific HCPCS codes. Filing deadlines range from 90-365 days depending on state. Medicaid pays $20-$100 per trip depending on service level and state rates.
What HCPCS Codes Are Used for NEMT Billing?
Common NEMT HCPCS codes include A0080 (wheelchair mileage), A0090 (ambulette), A0100 (taxi), A0130 (wheelchair van mileage), T2001-T2005 (commercial NEMT transport), and S0209/S0215 (mileage add-ons). Each code requires matching origin/destination modifiers (R for residence, H for hospital, P for physician office, etc.) and appropriate ICD-10 diagnosis codes establishing medical necessity.
What Documents Are Required for NEMT Billing?
NEMT billing requires trip logs with pickup/drop-off addresses, GPS-verified mileage, sequential timestamps, patient signatures, driver attestation, and linked HCPCS/ICD-10 codes. Wheelchair and stretcher transport require Physician Certification Statements (PCS) documenting medical necessity. All records must be HIPAA-compliant and retained for 7-10 years. Missing documentation causes approximately 22% of NEMT claim denials.
How Much Does Medicaid Pay for NEMT?
Medicaid NEMT reimbursement varies by state and service level. Typical rates include $20-$50 for ambulatory trips, $40-$100 for wheelchair transport, and $150-$300 for stretcher services, plus $2-$5 per loaded mile. Broker-contracted rates may differ from direct Medicaid fee schedules. Payment timelines range from 15-60 days depending on state and submission method.
Does Medicare Cover NEMT?
What Is NEMT Billing?
NEMT billing is the process of submitting claims to Medicaid, Medicare Advantage, brokers, and private insurers for non-emergency medical transportation services. It includes eligibility verification, trip documentation, HCPCS coding, electronic claim submission via EDI 837P, payment posting, and denial management. Professional NEMT billing requires understanding payer-specific rules, compliance requirements, and revenue cycle optimization.
How Do You Bill for NEMT Services?
NEMT billing follows a seven-step process: (1) verify patient eligibility 24-48 hours before service, (2) document trips with GPS mileage, timestamps, and signatures, (3) assign correct HCPCS codes and modifiers, (4) scrub claims for errors, (5) submit via EDI 837P within timely filing limits, (6) post payments and reconcile ERAs, (7) manage denials and appeals. Automation increases clean claim rates above 92% and reduces denials by up to 20%.
How Do You Bill Medicaid for NEMT?
To bill Medicaid for NEMT, providers must enroll with their state Medicaid program or contracted broker (ModivCare, MTM, Access2Care), verify patient eligibility before each trip, obtain required authorizations, document services with GPS-verified mileage and signatures, and submit EDI 837P claims using state-specific HCPCS codes. Filing deadlines range from 90-365 days depending on state. Medicaid pays $20-$100 per trip depending on service level and state rates.
What HCPCS Codes Are Used for NEMT Billing?
Common NEMT HCPCS codes include A0080 (wheelchair mileage), A0090 (ambulette), A0100 (taxi), A0130 (wheelchair van mileage), T2001-T2005 (commercial NEMT transport), and S0209/S0215 (mileage add-ons). Each code requires matching origin/destination modifiers (R for residence, H for hospital, P for physician office, etc.) and appropriate ICD-10 diagnosis codes establishing medical necessity.
What Documents Are Required for NEMT Billing?
NEMT billing requires trip logs with pickup/drop-off addresses, GPS-verified mileage, sequential timestamps, patient signatures, driver attestation, and linked HCPCS/ICD-10 codes. Wheelchair and stretcher transport require Physician Certification Statements (PCS) documenting medical necessity. All records must be HIPAA-compliant and retained for 7-10 years. Missing documentation causes approximately 22% of NEMT claim denials.
How Much Does Medicaid Pay for NEMT?
Medicaid NEMT reimbursement varies by state and service level. Typical rates include $20-$50 for ambulatory trips, $40-$100 for wheelchair transport, and $150-$300 for stretcher services, plus $2-$5 per loaded mile. Broker-contracted rates may differ from direct Medicaid fee schedules. Payment timelines range from 15-60 days depending on state and submission method.
Is NEMT Covered by Private Insurance?
Private insurance NEMT coverage varies by plan and is not federally mandated. Coverage is most common for dialysis transportation, chemotherapy appointments, post-surgical discharge, and ongoing rehabilitation. When covered, private insurers typically pay $30-$150 per trip depending on service level. Prior authorization is usually required. Many patients pay privately when insurance doesn’t cover transportation.
How Much Should You Charge for NEMT Services?
Private-pay NEMT rates typically range from $35-$75 for ambulatory trips, $60-$150 for wheelchair transport, and $200-$400 for stretcher services, plus mileage ($2-$6 per mile). Pricing should target 25-35% profit margins after accounting for vehicle costs, driver wages, fuel, insurance, and administrative overhead. Medicaid and broker rates are regulated and non-negotiable in most states.
How Much Do NEMT Business Owners Make?
NEMT business owners typically earn $100,000-$500,000+ annually depending on fleet size, payer mix, operational efficiency, and local market conditions. A well-managed 20-vehicle fleet generating $1.2M in annual revenue can net approximately $300,000-$420,000 at industry-standard 25-35% profit margins. Revenue per vehicle ranges from $150,000-$250,000 annually for optimized operations.
What Is a Good Clean Claim Rate for NEMT?
A good NEMT clean claim rate exceeds 95%, meaning 95% or more of submitted claims are accepted on first submission without rejection or denial. Industry average is 85-90%, while poorly managed operations fall below 80%. Each percentage point improvement in clean claim rate directly increases revenue and reduces administrative rework costs. AI-powered claim scrubbing helps achieve 95%+ rates.
What Causes NEMT Claim Denials?
Common NEMT denial causes include eligibility issues (PR-19), coding errors (CO-96), missing documentation (COWhat Causes NEMT Claim Denials?
197), lack of prior authorization (CO-16), timely filing violations (CO-29), and duplicate submissions (CO-18). Industry-wide denial rates average 10-20%, though optimized operations achieve under 5%. Approximately 65% of denied claims are never appealed, representing significant recoverable revenue.
How Long Do You Have to Bill for NEMT?
NEMT timely filing limits vary by payer: Medicaid programs typically require 90-180 days, some states allow up to 365 days, Medicare Advantage plans range from 90-365 days, and brokers often require 30-90 days. Missing timely filing deadlines results in permanent, non-appealable claim denials. Implementing claim aging alerts at 30, 60, and 90 days prevents deadline-related revenue loss.
Should I Outsource NEMT Billing?
Consider outsourcing NEMT billing when denial rates exceed 10%, A/R days exceed 60, staff turnover disrupts continuity, or growth requires owner focus on operations rather than billing. Outsourced billing typically costs 4-7% of collections while achieving 95%+ clean claim rates—often delivering 20-40% more net revenue than in-house billing for fleets under 50 vehicles. Learn more about professional NEMT billing services.
What Is the Golden Rule of Medical Billing?
The golden rule of medical billing is to bill only for services that were actually rendered, medically necessary, and fully documented. This principle prevents fraud violations under the False Claims Act, reduces audit exposure, and ensures sustainable revenue. Accurate documentation supports every claim—if it isn’t documented, it didn’t happen and cannot be billed.
How Do NEMT Brokers Work?
NEMT brokers (ModivCare, MTM, Access2Care, Veyo) manage Medicaid transportation benefits on behalf of state agencies. Brokers assign trips to credentialed providers, set reimbursement rates, process claims, and issue payments within 15-30 days. Providers must complete broker credentialing, maintain performance metrics (on-time percentage, complaint rates), and submit claims through broker portals or APIs.
What Is a PCS Form in NEMT?
A Physician Certification Statement (PCS) is a medical necessity document signed by a physician certifying that a patient requires wheelchair or stretcher transportation due to mobility limitations. PCS forms are required for non-ambulatory NEMT claims in most state Medicaid programs. Valid PCS must include diagnosis, mobility limitation description, and physician signature with credentials. Validity periods range from 30-180 days depending on state.
How Long Must NEMT Records Be Retained?
NEMT billing records must be retained for 7-10 years depending on state Medicaid requirements and payer contracts. Required records include trip logs, GPS data, signatures, Physician Certification Statements, eligibility verification records, claim submissions, payment documentation, driver credentials, and vehicle records. Digital storage with secure backup ensures compliance while enabling rapid audit retrieval.
Is NEMT Billing Profitable?
Yes, NEMT billing is profitable when executed correctly. Well-managed operations achieve 25-35% profit margins with 95%+ clean claim rates and under 30 days in A/R. The $10.8 billion NEMT market growing to $19.9 billion by 2034 provides sustainable demand backed by Medicaid’s federal transportation mandate. Profitability depends on denial management, payer mix optimization, and operational efficiency.
What Software Do NEMT Companies Use for Billing?
NEMT companies use specialized billing software including Bambi NEMT, RouteGenie, TripMaster, MediRoutes, AngelTrack, and Tobi Cloud. Essential features include EDI 837P claim submission, eligibility verification (270/271), claim scrubbing, ERA auto-posting (835), denial management, broker portal integration, and compliance reporting. Platform selection depends on fleet size, payer mix, and integration requirements.
Conclusion: Mastering NEMT Billing for Sustainable Growth
NEMT billing complexity separates thriving operations from struggling ones. The providers who master eligibility verification, documentation, coding, compliance, and denial management consistently outperform competitors—achieving 95%+ clean claim rates, under 30 days in A/R, and 25-35% profit margins that fund sustainable growth.
The fundamentals covered in this guide provide the foundation. Implementation determines outcomes.
For providers ready to optimize their billing operations, the path forward depends on current performance and growth trajectory:
- Operations with denial rates above 10% should prioritize eligibility verification and claim scrubbing improvements
- Operations with A/R exceeding 60 days need systematic follow-up processes and payment posting automation
- Growing operations approaching 10+ vehicles should evaluate whether in-house billing complexity warrants professional partnership
Whatever approach you choose, measuring KPIs, tracking improvement, and continuously refining processes separates sustainable NEMT businesses from those leaving revenue on the table.
Contact EliteMed Financials to discuss how professional NEMT billing services can optimize your revenue cycle, reduce denials, and accelerate cash flow—letting you focus on growing your transportation business.
Ready to Optimize Your NEMT Billing?
Stop leaving revenue on the table. Whether you’re struggling with denials, compliance complexity, or cash flow delays, professional NEMT billing services can transform your operation’s financial performance.

