
Let me start with a number that should stop you cold: $200,000. That’s how much the average mid-sized wound care practice leaves on the table every single year — not because they’re delivering bad care, but because their revenue cycle wasn’t built for the complexity of what they actually do.
Wound care billing isn’t general medical billing with a specialty twist. It’s a completely different animal. The coding is depth-dependent, the documentation standards are hyper-specific, the payer rules shift by jurisdiction, and the regulatory environment has tightened significantly heading into 2026. If your revenue cycle was designed by someone who learned it billing for family practice, you are almost certainly losing money on procedures you’ve already performed.
This guide covers everything — from the definition of wound care RCM to the exact leakage points draining your practice, the 2026 CMS changes that caught a lot of practices off guard, and the denial prevention strategies that can realistically cut your rejection rate from 25–30% down to single digits. If you want the short version: wound care is one of the highest-value, highest-complexity billing specialties in outpatient medicine. Get it right, and the financial impact is dramatic. Get it wrong, and you’re funding your denials instead of your growth.
Already know the basics and just want an expert team handling this for you? See our wound care billing services — we handle the entire cycle.
Table of Contents
What Is Wound Care RCM?
Wound care revenue cycle management (RCM) is the specialized, end-to-end process of managing every financial transaction that flows through a wound care practice — from the moment a patient schedules their first appointment to the day the final payment posts on the last claim. That sounds simple until you realize what that actually involves for a wound clinic.
General RCM is built around predictable procedure codes, standard documentation, and payer rules that apply consistently across most specialties. Wound care RCM has none of those luxuries. Every debridement requires depth-based CPT code selection, meaning the code you bill depends on the deepest tissue layer removed during the procedure — not the surface appearance of the wound. That’s CPT 11042 for subcutaneous tissue, 11043 for muscle and fascia, and 11044 for bone — each requiring specific documentation to survive an audit. Skin substitute applications trigger HCPCS Q41xx codes under the 2026 CMS flat-rate model at $127.14 per square centimeter. Diabetic foot ulcers require dual ICD-10 coding in the correct sequence (etiology code E11.621 before the manifestation code L97.5xx) — miss that sequence and you’re looking at an automatic CO-97 denial.
This is why wound care denial rates average 15–30% compared to 10–15% for general medical billing. The complexity is built into the nature of the specialty itself. A wound care RCM framework that actually works has to account for MAC-specific Local Coverage Determinations (LCDs), NCCI bundling edits, the 12/360 frequency rule, prior authorization requirements for biologics, and documentation standards that can withstand post-payment audits from CMS, OIG, and CERT reviewers.
In short: wound care RCM is the financial backbone that ensures your clinic gets paid for the complex, high-value care you deliver — and protects you from the compliance exposure that comes when it isn’t done correctly.
Why Wound Care Billing Is Genuinely More Complex Than General Practice
If you’ve ever tried to explain wound care billing to a general medical biller, you’ve probably watched their eyes glaze over at the words “depth-based CPT selection.” The complexity here isn’t just academic — it has real dollar consequences. Here’s what makes it different:
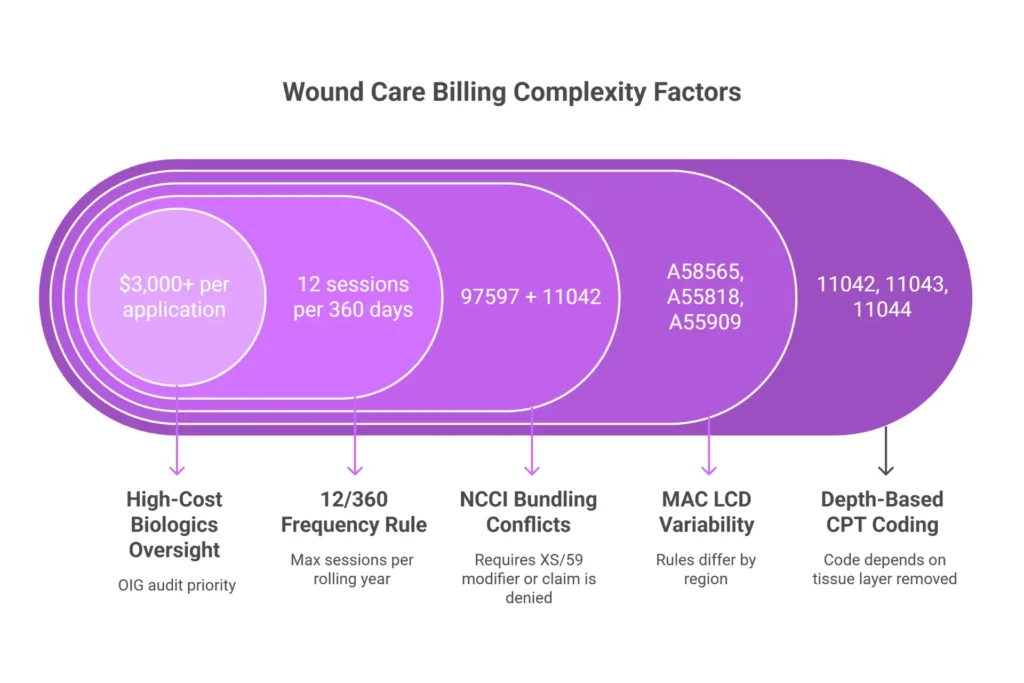
Depth-based CPT selection. The code you bill for debridement is determined by the deepest tissue layer you removed, not the visible wound depth. A wound can look like a subcutaneous debridement and actually require an 11043 (muscle/fascia) based on the tissue your physician documented removing. Upcoding and downcoding both create risk here — one triggers audits, the other leaves money on the table.
MAC LCD variability. Your Medicare Administrative Contractor (MAC) determines which diagnoses qualify for coverage under your jurisdiction. Noridian’s LCD A58565 (Rev 11, effective January 2026) lists 1,173 Group 1 ICD-10 codes. Palmetto GBA’s A55818 has different criteria. CGS’s A55909 enforces its own documentation requirements including serial wound photos. A claim that flies through Noridian can get denied under Palmetto for the same procedure with the same documentation. If your billing team doesn’t know which MAC covers your jurisdiction — or doesn’t know what changed in the most recent LCD update — you’re billing blind.
NCCI bundling conflicts. The National Correct Coding Initiative Chapter 4G contains bundling edits that are specific to wound care and not always intuitive. Billing 97597 (selective debridement) alongside 11042 (surgical debridement) on the same date triggers automatic bundling. The 29580 compression application bundles with debridement codes under the limb bundle rule. These aren’t errors your team will catch by reading the CPT manual — they require wound-specific scrubbing logic built into your clearinghouse or billing platform.
The 12/360 rule. Medicare limits debridement procedures (CPT 97597–11047) to 12 sessions per 360-day rolling period. Exceed that without an Advance Beneficiary Notice (ABN), a KX modifier, and documented medical necessity, and you have a denial that cannot be appealed. These aren’t recoverable — they’re permanent write-offs.
High-cost biologics and skin substitutes. A single skin substitute application can generate a claim worth $3,000 or more. The 2026 CMS flat-rate model changed how these are billed and reimbursed. The documentation requirements to survive prior authorization, receive correct payment, and withstand audit scrutiny are extensive. Federal investigators have already prosecuted a $1 billion amniotic allograft fraud scheme — which means every wound clinic billing skin substitutes is operating under heightened oversight.
This is the environment your revenue cycle has to navigate every single day.
The 7 Stages of the Wound Care Revenue Cycle
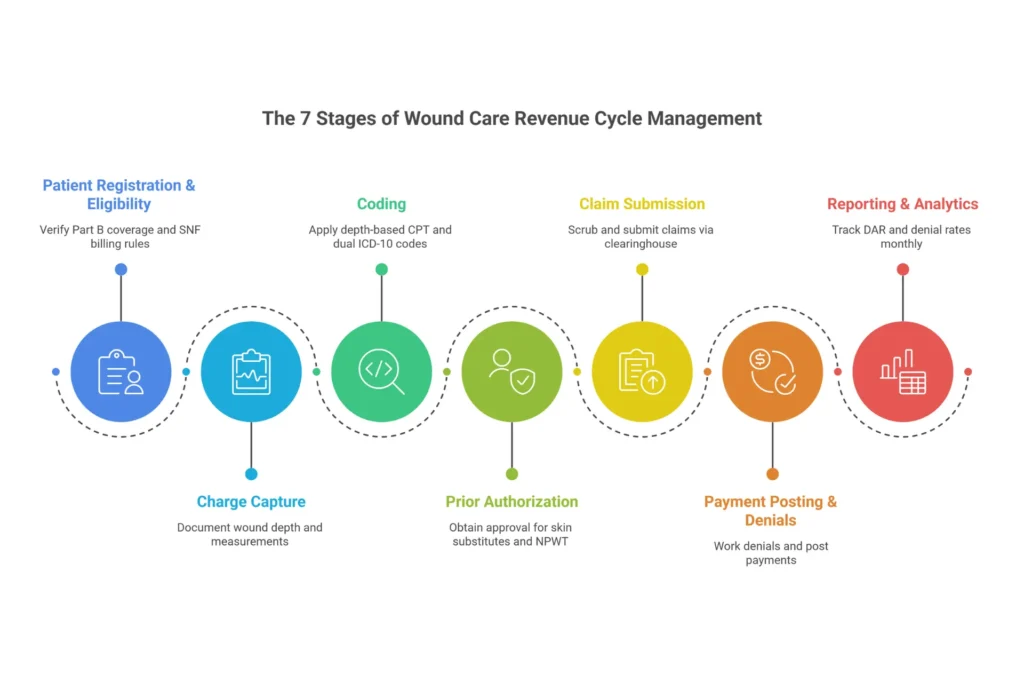
A lot of practices think of their revenue cycle as “billing and collections.” The reality is that a functional wound care RCM has seven distinct stages, and failure at any one of them creates downstream problems that compound into serious revenue loss. Here’s how each stage works in practice:
Stage 1: Patient Registration and Eligibility Verification
Everything starts here, and mistakes here are the most expensive kind — because you often don’t discover them until after you’ve delivered care. For wound care, eligibility verification means more than confirming that a patient has active insurance. You need to determine whether they’re under Medicare Part A (SNF consolidated billing rules) or Part B outpatient coverage. Treating a patient who’s in a covered SNF Part A stay and billing Medicare Part B directly results in automatic denials and complicated recoupment situations that require retroactive rebilling.
For skin substitute applications, you need to verify coverage for biologics under the specific payer — approximately 80–90% of Medicare Advantage plans require prior authorization for advanced biologics, and that authorization process starts at registration, not on the day of service. Revenue codes for facility billing (0361, 0510, 0761 on the UB-04) need to be mapped correctly from the start.
Practices that run automated eligibility verification catch 15% of potential denials before they ever submit a claim. That’s not a small number.
If Your Practice Uses Wound Care Grafts, Product Selection Is a Revenue Cycle Decision
Most practices treat graft procurement and billing as two separate workflows. That separation is exactly where denials originate. An unverified graft product — one without pre-confirmed FDA HCT/P documentation, a correct Q-code assignment, and patient-specific Medicare eligibility confirmed before the application — is one of the leading causes of skin substitute claim denials and RAC audit flags at the eligibility stage.
Product selection needs to be made during Stage 1 — not on the day of application. Confirming that the specific product is covered under your MAC's active LCD, that the Q-code is pre-loaded, and that the patient's insurance is active before you order the graft is what keeps your graft claims clean from the first submission.
Patient Medicare coverage, LCD compliance, and prior auth status confirmed before every graft order — not after application
Correct Q-code pre-loaded from FDA documentation before shipment — Q-code on claim matches product in hands, every time
6-Year Claims Protection backs every verified graft claim with active audit defense — the only program of its kind in wound care
Our verified graft program integrates directly into your RCM workflow — provider verification, manufacturer documentation, and patient insurance all confirmed at Stage 1, before you ever apply the product.
See our verified graft program →Stage 2: Charge Capture
Charge capture is where clinical documentation translates into billable services — and it’s also where a significant portion of wound care revenue quietly disappears. Charge lag (the gap between service delivery and charge entry) should stay under 3–7 days. Let it stretch to 15–30 days and you’re not just dealing with cash flow delays; you’re losing add-on codes that don’t get captured because no one went back to document additional wound areas treated in the same session.
Add-on codes are the single biggest per-visit leakage point in wound care. CPT +11045, +11046, +11047, and +97598 are add-on codes for additional surface area debrided beyond the initial 20 square centimeters. A wound that covers 45 square centimeters should generate the primary code plus at least one add-on. Most general billing workflows don’t flag this. Specialized wound care billing does — and the difference is $100–$400 per visit, which adds up to $36,000–$96,000 per year for a practice doing 2,000 annual visits with even a 20% miss rate.
EHR templates that auto-populate wound measurements and prompt for add-on code capture reduce this leakage dramatically. This is one of the core reasons why specialized medical billing services deliver better financial outcomes than generalist teams — the workflows are built for the specialty.
Stage 3: Professional and Facility Coding
This is the technical heart of wound care RCM and the stage where CWCC (Certified Wound Care Coder) certification makes a measurable difference. CWCC-certified coders achieve 18% lower denial rates — 12% versus 30% for uncertified teams — and 95% first-pass rates compared to 80% for non-certified billers. That’s not marketing language; it’s the difference between coders who know that 11044 requires radiographic or clinical bone exposure documentation and those who bill it based on wound depth alone.
For diabetic foot ulcers, coding requires the etiology code (E11.621 for Type 2 diabetes with foot ulcer) before the manifestation code (L97.5xx for the ulcer location). Reverse the sequence and you trigger CO-97 denials in 40% of diabetic wound claims. Add correct ICD-10 specificity (laterality, depth, bone exposure) and you protect the claim from both denial and audit exposure.
Skin substitute applications under the 2026 model require HCPCS Q41xx codes paired with CPT 15271–15278, with precise square centimeter documentation. Our medical coding services include wound-specific code validation built around the latest CMS guidance — including the January 2026 changes that caught many practices unprepared.
Stage 4: Prior Authorization
Prior authorization for skin substitutes and NPWT is one of the most time-consuming and denial-prone stages in wound care RCM. For Medicare Advantage plans, roughly 90% require prior authorization for advanced biologics. The documentation package required is substantial: four weeks of conservative care failure (with dated wound measurements and photos proving the wound failed to heal), Wagner grade assessment, ABI/TCOM vascular studies, and complete treatment history.
Missing documentation results in 60–70% denial rates for advanced therapies before you’ve even submitted the claim. Authorization caps (typically 8 applications per 16-week period) need to be tracked per patient, per wound. Expiration dates need to be monitored. Payer-specific variations — Aetna’s 30-day conservative care requirement, UnitedHealthcare’s >1cm² DFU criteria, MassHealth’s surgeon requirement — need to be built into your intake workflow. This is a stage that genuinely rewards automation and penalizes manual tracking.
Stage 5: Claims Submission and Scrubbing
Before any wound care claim hits the clearinghouse, it needs specialty-specific scrubbing — and that means more than running standard NCCI edits. It means validating depth-based CPT selection against documented tissue type, checking that NCCI bundled pairs like 11042 and 29580 are separated with correct modifiers, verifying that Q41xx square centimeter units match the documented surface area, and confirming that the place of service code (POS 11 for office, POS 22 for HOPD) is correct for the setting.
Standard clearinghouse edit engines catch syntax errors and basic format problems. They don’t catch wound-specific bundling issues, depth documentation mismatches, or MAC LCD compliance problems. That gap is why unscrubbed wound care claims face 20–25% rejection rates. Practices using wound-specific pre-submission scrubbing routinely see this drop to 5% or less.
Stage 6: Payment Posting and Denial Management
Payment posting for wound care isn’t just matching ERA payments to claims — it’s actively auditing every remittance for underpayments. The 2026 Q41xx flat-rate transition created a wave of underpayments for practices that didn’t recalculate their square centimeter documentation. A miscalculation of even 5 square centimeters on a $3,000 skin substitute claim can result in $635 in underpayment per application. Across a moderate-volume practice, that’s $500–$1,000 per application in silent losses that never generate a denial code — they just post at lower than expected amounts.
CO-97 denials (35–40% of all wound care denials) should be worked within a 14-day window. The Level 1 Redetermination success rate for wound care CO-97 denials is 60–70% when the appeal bundle includes initial assessment, vascular study results, 4 weeks of progress notes showing measurable wound reduction (≥20%), serial photos, and depth documentation citing the specific LCD. That 60–70% success rate drops below 15% without complete documentation. This is not a stage where volume-based billing teams can afford to be reactive.
Stage 7: Reporting and Analytics
The practices that consistently outperform their peers on revenue aren’t working harder — they’re working from better data. Monthly KPI reviews should track Days in AR (target: under 35 days), denial rates by CPT category, first-pass claim rate (target: above 95%), net collection ratio (target: above 95–96%), and payer mix trends. Supply margin reports comparing biologic acquisition cost against collected reimbursement tell you whether your skin substitute program is actually profitable.
The benchmark that most practices ignore is service-specific denial trending. Debridement codes averaging 20–25% denials, skin substitutes averaging 25–35%, and NPWT averaging 20–30% all require different corrective actions. Aggregate denial rates hide the signal. CPT-level denial data reveals exactly where your revenue is leaking — and makes it fixable.
Wound Care-Specific KPIs: The Numbers That Tell You What’s Actually Happening
You can’t fix what you can’t measure. Here’s what the benchmarks actually look like for wound care — and what the numbers mean in practical terms:
Days in Accounts Receivable (DAR)
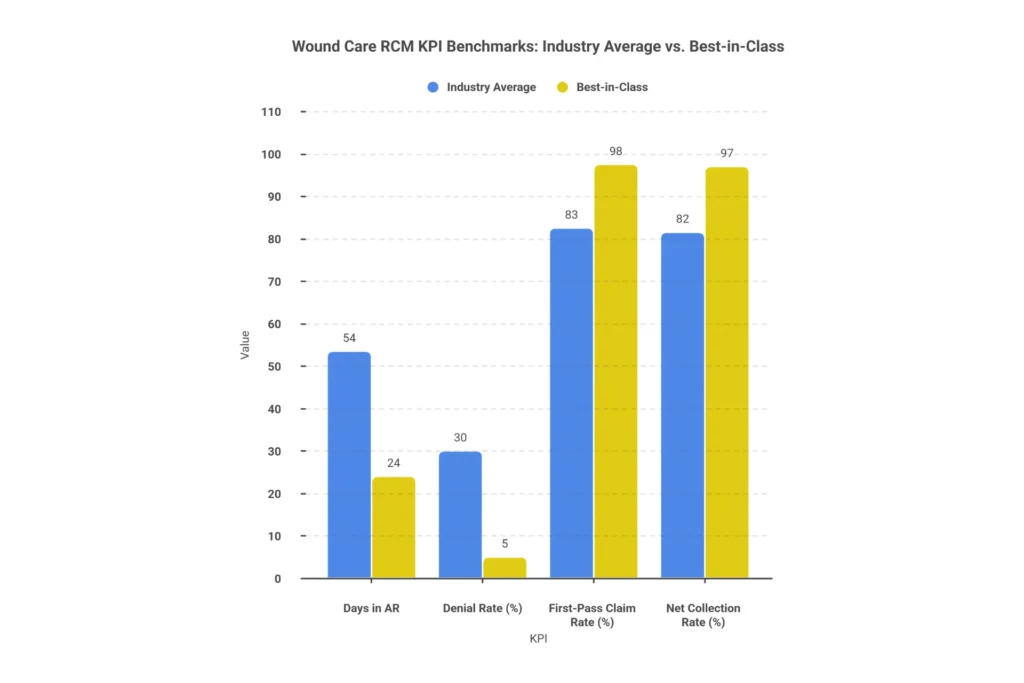
The wound care industry average for Days in AR is 45–62 days, meaningfully higher than general outpatient medicine. Prior authorization holds for skin substitutes add 20–30 days. CO-97 denial appeals add 45+ days. Best-in-class specialized RCM teams achieve 22–26 days through automated scrubbing and proactive authorization tracking. A DAR above 60 days isn’t just a cash flow problem — it’s a signal that there are systematic process failures in your revenue cycle worth investigating.
First-Pass Claim Rate
The industry average first-pass rate for wound care is 80–85%. Generic RCM frequently falls below 80%. Wound-specific practices with proper code validation and pre-submission scrubbing regularly exceed 95%. Every percentage point here represents claims that don’t require rework, appeals, or delayed payment. A 15% improvement in first-pass rate is worth 15–20 additional days in cash flow annually.
Denial Rate by Service Type
This is the KPI that most practices track too broadly. Overall denial rates mask the problem. Here’s the breakdown that matters:
| Service Type | CPT Codes | Average Denial Rate | Primary Cause | Target with Specialized RCM |
|---|---|---|---|---|
| Surgical Debridement | 11042–11047 | 20–25% | Depth documentation gaps, 12/360 exceedance | <8% |
| Selective Debridement | 97597–97598 | 18–22% | NCCI bundles with 11042, missing add-ons | <7% |
| Skin Substitutes | 15271–15278 + Q41xx | 25–35% | PA failure, sq cm errors, no conservative care docs | <10% |
| NPWT | 97605–97608 | 20–30% | Size threshold not met, missing disposable serial number | <9% |
| Compression | 29580–29581 | 15–20% | Bundled with debridement (NCCI Chapter 4G) | <6% |
Net Collection Rate
Best-in-class wound care practices using specialized RCM achieve net collection rates of 96–98%. Generic billing services typically land at 78–82%. For a $3 million practice, that 18-percentage-point gap represents $540,000 in annual revenue. The math on specialized wound care RCM is compelling: fees of 5–6% on improved collections easily generate a 2–3x return on investment.
The 2026 CMS Skin Substitute Changes: What Actually Changed and What It Means for Your Practice

The 2026 CMS reimbursement overhaul for skin substitutes was the most significant change to wound care billing in years, and a lot of practices were either unprepared or received incomplete guidance about what it actually required.
Here’s what changed: CMS eliminated product-specific pass-through payments and replaced them with a flat-rate model using Q41xx HCPCS codes, reimbursed at $127.14 per square centimeter regardless of the specific biologic product used. The products were reclassified as “incident-to” supplies rather than separately reimbursable items. The applications are billed using CPT 15271–15278 alongside the Q41xx supply codes, with reimbursement based entirely on documented surface area.
What this means practically:
First, accurate square centimeter measurement is no longer optional — it’s the entire basis of reimbursement. A practice that was billing based on product cost under the old ASP+6% model and didn’t recalibrate its documentation to precise wound measurement is likely receiving significantly lower reimbursement than it should be. EHR templates that auto-calculate square centimeters from documented wound dimensions become financially critical under this model.
Second, legacy HCPCS codes that weren’t mapped to the Q41xx structure trigger PR-96 denials. Practices that didn’t test their claims before January 2026 faced immediate denials and PR-96 rejections with losses of $500–$1,000 per application. If you’re still seeing unexplained skin substitute denials in 2026, this is the first place to investigate.
Third, LCD compliance under Noridian A58565 Rev 11 (which added 50 new ICD-10 codes effective January 2026) is mandatory for claims to pass medical necessity review. This isn’t the same LCD list from 2025 — it expanded significantly. Billing teams that didn’t update their scrubbing rules for the new revision are generating denials on legitimate claims.
For a detailed breakdown of exactly how to navigate Medicare wound care reimbursement in this environment, our Medicare wound care billing guide covers the specifics.
Wound Care Claims Processing: A 10-Step Workflow That Actually Works
Theory is fine. Here’s what an optimized wound care claims processing workflow looks like in practice:
Step 1 — Verify patient registration and insurance eligibility before every appointment. Confirm Medicare Part B vs. Part A status, check secondary payer coordination, and flag any SNF consolidated billing overlap. Use automated eligibility verification that runs 24–48 hours before the appointment, not the morning of service.
Step 2 — Confirm prior authorization status for any planned skin substitute application, NPWT, or HBOT. Verify the authorization is active on the date of service, check remaining approved units, and flag any approaching authorization limits. Set a system alert at 8 sessions to initiate ABN workflow before the 12/360 limit applies.
Step 3 — Review clinical documentation against billing requirements before coding begins. Wound measurements should be documented in centimeters, not vague descriptors. Tissue type removed should be named (subcutaneous fat vs. muscle fascia vs. bone cortex). Serial photos should be present for skin substitute applications. Conservative care failure documentation should span at least 30 days.
Step 4 — Assign CPT, ICD-10, HCPCS codes and modifiers. Select depth-based CPT with add-ons for surface area exceeding 20 square centimeters. Sequence ICD-10 codes with etiology first (E11.621 before L97.5xx for diabetic ulcers). Apply KX modifier when exceeding 12/360 with documented medical necessity. Apply modifier 25 for same-day E/M services with separate clinical documentation.
Step 5 — Run wound-specific NCCI edit scrubbing that goes beyond standard clearinghouse logic. Check bundled pairs (97597+11042, 11042+29580). Validate modifier 59/XS for distinct anatomical sites. Verify units of service match documented square centimeters. Cross-check against your MAC’s current LCD ICD-10 list.
Step 6 — Submit via clearinghouse (837P for professional claims, 837I for facility). Include correct POS code (11 office, 22 HOPD, 24 ASC). Confirm taxonomy codes match provider specialization. Receive clearinghouse acknowledgment on Day 1.
Step 7 — Track claim status at Day 14 via 276/277 EDI status check. A claim still showing “pending” at Day 14 often signals an impending CO-97 — begin documentation preparation now rather than waiting for the formal denial. Escalate claims still pending at Day 30.
Step 8 — Post payments and identify underpayments. Reconcile ERA payments line by line against expected reimbursement. Flag any Q41xx payment that doesn’t match documented square centimeters × $127.14. The 5–10% underpayment rate from square centimeter miscalculations is largely silent — it doesn’t generate a denial code, it just posts low.
Step 9 — Work denials within 14 days. CO-97 appeals should include wound photos from at least 3 visits, serial measurements showing the wound trajectory, excised tissue description with depth confirmation, and direct citation of the applicable LCD criteria. The Level 1 Redetermination 60–70% success rate only applies when the documentation bundle is complete.
Step 10 — Audit monthly and update quarterly. Review a 5% random sample of charts monthly against billing. Update scrubbing rules every quarter when NCCI edits are released (January, April, July, October). Review MAC LCD updates for your jurisdiction whenever a new revision is published.
For a deeper look at the claims workflow from a coding perspective, see our resource on wound care billing codes and the specifics around wound care billing guidelines.
Where Your Revenue Is Actually Going: The 7 Biggest Leakage Points in Wound Care Billing
Most practices that are losing significant revenue to billing problems don’t know exactly where the money is going. These are the seven areas where wound care practices hemorrhage revenue — in order of impact:
1. Missing Add-On Codes
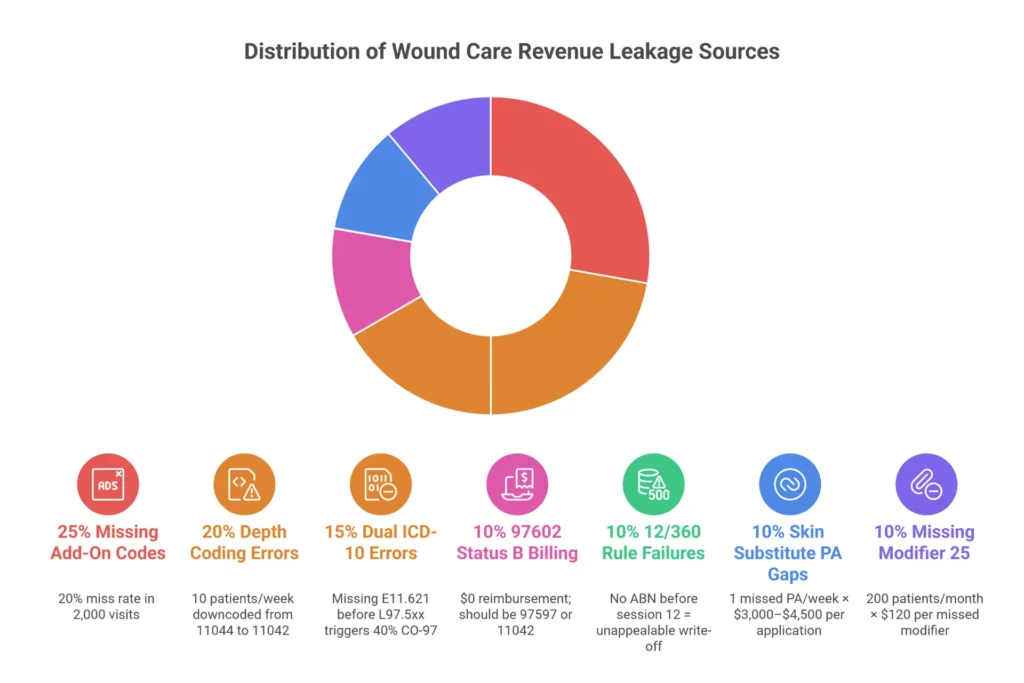
This is the single largest per-visit leakage point. If you’re billing 11042 for a 45 square centimeter debridement and not billing +11045 for the additional surface area, you’re billing for one 20 sq cm zone and ignoring the rest. The loss is $100–$150 for each missed +11045 unit, $80 for each missed +97598 unit. At a 20% miss rate across 2,000 annual visits, a $600,000 practice loses $36,000–$96,000 per year on this single issue alone.
2. Depth Coding Errors
Downcoding out of caution is nearly as expensive as getting denied for upcoding. Billing 97597 (selective debridement, ~$90) instead of 11042 (subcutaneous debridement, ~$120) because the documentation was ambiguous loses $30 per visit. Billing 11042 instead of 11044 (bone debridement, ~$250) on a wound where bone was exposed loses $130 per claim. A practice doing 10 patients per week with under-documented bone debridement loses over $100,000 annually. The fix isn’t to upcode — it’s to document tissue type and depth clearly in the operative note so the correct code is defensible.
3. Dual ICD-10 Errors for Diabetic Ulcers
Forty percent of diabetic wound care claims are denied when the etiology-manifestation pair is missing or sequenced incorrectly. Every diabetic foot ulcer claim requires E11.621 (Type 2 diabetes with foot ulcer) listed first, with the specific ulcer code (L97.5xx series) listed second. Missing either code, or reversing the order, generates an automatic CO-97 denial. For a practice with 500 diabetic wound visits annually at $100–$200 per denied claim, the annual exposure is $25,000–$100,000 from this one documentation failure.
4. The 97602 Status B Billing Error
CPT 97602 (non-selective debridement) carries a Status B designation on the Medicare Physician Fee Schedule — meaning it bundles into the E/M visit and generates $0 in additional reimbursement in an office setting. Approximately 30–40% of practices that aren’t specifically wound-focused bill 97602 when they should be billing 97597 or 11042. Every visit where this error occurs means the provider delivered a service and received nothing for it beyond the base office visit reimbursement. For a practice doing 50 of these visits monthly at $80–$120 per missed code, the annual loss approaches $60,000–$72,000.
5. 12/360 Rule Tracking Failures
The 12-session rolling limit on debridement procedures is tracked per wound across all visits — which means it’s tracked across time in a way that’s very easy to lose count of without a dedicated system. Practices that exceed the limit without the proper ABN in place, signed by the patient before the service that pushes them over the limit, face denials they cannot appeal and supply costs they cannot recover. Two skin substitute applications per month over the limit at $3,000 each means $72,000 in unrecoverable supply costs annually.
6. Skin Substitute Prior Authorization Gaps
A single missed prior authorization on a $3,000–$4,500 skin substitute application is a hard loss. Sixty to seventy percent of advanced therapy claims are denied when prior authorization is missing. For a practice doing one graft per week without consistent authorization management, the annual exposure is over $54,000 in unrecoverable write-offs. The required documentation — 4-week conservative care log with dated wound photos, Wagner grade ≥2, wound size measurements, and vascular study results — must be in place before the claim is submitted, not assembled after the denial arrives.
7. Missing Modifier 25 for Same-Day E/M Services
When a physician performs a significant evaluation and management service (99214, for example) on the same day as a debridement, modifier 25 is required on the E/M code to prevent automatic bundling with the procedure. Without it, 20% of same-day E/M claims are denied. For a practice seeing 200 patients monthly with same-day E/M, that’s $4,800 in monthly losses — $57,600 annually — from a single missing modifier that requires only separate documentation paragraphs to support.
To get a full picture of where your practice’s revenue might be leaking, see our detailed analysis of wound care billing guidelines or explore the complete revenue cycle management process.
Denial Prevention That Actually Works: A Three-Tier Strategy
Up to 90% of wound care claim denials are preventable. The practices that achieve denial rates below 10% aren’t just lucky — they’ve built a systematic prevention framework that addresses denials before, during, and after submission. Here’s how that framework works:
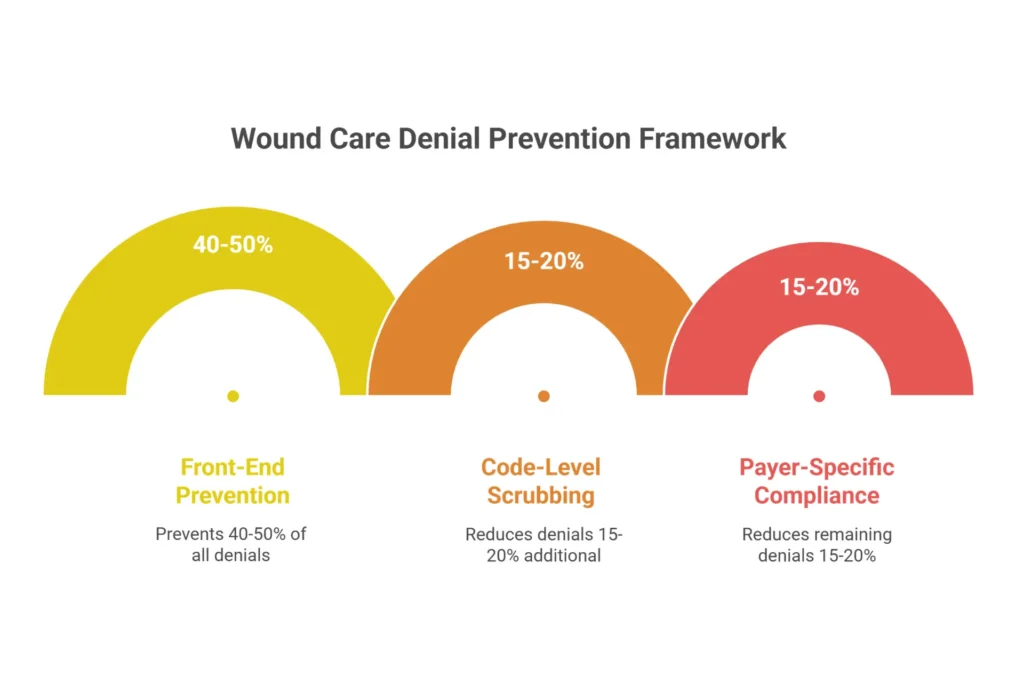
Tier 1: Front-End Prevention
Front-end prevention stops denials before care is delivered. This means running automated eligibility verification that flags Medicare Part A SNF overlaps, confirming prior authorization for skin substitutes and NPWT 48–72 hours before the appointment, and having hard-stop documentation standards in the EHR that prevent a wound assessment from being saved without wound measurements, tissue type documentation, and progress notes from prior visits.
ABN workflow automation is critical here. When a patient is approaching their 12/360 session limit, the system should alert billing staff at 8 sessions (not 12), generate the ABN for patient signature, and apply the GA modifier to the claim if the patient signs. Without this process, you’re gambling on whether the patient is covered — and when you lose, it’s a write-off, not a denial you can appeal.
Tier 2: Code-Level Technical Scrubbing
This is where wound-specific claim scrubbers earn their value. Beyond standard NCCI edit checking, effective wound care scrubbing validates: depth-based CPT selection against tissue type documented in the note; etiology-manifestation ICD-10 sequencing for diabetic diagnoses; NCCI bundled pairs specific to wound care (11042+97597, 11042+29580, NPWT+debridement); Q41xx square centimeter units against documented wound measurements; and MAC LCD ICD-10 compliance against the current LCD for your jurisdiction.
Practices implementing specialized pre-submission NCCI scrubbing routinely see 15–20% reduction in denial rates at the code-validation stage alone. This is the difference between catching a bundling error before submission and spending 45+ days working the denial after the fact.
Tier 3: Payer-Specific Compliance
Jurisdiction-aware billing means your billing rules engine knows that you’re billing under Noridian A58565 versus Palmetto A55818 versus CGS A55909, and applies the correct coverage criteria for each. This matters because the same procedure with the same ICD-10 code can be covered under one MAC and denied under another. A wound care clinic that crosses MAC jurisdictions — seeing patients from different parts of the state — needs to validate diagnosis codes against the specific LCD for each patient’s coverage, not just one generic list.
Commercial payer requirements are equally varied: Aetna requires 30-day progressive documentation of non-healing; UnitedHealthcare has DFU size requirements; Humana mandates dual ICD coding. None of these are defaults in a general billing system — they require payer-specific rule tables built and maintained by billing staff who know wound care.
When you’re ready to stop patching denials reactively and build a prevention-first revenue cycle, our RCM services include the full three-tier framework built specifically for wound care.
Technology in Wound Care RCM: What to Look For (and What to Avoid)
The right technology doesn’t just process claims faster — it prevents the errors that generate denials in the first place. Here’s what wound care practices should actually be looking for in their RCM technology stack:
Wound-specific EHR functionality. Net Health’s WoundExpert platform, OmniMD, and Swift Skin & Wound are built for wound care workflows — they include depth-based CPT assignment templates, Q41xx square centimeter calculation, KX modifier auto-insertion for 12/360 compliance, and LCD compliance alerts tied to specific MAC rules. A general EHR like Athenahealth or DrChrono can handle wound care billing, but requires middleware or manual processes to achieve the same compliance checks — and that’s where errors occur.
AI-driven claim scrubbing. Platforms like Aptarro, the Net Health AI Scrubber, and BillFlash’s denial AI do more than flag NCCI codes — they analyze clinical note content for depth documentation, detect missing etiology-manifestation pairs, and validate Q41xx units against wound measurements. Practices using AI scrubbing report 12–18% higher first-pass rates and 25% fewer denials compared to traditional NCCI-only systems. That’s not marginal — it’s transformational for a high-volume wound clinic.
Prior authorization automation. Platforms like Availity PA Manager and Net Health’s PA Genie auto-populate skin substitute authorization forms with EHR-extracted data — wound photos, conservative care logs, Wagner grade, and measurements — reducing manual processing time from 4 hours to about 30 minutes per request and improving approval rates by approximately 20%.
Clearinghouse with wound-specific edit engines. Waystar’s Claim Manager, for example, offers custom edit engines that can be configured with MAC-specific LCD rules. Standard clearinghouse scrubbing catches format errors; wound-specific scrubbing catches medical necessity compliance problems before the payer even sees the claim.
If you’re evaluating technology, the questions to ask vendors are specific: Can they demonstrate their 12/360 tracking? Do they know what changed in A58565 Rev 11? Can they show you how their system handles Q41xx square centimeter validation? If the vendor can’t answer those questions, they’re a general RCM platform, not a wound care solution.
Wound Care RCM Revenue Leakage Calculator
Enter your practice numbers below to see how much revenue you may be losing each year to common wound care billing errors — and what you could realistically recover.
When to Consider Outsourcing Your Wound Care Revenue Cycle
Outsourcing wound care RCM isn’t the right move for every practice at every stage. But there are five signals that typically indicate the in-house model has hit its ceiling:

Your Days in AR consistently exceeds 50 days. Your denial rate is above 20%. Your net collection rate has dropped below 92%. You’ve had billing staff turnover in the last 12 months and things never quite recovered. You know you’re missing add-on codes but don’t have the system to catch them.
If three or more of those apply, the math on outsourcing to a specialized wound care team becomes very compelling. For a $600,000 practice currently running at a 15% denial rate with 60% recovery, the annual loss to unrecovered denials alone is approximately $54,000. A specialized RCM team running an 8% denial rate with 85% recovery reduces that loss to $12,000 — a $42,000 improvement. At a 6% service fee ($36,000), the net first-year gain is $6,000 plus 20–30 days of faster cash flow. Year two and beyond, the numbers improve significantly.
The key is choosing a team that was built for wound care specifically — not a generalist billing company that “handles wound care too.” The difference is whether they can demonstrate their 12/360 tracking system, explain what changed in Noridian A58565 Rev 11, and show you how they handle Q41xx flat-rate reimbursement under the 2026 model. If they can’t answer those questions in a sales call, they don’t have the depth to protect your revenue.
Our guide to outsourcing wound care billing walks through the evaluation process in detail. And if you want to skip the research and talk directly about your practice’s situation, our wound care billing team offers a free 90-day revenue leakage assessment with no obligation.
What Proper Credentialing Has to Do With Wound Care Revenue
One overlooked piece of the revenue puzzle: credentialing delays. When a wound care provider isn’t enrolled with the right payers — or when their credentials lapse — claims submit and get denied at the payer level before medical necessity is even reviewed. For practices adding new providers or expanding to new payer networks, proper Medicare credentialing services ensure there are no gaps in your ability to bill. It’s a foundational issue that billing optimization can’t fix if the enrollment isn’t right.
People Also Ask: Wound Care RCM Questions Worth Knowing
These are the questions wound care billing professionals and practice managers are actually asking — with the straight answers:
Does Medicare require prior authorization for wound care debridement?
Traditional Medicare does not require prior authorization for debridement procedures — but you must comply with the LCD for your MAC jurisdiction (Noridian A58565, Palmetto A55818, CGS A55909, depending on your region). Medicare Advantage plans are a different story: the majority require prior authorization for skin substitutes, NPWT, and HBOT. Always verify the specific plan’s requirements.
How do I know which MAC LCD applies to my wound care practice?
Your MAC is determined by the state where your practice is located and the type of claim you’re submitting (Part A or Part B). CMS maintains a MAC jurisdiction map at cms.gov. For wound care, the most common MACs are Noridian (Jurisdiction A), Palmetto GBA (multiple jurisdictions), CGS (Jurisdiction 15), and WPS. Each publishes their LCD with specific ICD-10 requirements, documentation standards, and coverage criteria. Your billing team needs to track the specific LCD for your jurisdiction — not just generic wound care guidelines.
What is the difference between CPT 97597 and CPT 11042?
CPT 97597 is selective debridement — the removal of only non-viable tissue (fibrin, slough, biofilm) using sharp instruments, autolytic, or enzymatic methods, without extending into the subcutaneous tissue. It’s appropriate for superficial wound bed preparation. CPT 11042 is surgical debridement of subcutaneous tissue — it involves removing non-viable subcutaneous fat and requires documentation of tissue type removed. The depth distinguishes them. Billing 97597 when the clinical note documents subcutaneous tissue removal leaves money on the table; billing 11042 without depth documentation creates audit exposure.
Can wound care and E/M codes be billed together on the same date?
Yes — but only when the evaluation and management service is significant and separately identifiable from the procedure, documented with its own clinical decision-making rationale in a separate section of the note. The E/M code requires modifier 25 to indicate this. The OIG has flagged modifier 25 usage as a high-audit area for wound care practices, so the documentation needs to clearly demonstrate that the E/M was not simply the pre-service assessment for the procedure.
How do workers compensation wound care claims differ from Medicare?
Workers compensation wound care claims require state-specific forms (California uses the DWC-UB-04, for example), an injury causation narrative linking the wound to the workplace incident, and an approved treatment plan before NPWT or skin substitute applications. There’s no prior authorization requirement in the Medicare sense, but a treatment plan must be approved by the WC adjuster. Days in AR for WC wound claims typically runs 60–90 days versus 14–30 days for Medicare — significantly longer, requiring active follow-up to prevent write-offs.
Voice Search: Quick Answers to Wound Care Billing Questions
These answers are written to match how people ask questions naturally — and to be accurate enough to cite:
What is wound care revenue cycle management?
Wound care revenue cycle management is the specialized billing and collections process for wound treatment services. It handles everything from checking insurance eligibility before the visit to coding debridement procedures and skin grafts using precise CPT codes, submitting claims, managing denials, and collecting payment. It’s more complex than general medical billing because codes depend on wound depth, payer rules vary by region, and documentation requirements are extensive.
Why do wound care claims get denied so often?
Wound care claims are denied frequently because they require very specific documentation — the exact depth of tissue removed, wound measurements in centimeters, and the correct pairing of diagnosis codes for diabetic wounds. Missing any of these, using the wrong CPT code for the depth of debridement, or failing to get prior authorization for skin grafts can trigger automatic denials. Wound care has a denial rate of 25 to 35 percent, compared to about 12 percent for general medicine.
What changed with skin substitute billing in 2026?
In 2026, Medicare switched from paying for each skin substitute product individually to a flat-rate system that pays $127.14 per square centimeter regardless of the product used. Practices now bill using Q41xx codes combined with CPT 15271 through 15278. The key change is that accurate wound measurement is now the basis of all reimbursement, and practices that don’t document precise surface area in square centimeters receive significantly less than they should.
How many wound care sessions does Medicare allow per year?
Medicare limits debridement procedures to 12 sessions within any 360-day rolling period. This is called the 12/360 rule. If a patient needs more than 12 sessions, the provider must document medical necessity, have the patient sign an Advance Beneficiary Notice before the 12th session is exceeded, and apply the KX modifier on the claim. Without these steps, the additional sessions are automatically denied and cannot be appealed.
How do you appeal a denied wound care claim?
To appeal a denied Medicare wound care claim, you file a Level 1 Redetermination with your MAC within 120 days of the denial. Include a complete documentation bundle: wound photos from at least three visits, serial measurements showing wound progression, procedure notes describing the tissue removed, vascular study results if applicable, and a citation of the specific Medicare LCD criteria that supports coverage. This approach succeeds about 60 to 70 percent of the time when documentation is complete.
Is outsourcing wound care billing worth it?
For most wound care practices, yes — especially those with denial rates above 20% or Days in AR above 50 days. Specialized wound care billing companies typically reduce denials by 15 to 20 percent, improve cash collections by 15 to 25 percent, and shorten payment timelines significantly. Most mid-sized practices see two to three times return on the billing service fees through improved revenue capture.
Frequently Asked Questions: Wound Care RCM
What is wound care RCM?
Wound care revenue cycle management (RCM) is the specialized end-to-end financial process for wound treatment services — from patient registration and insurance verification through CPT coding, claim submission, denial management, and final payment posting. It differs from general RCM due to depth-based CPT code selection (CPT 11042–11047), dual ICD-10 requirements for diabetic wounds (E11.621 + L97.5xx), MAC-specific Local Coverage Determinations, NCCI bundling edits, and frequency limits like the 12/360 rule. Wound care practices experience denial rates of 25–35% compared to 10–15% for general medicine, and revenue leakage often exceeds $200,000 annually for mid-sized clinics.
What are the 7 stages of wound care revenue cycle management?
The seven stages are: (1) Patient Registration and Eligibility Verification — confirming Medicare Part A vs. Part B coverage and skin substitute coverage; (2) Charge Capture — documenting wound depth, measurements, and photos for billing; (3) Coding — assigning depth-based CPT codes (11042–11047, 97597–97598), add-on codes (+11045, +97598), and dual ICD-10 pairs; (4) Prior Authorization — securing approval for skin substitutes and NPWT with conservative care documentation; (5) Claim Submission — submitting scrubbed 837P/837I claims through the clearinghouse; (6) Payment Posting and Denial Management — reconciling ERA payments and working CO-97 denials within 14 days; and (7) Reporting — tracking KPIs including Days in AR, denial rates by CPT, and net collection ratio.
What is the biggest cause of wound care claim denials?
CO-97 medical necessity denials cause 35–40% of all wound care claim rejections. The primary triggers are: missing or insufficient depth documentation for deep debridement codes (11043, 11044), incorrect dual ICD-10 sequencing for diabetic foot ulcers (failing to list E11.621 before L97.5xx), missing 30-day progressive wound documentation required for skin substitute approvals, and NCCI bundling conflicts that automatically deny paired codes. Prevention requires EMR documentation templates with hard stops, etiology-first ICD sequencing validation, serial wound photos, and pre-submission NCCI scrubbing.
How long does wound care claims processing take?
Wound care claims processing timelines vary by payer: Medicare averages 14–30 days (check 276/277 claim status at Day 14); Medicare Advantage averages 30–45 days due to prior authorization review; commercial payers (Aetna, UnitedHealthcare) average 21–40 days; Medicaid varies by state at 45–60 days. Skin substitute prior authorization holds add 20–30 days to the cycle. Wound care industry average Days in AR is 45–62 days. Best-in-class specialized RCM teams achieve 22–26 days through pre-submission scrubbing and proactive authorization management.
What is a good denial rate for wound care billing?
The industry average denial rate for wound care is 25–35%, significantly higher than the 10–15% average for general medical billing. A well-managed wound care practice should target under 12%. Practices using CWCC-certified coders (Certified Wound Care Coder through AAPC) with wound-specific billing workflows typically achieve denial rates of 8–12%, compared to 25–30%+ for practices using general medical billing services. Skin substitute codes (15271–15278) carry the highest denial rate at 25–35%; debridement codes average 20–25%; NPWT codes average 20–30%.
What CPT codes are most commonly denied in wound care?
The most frequently denied wound care CPT codes are: debridement codes 11042–11047 (20–25% denial rate, primarily from NCCI bundling with 97597 and missing depth documentation), skin substitute application codes 15271–15278 (25–35%, from missing prior authorization, square centimeter errors, and inadequate conservative care documentation), and NPWT codes 97605–97608 (20–30%, from absent size threshold documentation). E/M codes 99202–99215 on the same day as procedures are denied at about 20% when modifier 25 is missing.
Can wound care revenue cycle management be outsourced?
Yes — and for many wound care practices, outsourcing to a specialized team delivers significantly better results than general billing. Specialized outsourcing covers end-to-end functions including coding audits, prior authorization automation, denial appeals, 12/360 frequency tracking, and Q41xx flat-rate reimbursement management. Look specifically for CWCC-certified coders (AAPC certification) and MAC LCD expertise. Most mid-sized practices achieve 2–3x ROI through denial reduction and improved collections. Fees typically range 4–8% of collected revenue. A 90-day pilot with performance benchmarks is standard with reputable vendors.
How does the 2026 CMS skin substitute change affect wound care billing?
Beginning January 2026, CMS replaced product-specific pass-through payments for skin substitutes with a flat-rate model at $127.14 per square centimeter using Q41xx HCPCS codes, paired with CPT 15271–15278 application codes. Products were reclassified as “incident-to” supplies, eliminating the previous ASP+6% cost-plus model. Practices must now document precise wound surface area in square centimeters — the entire basis of reimbursement. Practices that didn’t map legacy HCPCS codes to Q41xx before January 2026 received PR-96 denials with $500–$1,000 losses per application. LCD compliance under Noridian A58565 Rev 11 (which added 50 new ICD-10 codes) is required for all Medicare claims.
The Bottom Line: Wound Care Is Too Complex for General Billing
There’s a phrase I hear from wound care physicians fairly regularly after they switch to a specialized billing team: “I didn’t realize how much I was leaving behind.” It’s not that their previous billing was bad — it was just built for a different kind of practice. Wound care has genuine complexity that general billing workflows aren’t designed to handle: depth-based coding, MAC variability, the 12/360 rule, dual ICD requirements, skin substitute prior authorization, and the 2026 flat-rate transition that changed how the biggest-dollar procedures in wound care are reimbursed.
The revenue impact of getting this right is not marginal. For a $600,000 practice, the difference between a general billing service and a wound-care-specific team is often $40,000–$90,000 in annual revenue — before you account for improved Days in AR, better supply margin management, and reduced audit exposure. That’s not an estimate pulled from thin air; it’s what the KPI benchmarks show consistently when wound care practices switch to specialized RCM.
Whether you’re evaluating your current billing arrangement, dealing with a spike in denials after the 2026 changes, or building out a new wound care program, the fundamentals are the same: the revenue cycle needs to be built around the actual complexity of what you do.
If you want to find out exactly how much revenue your practice might be leaving on the table, start with our free 90-day claims assessment. We’ll review your actual claims data, identify your top leakage points, and give you a specific dollar figure for recoverable revenue — with no obligation to work with us afterward.
Ready to Stop Losing Revenue on Claims You’ve Already Worked For?
Our wound care billing specialists use MAC-specific LCD validators, AI-driven denial prevention, and depth-based CPT automation to maximize every claim — from debridement to skin substitutes under the 2026 flat-rate model.
Free 90-day claims review • No obligation • CWCC-certified wound care coders • Results tracked on shared KPI dashboard
Related Resources from Elite Med Financials
- Complete Guide to Wound Care Billing Codes
- Medicare Wound Care Billing Guide (2026 Updated)
- Should You Outsource Your Wound Care Billing?
- Wound Care Billing Guidelines and Compliance
- Wound Care Billing and Coding Services
- How to Improve Revenue Cycle Management
- Revenue Cycle Management: Complete Overview
- Healthcare Revenue Cycle Best Practices

