
Drug diversion monitoring software is a specialized system that tracks, detects, and helps prevent the unauthorized transfer, theft, or misuse of controlled medications across an Opioid Treatment Program (OTP). For methadone clinics and MOUD providers, it builds accountability across the entire medication lifecycle: inventory receipt, observed dosing at the window, take-home bottle issuance, bottle returns, and random callbacks. Modern platforms connect EMR records, dispensing pump data, toxicology, and PDMP/MAPS context, then apply automated workflows and risk analytics to surface potential diversion early.
OTPs need software built for their model, not borrowed from hospitals. Hospital diversion tools watch staff activity inside automated dispensing cabinets. OTPs must also manage patient-facing accountability: proxy-dosing prevention, serialized take-home bottle tracking, pump reconciliation, Diversion Control Plan (DCP) documentation, and audit-ready records that hold up during DEA inspections and accreditation surveys.
See OTP diversion control in a live workflow
Biometric dosing window, automated callbacks, serialized bottle tracking, and real-time risk scoring — using your own clinic scenarios.
Book Diversion Control DemoKey Takeaways
- Drug diversion monitoring software helps clinics detect, document, and investigate controlled-substance diversion risk — it flags signals for review rather than proving wrongdoing on its own.
- OTPs need specialized workflows because methadone clinics manage observed dosing, liquid methadone, take-home bottles, callbacks, and DCP documentation.
- Hospital diversion tools are strong for automated dispensing cabinets and staff behavior, but they usually miss patient-facing OTP accountability.
- The best OTP systems connect bottle tracking, callbacks, pump sync, toxicology, patient identity, and audit-ready reporting in one record.
- MASE is built for OTP medication accountability, including diversion-control workflows, pump integration, and optional OTP billing/RCM support.

Who Should Read This Guide?
This guide is for OTP owners, program sponsors, medical directors, nursing directors, compliance officers, and operations leaders trying to replace manual diversion tracking, disconnected pump logs, spreadsheet callbacks, paper bottle returns, or hospital-style diversion tools that do not fit methadone clinic workflows. For operators comparing methadone clinic diversion control software, the key question is whether the platform can document what happens after medication leaves the dosing window.
Table of Contents
What Is Drug Diversion Monitoring Software?
Drug diversion monitoring software is a controlled-substance monitoring tool that watches the movement of regulated medications and flags unusual patterns for human review. Diversion means any point where a controlled drug leaves its legitimate path, whether that is staff theft, falsified records, proxy dosing, or a take-home bottle that is shared or sold. The software does not prove wrongdoing on its own. It surfaces risk signals so trained staff can investigate, confirm, or clear them.
Across most platforms, diversion monitoring software pulls from dispensing records, inventory logs, medication administration records (MAR), waste and return documentation, audit logs, toxicology results, and, where relevant, PDMP data. It then reconciles those streams to find discrepancies, such as a dispense with no matching administration, an unreturned bottle, or a dosing pattern that does not match a patient’s history.
How Drug Diversion Monitoring Software Works
At a basic level, the software ingests data from connected systems, normalizes it, reconciles each transaction against expected activity, and assigns risk based on the anomalies it finds. In a hospital, that usually means matching automated dispensing cabinet (ADC) pulls against the EHR and waste records. In an OTP, the same logic must extend to the dosing window and into the community, where take-home medication creates a chain-of-custody problem hospitals rarely face.
It is worth repeating: this is diversion surveillance and diversion detection, not automated judgment. A risk flag is a starting point for review, supported by an audit trail, not a verdict.
Hospital Drug Diversion Monitoring vs. OTP Diversion Monitoring
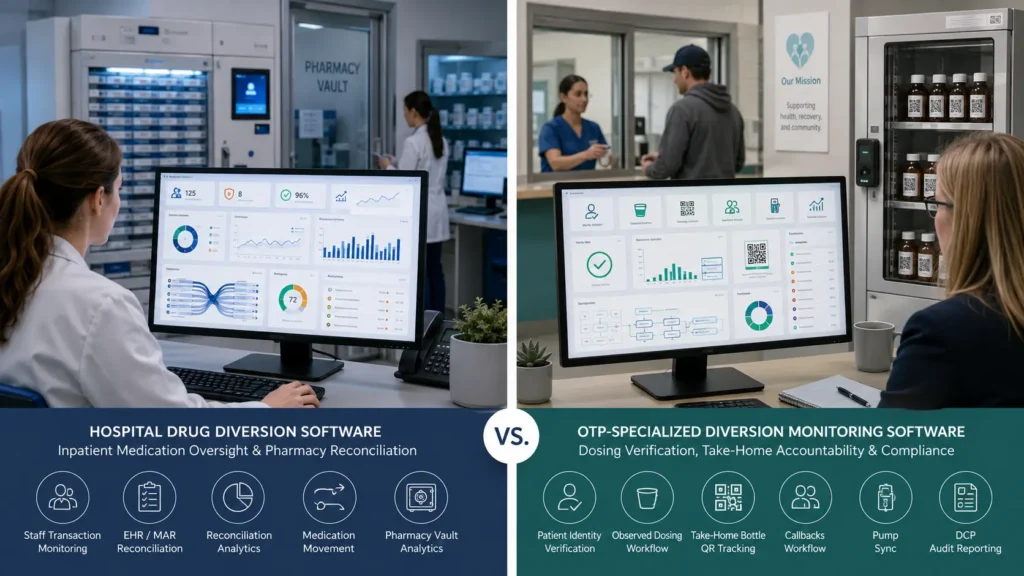
Hospital diversion monitoring is built around closed, acute-care environments. Controlled substances live in vaults and ADCs, are pulled by licensed staff, administered to admitted patients, and wasted under witness. The monitoring question is essentially: did a staff member take more than the patient received?
OTP diversion monitoring has to answer a different question: did the right patient receive the right dose, and can the clinic account for every take-home bottle after it leaves the building? That shifts the focus from staff-only transaction monitoring to patient-facing accountability — observed dosing, identity verification, bottle returns, callbacks, and pump reconciliation for liquid methadone.
Why Methadone Clinics Need OTP-Specific Diversion Monitoring
Methadone dispensed on-site at an OTP is not the same as a controlled substance filled at a retail pharmacy. There is no pharmacy claim and often no PDMP entry for the daily observed dose, so PDMP/MAPS data cannot be the primary source of truth for OTP methadone. Accountability instead rests on dispensing logs, bottle tracking, callbacks, toxicology, visit patterns, take-home decisions, and DCP documentation. That is exactly the combination generic tools miss, and it is why purpose-built OTP clinic software exists — typically anchored to an OTP methadone EMR rather than a bolt-on monitoring tool.
Why OTPs and Methadone Clinics Face Higher Diversion Risk
OTPs do not face elevated diversion risk because they are careless. They face it because their care model is structurally more complex than almost any other outpatient setting. Daily observed dosing, liquid methadone, and patient-controlled take-home medication each add risk surfaces that a hospital ADC model never has to manage.
Take-Home Methadone Creates Chain-of-Custody Risk
Take-home dosing is a core part of modern, recovery-oriented OTP care, and expanded take-home flexibility has improved access and retention for many patients. It also moves more bottles into the community. Once medication leaves the clinic, it can be shared, sold, lost, or tampered with. Empty-bottle return rates, late returns, and damaged bottles become meaningful signals, yet many programs still track them on paper. Scalable monitoring is now a practical necessity, not a luxury.
Daily Observed Dosing Still Requires Strong Controls
High-volume daily dosing creates speed pressure at the window, and speed pressure creates openings. Proxy dosing — a patient sending someone else to receive a dose — and simple wrong-patient dosing are the two patient-facing risks observed therapy is meant to prevent. Basic photo-ID checks are easy to rush in a busy lobby, which is why identity verification at the dosing window matters so much in an OTP.
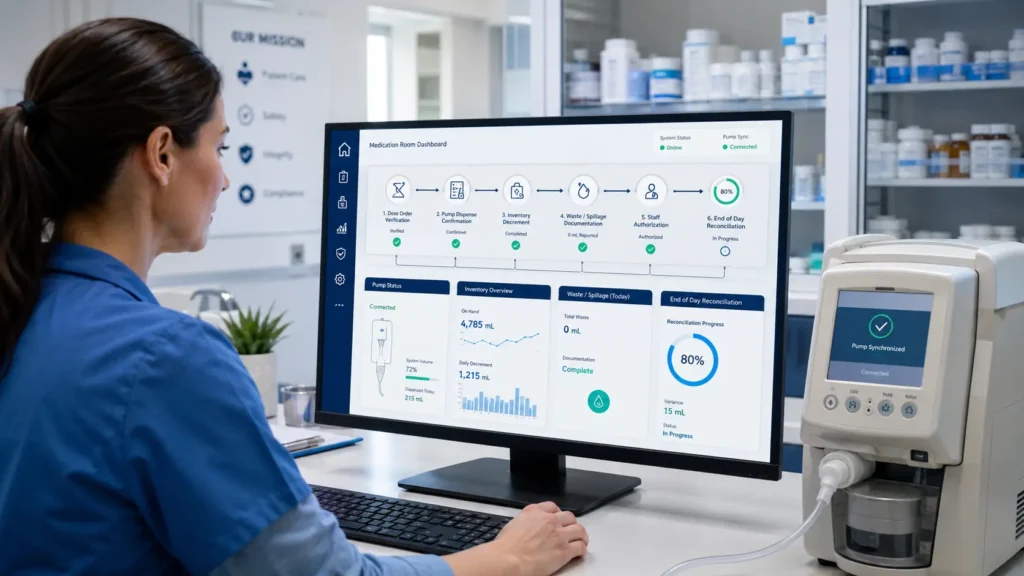
Manual Documentation Makes Diversion Control Harder to Prove
Liquid methadone has to be reconciled precisely. Pump calibration, overage and shortage, spillage, and inventory counts all have to line up. When pump dispenses, poured doses, and recorded inventory live in separate systems, discrepancies are easy to miss and hard to explain later. The same fragmentation hits callbacks, bottle counts, and toxicology: when the signals never meet, diversion tends to surface during an audit rather than in real time.
Why Hospital Diversion Tools Miss OTP-Specific Risk
Most commercial diversion platforms were built for inpatient hospitals. They are strong at ADC transaction monitoring, waste discrepancies, and clinician peer benchmarking. They were never designed for observed therapy at a dosing window, serialized take-home bottle tracking, 42 CFR Part 8 callback workflows, or integration with methadone dispensing pumps. Running an OTP on a hospital tool leaves the highest-risk workflows under-monitored. Importantly, this is also where staff diversion and patient diversion diverge: hospital tools focus almost entirely on staff, while OTPs must monitor both.
42 CFR Part 8, DEA, and Accreditation Requirements for Diversion Control
Diversion control in an OTP is a regulatory obligation enforced from several directions at once. Software can support and document these requirements, but it does not replace policies, trained staff, physical controls, or a program’s regulatory responsibility.
42 CFR Part 8 and the Diversion Control Plan Requirement
Under 42 CFR §8.12, every OTP must maintain a current Diversion Control Plan as part of its quality assurance program. The DCP must include specific measures to reduce the possibility that dispensed MOUD is diverted, and it must assign clear responsibility to identified staff. The same section ties take-home decisions to diversion-risk factors such as the absence of known recent diversion activity, the ability to safely store and transport medication, and documented clinical rationale. Good software helps operationalize DCP workflows and helps document take-home decisions, but the SAMHSA Diversion Control Plan itself remains the program’s responsibility.
DEA Recordkeeping and Schedule II Inventory Controls
Methadone is a Schedule II controlled substance, so DEA recordkeeping rules apply in full. OTPs should maintain accurate, readily retrievable controlled-substance records that support inventory, dispensing, receiving, waste, return, and investigation workflows, and theft or significant loss must be reported on time. The federal requirements for records and reports of registrants are set out in 21 CFR Part 1304. Software supports DEA inspection readiness by keeping a continuous, searchable audit trail and helping reconcile inventory, so records are not reconstructed under pressure during an inspection.
DEA Form 222, CSOS, and Methadone Ordering Documentation
Schedule II ordering is documented through DEA Form 222 or its electronic equivalent, the Controlled Substance Ordering System (CSOS), which allows secure electronic transmission of controlled-substance orders without the supporting paper Form 222. If supported by the clinic’s ordering process, software should help connect controlled-substance ordering, receiving, and internal inventory records so CSOS or DEA Form 222 documentation can be reconciled with dispensing activity. Software supports this documentation; it does not replace the registrant’s ordering obligations.
Take-Home Accountability and Documentation
Beyond ordering and inventory, surveyors want to see that take-home medication is accounted for after it leaves the clinic. Serialized bottle tracking, documented bottle returns, callback results, and tamper checks all become part of the evidence that the DCP is working in practice, not just on paper. Software helps maintain audit-ready records of each of these events.
Accreditation Survey Readiness and Audit Trails
CARF and The Joint Commission surveyors examine whether a program’s actual practices control diversion, not just whether a policy document exists. They look for contemporaneous, readily retrievable records. A platform that captures identity, dosing, bottles, callbacks, and inventory in one audit trail supports survey readiness by making that evidence easy to produce. To be clear about the limits: no software is DEA-approved or SAMHSA-approved, none guarantees compliance or guarantees passing an audit, and none eliminates DEA risk. The software is a tool that supports compliance documentation; the responsibility stays with the program.
Required Features in OTP Drug Diversion Monitoring Software
Several capabilities have moved from “advanced” to essential for OTP diversion control in 2026. For each one, it helps to ask the same four questions: what does it do, why do OTPs need it, what risk does it close, and what do generic or hospital tools usually miss?
1. Serialized QR/Barcode Bottle Tracking and Take-Home Chain-of-Custody
Assigns a unique serial (often a QR or barcode) to every take-home bottle at issuance and tracks it through return. It closes the single biggest OTP-specific gap — accountability after medication leaves the building. Hospital tools track inventory inside the vault, not serialized bottles in the community.
2. Automated Callback Workflows
Randomly selects patients for callbacks, sends SMS reminders, schedules visits, and logs bottle counts and toxicology results into the chart, escalating missed callbacks. It operationalizes a core DCP requirement that most clinics still run on spreadsheets and phone trees. Hospital platforms have no concept of patient callbacks.
3. Facial Biometric Verification at the Dosing Window
Confirms patient identity in real time before a dose is released, using a facial-matrix approach rather than a single image match. It directly addresses proxy dosing, which photo-ID checks and legacy fingerprint/iris systems can miss in a busy lobby. Hospital tools verify staff badges, not patients at a dosing window.
4. Geofencing / Context Verification
Adds location context to a dosing or take-home event, confirming that activity is happening where it should. Combined with identity, it strengthens the audit trail for each dose. Generic tools have no patient-location context.
5. Methadone Pump Integration and Inventory Reconciliation
Connects bidirectionally to dispensing pumps so each dispense is logged and reconciled against inventory automatically. It catches overage, shortage, and spillage discrepancies in liquid methadone in real time. Hospital ADC monitoring does not speak to OTP pumps.
6. Composite Patient Diversion Risk Scoring
Combines callback compliance, bottle returns, toxicology, dosing-pattern anomalies, and PDMP flags into one patient-level score with alerts. It moves a program from reactive investigation to proactive review. Hospital scoring is staff-level peer benchmarking, not patient-level.
7. Toxicology and PDMP/MAPS Context
Brings toxicology results and PDMP/MAPS context into the same view as dosing and bottle data. In an OTP, toxicology and visit patterns matter more than PDMP alone, since the daily observed dose usually never reaches a PDMP. Hospital tools lean heavily on PDMP and miss the OTP nuance.
8. DEA/DCP Audit-Ready Reporting
Generates exportable, timestamped reports that map to DCP measures and DEA recordkeeping. It turns daily activity into review-ready evidence. Generic reporting is built around hospital investigation workflows, not OTP DCP structure.
9. Role-Based Access, Logs, and Exportable Records
Enforces role-based permissions, keeps immutable access logs, and exports records on demand. It protects PHI and produces the readily-retrievable records surveyors expect. This is table stakes, but OTP-specific record types are often missing in adapted tools.
10. Integration with EMR, Billing/RCM, Inventory, and Compliance Workflows
Connects diversion monitoring to the clinical record, inventory, and revenue cycle so accountability and documentation are not siloed. Fragmentation across separate tools is the exact condition that lets diversion hide until an audit.
| Feature | What It Does | OTP Risk It Solves | Why Hospital Tools Miss It | MASE Fit |
| Serialized QR bottle tracking | Serializes & tracks take-home bottles to return | Take-home chain-of-custody gaps | They track vault inventory, not community bottles | Native serialized QR tracking + return verification |
| Automated callbacks | Randomizes, reminds, schedules, logs, escalates | Manual callback gaps under the DCP | No patient callback concept | Full end-to-end callback automation tied to the chart |
| Facial biometric verification | Verifies patient identity at the window | Proxy & wrong-patient dosing | They verify staff, not patients | Facial-matrix verification at the dosing window |
| Geofencing / context | Adds location context to dose events | Unverified dosing context | No patient-location awareness | Geofencing layered with biometrics |
| Pump integration | Syncs dispenses to inventory | Liquid methadone overage/shortage | No OTP pump connectivity | Native sync with MethaSpense, SciLog, IVEK |
| Composite risk scoring | Scores patient-level risk across signals | Late, pattern-based diversion | Staff-level scoring only | Multi-signal patient risk scoring |
| Toxicology & PDMP context | Unifies tox + PDMP with dosing | Missed correlation signals | Over-reliance on PDMP | Tox + PDMP/MAPS in one view |
| DEA/DCP reporting | Exports audit-ready evidence | Audit reconstruction under pressure | Hospital investigation format | DCP-aligned audit-ready reporting |
| Role-based access & logs | Permissions + immutable logs | PHI exposure, missing records | OTP record types absent | Role-based access with exportable logs |
| EMR / RCM integration | Connects clinical, inventory, billing | Data silos hiding diversion | Standalone hospital scope | Unified EMR + RCM workflows |
| Example: Pump log does not match inventory The EMR shows one dose, the pump log shows another dispense, and end-of-day inventory is short. A connected platform should help staff review the dose order, pump transaction, inventory decrement, waste/spillage documentation, and staff signature together — instead of chasing three separate logs the next morning. |
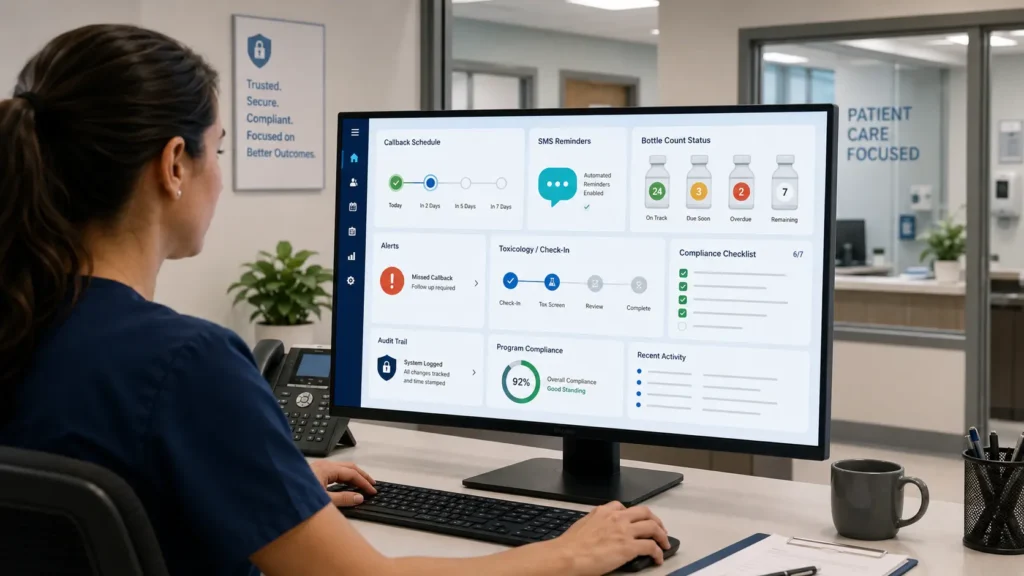
Automated Callbacks and Bottle Counts: Useful, But Not Enough Alone

Callbacks are a cornerstone of nearly every OTP Diversion Control Plan. A callback asks a patient to return to the clinic — often within a short window such as 24 hours where the program’s policy supports it — for a random medication count and toxicology check. Done well, callbacks confirm that take-home bottles are present, intact, and untampered, and they produce a documented record that the program is actively controlling diversion.
A complete callback workflow includes random selection, SMS reminders, scheduling, on-site bottle count documentation, urinalysis or toxicology and tamper checks, missed-callback escalation, and automatic chart logging. Automating this reduces staff burden and removes the documentation gaps that manual phone trees and spreadsheets create.
But callbacks alone are not enough. A callback is a single point-in-time check. Without connection to serialized bottle tracking, toxicology trends, composite risk scoring, and DCP documentation, a clean callback can hide a developing pattern. Kipu Health has one of the better-documented callback workflows in the market, with solid automation and chart logging. Even so, a callback module on its own leaves the rest of the accountability picture disconnected. Callbacks deliver their full value when they feed the same risk view as bottles, dosing history, and pump data.
| Example: Missed callback with missing bottles A patient receives 14 take-home bottles and is selected for a random callback. The patient returns late with two bottles missing. In a manual workflow, the note may live in one place and the toxicology result in another. In OTP diversion monitoring software, callback status, bottle return, toxicology, and risk score should update in one record. |
Biometric + Geofencing Accountability at the Dosing Window
Proxy dosing is one of the most persistent diversion risks in methadone clinics: someone other than the enrolled patient presents at the window to receive a dose. The defense is reliable patient identity verification at the exact moment medication leaves secure inventory.
There are several identity options. Photo-ID checks are fast but easy to rush and easy to fake. Fingerprint and iris systems are stronger but can be slow, require contact, and struggle in high-volume settings. Facial biometric verification — particularly a facial-matrix approach that reads multiple points across the face — adds a fast, non-contact layer that fits the realities of a busy dosing line and helps verify that the right patient is present.
Geofencing adds context. It confirms that a dosing event is occurring in the expected clinical location, which is useful for satellite or mobile dosing and for strengthening the audit trail. The combination of identity + location + dose event is stronger documentation than any single check. None of this eliminates proxy dosing; it helps reduce it, helps verify identity, adds an accountability layer, and supports audit trails. Biometrics also carry real privacy and operational caveats — enrollment quality, consent, and lighting all matter — which is why these tools support staff judgment rather than replace it. Where confirmed in its product configuration, MASE supports facial biometric verification combined with geofencing at the dosing window as part of its medication-accountability model.
| Example: Proxy dosing risk at 7:30 a.m. A busy clinic is moving patients through the dosing line. A patient photo looks similar, staff are under pressure, and a manual ID check is rushed. Facial biometric verification plus dosing-window audit logs can help create a stronger identity record before medication is dispensed — adding an accountability layer rather than replacing staff judgment. |
Serialized Take-Home Bottle Tracking and Chain-of-Custody
Take-home bottles are the single biggest OTP-specific gap in most diversion tools. Inside the clinic, dosing is observed. The moment a bottle is issued, visibility usually drops to a manual log. Serialized bottle tracking closes that gap.
At issuance, each bottle receives a unique serial, typically encoded in a QR or barcode, linked to the patient, dose, lot, serial number, pour date, dispensing staff user, and take-home schedule. On return, the bottle is scanned and verified against what was issued. The system flags late, missing, or damaged bottles automatically and captures tamper documentation when it occurs.
Serialized tracking is most powerful when it is not standalone. Bottle counts from callbacks should reconcile against issued serials; unreturned or tampered bottles should raise the patient’s composite risk score; and every event should land in the audit trail as evidence for DEA and accreditation review. Where confirmed in its product configuration, MASE provides native serialized QR bottle tracking with return verification, wired directly into its callback and risk-scoring workflows and into the underlying OTP methadone EMR.
Hospital Diversion Software vs. OTP-Specialized Software
Hospital diversion platforms — Bluesight ControlCheck, Wolters Kluwer Sentri7, Imprivata Drug Diversion Intelligence, BD HealthSight, Omnicell, and Iatric DetectRx — are built around ADCs, EHR/MAR reconciliation, staff behavior and peer benchmarking, waste, returns, pharmacy vaults, and investigation case workflows. They are genuinely good at what they were designed for: catching staff diversion inside a hospital.
OTP-specialized platforms have to cover a different surface: observed dosing, take-home bottles, callbacks, liquid methadone, pump synchronization, patient identity, geofencing, DCP documentation, and patient-level risk scoring. The honest framing is that several capabilities are publicly documented for hospital tools and not clearly documented for OTP use, and vice versa. The table below compares categories, not vendor marketing claims.
| Capability | Hospital Diversion Tools | General MAT/BH EHRs | Callback-Only Tools | OTP-Native Platform Like MASE |
| ADC/staff transaction monitoring | Core strength | Limited | No | Not the focus (patient-facing) |
| EHR/MAR reconciliation | Yes | Partial | No | Yes, OTP-oriented |
| Observed dosing support | No | Partial | No | Yes |
| Facial biometric verification | No | Rare | No | Yes (facial matrix) |
| Geofencing / context verification | No | No | No | Yes |
| Automated callbacks | No | Sometimes | Yes | Yes |
| Serialized bottle tracking | No | Rare | No | Yes |
| Pump synchronization | No | Sometimes | No | Yes (MethaSpense/SciLog/IVEK) |
| Liquid methadone inventory reconciliation | No | Partial | No | Yes |
| Patient-level diversion risk scoring | No (staff-level) | Flags only | Limited | Yes (composite) |
| DCP documentation | No | Partial | Partial | Yes |
| Audit-ready reporting | Yes (hospital format) | Partial | Limited | Yes (DCP-aligned) |
| OTP workflow fit | Poor | Moderate | Narrow | Built for OTPs |
Two practical takeaways: hospital tools create blind spots at the dosing window and in the community, and partial solutions still leave gaps. To be fair about it, hospital diversion platforms are not “bad” tools — they are often strong for inpatient medication surveillance, staff behavior analytics, ADC reconciliation, and pharmacy investigation workflows. The issue is category fit. OTPs need those same accountability principles translated into a different operating model: observed dosing, take-home bottles, callbacks, pump reconciliation, and patient-level diversion risk.
If you are searching for Bluesight ControlCheck alternatives, Sentri7 diversion software, Protenus drug diversion surveillance, or other drug diversion monitoring software alternatives, first decide whether your main risk is hospital staff diversion or OTP take-home medication accountability. The best OTP diversion control software should connect take-home bottle tracking, callbacks, pump reconciliation, toxicology, and DCP reporting without forcing staff back into spreadsheets.
If you are weighing a general behavioral-health EHR, it is worth reviewing an AZZLY Rize alternative for methadone clinics against OTP-specific criteria rather than hospital-style ones. For a fuller field, compare the best OTP EMR software side by side.
Hospital tool or OTP-native platform?
Compare MASE against hospital diversion tools using an OTP-specific checklist — dosing window, take-homes, callbacks, and pump sync.
Book a Diversion Control DemoDrug Diversion Monitoring Software Pricing and Total Cost of Ownership
Buyers searching to compare the prices of drug diversion monitoring software solutions quickly hit a wall: most vendors, especially hospital platforms, use quote-based enterprise pricing with little public transparency. Rather than invent exact competitor numbers, the more useful approach is to compare the cost categories that actually drive total cost of ownership.
Those categories include subscription cost, setup and implementation, pump integration, SMS and callback tooling, bottle labeling and QR supplies, staff training, compliance reporting, the staff time spent on manual reconciliation, and RCM/billing integration. The hidden line item is the opportunity cost of fragmented tools — three systems that do not talk to each other cost more in labor and risk than their combined invoices suggest.
| Cost Area | Hospital Diversion Tools | General MAT EHR | Manual/Spreadsheet Process | MASE OTP Platform |
| Subscription | Custom quote; commonly enterprise-priced | Custom quote | Low license cost | $450 per active provider / month (confirm current pricing) |
| Setup / implementation | Varies; can be significant | Varies | None upfront | $0 setup where offered |
| Pump integration | Not OTP-focused | Sometimes add-on | Manual | Designed to support MethaSpense/SciLog/IVEK where configured |
| SMS / callback tooling | Not included | Sometimes add-on | Phone trees | Available in configured implementation |
| Bottle labeling / QR | Not applicable | Rare | Manual labels | Serialized QR available if included in configuration |
| Staff training | Significant | Moderate | High ongoing | Onboarding/support based on agreement |
| Compliance reporting | Hospital format | Partial | Manual assembly | DCP-aligned, exportable |
| Manual reconciliation time | Moderate | Moderate-high | Highest | Designed to reduce manual reconciliation |
| RCM / billing integration | No | Sometimes | No | Optional RCM (confirm current rate) |
Pricing varies by clinic size, modules, integrations, contract terms, and implementation needs. Clinics should confirm all pricing directly with vendors. Where its product configuration confirms it, MASE lists transparent pricing at $450 per active provider per month with $0 setup fees, optional Revenue Cycle Management at 2.85% of collections, and a Growth Bridge model that can reduce upfront cost for qualifying programs during the initial period. That structure often lowers total cost of ownership by consolidating multiple tools into one, but it will not save every clinic money in every scenario. For deeper figures, see the methadone clinic software pricing breakdown, and review OTP billing services if clinical accountability and revenue capture matter together.
Map the real cost to your clinic
Walk through pricing, pump integration, callbacks, and DCP documentation against your take-home volume and audit pain points.
Schedule a DCP-Focused MASE WalkthroughHow to Choose the Best OTP Diversion Control Software in 2026
Start the evaluation from OTP-specific risk, not hospital-only criteria. A platform can score perfectly on ADC monitoring and still fail every workflow that defines a methadone clinic. When you shortlist methadone clinic diversion control software, prioritize take-home bottle tracking and callback automation first, then evaluate pump integration, biometric and geofencing verification, dosing-window controls, composite patient risk scoring, DCP documentation, and audit-ready reporting. Compare total cost of ownership, not just the subscription line.
| Evaluation Area | Must-Have Requirement | Questions to Ask the Vendor | Red Flag |
| OTP workflow fit | Built for observed dosing + take-homes | Does the platform support OTP workflows specifically? | Hospital logic retrofitted |
| Take-home accountability | Serialized bottle tracking + returns | Does it support take-home bottle tracking? | Manual logs only |
| Callbacks | Randomize, remind, log, escalate | Does it automate callbacks end to end? | Spreadsheet workarounds |
| Pump integration | Native, bidirectional sync | Does it integrate with MethaSpense, SciLog, or IVEK? | “Coming soon” or manual export |
| Identity | Patient verification at the window | Does it support facial biometric verification or identity checks? | Photo ID only |
| Context | Location verification | Does it support geofencing / context verification? | No location context |
| Risk visibility | Unified patient risk view | Can it connect toxicology, callbacks, bottles, and dosing into one risk score? | Isolated flags only |
| Audit readiness | Exportable DCP evidence | Can it export audit-ready DCP evidence? | Reports need manual assembly |
| Integration | Clinical + inventory + billing | Does it connect clinical, inventory, and billing workflows? | Standalone silo |
| Total cost | Transparent TCO | What setup, training, SMS, integration, and support fees apply? | Opaque pricing, hidden fees |
If a vendor cannot answer the OTP-specific questions clearly, that is itself a signal. The platforms worth shortlisting are the ones that can connect dosing, take-homes, callbacks, toxicology, and pump records into a single, exportable accountability record. That is the bar MASE is built to meet.
Why MASE Is Purpose-Built for OTP Medication Accountability
MASE is not trying to be another generic behavioral health EMR with a dosing module. It is built around the operational reality of OTPs: morning dosing pressure, liquid methadone reconciliation, take-home accountability, callbacks, compliance documentation, and billing complexity. In other words, it is positioned as drug diversion monitoring software for OTPs, not a hospital surveillance platform adapted for methadone clinic workflows.
MASE is OTP-native. It was designed around methadone clinic realities rather than retrofitted from hospital diversion software, and it is built around medication accountability from the dosing window into the community.
Where confirmed in a clinic’s product configuration, MASE helps connect dosing, take-homes, callbacks, toxicology, pump records, and audit evidence into one workflow. That includes observed dosing plus take-home accountability, facial biometric verification combined with geofencing at the dosing window, serialized QR/barcode bottle tracking with return verification, fully automated callback workflows, composite patient risk scoring, and pump synchronization designed to support MethaSpense, SciLog, and IVEK depending on implementation scope.
On the compliance side, MASE supports diversion-control documentation with DEA/DCP audit-ready records and digital DEA Form 222 / CSOS workflows, and it pairs naturally with optional OTP billing and RCM so clinical accountability and revenue capture live in one place — backed by a methadone clinic EMR rather than a bolt-on. For qualifying programs, the Growth Bridge model can reduce upfront cost during the initial period. The MethaSpense and SciLog hardware integration was built and tested directly on the pumps, which is part of why the MethaSpense and SciLog pump sync works as a native reconciliation path rather than a manual export.
None of this makes MASE the only platform, the first-in-country option, or universally best for every OTP, and it does not guarantee compliance or prevent all diversion. What it does is help reduce manual reconciliation and help create review-ready evidence, built for OTP realities rather than generic hospital diversion monitoring. The most useful next step is a scoped demo against your own dosing, pump, take-home, callback, and audit workflows.
| OTP Pain Point | MASE Workflow |
| Manual take-home bottle logs | Serialized QR/barcode bottle tracking |
| Missed callback documentation | Automated callback selection, reminders, logging, escalation |
| Proxy dosing risk | Facial biometric verification + geofencing where configured |
| Pump/inventory mismatch | MethaSpense/SciLog/IVEK pump sync where configured |
| Audit scramble | DCP-aligned reports and timestamped audit trails |
| Billing leakage | Optional OTP billing/RCM support |
FAQs About Drug Diversion Monitoring Software
What is drug diversion monitoring software?
Drug diversion monitoring software is a controlled-substance monitoring tool that tracks regulated medications across their lifecycle and flags unusual patterns for human review. It reconciles dispensing, inventory, waste, returns, and audit logs to surface possible diversion. It supports investigation and documentation; it does not, on its own, prove that diversion occurred.
What is drug diversion monitoring software for OTPs?
Drug diversion monitoring software for OTPs extends standard controlled-substance monitoring to patient-facing accountability in methadone clinics. It adds observed-dosing identity checks, serialized take-home bottle tracking, automated callbacks, pump reconciliation, and toxicology context, then unifies those signals into DCP documentation and audit-ready records built for the OTP model.
Is drug diversion monitoring software required under 42 CFR Part 8?
42 CFR Part 8 does not mandate a specific drug diversion monitoring software product. It does require every OTP to maintain a current Diversion Control Plan with specific measures and assigned staff responsibility. Software is not legally required, but it makes implementing, documenting, and demonstrating those controls far easier during DEA inspections and accreditation surveys.
What is an OTP Diversion Control Plan?
An OTP Diversion Control Plan (DCP) is a required part of a program’s quality assurance under 42 CFR Part 8. It documents the specific measures the clinic uses to reduce the chance that dispensed MOUD is diverted, assigns responsibility to identified staff, and ties take-home decisions to diversion-risk assessment. Software helps operationalize and document the DCP.
How is hospital drug diversion software different from OTP diversion software?
Hospital drug diversion software monitors staff activity inside automated dispensing cabinets and reconciles EHR/MAR and waste records in closed acute-care settings. OTP diversion software must also handle patient-facing accountability: dosing-window identity, take-home bottle chain-of-custody, callbacks, liquid methadone pump reconciliation, and 42 CFR Part 8 DCP documentation. The workflows and risk vectors differ substantially.
How do automated callbacks work in methadone clinics?
Automated callbacks randomly select take-home patients to return — often within a short policy window — for a medication count and toxicology check. The software sends SMS reminders, schedules the visit, documents bottle counts and tamper checks, logs results to the chart, and escalates missed callbacks. Connected to bottle tracking and risk scoring, callbacks become continuous diversion-control evidence rather than isolated events.
How does bottle tracking help prevent methadone diversion?
Serialized bottle tracking assigns each take-home bottle a unique QR or barcode at issuance, linked to patient, dose, lot, pour date, and schedule. On return, bottles are scanned and verified, and late, missing, or damaged bottles are flagged automatically. This creates chain-of-custody evidence for the highest-risk part of OTP care and helps reduce — though not eliminate — take-home diversion.
How do facial biometrics and geofencing help at the dosing window?
Facial biometric verification confirms the enrolled patient is present before a dose is released, helping reduce proxy dosing that photo-ID checks can miss. Geofencing adds location context that the dose is happening in the expected clinical setting. Together they create a stronger identity-plus-context audit trail. They support staff judgment and audit readiness rather than replacing them.
How much does drug diversion monitoring software cost?
Drug diversion monitoring software pricing is usually quote-based, especially for hospital platforms, so published numbers are rare. Total cost of ownership includes subscription, setup, pump and callback tooling, QR supplies, training, reporting, and manual reconciliation time. MASE lists transparent pricing at $450 per active provider per month with $0 setup, but clinics should confirm all pricing directly with vendors.
What is the best drug diversion monitoring software for methadone clinics?
The best drug diversion monitoring software for methadone clinics is the one built for OTP workflows rather than adapted from hospital tools. Prioritize serialized bottle tracking, automated callbacks, pump integration, dosing-window identity verification, and composite patient risk scoring in one audit-ready system. MASE is purpose-built for these requirements; compare it against your own workflows in a scoped demo.
What are Bluesight ControlCheck alternatives for OTPs?
Bluesight ControlCheck is primarily positioned around hospital and health-system diversion monitoring. OTPs comparing alternatives should look for patient-facing workflows such as observed dosing support, take-home bottle tracking, automated callbacks, methadone pump integration, and DCP documentation. For methadone clinics, category fit matters more than generic diversion analytics.
Is hospital drug diversion software enough for a methadone clinic?
Usually not by itself. Hospital drug diversion software is designed around automated dispensing cabinets, staff access, waste documentation, and inpatient medication administration. Methadone clinics also need patient identity verification, take-home bottle chain-of-custody, callback documentation, pump reconciliation, and 42 CFR Part 8 Diversion Control Plan evidence.
Ready to evaluate OTP-native diversion control software? Schedule a scoped MASE demo focused on your dosing, pump, take-home, callback, billing, and compliance workflows.
Evaluate OTP-native diversion control software
Schedule a scoped MASE demo focused on your dosing, pump, take-home, callback, billing, and compliance workflows.
Schedule a Scoped MASE Demo
