NEMT Denial Codes Explained: Complete Guide to Claim Rejections, Appeals & Prevention
Table of Contents
The average NEMT provider loses $50,000 to $150,000 annually to preventable claim denials. With industry denial rates hovering between 15-25%, that translates to roughly $10.6 billion in lost revenue across the non-emergency medical transportation sector each year.
Here’s what makes that number particularly frustrating: 65-70% of NEMT denials are completely preventable. They stem from missing documentation, coding errors, and authorization gaps—problems that proper workflows and training can eliminate before they cost you money.
This guide provides a complete reference to every denial code you’ll encounter in NEMT billing, with specific causes, step-by-step resolution processes, and prevention strategies tailored to transportation providers. Whether you’re troubleshooting a CO-16 denial on your desk right now or building systems to prevent future rejections, you’ll find actionable guidance here.
Understanding NEMT Claim Denials {#understanding-denials}
Before diving into specific codes, let’s clarify the terminology that confuses many providers.
What Is a Claim Denial vs. Rejection?
A claim rejection occurs before the payer ever processes your claim. The clearinghouse or payer system kicks it back immediately due to technical errors—invalid patient ID, missing data fields, incorrect HCPCS codes. Rejections never enter the adjudication system and must be corrected and resubmitted.
A claim denial occurs after the payer reviews and processes your claim but refuses payment. The payer examined your documentation and made a coverage, authorization, or medical necessity determination against you. Denials require formal appeals to recover payment.
The distinction matters because rejections are usually faster to fix (correct the error, resubmit), while denials involve longer timelines and formal appeal processes.
How Denial Codes Work: CARC and RARC Explained
When a claim is denied or adjusted, the payer communicates the reason through standardized codes on your Explanation of Benefits (EOB) or Electronic Remittance Advice (ERA).
CARC (Claim Adjustment Reason Codes) explain why payment was adjusted, reduced, or denied. They appear with group codes that indicate financial responsibility:
| Group Code | Meaning | Can Bill Patient? |
|---|---|---|
| CO | Contractual Obligation | No |
| PR | Patient Responsibility | Yes |
| OA | Other Adjustment | Varies |
| PI | Payer Initiated | No |
| CR | Correction/Reversal | No |
RARC (Remittance Advice Remark Codes) provide supplemental explanations that clarify the CARC. They often identify the specific missing field or required action. Common RARCs in NEMT include M12 (missing documentation), N264 (missing provider ID loop), and N522 (refer to payer manual).
Always read CARC and RARC together—the CARC tells you the category of problem, while the RARC points to the specific fix.
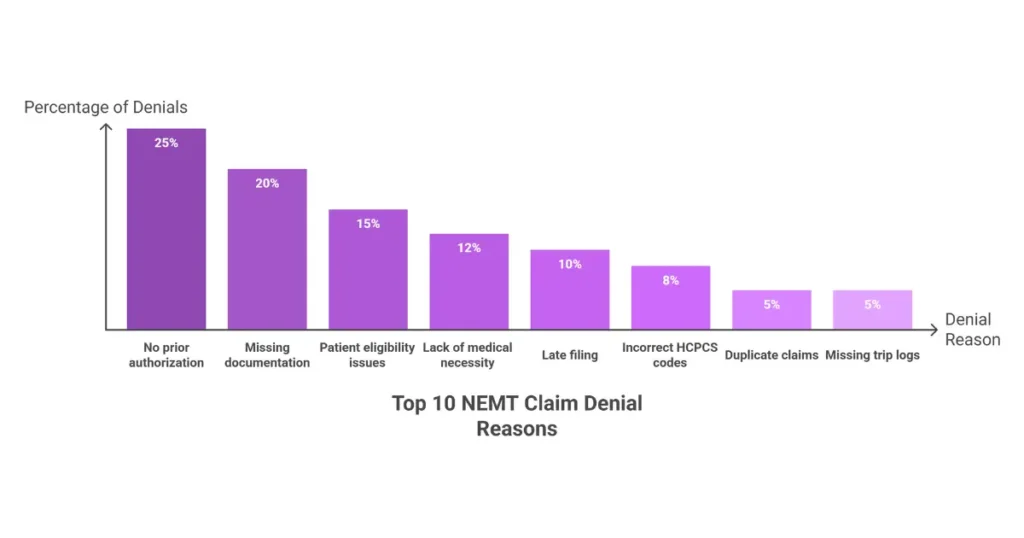
Why NEMT Claims Get Denied: The Top 10 Reasons
NEMT claims face unique denial patterns that differ from general medical billing:
| Rank | Denial Reason | % of Denials | Preventable? |
|---|---|---|---|
| 1 | Missing or invalid Medicaid ID | 12-15% | Yes |
| 2 | No prior authorization or trip certification | 20-25% | Yes |
| 3 | Incorrect HCPCS codes (A0425 without mileage) | 8-12% | Yes |
| 4 | Lack of medical necessity documentation | 10-15% | Yes |
| 5 | Duplicate trip billing | 5-8% | Yes |
| 6 | Late filing beyond payer deadlines | 8-12% | Yes |
| 7 | Ineligible patient or non-covered service | 10-15% | Partially |
| 8 | Missing trip logs (origin/destination mismatch) | 8-10% | Yes |
| 9 | Inactive or invalid NPI/credentialing | 3-5% | Yes |
| 10 | Date-of-service vs. submission timing errors | 3-5% | Yes |
The pattern is clear: administrative and documentation errors drive 60-70% of NEMT denials, coverage and medical necessity issues account for 20-30%, and duplicates or late filing cause 10-15%.
The Financial Impact of NEMT Denials
Understanding denial costs helps prioritize prevention investments:
| Cost Component | Amount |
|---|---|
| Administrative rework per denial | $25-$125 |
| Lost revenue/opportunity cost | $100-$300 |
| Total cost per denial | $125-$425 |
| Annual loss (small-mid provider) | $50,000-$250,000 |
| Appeal success rate | 40-60% |
| Unappealed denials (industry avg.) | ~65% |
That last statistic is critical: 65% of denied NEMT claims are never appealed, leaving approximately $6.9 billion in recoverable revenue abandoned annually across the industry.
For detailed billing procedures that prevent these denials, see our complete NEMT billing guide.
CO-16, CO-18, CO-29: Documentation & Filing Codes {#co-16-18-29}
These three codes represent the most common NEMT denials—and the most fixable. They relate to documentation completeness, duplicate submissions, and filing deadlines.
CO-16 Denial Code: Missing or Incomplete Information
What Is CO-16?
CO-16 means “Claim/service lacks information or has submission/billing error(s).” The payer cannot adjudicate your claim because required data elements are missing or invalid.
CO-16 accounts for approximately 20% of all NEMT denials—making it the single most common code you’ll encounter.
Common Causes of CO-16 in NEMT:
- Missing or unsigned trip logs/manifests
- Mileage billed (A0425) not matching GPS data (>10% variance)
- Incomplete or vague Physician Certification Statement (PCS)
- Missing origin/destination modifiers (HR, RH, HE, UD)
- Missing or mismatched prior authorization numbers
- Invalid or missing referring provider NPI
- Incomplete pickup/drop-off times or odometer readings
Remark Codes Commonly Paired with CO-16:
| RARC Code | Meaning |
|---|---|
| M12 | Missing or incomplete documentation |
| M51 | Missing required documentation |
| M60 | Invalid or missing procedure code |
| M124 | Invalid or missing service dates |
| N56 | Missing or incomplete claim information |
| N264 | Missing X12 provider ID loop |
| N575 | Missing information for authorization |
| N522 | Refer to payer manual |
How to Fix CO-16 Denials:
- Review the EOB/ERA and identify the paired RARC code
- Collect missing documentation (trip log, PCS, GPS proof)
- Correct claim fields and modifiers in your billing system
- Resubmit as corrected claim within payer timeframe
- Track acceptance via clearinghouse or broker portal
If correction and resubmission fails, file a Level 1 appeal within 30-60 days with corrected claim, PCS, trip manifest, and GPS logs.
CO-16 Prevention Checklist:
- ✅ Pre-trip PCS uploaded and validated
- ✅ GPS mileage auto-sync enabled
- ✅ Origin/destination modifiers auto-populated
- ✅ Claim scrubber flags missing X12 loops
- ✅ Quarterly HCPCS and Medicaid update training
CO-18 Denial Code: Duplicate Claim
What Is CO-18?
CO-18 indicates an “exact duplicate claim or service.” The payer identifies matching details—date of service, HCPCS/CPT code, provider NPI, place of service, and charge amount—already processed or pending.
Common Causes of CO-18 in NEMT:
- Same trip submitted twice after initial rejection
- Clearinghouse auto-resubmission without frequency code 7
- Round trips billed without distinct modifiers or timestamps
- Broker trip ID billed under two separate entries
- Manual re-entry after broker approval without reconciliation
How to Fix CO-18 Denials:
- Pull original claim and ERA for comparison
- Verify if it’s a true duplicate (identical in all respects)
- If truly duplicate: Void/delete—no recovery possible
- If not duplicate: Add proper modifier or frequency code 7, attach trip documentation with distinct timestamps, and resubmit
When to Appeal CO-18:
- True duplicate: No appeal (no recovery)
- False duplicate: Appeal within 30 days with side-by-side claim comparison showing distinct services
- Appeal success rate for false duplicates: 50-70%
CO-18 Prevention Strategies:
- Unique trip ID enforcement in dispatch system
- Duplicate detection via clearinghouse
- Broker API integration for real-time status
- Daily reconciliation logs
- Staff training on claim frequency codes
CO-29 Denial Code: Timely Filing Exceeded
What Is CO-29?
CO-29 means “The time limit for filing has expired.” Your claim was received after the payer’s contractual submission deadline, measured from the date of service (DOS).
This is typically a hard denial with very limited appeal options.
Timely Filing Limits by Payer:
| Payer Type | Filing Deadline |
|---|---|
| State Medicaid (varies) | 90-365 days |
| California | 90 days |
| Texas | 95 days |
| New York | 90 days |
| Florida | 365 days |
| NEMT Brokers | |
| ModivCare | 90 days |
| MTM | 120 days |
| Veyo | 60-90 days |
| Access2Care | 180 days |
| Medicare Advantage | 120-365 days |
Common Causes of CO-29 in NEMT:
- Late receipt of driver trip logs from field
- Delayed broker authorization posting
- Manual billing backlogs in high-volume operations
- Incorrect assumption that deadline starts after approval (it starts at DOS)
- Lack of submission tracking or deadline alerts
How to Fix CO-29 Denials:
- Verify payer-specific filing deadline
- Check submission logs or clearinghouse reports
- If filing was late: Write off (usually non-recoverable)
- If filed timely: Submit proof of timely filing with appeal
CO-29 Appeal Options:
CO-29 appeals rarely succeed (10-20% success rate) except when you can provide:
- Proof of timely submission (clearinghouse timestamp)
- Evidence of payer system error
- Good cause exception (disaster, retroactive eligibility)
With documented proof of timely filing, success rates increase to 30-50%.
CO-29 Prevention Strategies:
- Automated timely filing alerts 7-14 days before deadline
- Weekly “unbilled trips” audits
- Same-day broker approval reconciliation
- Submission timestamp documentation retained for all claims
CO-197, CO-96, CO-15: Authorization & Coverage Codes {#co-197-96-15}
Authorization-related denials are among the costliest in NEMT billing because they often involve completed trips where you’ve already incurred the expense of providing service.
CO-197 Denial Code: Missing Prior Authorization
What Is CO-197?
CO-197 means “Precertification/authorization/notification absent.” No payer or broker approval was obtained or documented before the service.
CO-197 represents approximately 20-25% of NEMT denials and is particularly common with broker-managed programs (ModivCare, MTM, Veyo) where trip-level authorization is mandatory.
Common Causes of CO-197 in NEMT:
- No prior broker authorization (missing trip ID)
- Authorization expired before date of service
- Level of service mismatch (wheelchair authorized, stretcher billed)
- Authorization requested after trip completion
- Mileage thresholds exceeded without updated PA
- Provider mismatch between authorization and billing entity
The Difference Between CO-197 and CO-198:
| Code | Meaning |
|---|---|
| CO-197 | No authorization exists at all |
| CO-198 | Authorization exists but is invalid, mismatched, or doesn’t apply to billed service |
| CO-15 | Authorization exists but is missing or invalid on the claim itself |
| PR-197 | Same as CO-197 but patient assigned responsibility (rare in NEMT) |
How to Fix CO-197 Denials:
- Check if retroactive authorization is available (some Medicaid plans and brokers allow retro-auth within 24-72 hours; extended retro-auth possible within 30 days with medical necessity documentation)
- Gather required documentation: PCS, physician necessity letter, trip logs, GPS records
- Submit retroactive authorization request through broker portal
- If retro-auth denied, file formal appeal within 30-60 days
- Include corrected CMS-1500 with valid authorization in Block 23
Retroactive authorization success rate: 60-80% with complete documentation.
CO-197 Prevention Strategies:
- Broker portal checks 48 hours pre-trip
- Authorization expiration alerts via NEMT dispatch software
- API integrations with MTM, ModivCare for real-time auth status
- PCS templates uploaded before trip assignment
- Block 23 audit before claim submission
CO-96 Denial Code: Non-Covered Service
What Is CO-96?
CO-96 means “Non-covered charge(s).” The service you billed falls outside the patient’s plan benefits—it’s not a coding error, it’s a coverage determination.
Common Causes of CO-96 in NEMT:
- Non-medical destinations (pharmacy-only trips, grocery store)
- Luxury or non-covered vehicle class (sedan when ambulatory required)
- Escort/attendant fees not included in benefit
- Deadhead mileage billed without patient onboard
- Wrong payer billed (Medicare vs. Medicaid)
- Benefit exhausted (annual trip limit reached)
How to Fix CO-96 Denials:
- Verify coverage under patient’s specific plan
- If wrong payer: Rebill correct payer within their filing deadline
- If coverage dispute exists: Appeal with medical necessity documentation and PCS
- If truly non-covered: Bill patient only if Advance Beneficiary Notice (ABN) was signed before service; otherwise, write off
CO-96 Prevention:
- Real-time eligibility verification before every trip
- Benefit confirmation including trip limits
- ABN signed before non-covered services
- Driver training on covered vs. non-covered destinations
CO-15 Denial Code: Authorization Number Missing/Invalid
What Is CO-15?
CO-15 means “Authorization number is missing, invalid, or does not apply to the billed service.” Unlike CO-197 (no auth exists), CO-15 indicates an authorization exists but wasn’t properly included or matched on the claim.
Common Causes of CO-15 in NEMT:
- Authorization number not entered in claim Block 23
- Authorization number entered incorrectly (typo)
- Authorization expired on date of service
- Authorization issued for different provider than billing entity
- Authorization for different service level than billed
How to Fix CO-15 Denials:
- Verify authorization exists in broker/payer system
- Correct authorization number in Block 23
- Confirm service level matches (wheelchair auth = wheelchair billing)
- Resubmit corrected claim
This is typically a “soft denial” that resolves quickly with correction—no formal appeal needed unless the underlying authorization is disputed.
Additional Denial Codes: CO-45, CO-50, CO-11, PR Codes {#additional-codes}
Beyond the major denial codes, several additional codes appear frequently in NEMT billing.
CO-45: Charges Exceed Fee Schedule
What It Means: You billed more than the payer’s contracted or legislated maximum allowable fee.
NEMT Context: Mileage billed above state Medicaid per-mile cap, incorrect rate loaded in billing system, or broker rate differs from what you expected.
Resolution: Adjust to allowed amount; the excess is a contractual write-off. Appeal only if payment is below your signed contract rate.
CO-50: Non-Covered / Not Medically Necessary
What It Means: Service not covered because the diagnosis doesn’t support medical necessity.
NEMT Context: Wheelchair transport billed when ambulatory was deemed sufficient based on diagnosis; stretcher transport without supporting clinical documentation.
Resolution: Submit PCS with clear mobility limitations, appeal with physician letter emphasizing medical necessity and safety.
CO-11: Diagnosis Inconsistent with Procedure
What It Means: The diagnosis code is incorrect or inconsistent with the billed procedure.
NEMT Context: Ambulatory code billed with paralysis diagnosis; wheelchair transport billed with minor or unrelated diagnosis that doesn’t justify the service level.
Resolution: Review clinical notes, correct diagnosis code(s) to align with transport level, resubmit.
CO-97: Bundled Service
What It Means: The service is included in payment for another already adjudicated service—you can’t bill it separately.
NEMT Context: Round-trip mileage billed when one leg already paid; wait-time or escort fees bundled into base rate.
Resolution: Verify bundling rules; if services are truly distinct, submit split-trip logs with separate timestamps and appeal.
Patient Responsibility Codes: PR-1, PR-2, PR-3
These codes indicate amounts the patient must pay—they’re not denials in the traditional sense.
| Code | Meaning | NEMT Application |
|---|---|---|
| PR-1 | Deductible | Patient hasn’t met annual deductible (common in Medicare Advantage) |
| PR-2 | Coinsurance | Patient owes percentage after deductible (typically 10-20%) |
| PR-3 | Copayment | Fixed dollar amount per service ($1-$10 per trip) |
Important: For Medicaid NEMT, balance billing is prohibited. PR codes must be adjusted to $0—billing Medicaid patients is a compliance violation.
For Medicare Advantage and commercial plans, you may collect PR amounts from patients through proper billing procedures.
Broker & Payer-Specific Denial Patterns {#broker-patterns}
Different brokers and payers have distinct denial patterns. Understanding these helps you tailor prevention and resolution strategies.
ModivCare Denial Patterns
Top Denial Codes: CO-16, CO-197, CO-29, CO-18, CO-150
Primary Triggers:
- Missing or incorrect Trip ID
- GPS route vs. billed mileage mismatch
- Unsigned driver or patient trip sheets
- Level of service mismatch
- Claims filed after 90-day window
Resolution Workflow:
- Portal: TripCare/Provider Portal → Claims → Correct/Reconsider
- Upload GPS logs, driver trip sheet, manifest
- Resubmit within 90 days
- Appeals window: 60 days
- Success rate: ~50% with complete GPS + trip logs
Prevention Tips:
- Pre-upload routes before billing
- Validate Trip ID before submission
- Monitor “Pending” errors in real-time portal
MTM Denial Patterns
Top Denial Codes: CO-15, CO-18, CO-96, CO-27, CO-222
Primary Triggers:
- Authorization expiring during multi-leg trips
- Eligibility lapses between scheduling and service
- Incorrect origin/destination modifiers
- Units billed exceed authorized mileage
Resolution Workflow:
- Portal: Provider Zone → Disputes
- Attach retroactive authorization, physician letter/PCS
- Appeals window: 60-120 days (state dependent)
- Success rate: 60-70% with retro auth + PCS
Prevention Tips:
- Use MTM API for real-time auth verification
- Weekly eligibility scrubs
- Batch eligibility checks 24 hours pre-trip
Veyo Denial Patterns
Top Denial Codes: CO-198, CO-50, PR-19, CO-97, CO-16
Primary Triggers:
- App-generated trip sheet errors
- Incorrect wheelchair vs. ambulatory coding
- Missing patient signature (POD)
- Mileage entry issues during peak hours
Resolution Workflow:
- Veyo Driver App → Billing → Dispute
- Upload photos of trip sheets, GPS screenshots
- Appeals window: 45 days
- Success rate: ~40% with photo evidence
Prevention Tips:
- Screenshot every completed trip
- Avoid peak-hour submissions when possible
- Review QA alerts in app regularly
State Medicaid (FFS) Denial Patterns
Top Denial Codes: CO-197, CO-29, CO-16, CO-96
Common Patterns:
- Texas: PCS required for all trips
- California: GPS logs mandatory
- New York: 90-day filing limit strictly enforced
- Florida: 365-day filing but rigorous mileage audits
Resolution: Check state Medicaid portal for denial reason, submit retro auth/PCS via state system, appeal within 30-120 days with trip logs, manifests, and GPS.
Appeal Success Rate: ~60% with complete documentation
Medicare Advantage Denial Patterns
Top Denial Codes: PR-204, CO-96, CO-50, CO-197, CO-15, CO-119
Primary Drivers:
- Annual trip caps (12-40 trips/year)
- Luxury or upgraded transport excluded
- PCP referral required but missing
- Plan-specific authorization rules vary significantly
Resolution: Verify remaining benefits via Availity, appeal with physician note, resubmit corrected auth, bill patient for PR balances when allowed.
Recovery Rate: ~50% on appealed claims
Broker Comparison Summary
| Entity | Typical Denial Rate | Primary Fix | Appeal Success |
|---|---|---|---|
| ModivCare | ~25% | GPS & Trip ID proof | ~50% |
| MTM | ~18% | Retro auth + PCS | 60-70% |
| Veyo | ~20% | App screenshots | ~40% |
| Access2Care | ~15% | Split AM/PM legs | ~55% |
| Medicaid FFS | 18-25% | State portals | ~60% |
| Medicare Advantage | 20-30% | Benefit verification | ~50% |
How to Appeal NEMT Claim Denials {#appeals}
When prevention fails and denials occur, a systematic appeal process recovers revenue that would otherwise be lost.
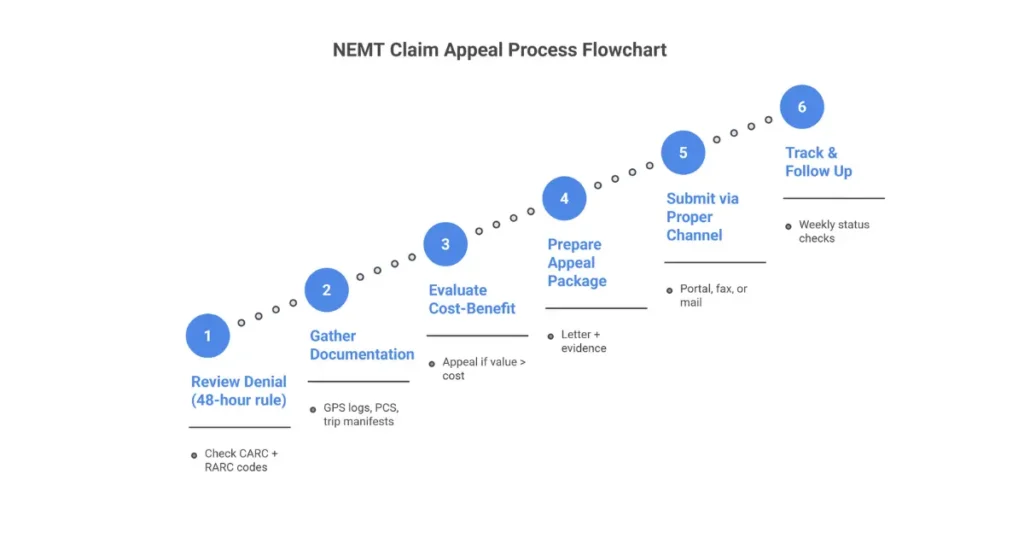
Step 1: Review the Denial Thoroughly (48-Hour Rule)
Review every denial within 48 hours of receiving the EOB/ERA:
- Identify the CARC code (CO-197, CO-16, etc.)
- Identify the RARC code (M81, N522, etc.) for specific guidance
- Categorize the denial:
- Administrative: NPI typo, missing modifier, invalid ID
- Clinical/Logical: Medical necessity, trip feasibility
- Technical: GPS mileage vs. billed mileage
- Cross-reference X12.org, state Medicaid portals, or broker guidelines
Step 2: Gather Supporting Documentation
Golden Rule: If it wasn’t logged, it didn’t happen.
| Denial Type | Required Documentation |
|---|---|
| Authorization (CO-197, CO-15) | Retroactive auth, PCS, broker trip ID, physician letter |
| Documentation (CO-16) | Signed trip manifests, GPS logs, origin/destination proof, signatures |
| Timely Filing (CO-29) | Original submission timestamps, clearinghouse acceptance reports |
| Non-Covered (CO-96) | ABN, benefit verification printouts, PCS if disputable |
Step 3: Determine if Appeal is Worthwhile
Use this cost-benefit formula:
Appeal if: (Claim Amount × Success Probability) > Appeal Cost
Example: $100 claim × 50% success = $50 expected value $50 > $25 appeal cost → Yes, appeal
When to Write Off Instead:
- Revenue < $25
- Success odds < 25%
- Hard CO-29 without proof of timely filing
- Medicaid PR codes (no balance billing allowed)
- Repeated denial after 2 appeals
- Aging > 120 days
Step 4: Prepare the Appeal Package
Every NEMT appeal letter should include:
- Claim number / ICN
- Date(s) of service
- Patient name and member ID
- Denial code(s) received
- Clear explanation of why the denial was incorrect
- Reference to specific policy or criteria
- List of attached supporting documents
- Explicit request to reprocess the claim
Sample Appeal Language:
Opening: “We are formally appealing the denial of the above-referenced claim, which was denied under code CO-197. This determination was made in error based on the documentation provided.”
Argument: “Although the claim was denied for missing authorization, authorization #123456 was approved on [date] for this specific transport as documented in the attached broker confirmation.”
Evidence: “Attached GPS logs confirm pickup at 123 Main St at 09:14 AM, route, and 23.4 miles traveled—consistent with the authorized dialysis transport trip.”
Close: “We respectfully request reconsideration and reprocessing of this claim for payment.”
Step 5: Submit Through Proper Channels
| Payer Type | Primary Submission | Appeal Window |
|---|---|---|
| State Medicaid | State portal | 30-120 days |
| NEMT Brokers | Broker portal | 45-120 days |
| Medicare Advantage | Plan portal or mail | 60-180 days |
Always capture confirmation numbers and timestamps. Avoid email unless explicitly permitted by the payer.
Step 6: Track and Follow Up
- Expected response: 30-45 days
- Check status weekly
- Document all communication
- Escalate if no response after 45 days
Escalation Path:
- Level 1 denied → File Level 2 within 15-30 days
- State Medicaid → Administrative review → Fair hearing
- Medicare Advantage → Independent Review Entity (IRE) within 65 days
Appeal Success Rates by Denial Type
| Denial Code | Success Rate | Key Factor |
|---|---|---|
| CO-197 (Auth) | 60-70% | Retro auth highly effective |
| CO-16 (Docs) | 50-65% | GPS & manifests critical |
| CO-29 (Timely) | 20-40% | Proof-dependent |
| CO-96 (Coverage) | 30-50% | PCS & benefit proof |
Industry-wide: Average appeal success is 40-60%, with top performers achieving up to 70% through systematic tracking and complete documentation.
Denial Prevention Strategies {#prevention}
Preventing denials is significantly more cost-effective than appealing them. A 5% reduction in denial rate on $1M annual billing recovers $50,000—far exceeding the cost of prevention systems.
Pre-Service Prevention (Before the Trip)
Eligibility Verification:
- Run EDI 270/271 eligibility checks at scheduling
- Confirm active Medicaid/Medicare Advantage coverage
- Verify NEMT benefit carve-outs and trip limits
- Reconfirm coverage 24-48 hours prior via broker portals
- Flag inactive IDs early to prevent PR-19 denials
Prior Authorization Management:
- Auto-request trip IDs via broker or state Medicaid APIs
- Ensure authorization matches level of service (sedan vs. wheelchair vs. stretcher)
- Verify date of service falls within authorization window
- Attach PCS templates for dialysis and recurring trips
- Track authorization expiration dates
Medical Necessity Documentation:
- Obtain physician-signed PCS before the trip
- PCS must clearly state functional limitation and inability to self-transport
- Scan PCS into dispatch/billing system pre-trip
Point-of-Service Prevention (During the Trip)
Driver Documentation Requirements (The 5 Pillars):
- Member name verification
- Pickup and drop-off timestamps
- Origin and destination addresses
- Vehicle ID
- Trip purpose
GPS & Mileage Capture:
- Use driver apps with real-time GPS (RouteGenie, TobiCloud, Bambi)
- Sync loaded mileage directly to A0425 billing
- Auto-flag mileage discrepancies > 10%
- GPS ping at every status change (Arrived, Loaded, Unloaded)
Proof of Delivery (POD):
- Electronic patient signature on every trip
- Include timestamp and GPS coordinates
- Digital PODs reduce CO-16 denials and audit recoupments
Claim Submission Prevention (Before Filing)
Claim Scrubbing:
- Validate HCPCS codes (A0425, A0428)
- Verify modifiers (GM, HR, RH, TN, GY, UD)
- Confirm diagnosis-to-procedure matches
- Check against payer fee schedules and mileage caps
- Block CO-45, CO-50, CO-11 errors pre-submission
Duplicate & Frequency Controls:
- Scan for duplicates using Trip ID + DOS + Patient ID
- Prevent auto-resubmission without frequency code 7
- Detect round-trip overlaps before they become CO-18 denials
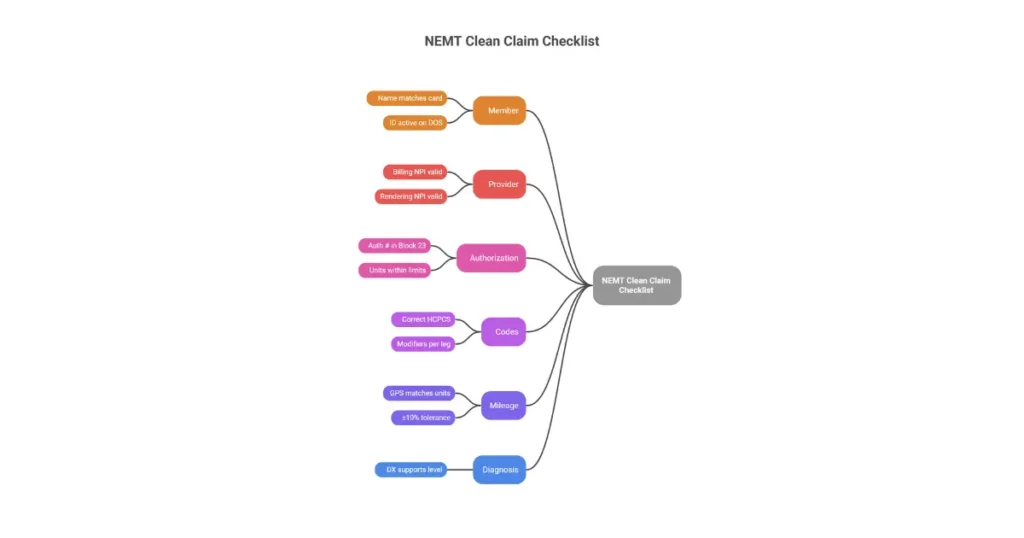
Clean Claim Submission Checklist
Use before batching every claim:
| Category | Verification |
|---|---|
| Member | Name matches Medicaid card; ID active on DOS |
| Provider | Billing & Rendering NPIs present and valid |
| Authorization | Auth # in Field 23; units within authorized limits |
| Codes | Correct HCPCS & modifiers per trip leg |
| Mileage | Odometer/GPS matches billed units (±10%) |
| Diagnosis | DX supports medical necessity for transport level |
| Deadlines | Within timely filing window |
Technology Solutions for Denial Prevention
Essential NEMT Software Features:
- Broker API connectivity (real-time auth status)
- Auto-scrubbing for current HCPCS A-codes
- GPS reconciliation with tolerance thresholds
- Denial risk scoring before submission
- Auto-resubmit workflows for corrected claims
- HIPAA-compliant e-signatures and audit trails
ROI of Prevention Technology:
- Denial reduction: 35-70%
- Clean claim rate improvement: to > 95%
- ROI: 5-12x investment
- Revenue recovery: $100K/year per $1M billed
- Payback period: 3-6 months
Denial Management Metrics & KPIs {#metrics}
What gets measured gets managed. Track these metrics to identify problems early and demonstrate improvement.
Key Metrics and Formulas
Clean Claim Rate (CCR)
- Formula: (Claims Paid on First Submission ÷ Total Submitted) × 100
- Target: 95-98%+
- What it measures: Billing accuracy and process quality
Initial Denial Rate
- Formula: (Denied Claims ÷ Total Submitted) × 100
- Target: < 5% (top tier), < 10% (acceptable)
- What it measures: Prevention effectiveness
First-Pass Payment Rate
- Formula: (Claims Paid First Pass ÷ Total Submitted) × 100
- Target: 90-95%
- What it measures: End-to-end billing efficiency
Days in A/R
- Formula: Total A/R ÷ Average Daily Charges
- Target: < 30 days (clean claims), < 45 days (overall)
- What it measures: Cash flow health
Appeal Success Rate
- Formula: (Appeals Won ÷ Total Appeals Submitted) × 100
- Target: 50-70%
- What it measures: Appeal process effectiveness
Cost per Denial
- Formula: (Staff Hours × Hourly Rate) + Opportunity Cost
- NEMT Average: $25-$75 per denial
- What it measures: True impact of denial problems
Industry Benchmarks
| Metric | Top Tier | Average | Poor |
|---|---|---|---|
| Denial Rate | < 5% | 10-15% | > 20% |
| Clean Claim Rate | 95%+ | 85-90% | < 80% |
| Days in A/R | < 30 | 45-60 | > 90 |
| Appeal Success Rate | 65-70% | ~50% | < 40% |
Monthly Denial Review Process
Timing: 5th business day of each month
60-Minute Agenda:
- 0-15 min: Clean Claim Rate vs. 98% goal
- 15-30 min: Top 5 CARC codes (root cause analysis)
- 30-45 min: Aging A/R > 60 days (timely filing risk)
- 45-60 min: Action plan (training, system fixes, SOP updates)
Track Quarter-Over-Quarter:
- Denial rate trend by payer
- Denial rate trend by code
- A/R aging bucket movement
- Revenue impact calculations
Quick Reference: All NEMT Denial Codes {#quick-reference}
Complete NEMT Denial Code Table
| Code | Category | Description | Common NEMT Cause | Quick Fix |
|---|---|---|---|---|
| CO-15 | Authorization | Auth missing/invalid on claim | Trip ID not in Block 23 | Correct auth number, resubmit |
| CO-16 | Documentation | Missing/incomplete information | GPS logs, trip manifests absent | Upload docs, resubmit |
| CO-18 | Duplicate | Duplicate claim/service | Same trip billed twice | Void duplicate or add modifiers |
| CO-27 | Eligibility | Patient coverage expired | Medicaid inactive on DOS | Check retro-eligibility |
| CO-29 | Timely Filing | Filing deadline missed | Late submission | Appeal with proof or write off |
| CO-45 | Fee Schedule | Charge exceeds allowed amount | Billed above Medicaid cap | Contractual write-off |
| CO-50 | Medical Necessity | Not medically necessary | Insufficient diagnosis support | Appeal with PCS |
| CO-96 | Coverage | Non-covered service | Non-medical destination | Verify coverage, ABN |
| CO-97 | Bundling | Service bundled | Round-trip mileage overlap | Split with timestamps |
| CO-119 | Compliance | Regulatory requirement unmet | Credentialing issue | Resolve credentialing |
| CO-150 | Mileage | Mileage inconsistent | GPS vs. billed mismatch | Submit GPS breadcrumbs |
| CO-197 | Authorization | No prior auth obtained | Missing broker trip ID | Retro auth + appeal |
| CO-198 | Authorization | Auth invalid/mismatched | Wrong service level on auth | Correct auth, resubmit |
| PR-1 | Patient Responsibility | Deductible | Annual deductible unmet | Bill patient |
| PR-2 | Patient Responsibility | Coinsurance | Patient owes percentage | Bill patient |
| PR-3 | Patient Responsibility | Copayment | Fixed copay per trip | Collect at service |
| PR-19 | Eligibility | Coverage inactive | Lapsed during treatment | Re-verify, write off Medicaid |
| PR-204 | Benefit Limit | Trip limit reached | Annual cap exhausted | Appeal for exception |
Code Priority Guide:
- 🔴 Hard Denials: CO-29, CO-27, CO-96, CO-119 (limited appeal options)
- 🟡 Correctable: CO-15, CO-16, CO-18, CO-50, CO-197 (fix and resubmit)
- 🔵 Informational: CO-45, PR-1, PR-2, PR-3 (adjustments, not true denials)
Frequently Asked Questions: NEMT Denial Codes {#faq}
What is a CO-16 denial code?
CO-16 indicates a claim lacks required information or has submission/billing errors, such as missing patient details, GPS logs, or trip sheets. In NEMT, it often flags absent trip manifests, odometer readings, or origin/destination modifiers. Review the paired RARC code (like M12 or N264) to identify exactly what’s missing, then gather the documentation and resubmit within 30-90 days.
How do I fix a CO-16 denial?
To fix a CO-16 denial, first review the RARC code to identify the specific missing element. Gather required documentation such as GPS logs, trip manifests, and PCS forms. Correct the claim fields and modifiers in your billing system. Resubmit as a corrected claim within the payer’s timeframe. If resubmission fails, file a formal appeal with complete documentation.
What does CO-197 denial code mean?
CO-197 means precertification, authorization, or notification was not obtained before the NEMT service. This is one of the most common and costly denials in transportation billing, occurring when broker trip IDs or PCS forms are missing. The claim cannot be processed until retroactive authorization is obtained or a formal appeal is filed with supporting documentation.
How do I fix a CO-197 denial?
First, check if retroactive authorization is available—many brokers allow retro-auth within 24-72 hours. Gather PCS forms, physician necessity letters, and trip documentation. Submit the retro-auth request through the broker portal. If retro-auth is denied, file a formal appeal within 30-60 days with complete documentation. Success rate with proper documentation: 60-70%.
What is the difference between CO-197 and CO-198?
CO-197 means no authorization exists at all—you never obtained approval for the trip. CO-198 means an authorization exists but is invalid, mismatched, or doesn’t apply to the service you billed (wrong service level, wrong dates, wrong provider). CO-197 requires obtaining retroactive authorization; CO-198 usually requires correcting the authorization number and resubmitting.
What are the most common NEMT denial codes?
The most common NEMT denial codes are CO-16 (missing information, ~20% of denials), CO-197 (missing authorization, ~20-25%), CO-29 (late filing, ~10-15%), CO-18 (duplicate claims, ~5-8%), and CO-96 (non-covered service, ~10-15%). Together, these five codes account for approximately 70% of all NEMT claim denials.
How do I appeal a denied NEMT claim?
To appeal a denied NEMT claim: (1) Review the denial code and RARC within 48 hours, (2) Gather supporting documentation including GPS logs, trip manifests, and PCS forms, (3) Prepare an appeal letter citing the specific error and policy reference, (4) Submit through the payer’s preferred channel (portal, fax, mail) within the appeal window, (5) Track and follow up weekly until resolution.
What are the odds of winning an insurance appeal?
NEMT appeal success rates average 40-60%, with top-performing providers achieving up to 70%. Success varies by denial type: CO-197 authorization appeals succeed 60-70% of the time, CO-16 documentation appeals 50-65%, and CO-29 timely filing appeals only 20-40%. Complete documentation and timely submission significantly improve your odds.
Can you dispute a claim that was denied?
Yes, all denied claims can be disputed through the payer’s appeal process. For NEMT claims, submit appeals through broker portals (ModivCare, MTM, Veyo) or state Medicaid systems within the specified timeframe (typically 30-120 days). Include the denial code, corrected claim, and supporting documentation. Even hard denials like CO-29 can sometimes be overturned with proof of timely filing.
What should I do if my NEMT claim is rejected?
A rejection (not a denial) means the claim was never processed due to technical errors. Review the rejection reason, correct the specific error (invalid ID, missing field, incorrect code), and resubmit immediately. Rejections don’t require appeals—they just need correction. Act quickly to avoid missing timely filing deadlines while correcting and resubmitting.
How can I prevent NEMT claim denials?
Prevent NEMT denials by: (1) Verifying eligibility and authorization before every trip, (2) Capturing complete GPS/POD documentation during service, (3) Using claim scrubbing software before submission, (4) Training staff quarterly on coding and documentation requirements, (5) Tracking denial patterns monthly to identify systemic issues. These practices can reduce denial rates by 35-70%.
What is a clean claim rate and why does it matter?
Clean claim rate measures the percentage of claims paid on first submission without edits, rejections, or denials. Target: 95-98%. A 95% clean claim rate versus 85% on $1M annual billing represents $100,000 in faster revenue collection and reduced administrative costs. It’s the single best indicator of billing department effectiveness.
Conclusion: From Denial Frustration to Revenue Recovery
NEMT claim denials cost the industry billions annually—but the providers who master denial prevention and resolution capture revenue their competitors leave on the table.
The key insights from this guide:
- 65-70% of NEMT denials are preventable through proper eligibility verification, authorization management, and documentation capture
- CO-16 and CO-197 account for 40%+ of all denials—focus prevention efforts here first
- Appeal success rates of 50-70% are achievable with systematic processes and complete documentation
- Technology investments pay back 5-12x through reduced denials and faster collections
Your denial rate is a direct reflection of your billing processes. A 15% denial rate on $1M in annual billing means $150,000 at risk—of which $100,000+ is likely recoverable with proper systems.
For providers seeking expert support with denial management, our NEMT billing specialists handle prevention, appeals, and recovery so you can focus on providing transportation services.
Contact us for a free denial analysis—we’ll identify your top denial patterns and show you exactly how much revenue you’re leaving uncollected.

