NEMT Prior Authorization Guide 2026: Requirements, Forms & Step-by-Step Process
The Complete Provider Reference for Medicaid & Medicare Transportation Authorization
Table of Contents
Introduction: Why NEMT Prior Authorization Determines Your Revenue
A single missed prior authorization can cost your NEMT company between $125 and $425 per trip. Multiply that across hundreds of monthly transports, and you’re looking at annual revenue losses of $75,000 to $150,000—money that disappears because of preventable paperwork failures. NEMT prior authorization isn’t just administrative busywork; it’s the gatekeeping mechanism that determines whether you get paid for the services you provide.
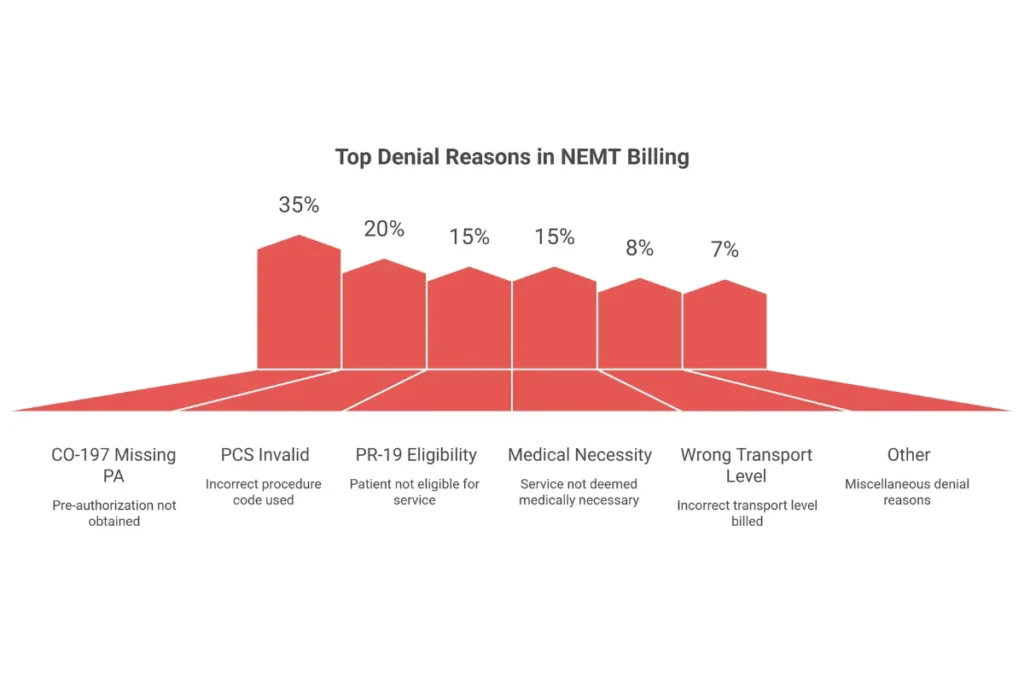
The non-emergency medical transportation industry faces a denial rate of 15% to 25%, with the CO-197 denial code (“No prior authorization on file”) accounting for roughly 35% of all rejected claims. These aren’t abstract statistics. They represent real trips completed, real fuel consumed, and real drivers paid—without a dollar of reimbursement coming back. Understanding why claims get rejected and how to prevent common billing errors is essential for any transportation provider serious about profitability.
What makes this particularly frustrating is that most denials are entirely preventable. The Centers for Medicare & Medicaid Services (CMS) and state Medicaid programs don’t deny claims because they want to. They deny claims because providers submit incomplete documentation, miss deadlines, or fail to match transport levels to documented medical necessity. Understanding how the prior authorization for medical transportation system works—and building workflows that prevent failures before they happen—is the difference between a profitable NEMT operation and one that bleeds money on every trip.
This guide covers everything transportation providers, billing staff, and healthcare facility coordinators need to know about Medicaid NEMT prior authorization in 2026. You’ll learn when PA is required, what documentation you need, how to navigate state-specific requirements, and how to build systems that achieve first-pass approval rates above 90%. Whether you’re operating wheelchair vans in Texas, stretcher transports in California, or ambulance services across multiple states, the principles here apply to your operation.
The regulatory landscape is shifting. CMS finalized rules requiring 7-day standard decisions and 72-hour expedited reviews, while states continue tightening their utilization controls. Brokers like ModivCare, MTM, and Veyo now process the majority of Medicaid NEMT authorizations, each with their own portals, documentation standards, and approval timelines. If you’re exploring whether medical transportation is a profitable business venture, mastering prior authorization is non-negotiable for success.
What Is NEMT Prior Authorization?
Definition and Core Purpose
NEMT prior authorization is the mandatory pre-service approval process that verifies a patient’s medical transportation is covered, medically necessary, and appropriate for the requested transport level. Before a provider can bill Medicaid, Medicare, or managed care for non-emergency medical transportation, the payer must confirm that the trip meets specific clinical and administrative criteria.
Unlike prior authorization for clinical services like surgeries or imaging studies, NEMT PA focuses on whether the patient can safely use alternative transportation. The fundamental question isn’t “Does this patient need medical care?”—it’s “Does this patient’s medical condition prevent them from getting to that care through normal means?” A dialysis patient who can walk independently doesn’t automatically qualify for wheelchair transport. A patient recovering from knee surgery might need stretcher transport for the first week but ambulatory transport by week three.
The regulatory foundation for NEMT authorization comes from 42 CFR § 431.53, which requires state Medicaid agencies to assure transportation to and from medical services. According to the Code of Federal Regulations on eCFR.gov, states must ensure that necessary transportation is available for Medicaid recipients. Section 1902(a)(4) of the Social Security Act gives states the authority to implement utilization controls—including prior authorization—to ensure efficient program administration. For Medicare, the Repetitive Scheduled Non-Emergent Ambulance Transport (RSNAT) program establishes PA requirements for patients requiring frequent ambulance services.
Prior Authorization vs. Related Concepts
Confusion between prior authorization and related terms causes significant billing problems. Understanding the distinctions prevents submitting the wrong requests through the wrong channels.
| Term | What It Does | NEMT Application |
|---|---|---|
| Prior Authorization | Approves specific service based on medical necessity review | Required before non-emergency ambulance, stretcher, and certain wheelchair transports |
| Pre-certification | Confirms coverage exists but doesn’t evaluate medical need | Verifies transport benefit is active; doesn’t replace PA requirement |
| Prior Notification | Alerts payer of upcoming service; no approval needed | Some states require notification for routine trips without full PA |
| Eligibility Verification | Confirms member has active coverage | EDI 270/271 check; must happen before PA but doesn’t replace it |

What NEMT Prior Authorization Verifies
When payers process a prior authorization request, they evaluate multiple criteria. Understanding what they’re looking for helps you build requests that get approved on the first submission.
Medical necessity criteria: Can the patient physically use personal transportation, public transit, or a lower-acuity transport mode? Documentation must establish that the patient’s condition creates a genuine barrier to self-transport.
Transport level appropriateness: Does the clinical presentation justify the requested mode? Requesting ambulance transport for a patient who can safely use a wheelchair van triggers denials and may trigger fraud investigations.
Member eligibility: Is the patient actively enrolled in Medicaid, Medicare, or the managed care plan covering the transport? Eligibility gaps—even single days—result in automatic denials.
Provider qualification: Is the transportation provider enrolled with the payer, credentialed appropriately, and contracted to provide the requested service type?
Destination appropriateness: Is the patient traveling to a covered medical service? Transport to non-medical destinations—even if the patient has mobility limitations—isn’t covered.
Who Bears Responsibility for Obtaining PA
The NEMT provider or contracted transportation broker holds primary responsibility for obtaining prior authorization. This differs from clinical healthcare, where the ordering physician or treating facility often initiates PA requests. In medical transportation, the driver picks up a patient and completes a trip—if no authorization exists, the provider absorbs the full cost.
Physicians play a supporting role by completing Physician Certification Statements (PCS) that document medical necessity, but they don’t submit the actual PA request. Healthcare facilities schedule transports and provide clinical documentation, but ultimate responsibility falls on the transport provider. When PA is missing and a claim is denied under code CO-197, the transport company—not the hospital, not the physician—loses the revenue.
This responsibility structure means NEMT companies must build internal systems to verify PA exists before dispatch. Relying on facilities to “handle the paperwork” guarantees losses. The successful provider assumes nothing is authorized until their own staff confirms it. For a deeper understanding of the complete revenue cycle, our comprehensive guide to medical transportation billing and coding covers every aspect from enrollment to payment posting.
When Is Prior Authorization Required for NEMT?
Not every medical transport requires prior authorization. Understanding the triggers—and the exceptions—prevents both unnecessary administrative work and devastating claim denials. Requirements vary by transport type, distance, frequency, payer, and state, creating a matrix of rules that billing staff must navigate daily.
Transport Types That Always Require Prior Authorization
Certain transport categories trigger mandatory PA regardless of state, distance, or frequency. These high-acuity services carry significant cost exposure for payers, making upfront authorization non-negotiable.
Non-emergency BLS and ALS ambulance transport: Any scheduled ambulance service—Basic Life Support (A0428) or Advanced Life Support (A0426)—requires PA under both Medicare RSNAT rules and virtually all state Medicaid programs. The high cost per trip and historical fraud patterns make ambulance PA universal.
Air ambulance transport: Fixed-wing (A0430) and rotary-wing (A0431) air ambulance requires PA in every jurisdiction. These services cost thousands per flight, demanding extensive medical necessity documentation including time-critical treatment needs and geographic isolation factors.
Stretcher and litter van transport: Patients requiring supine positioning (T2005) must have clinical documentation establishing why seated transport is medically contraindicated. Stretcher requests without clear bed-confinement documentation face high denial rates.
Out-of-state transportation: Crossing state lines adds complexity around provider enrollment, rate agreements, and medical necessity justification. Why can’t the patient receive equivalent care in-state? PA review addresses this question.
Bariatric and specialty transport: Patients requiring equipment rated above standard capacity (typically 350+ pounds) need documentation of weight, standard vehicle limitations, and specialized equipment requirements.
Conditional PA Triggers: Thresholds and Limits
Some transport types require PA only when specific thresholds are crossed. These conditional triggers vary significantly by state and payer, requiring providers to track multiple rule sets simultaneously.
Mileage thresholds: Indiana requires PA for any trip exceeding 50 miles. North Dakota triggers wheelchair van review after 15 miles. Ohio flags trips beyond 75 miles. Texas MCOs scrutinize transports over 150 miles. These distance limits exist because long-haul trips cost more and create opportunities for unnecessary utilization. For current reimbursement rates and fee schedules across all 50 states, understanding rate structures helps with financial planning.
Frequency thresholds: Medicare’s RSNAT program kicks in after 40 round trips (or 80 one-way trips) within a 60-day period. Once this threshold is crossed, every subsequent ambulance transport requires prior authorization with a Physician Certification Statement. States may impose their own frequency limits for wheelchair and sedan services.
Mode upgrade requests: When a patient’s condition changes and a higher transport level is needed—wheelchair to stretcher, stretcher to BLS—the upgrade requires fresh PA with updated clinical justification. Previous authorizations don’t automatically extend to higher-acuity modes.
When Prior Authorization Is NOT Required
Not every trip needs PA, and submitting unnecessary requests wastes staff time while potentially delaying service. Knowing the exceptions matters as much as knowing the requirements.
Emergency ambulance transport: True 911 emergencies bypass prior authorization entirely. The distinction matters: a non-emergency ambulance scheduled for Tuesday requires PA; an ambulance responding to acute chest pain on Tuesday does not.
Basic ambulatory transport: Many states don’t require PA for sedan or standard van transport when the patient can walk independently. These low-cost services often operate under broker auto-approval or simple eligibility verification.
Pre-approved recurring services: Once a standing order PA is approved for recurring transport (dialysis, chemotherapy), individual trips within the authorization period don’t require separate requests. The initial PA covers the series.
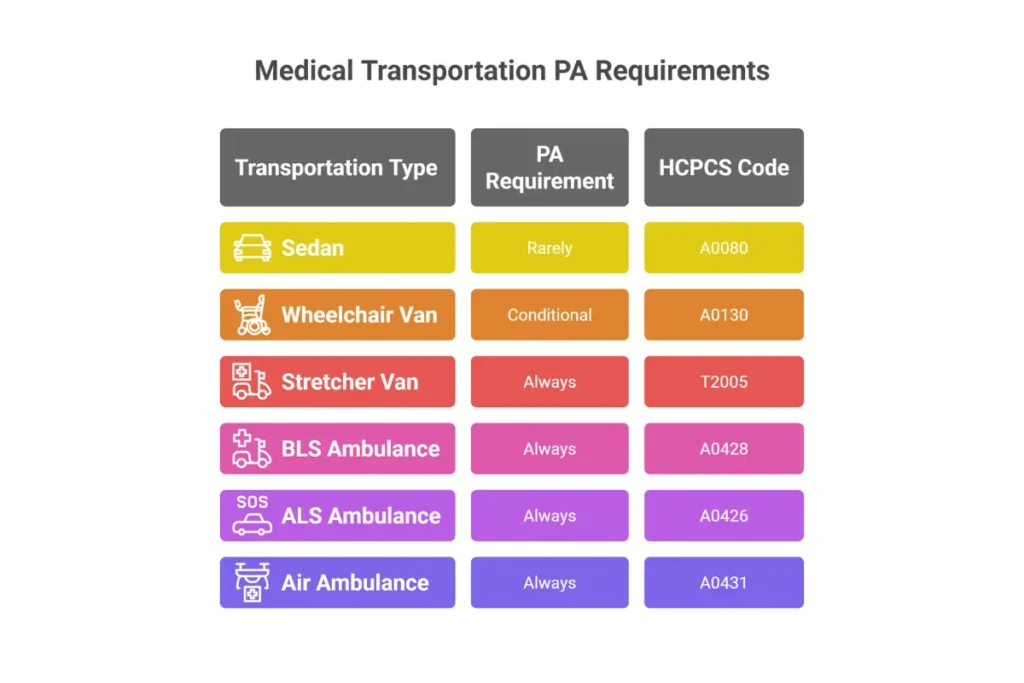
Prior Authorization Requirements by Transport Type
| Transport Mode | HCPCS Code | PA Required? | Key Documentation |
|---|---|---|---|
| Ambulatory/Sedan | A0080 | Rarely | Eligibility verification; destination confirmation |
| Wheelchair Van | A0130 | Conditional | PCS for mobility limitation; distance triggers vary |
| Stretcher Van | T2005 | Always | PCS documenting bed confinement or supine requirement |
| BLS Ambulance | A0428 | Always | PCS + medical records; bed confinement criteria |
| ALS Ambulance | A0426 | Always | PCS + clinical justification for ALS-level monitoring |
| Air Ambulance (Fixed) | A0430 | Always | Flight physician certification; time/distance analysis |
| Air Ambulance (Rotary) | A0431 | Always | Flight physician certification; terrain/access factors |
| Bariatric Transport | Varies | Always | Weight documentation; equipment specifications |
Federal NEMT Prior Authorization Requirements
Federal regulations establish the baseline framework for NEMT prior authorization, but they grant states significant flexibility in implementation. Understanding where federal requirements end and state discretion begins helps providers navigate compliance across multiple jurisdictions.
42 CFR § 431.53: The Transportation Assurance Mandate
The Code of Federal Regulations at 42 CFR § 431.53 requires state Medicaid agencies to “assure necessary transportation” for recipients to and from medical providers. This mandate doesn’t prescribe specific prior authorization procedures—it establishes that states must ensure transportation access while giving them authority to implement controls.
Prior authorization serves as the primary mechanism states use to fulfill this assurance while controlling costs. The regulation’s language—”necessary transportation”—creates the medical necessity standard that PA requests must meet. If transport isn’t medically necessary, states have no obligation to provide it.
Social Security Act Section 1902(a)(4): Administrative Efficiency
Section 1902(a)(4) of the Social Security Act requires states to administer their Medicaid programs efficiently and effectively. This provision provides the legal basis for utilization controls including prior authorization, transportation brokers, and managed care arrangements. When states contract with brokers like ModivCare or MTM to manage NEMT, they’re exercising authority under this section.
42 CFR § 438.210: Managed Care PA Requirements
For NEMT services delivered through Managed Care Organizations (MCOs), 42 CFR § 438.210 establishes additional requirements. MCOs must use clinical criteria for PA decisions, provide timely determinations, and issue proper denial notices. These regulations standardize how managed care plans process authorization requests, creating more predictable timelines than traditional fee-for-service Medicaid.
Medicare RSNAT: The National PA Model
The Medicare Repetitive Scheduled Non-Emergent Ambulance Transport (RSNAT) program operates nationwide as of 2024, establishing uniform prior authorization requirements for patients requiring frequent ambulance services. RSNAT applies when a beneficiary receives 40 or more round trips (or 80 one-way trips) within a 60-day period for scheduled, non-emergency ambulance transport.
The program emerged from CMS pilot projects demonstrating that prior authorization could dramatically reduce improper payments. According to CMS data on the RSNAT program, pilot areas showed cost reductions of 67% and improper trip reductions of 58%. Based on these results, CMS expanded RSNAT nationally, making it the most significant federal NEMT PA requirement.
RSNAT PA requirements include:
- Physician Certification Statement signed before transport
- Medical records documenting patient’s inability to self-transport
- Bed confinement status or equivalent mobility impairment
- Submission through Medicare Administrative Contractor (MAC) portal
Federal Medical Necessity Standards
CMS defines medical necessity for NEMT based on the patient’s functional ability to use alternative transportation. The standard isn’t whether the patient is sick or has a medical appointment—it’s whether their condition prevents safe use of personal vehicles, public transit, or lower-acuity transport modes.
Key medical necessity criteria:
- Patient is physically unable to transport independently
- No safe alternative transportation exists
- Bed confinement or equivalent mobility impairment is documented
- Requested transport mode matches clinical presentation
CMS 2024-2026 Policy Directives
Recent CMS rulemaking under CMS-0057-F establishes new standards affecting NEMT prior authorization across Medicare and Medicaid. These rules push the industry toward electronic submission and standardized timelines.
Mandated decision timelines: 7 calendar days for standard PA requests; 72 hours for expedited/urgent requests
Electronic submission requirements: FHIR-based APIs for PA submission and status checking are being phased in
Interoperability standards: Health plans must share PA information electronically with providers
Transparency requirements: Denial reasons must be specific and actionable
State-Specific Prior Authorization Requirements
While federal regulations create the framework, state Medicaid agencies implement the specific rules that govern daily operations. Each state determines its own PA thresholds, required forms, submission portals, and processing timelines. Multi-state providers must track dozens of distinct requirements, making state-level knowledge essential for compliance.

Texas
Texas operates its NEMT program through the Texas Medicaid & Healthcare Partnership (TMHP) and the Medical Transportation Program (MTP). Prior authorization is required for all non-emergency ambulance transport, air ambulance, and out-of-state trips. Ambulatory trips typically route through brokers without formal PA.
Primary PA form: Form F00045 (Nonemergency Ambulance Prior Authorization Request)
Supporting form: Form 4214 (Medical Necessity)
Submission methods: TMHP Provider Portal (preferred), fax to 512-514-4205, or mail
Typical processing: 3 business days for standard requests; MCO-managed transports follow plan-specific timelines
California
California’s Medi-Cal program presents unique challenges due to county-level variations. The Department of Health Care Services (DHCS) sets statewide policy, but Geographic Managed Care (GMC) and Plan Healthcare (PHC) plans implement their own PA procedures. This creates a patchwork where requirements differ between Los Angeles, San Diego, and Northern California regions.
Primary PA form: Treatment Authorization Request (TAR)
Supporting form: DHCS Form 6182 (Certificate of Medical Necessity) varies by plan
Submission methods: Medi-Cal Provider Portal, GMC/PHC plan portals, fax to 833-701-0051
Typical processing: 24-48 hours urgent; 5-7 business days standard
Key requirement: TAR required for wheelchair, stretcher, and specialized transport; county codes must be accurate
Pennsylvania
Pennsylvania’s Medical Assistance Transportation Program (MATP) operates through county-level administration rather than a statewide broker. This decentralized model means PA procedures vary between Southeast PA, Northwest PA, and other regions. Providers must identify the correct county MATP office for each patient.
Primary PA documentation: Physician Certification Statement (PCS)
Submission methods: PROMISe™ Provider Portal, phone, fax, or mail by county
Typical processing: 72 hours urgent; up to 10 business days standard
Key requirement: PA required for stretcher, wheelchair, and non-ambulatory modes
Indiana
Indiana Health Coverage Programs (IHCP) contracts with Verida as the statewide NEMT broker. Verida manages authorization through its HealthSherpa portal, creating a centralized system that simplifies compliance compared to county-based models.
Primary PA form: Form 55427 (Certificate of Medical Necessity)
Submission methods: Verida HealthSherpa portal (primary), IN.gov downloads
Typical processing: 24-48 hours
PA triggers: Mileage exceeding 50 miles, ALS/BLS ambulance, out-of-state trips, air ambulance
New York
New York Medicaid operates through eMedNY statewide, with New York City Human Resources Administration (HRA) managing authorization for the NYC region separately. The state’s history with transportation fraud has resulted in strict documentation requirements, particularly for ambulette services.
Primary PA form: Form 389701 (Authorization Request for Transportation Services)
Supporting form: 2015 Medical Necessity Form (plan-dependent)
Submission methods: eMedNY portal, NYC HRA systems, MCO portals for managed care
Typical processing: 24 hours urgent; 3-5 business days standard
Key requirement: PA required for ambulettes and specialty wheelchair due to fraud-control guidelines
State Comparison Matrix
| State | Mileage Threshold | Primary Submission | Avg Timeline | Key Form |
|---|---|---|---|---|
| Texas | >150 mi (MCO review) | TMHP Portal | 3 business days | F00045 |
| California | Mode-based (not distance) | Medi-Cal/Plan Portals | 5-7 days | TAR |
| Pennsylvania | Mode-based | PROMISe™/County | Up to 10 days | PCS |
| Indiana | >50 miles | Verida Portal | 24-48 hours | Form 55427 |
| New York | Mode-based | eMedNY/HRA | 3-5 days | 389701 |
| Florida | >100 miles (varies) | MTM/MCO Portals | 7 days | PCS |
| Ohio | >75 miles | ODM/NET System | 7 days | ODM 03452 |
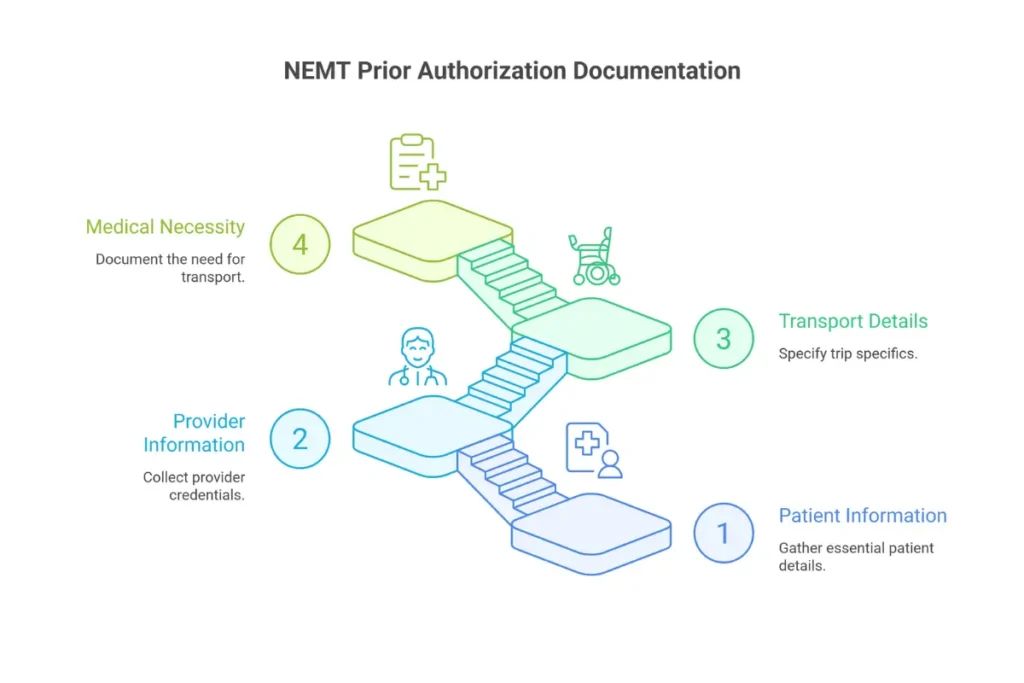
Required Documentation for NEMT Prior Authorization
Documentation failures cause more PA denials than any other factor. Missing fields, unsigned forms, and incomplete clinical justification trigger automatic rejections that delay service and cost staff hours to resolve. Building bulletproof documentation packets requires understanding exactly what each payer needs—and submitting it the first time.
Member Information Requirements
Every PA request begins with member identification. Errors in patient data create immediate rejections that could be avoided with basic verification procedures.
Essential member fields:
- Full legal name (matching Medicaid/Medicare enrollment exactly)
- Date of birth
- Medicaid ID, Medicare HICN/MBI, or MCO member number
- Current address (for pickup location verification)
- Phone number for contact
Provider Information Requirements
Provider credentialing issues cause denials that feel arbitrary but reflect enrollment gaps. If your company isn’t properly enrolled with the payer processing the PA, approval is impossible regardless of medical necessity.
Essential provider fields:
- National Provider Identifier (NPI)
- Taxonomy code matching service type
- State license number (if applicable)
- Medicaid/Medicare enrollment confirmation
- Broker contract status (for broker-managed states)
- Business address and contact information
Transport Information Requirements
Trip details must match across all submitted documents. Mismatches between the PA request, PCS, and eventual claim create audit triggers and potential fraud investigations.
Essential transport fields:
- Pickup address (origin)
- Destination address (medical facility)
- Date(s) of service
- Transport mode requested (ambulatory, wheelchair, stretcher, BLS, ALS)
- HCPCS code for the service (A0130, T2005, A0428, etc.)
- Estimated mileage (one-way and round-trip)
- Frequency and duration for recurring transport
Medical Necessity Documentation
Medical necessity documentation is where PA requests succeed or fail. Generic statements don’t work. Reviewers need specific clinical information that answers one question: Why can’t this patient use a lower-cost transport option?
Required clinical documentation:
- Signed Physician Certification Statement (PCS) with credentials
- ICD-10 diagnosis codes supporting the condition
- Functional narrative explaining why lower transport mode is unsafe
- Bed confinement status documentation (for ambulance/stretcher)
- Recent medical records supporting current condition
Common ICD-10 codes for NEMT authorization:
- N18.6 / Z99.2 — End-stage renal disease / Dialysis dependence
- Z51.11 / Z51.12 — Chemotherapy / Immunotherapy encounter
- G81.x / G82.x — Hemiplegia / Paraplegia
- I63.x — Cerebral infarction (stroke)
- S72.x — Hip fracture
- Z99.11 — Dependence on ventilator/oxygen
- Z74.01 — Bed confinement status
Supporting Clinical Documentation
Beyond the core requirements, attaching supporting documentation significantly increases approval rates, particularly for high-acuity transport levels or complex medical situations.
- Hospital discharge summaries (for post-acute transport)
- Dialysis center treatment schedules
- Chemotherapy/radiation treatment calendars
- Physical therapy/occupational therapy mobility assessments
- Wound care clinic notes (for pressure ulcer patients)
- Specialist letters affirming transport necessity
- Home health plan of care documentation
Complete Documentation Checklist
| Documentation Item | Status/Notes |
|---|---|
| ☐ Patient name, DOB, address | Must match enrollment exactly |
| ☐ Medicaid/Medicare ID number | Verify active status before submission |
| ☐ Eligibility verification (EDI 270/271) | Run 48 hours before service |
| ☐ Provider NPI and taxonomy | Confirm enrollment status current |
| ☐ Origin and destination addresses | Include ZIP codes; verify medical facility |
| ☐ Service date(s) and HCPCS code | Match code to transport mode |
| ☐ Mileage estimate | One-way and round-trip if applicable |
| ☐ ICD-10 diagnosis codes | Must support medical necessity narrative |
| ☐ PCS signed by authorized clinician | Signature date BEFORE first transport |
| ☐ Functional narrative/clinical notes | Explain WHY lower mode is unsafe |
| ☐ Bed confinement documentation | Required for ambulance/stretcher |
| ☐ Treatment schedule (if recurring) | Dialysis, chemo, radiation calendar |
| ☐ Supporting records attached | Discharge summary, PT/OT eval, specialist notes |
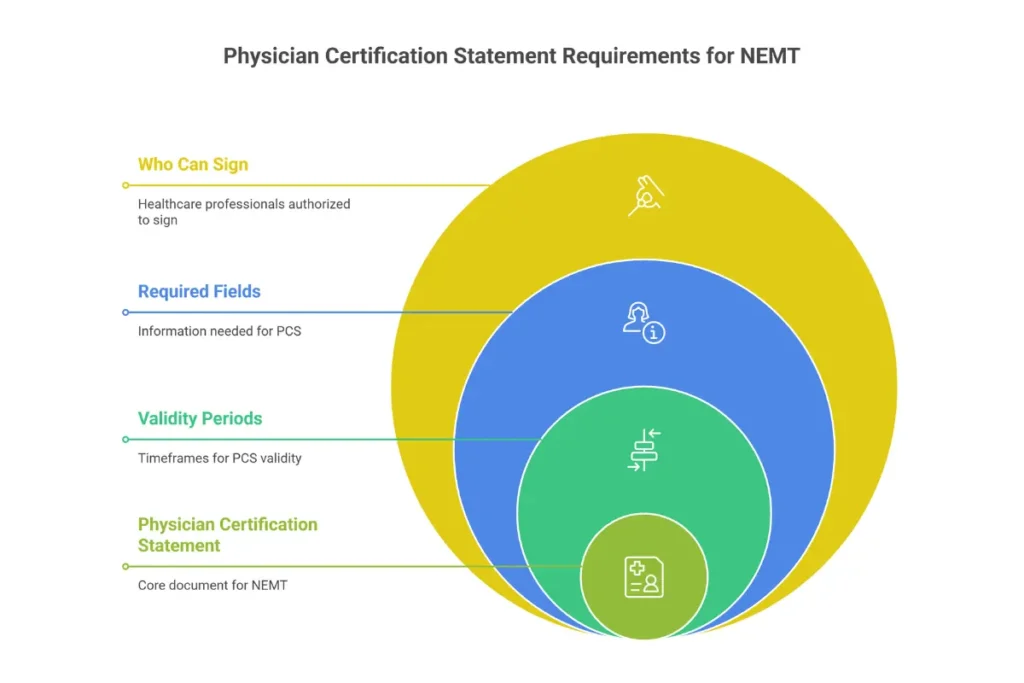
The Physician Certification Statement (PCS)
The Physician Certification Statement is the single most important document in NEMT prior authorization. Missing or defective PCS forms account for approximately 35% of all PA denials. Understanding PCS requirements—who can sign, what must be included, and how long certifications remain valid—directly impacts your approval rates and revenue.
What the PCS Certifies
A Physician Certification Statement is a signed medical document that verifies a patient’s medical condition prevents safe use of personal or public transportation, justifying the level of NEMT requested. The PCS doesn’t just confirm the patient is sick—it certifies that their specific condition creates transportation barriers that require medical transport.
The PCS certifies:
- Patient cannot safely use personal vehicle, taxi, or public transit
- Patient’s medical condition requires the requested transport level
- Lower transport modes would be medically inappropriate or unsafe
- For ambulance/stretcher: patient meets bed confinement criteria
Who Can Sign a PCS
Medicare and Medicaid programs accept PCS signatures from specified healthcare practitioners, though exact requirements vary by state. Using an unauthorized signer invalidates the entire certification, resulting in automatic denial.
Universally accepted signers:
- Physicians (MD, DO)
Generally accepted (Medicare and most states):
- Nurse Practitioners (NP)
- Physician Assistants (PA)
- Clinical Nurse Specialists (CNS)
State-variable (some Medicaid programs):
- Physical Therapists (for rehab-related transports)
- Licensed Clinical Social Workers (mental health transports)
- Treating specialists (nephrologists, oncologists)
Never accepted:
- Medical Assistants
- Non-treating clinicians (generic hospitalist for outpatient follow-up)
- Administrative staff
Required PCS Information Fields
Incomplete PCS forms trigger rejections before clinical review even begins. Every field matters, and missing data—even minor omissions—can invalidate the certification.
Mandatory PCS fields:
- Patient name, date of birth, and insurance ID
- Ordering clinician name, credentials (MD, DO, NP, PA), and NPI
- Treating provider specialty (if required by state)
- Origin and destination with medical necessity for both locations
- Transport type requested (ambulatory, wheelchair, stretcher, BLS/ALS)
- Bed confinement status (if applicable)
- ICD-10 codes supporting the medical condition
- Frequency and duration (one-time, weekly, recurring)
- Clinical reasoning narrative explaining why lower mode is unsafe
- Signature and date (signature date MUST be before first transport)
Bed Confinement Criteria
Ambulance and stretcher PA requests require documentation of bed confinement or equivalent functional limitation. CMS defines bed confinement not as “must stay in bed 24/7” but as clinical inability to safely use seated transport.
Bed confinement means the patient:
- Cannot rise from bed or chair safely without assistance
- Cannot ambulate independently
- Cannot transfer into a vehicle safely
Conditions commonly justifying bed confinement:
- Ventilator dependence
- Stage III-IV pressure ulcers
- Post-stroke paresis/paralysis
- Cardiac instability requiring monitoring
- Dialysis complications with severe weakness
PCS Validity Periods
PCS certifications don’t last forever. Validity periods vary by payer and transport frequency, and expired certifications result in automatic denials even if the patient’s condition hasn’t changed.
| Program/Payer | Recurring/Chronic | Acute/Temporary |
|---|---|---|
| Medicare (general) | 60 days maximum | 30 days or single trip |
| Medicare RSNAT | Standing order; reviewed every 21 days | N/A |
| Medicaid (varies by state) | 6-12 months depending on state | Duration of Plan of Care |
| MCOs/Managed Medicaid | 90 days typical | 7-14 days |
Common PCS Errors Causing Denials
Knowing what causes PCS rejections helps you prevent them. These errors appear repeatedly in denial data and are entirely avoidable with proper quality control.
Signature dated after first transport: The PCS must be signed before the first trip. A PCS signed on Tuesday for a Monday transport is invalid.
Missing or unclear credentials: “Dr. Smith” without MD/DO/NP designation creates ambiguity that triggers rejection.
Generic medical necessity language: “Patient needs wheelchair” fails. “Patient’s diabetic neuropathy causes severe balance impairment, creating fall risk during transfers” succeeds.
ICD-10 codes unsupported by narrative: Listing a diagnosis code without explaining how it affects transport ability invites denial.
Expired certification used: Submitting a PCS from March for an August transport when validity has lapsed.
Wrong transport level documented: PCS certifies wheelchair need but provider requests ambulance.
Step-by-Step Prior Authorization Process
The PA workflow follows a logical sequence, but skipping steps or executing them out of order creates failures that could have been prevented. This process applies across payers, with variations in submission methods and timelines by state and broker.
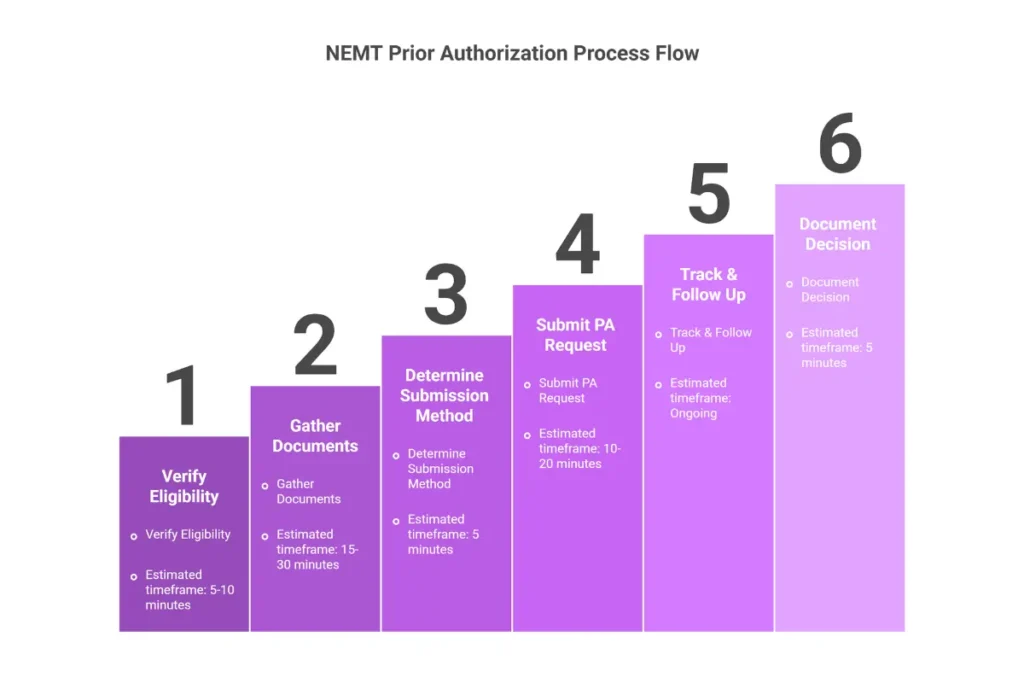
Step 1: Verify Member Eligibility
Before gathering documentation or completing forms, confirm the patient has active coverage. Run EDI 270/271 eligibility verification at least 48 hours before the scheduled transport. This check confirms:
- Active Medicaid/Medicare enrollment
- Benefit limits and trip caps
- PA flags (whether the service requires authorization)
- Covered transport modes
- Broker assignment (who processes the PA)
Eligibility gaps cause PR-19 denials that no amount of medical necessity documentation can overcome. A patient who was covered last month but lost benefits this month isn’t eligible—period.
Step 2: Gather Required Documentation
With eligibility confirmed, collect all necessary documentation before contacting the payer. Incomplete submissions create delays, multiple touchpoints, and increased denial risk.
- Use the documentation checklist from Section 6 to ensure nothing is missing
- Obtain a signed PCS from the ordering physician
- Collect medical records supporting the current condition
- Verify trip details match across all documents
- Confirm provider enrollment is current
Step 3: Determine Submission Method
Different payers require different submission channels. Using the wrong method delays processing or results in lost requests.
Electronic portal submission (preferred for speed):
- TMHP Portal for Texas
- Medi-Cal Provider Portal for California
- Verida HealthSherpa for Indiana
- eMedNY for New York
EDI 278 electronic PA: Submit through brokers like ModivCare, MTM, and Veyo
Fax submission: Available in most states as backup
Phone submission: Accepted for urgent requests in Pennsylvania and Florida
Step 4: Complete and Submit PA Request
With documentation in hand and submission method identified, complete the appropriate PA form for your state/payer. Double-check all fields before submission.
- Verify member information matches enrollment records
- Confirm provider NPI and enrollment status
- Attach PCS with valid signature and date
- Include all supporting documentation
- Submit through the appropriate channel
- Save confirmation number
Step 5: Track and Follow Up
PA requests don’t manage themselves. Active tracking prevents authorizations from stalling in review queues.
- Check status on Day 2-3 after submission
- Escalate pended requests after Day 5-7 if no decision
- Respond to Requests for Information (RFI) within 24 hours
- Document all communications and reference numbers
Step 6: Receive and Document Decision
When the payer issues a decision, document the outcome immediately.
For approvals: Record the authorization number, approved units/trips, validity period, and any service limitations. Link the auth number to driver manifests, trip sheets, and billing records.
For denials: Document the denial reason code, appeal deadline, and required corrective action.
Processing Timeline Expectations
| Request Type | Standard | Expedited | Best Method |
|---|---|---|---|
| Medicaid FFS | 2-5 business days | 24-72 hours | Portal |
| Managed Care/MCO | 2-5 days | 72 hours | Portal/EDI |
| Indiana (Verida) | 24-48 hours | Same day | Portal |
| Medicare RSNAT | ~7 days | 72 hours | MAC Portal |
| Broker (ModivCare/MTM) | 24-72 hours | Same day | API/Portal |
Urgent and Emergent PA Procedures
Life-threatening non-emergent situations and time-sensitive treatments qualify for expedited review. Most payers offer same-day or next-day decisions for urgent requests when documented appropriately.
Situations qualifying for expedited PA:
- Dialysis patients at risk of missed treatment
- Chemotherapy patients with scheduled infusions
- Patients with deteriorating conditions requiring specialty care
- Hospital discharges requiring immediate transport
Retroactive authorization is available in limited circumstances, typically within a 15-30 day window depending on state rules. True emergencies bypass PA entirely—a 911 response doesn’t require pre-authorization.
Prior Authorization Requirements by Transport Type
Each transport modality carries distinct PA requirements, documentation standards, and medical necessity criteria. Understanding the specific requirements for your service types prevents mismatched requests and reduces denial rates.
Wheelchair Van Transport (A0130)
Wheelchair van transport serves patients who cannot safely use standard vehicles due to mobility limitations but don’t require medical monitoring during transport. PA requirements vary significantly by state and distance.
PA trigger factors: Distance exceeding state threshold (Indiana: >50 miles), frequency (recurring trips), and lack of lower-cost alternatives.
Required documentation: PCS citing functional mobility limitations, ICD-10 codes demonstrating impairment (M62.3 muscle weakness, R26.2 difficulty walking), trip mileage estimate, and attestation that public transit is not viable.
Top denial reason: “Patient can ambulate with assistance”—documentation must show why ambulation with assistance doesn’t make sedan transport safe.
Stretcher/Litter Van Transport (T2005)
Stretcher transport is for patients who must remain supine during transport but don’t require medical monitoring or intervention. PA is always required given the higher cost and fraud history in this category.
Clinical standards: Patient must remain supine, risk of deterioration if positioned upright, PCS must specifically state stretcher requirement.
Required documentation: Bed confinement justification, mobility/balance assessment, recent medical notes documenting current condition.
Non-Emergency BLS Ambulance (A0428)
Basic Life Support ambulance transport provides medical monitoring and basic interventions during scheduled transports. PA is mandatory for both Medicare (after RSNAT threshold) and state Medicaid programs.
Medical necessity criteria: Patient’s illness/injury prevents use of lower transport levels, bed confinement as defined by CMS, need for medical observation during transport.
Required documentation: PCS with bed confinement certification, progress notes documenting current status, origin/destination medical necessity.
Non-Emergency ALS Ambulance (A0426)
Advanced Life Support ambulance transport provides higher-level interventions and monitoring when BLS capabilities are insufficient. Approval requires demonstrating why BLS isn’t adequate.
Trigger criteria for ALS: Cardiac monitoring required, IV medications during transport, ventilator management, unstable vital signs.
Required documentation: PCS specifying advanced care needs, ECG reports or cardiac documentation, clinical justification for ALS-level monitoring.
Air Ambulance (A0430/A0431)
Fixed-wing (A0430) and rotary-wing (A0431) air ambulance transport requires universal PA given costs of thousands per flight. Documentation must establish why ground transport is inadequate.
Approval criteria: Time-critical treatment that ground transport cannot meet, geographic isolation making ground transport impractical, patient condition that cannot tolerate extended ground transport time.
Required documentation: Flight physician certification, time/distance comparison with ground alternative, weather or terrain documentation if applicable.
Bariatric and Specialty Transport
Bariatric transport serves patients requiring equipment rated above standard capacity. PA is required to document equipment needs and justify the specialized service.
Bariatric requirements: Vehicle capacity typically >750 pounds, scaled weight documentation, medical necessity statement that standard van is unsafe.
Neonatal/Pediatric specialty: Life-support equipment requirements, neonatal team orders, incubator or temperature-control documentation.
Prior Authorization for Recurring and Repetitive Transport
Patients with ongoing treatment needs—dialysis, chemotherapy, radiation, wound care—require repeated transports over extended periods. Recurring PA structures reduce administrative burden by authorizing multiple trips under a single approval, but they require careful management to avoid coverage gaps.
Medicare RSNAT (Repetitive Scheduled Non-Emergent Ambulance Transport)
RSNAT applies when a Medicare beneficiary receives 40 or more round trips (or 80 one-way trips) within a 60-day period for scheduled, non-emergency ambulance transport. Once this threshold is crossed, every subsequent ambulance transport requires prior authorization.
Common RSNAT services: Dialysis (typically 3x weekly), wound care, radiation therapy, infusion treatments.
RSNAT requirements: PCS form submitted before transport, medical records proving inability to self-transport, documentation of bed confinement or equivalent limitation.
Dialysis Transportation Standing Orders
Dialysis patients represent the largest category of recurring NEMT users. Most payers accept standing order PA that covers multiple trips over 60-90 days, reducing per-trip authorization burden.
Initial approval period: 60-90 days typical; some states allow up to 365 days for stable ESRD patients.
Documentation required: ESRD documentation, dialysis center treatment schedule, ICD-10 codes (N18.6, Z99.2), PCS certifying ongoing transport need.
Renewal timing: Submit renewal 14-30 days before expiration to avoid coverage gaps.
Oncology Transport (Chemotherapy and Radiation)
Cancer treatment transport follows treatment schedules that can span weeks or months. PA requests should align with treatment protocols, typically in 6-week blocks matching radiation or chemotherapy cycles.
Relevant ICD-10 codes: Z51.11 (chemotherapy encounter), Z51.12 (immunotherapy/radiation encounter).
PA duration: Up to 180 days depending on treatment plan; resubmission required if treatment regimen changes.
Standing Order Limits and Renewals
Standing orders authorize multiple trips on a single PA, but validity periods vary by payer and patient condition.
Typical standing order limits:
- Acute conditions: 60-90 days
- Chronic conditions: Up to 365 days
- California: 90-day acute cap
- Texas: Duration follows treatment plan
Renewal requirements:
- Updated PCS with current clinical status
- Physician progress note confirming ongoing need
- Labs or imaging supporting continued medical necessity
Managing PA Expiration and Continuity
Expired PAs cause immediate denials for trips that would otherwise be covered. Proactive expiration management prevents revenue loss and service disruption.
Best practices for continuity:
- Log all PA expiration dates in scheduling/dispatch system
- Set alerts 30 days before expiration for renewal submission
- Submit renewal 14-30 days prior to expiration
- Notify payers of treatment changes within 72 hours
- Maintain documentation for retroactive PA requests (available within 30-60 days in most states)
Common Prior Authorization Denials and Prevention
The NEMT industry faces denial rates of 15-25%, with preventable documentation and process failures causing the majority of lost revenue. Understanding why denials occur—and building systems to prevent them—is the most direct path to improved financial performance. For a complete breakdown of rejection codes and how to resolve each one, understanding denial patterns is essential for revenue protection.
Top Denial Reasons and Prevention Strategies
Each denial reason has a specific prevention strategy. Implementing these strategies systematically reduces denial rates from 20%+ to under 10%.
| Denial Reason | Code/Frequency | Prevention Strategy |
|---|---|---|
| Missing prior authorization | CO-197 (~35%) | Verify PA exists before dispatch |
| Patient eligibility inactive | PR-19 (~15%) | Run 270/271 check 48 hours prior |
| PCS missing or invalid | ~20% | Checklist before submission; verify date |
| Medical necessity not established | ~15% | Detailed functional narrative in PCS |
| Incorrect transport level | ~8% | Match mode to documented condition |
| Provider enrollment issues | ~5% | Verify NPI/enrollment quarterly |
| Timely filing exceeded | ~3% | Submit within 30 days of service |
| Duplicate submission | ~2% | Track submission confirmation numbers |
Financial Impact of PA Denials
Each denied trip costs more than the lost reimbursement. Factor in staff time for rework, appeal processing, and opportunity cost, and the true cost of denial becomes clear.
Cost breakdown per denial:
- Lost revenue per trip: $100-$300
- Administrative rework: $25-$125
- Appeal processing: $50-$150 in staff time
- Total exposure per denial: $175-$675
For a provider handling 500 trips per month with a 20% denial rate, that’s 100 denied trips creating $17,500-$67,500 in monthly exposure. Annual losses can reach $75,000-$150,000 or more for mid-size operations.
Denial Prevention Checklist
Use this checklist before every PA submission to catch preventable errors:
☐ Eligibility verified within 48 hours (EDI 270/271)
☐ PA requirement confirmed for this transport type/payer
☐ PCS signed by authorized clinician with credentials visible
☐ PCS signature date is BEFORE first service date
☐ ICD-10 codes match functional narrative
☐ Transport level matches documented medical need
☐ Provider NPI and enrollment current
☐ Origin and destination addresses complete with ZIP
☐ Supporting documentation attached
☐ Submission confirmation saved with reference number
Appealing Prior Authorization Denials
When denials occur despite best efforts, appeals provide a path to recovery. Industry data shows 40-70% of appeals succeed when properly documented, yet 65% of denials go unappealed—representing significant lost revenue from winnable cases.
Appeal Rights and Timeframes
Federal and state regulations establish appeal rights, but timeframes vary significantly by payer type. Missing deadlines forfeits appeal rights entirely.
Standard appeal filing deadlines:
- Medicaid: 30-60 days from denial notice (state-specific)
- Medicare: 120 days from initial determination
- MCOs: 30-45 days typical (plan-specific)
- Indiana: 45 days
The Appeal Process
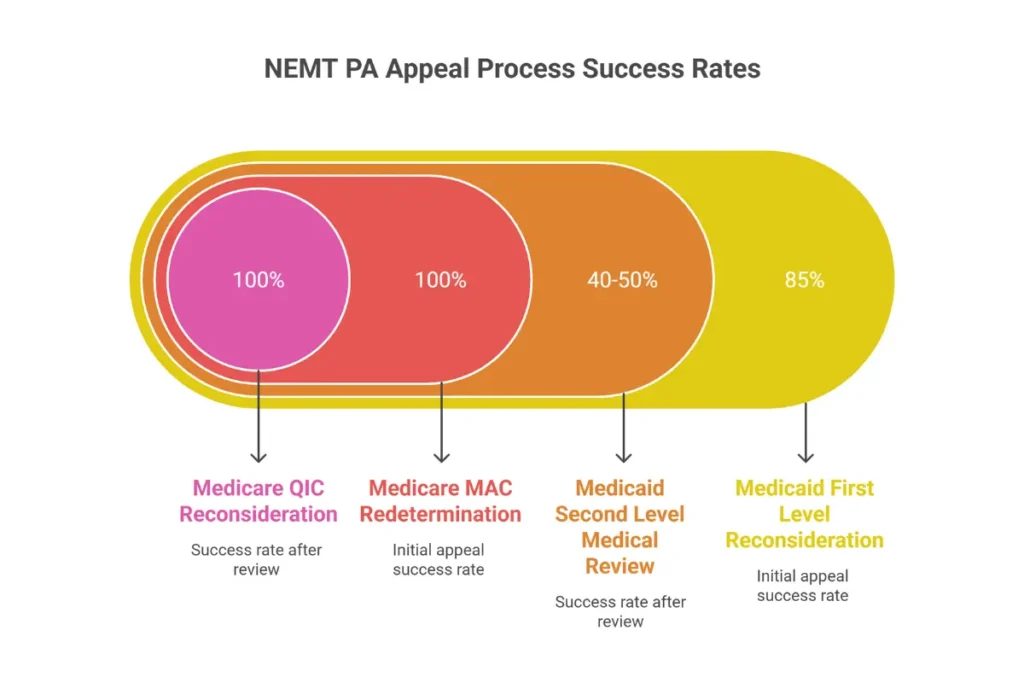
Appeals proceed through defined levels, with different success rates and processing times at each stage.
First-level reconsideration: Internal review by the payer. Most successful when denial resulted from administrative/documentation errors (85% overturn rate). Submit corrected documentation, updated PCS, and explanation of error.
Second-level medical review: Clinical review of medical necessity disputes. Success rate 40-50%. Requires physician letter, additional medical records, and clinical justification.
Medicaid Fair Hearing: Administrative hearing governed by 42 CFR § 431.220-250. For Medicaid denials not resolved through plan appeals.
Medicare 5-Level Hierarchy: MAC redetermination → QIC reconsideration → ALJ hearing → Medicare Appeals Council → Federal Court.
Peer-to-Peer Review
Peer-to-peer (P2P) review provides direct physician-to-physician discussion of medical necessity disputes. This process achieves 50-65% overturn rates and should be requested for stretcher, ambulance, and recurring transport denials.
Preparing for P2P:
- Have ordering physician available for scheduled call
- Prepare PCS and relevant medical records for reference
- Document specific safety concerns for lower transport modes
- Be prepared to explain why patient’s condition requires the requested level
Documentation for Successful Appeals
Appeals succeed or fail based on documentation quality. Submit everything needed to overturn the specific denial reason.
Standard appeal documentation:
- Original denial letter with reference number
- Corrected or updated PCS addressing denial reason
- Additional medical records not previously submitted
- Physician letter explaining medical necessity
- Response to specific denial reason with supporting evidence
- Citation to relevant CMS or state policy (42 CFR § 431.53)
Prior Authorization in Managed Care and Broker Systems
The majority of Medicaid NEMT now flows through managed care organizations (MCOs) and transportation brokers rather than traditional fee-for-service arrangements. These intermediaries create both efficiencies and complications for prior authorization, with each broker maintaining distinct portals, forms, and processing requirements.
How MCO PA Differs from Fee-for-Service
MCOs operate under 42 CFR § 438.210, which standardizes decision timelines and clinical criteria requirements. This creates more predictable processing but often increases documentation burden compared to traditional Medicaid.
| Requirement | MCOs (2026) | Traditional FFS |
|---|---|---|
| Standard decision | ≤7 calendar days | 5-14 days (state variable) |
| Expedited decision | 72 hours | Rarely defined |
| Submission portal | Broker/MCO portal | State Medicaid system |
| Documentation | PCS + care plan + ICD-10 | PCS or eligibility only |
Major Transportation Broker PA Processes
In 2026, brokers operate as clinical logic platforms with distinct processes. Understanding each broker’s requirements prevents submission errors and delays.
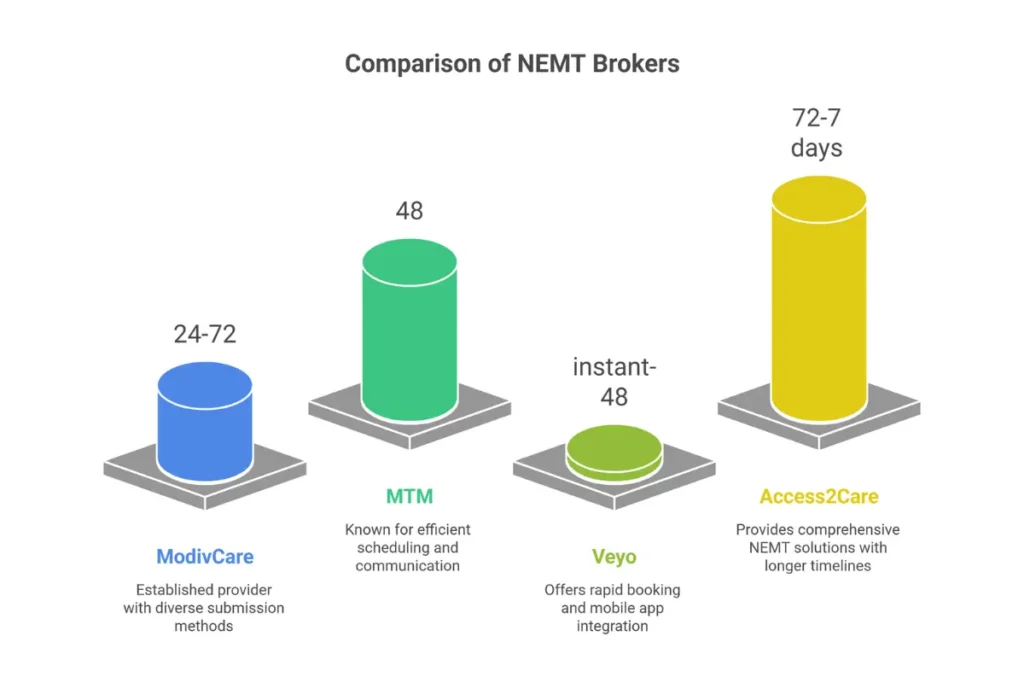
| Broker | Submission Method | Avg Timeline | Core Requirements |
|---|---|---|---|
| ModivCare | MODEM portal, API, phone | 24-72 hours | PCS, trip details, ICD-10, GPS match |
| MTM | Portal, EDI 278, phone | 48 hours | PCS mandatory for wheelchair/stretcher |
| Veyo | Mobile app + dispatch plugin | Instant-48 hrs | PCS when risk flags trigger |
| Access2Care | A2C provider portal | 72 hrs-7 days | State-specific form completion |
MCO Delegation Models
States and plans apply different delegation structures that determine who holds final PA authority:
Full delegation: Broker controls medical necessity per MCO rulebook. Faster decisions but harder to appeal.
Joint review: Broker authorizes routine trips; MCO approves high-acuity modes. Used by UnitedHealthcare and Anthem.
Direct MCO control: No broker involved; PA validated against EHR data. Used by Kaiser and some Florida/NC plans.
Managing Multiple Payer Requirements
The primary 2026 challenge is fragmentation—different logins, PCS templates, modifiers, and credential requirements across payers. Providers serving multiple MCOs must track distinct rule sets for each.
Solutions for multi-payer management:
- API-connected NEMT software that syncs with multiple broker portals
- FHIR-based middleware (Waystar, Practolytics) for unified submission
- Universal template libraries aligned to 42 CFR § 438.236
- Payer-specific credential and driver tracking by platform
Technology and Automation for Prior Authorization
Technology has transformed NEMT prior authorization from a manual paperwork bottleneck into a real-time digital workflow. In 2026, the industry standard is electronic prior authorization (ePA) with automated eligibility checking, trip validation, and broker integration. Providers who haven’t adopted these tools face competitive disadvantages in processing speed and accuracy.
Benefits of Electronic Prior Authorization
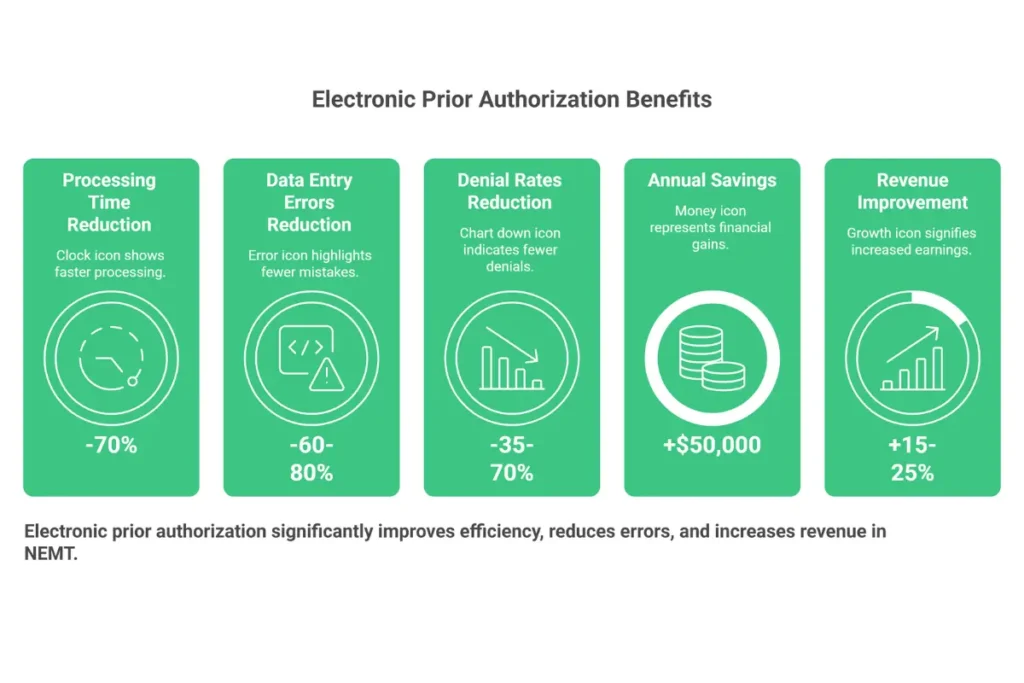
Across providers of all sizes, electronic PA delivers measurable operational gains that justify implementation costs:
Processing time reduction: 70% decrease (from days to hours)
Data entry errors: 60-80% reduction through auto-population
Denial rates: 35-70% reduction through validation before submission
Staff administrative cost: ~$50,000 annual savings per mid-size operation
Revenue improvement: 15-25% increase through clean first-pass approvals
Core Software Features for PA Management
Best-in-class NEMT software platforms include specific features that streamline PA workflows. For a detailed comparison of dispatch and billing platforms with authorization features, evaluating options helps identify the right fit for your operation size.
- Payer API connections: Direct integration with ModivCare, MTM, Veyo, and major MCOs
- State portal sync: EDI connections to eMedNY, TMHP, Medi-Cal, Oregon MMIS
- Trip-PA linking: Trips cannot dispatch without confirmed active authorization
- Exception-based workflows: Staff act on alerts rather than processing every submission
- Denial prediction: AI flags trip modes, mileage, or diagnosis combinations likely to reject
- Expiration tracking: Automated alerts before PA validity lapses
NEMT Software Platform Comparison
| Platform | Best Fit | PA Strengths |
|---|---|---|
| TobiCloud | Small-mid providers | Auto-attestation, state portal scraping, user-friendly |
| RouteGenie | Mid-size fleets | PA rule logic, clearinghouse integration |
| NEMT Cloud Dispatch | Multi-state operations | Custom workflows, digital form vault |
| Bambi | Tech-forward providers | AI auto-fill, predictive approvals |
| MediRoutes | Enterprise growth | Real-time broker sync, revenue risk analytics |
| TripMaster | Paratransit hybrids | Trip-bank, compliance-first tracking |
Emerging Technologies in NEMT PA
The future of NEMT prior authorization is AI-driven automation. Technologies emerging in 2026 promise further efficiency gains:
AI-generated documentation: Extracts data from EHRs or voice notes, reducing administrative time by an additional 40%.
Predictive PA outcomes: Analyzes denial patterns across diagnosis, mode, broker, and distance to help staff avoid submissions likely to fail.
Smart standing orders: Auto-maps dialysis, PT, and recurring trips to validity periods, eliminating expired authorization gaps.
Unified payer clearinghouses: One submission automatically routes to appropriate broker/payer, reducing multiple portal logins to one.
Prior Authorization Forms and Templates
No universal NEMT prior authorization form exists. Each state publishes its own templates, often available through Medicaid or broker portals. Knowing where to find the correct form—and how to submit it—prevents delays and rejections.
State PA Forms Directory
| State | Form Name/Number | Purpose | Where to Access |
|---|---|---|---|
| TX | F00045 | Ambulance PA Request | TMHP Portal, tmhp.com |
| TX | 4214 | Medical Necessity | TMHP Portal |
| CA | TAR | Treatment Authorization | Medi-Cal Provider Portal, plan portals |
| CA | DHCS 6182 | Certificate of Med Necessity | DHCS website, varies by plan |
| NY | 389701 | Transportation Auth Request | eMedNY portal |
| PA | PCS | Physician Certification | PROMISe™ Portal, county MATP |
| IN | 55427 | Certificate of Need | IN.gov, Verida HealthSherpa |
| OH | ODM 03452 | Statement of Med Necessity | ODM Enterprise System |
| FL | PCS (standard) | Physician Certification | MTM Portal, MCO portals |
Medicare RSNAT Templates
Medicare doesn’t use a CMS-484 form for non-emergency ambulance. Instead, providers must use a Physician Certification Statement template from:
- CMS RSNAT resources
- Medicare Administrative Contractor (MAC) websites (CGS, Novitas, Noridian)
- Local provider portals
These forms upload directly into the RSNAT submission workflow.
Electronic vs. Paper Submission
Every state still accepts paper or fax submissions, but 2026 trends strongly favor electronic channels. Portal submissions provide faster tracking, instant receipt confirmation, and reduced processing times. Fax-only submissions risk delays and lost requests.
Electronic advantages:
- Real-time status tracking
- Instant submission confirmation
- Automated error checking before submission
- Document attachment capabilities
Frequently Asked Questions
What is NEMT prior authorization and why is it required?
NEMT prior authorization is the mandatory pre-service approval process that verifies a patient’s medical transportation is covered, medically necessary, and appropriate for the requested transport level. It is required under 42 CFR § 431.53 to ensure Medicaid and Medicare funds are used appropriately and to prevent fraud. Without PA, claims will be denied under code CO-197, and providers will not receive reimbursement for completed trips.
Who is responsible for obtaining NEMT prior authorization?
The NEMT provider or contracted transportation broker holds primary responsibility for obtaining prior authorization. Physicians support the process by completing Physician Certification Statements (PCS), and healthcare facilities provide clinical documentation, but the transport company bears ultimate responsibility. When PA is missing and claims are denied, the provider—not the hospital or physician—absorbs the financial loss.
How long does NEMT prior authorization approval typically take?
Processing times vary by payer and submission method. Standard Medicaid PA takes 2-5 business days, while MCOs typically decide within 2-5 days under federal 7-day requirements. Indiana’s Verida system averages 24-48 hours. Urgent or expedited requests are processed within 72 hours. Electronic portal submissions generally process faster than fax or mail.
What documentation is required for NEMT prior authorization?
Required documentation includes: member identification (name, DOB, Medicaid/Medicare ID), provider information (NPI, enrollment status), transport details (origin, destination, HCPCS code, mileage), and medical necessity documentation (signed PCS, ICD-10 codes, clinical narrative). Supporting documents like hospital discharge summaries, treatment schedules, and specialist letters strengthen requests for higher-acuity transport levels.
What is a Physician Certification Statement (PCS) and when is it required?
A PCS is a signed medical document certifying that a patient’s medical condition prevents safe use of personal or public transportation, justifying the requested NEMT level. PCS is required for all ambulance transport (BLS/ALS), stretcher transport, air ambulance, and wheelchair transport in many states. The PCS must be signed by an MD, DO, NP, PA, or CNS before the first transport date.
Can I transport a patient without prior authorization?
Transporting without required PA results in claim denial at essentially 100% rates. True emergency 911 responses bypass PA, and some states allow retroactive authorization within 15-30 days for urgent situations. However, scheduled non-emergency transport without PA in place will not be reimbursed. Providers should verify PA exists before dispatch for every trip requiring authorization.
What happens if prior authorization is denied?
When PA is denied, providers receive a denial notice with a specific reason code. Appeals must be filed within 30-60 days (Medicaid) or 120 days (Medicare). Success rates average 40-70% when additional documentation is submitted. First-level reconsideration addresses documentation errors (85% overturn rate), while peer-to-peer review handles medical necessity disputes (50-65% success rate).
How long is NEMT prior authorization valid once approved?
PA validity varies by payer and condition type. Medicare general PA lasts up to 60 days for recurring transport. Medicaid allows 6-12 months for chronic conditions depending on state. MCOs typically limit validity to 90 days. Acute/temporary authorizations may last only 7-30 days. Track expiration dates and submit renewals 14-30 days before PA lapses to avoid coverage gaps.
Do dialysis patients require prior authorization for each transport?
No—standing order PA covers scheduled dialysis trips for 60-90 days or longer, depending on the payer. Initial authorization requires ESRD documentation, dialysis center treatment schedule, and PCS certifying ongoing transport need. Renewals require updated clinical status confirmation. Individual trips within an active standing order don’t require separate authorization.
How do I appeal a prior authorization denial?
Submit appeals through the same portal or fax used for the initial PA request. Include the original denial letter reference, corrected or updated PCS addressing the denial reason, additional medical records, physician support letter, and specific response to the denial reason. Request peer-to-peer review for medical necessity disputes. File within stated deadlines—30-60 days for Medicaid, 120 days for Medicare.
What is the difference between prior authorization and eligibility verification?
Eligibility verification confirms that a patient has active Medicaid/Medicare coverage. Prior authorization approves a specific trip based on medical necessity review. Both must be completed—eligibility check first, then PA if required for the transport type. Eligibility verification prevents PR-19 (inactive patient) denials, while PA prevents CO-197 (no authorization) denials. They serve different purposes and are not interchangeable.
Does Medicare require prior authorization for all non-emergency ambulance transports?
Medicare PA requirements apply under the RSNAT program after a beneficiary receives 40 or more round trips (or 80 one-way trips) within a 60-day period. Before reaching this threshold, PA isn’t required, but a Physician Certification Statement is always required for non-emergency ambulance billing regardless of frequency. Once the RSNAT threshold is crossed, every subsequent transport requires PA with PCS and medical records.
What does NEMT prior authorization mean?
NEMT prior authorization is a mandatory approval process where Medicaid, Medicare, or managed care plans verify that non-emergency medical transportation is medically necessary before the trip occurs. This pre-service review confirms the patient cannot safely use personal or public transportation, the requested transport level (wheelchair, stretcher, ambulance) matches the patient’s clinical condition, and the provider is enrolled and qualified to deliver the service.
How do I get prior authorization for medical transportation?
To obtain NEMT prior authorization: (1) Verify patient eligibility using EDI 270/271 at least 48 hours before service, (2) Obtain a signed Physician Certification Statement documenting medical necessity, (3) Complete the state-specific PA form with accurate ICD-10 codes and trip details, (4) Submit through the appropriate portal (TMHP for Texas, eMedNY for New York, Verida for Indiana), and (5) Track the request and respond to any information requests within 24 hours.
What is a PCS form for NEMT?
A Physician Certification Statement (PCS) is a signed medical document required for NEMT prior authorization that certifies a patient’s medical condition prevents safe use of personal or public transportation. The PCS must include patient identification, diagnosis codes (ICD-10), a narrative explaining functional limitations, the transport level required, and a signature from an MD, DO, NP, PA, or CNS dated before the first transport.
Who can sign a Physician Certification Statement for ambulance transport?
Medicare accepts PCS signatures from physicians (MD, DO), nurse practitioners (NP), physician assistants (PA), and clinical nurse specialists (CNS). State Medicaid programs may accept additional signers including physical therapists for rehab-related transport and treating specialists. Medical assistants and administrative staff cannot sign PCS forms under any program.
What is the CO-197 denial code?
CO-197 is the NEMT claim denial code meaning “No prior authorization on file.” This denial indicates the transport was completed without required PA in place. CO-197 accounts for approximately 35% of all NEMT claim denials and results in 100% revenue loss unless successfully appealed within 30-60 days (Medicaid) or 120 days (Medicare).
How long does Medicaid prior authorization take?
Standard Medicaid NEMT prior authorization takes 2-5 business days for fee-for-service and managed care plans. Indiana’s Verida broker averages 24-48 hours. Expedited requests for urgent situations are processed within 72 hours. California and New York allow 24-48 hours for urgent requests, 5-7 days for standard. Electronic portal submissions process faster than fax or mail.
What is Medicare RSNAT?
Medicare RSNAT (Repetitive Scheduled Non-Emergent Ambulance Transport) is the nationwide prior authorization program for Medicare beneficiaries requiring frequent ambulance services. RSNAT applies after 40 round trips (or 80 one-way trips) within 60 days. Once triggered, every subsequent ambulance transport requires PA with a Physician Certification Statement and medical records proving the patient cannot use lower-cost transportation.
What happens if you transport without prior authorization?
Transporting without required prior authorization results in claim denial at essentially 100% rates under denial code CO-197. The provider loses all reimbursement for the completed trip, including fuel, driver wages, and vehicle costs. Appeals may recover revenue if filed within deadlines (30-60 days for Medicaid, 120 days for Medicare), but success requires demonstrating medical necessity that should have been approved.
How do I appeal a denied NEMT prior authorization?
To appeal a denied NEMT PA: (1) File within the deadline (30-60 days for Medicaid, 120 days for Medicare), (2) Submit through the same portal or fax used for the original request, (3) Include the denial letter reference number, corrected PCS, additional medical records, and physician support letter, (4) Request peer-to-peer review for medical necessity disputes. Appeal success rates average 40-70% when additional documentation is provided.
What is the difference between PA and eligibility verification for NEMT?
Eligibility verification (EDI 270/271) confirms a patient has active Medicaid or Medicare coverage—it answers “Is this person insured?” Prior authorization approves a specific trip based on medical necessity review—it answers “Should this trip be covered?” Both are required. Eligibility verification prevents PR-19 denials (inactive coverage), while PA prevents CO-197 denials (no authorization). They are not interchangeable.
Do dialysis patients need prior authorization for every trip?
No. Dialysis patients receive standing order prior authorization that covers multiple trips over 60-90 days or longer. Initial authorization requires ESRD documentation, dialysis center treatment schedule, and PCS certifying ongoing transport need. Individual trips within the standing order validity period don’t require separate PA requests. Renewals must be submitted 14-30 days before expiration.
What HCPCS codes require prior authorization?
HCPCS codes requiring NEMT prior authorization include: A0428 (BLS ambulance), A0426 (ALS ambulance), A0430 (fixed-wing air ambulance), A0431 (rotary-wing air ambulance), and T2005 (stretcher van). A0130 (wheelchair van) requires PA in some states based on distance thresholds. A0080 (ambulatory sedan) rarely requires PA. All non-emergency ambulance codes require PCS regardless of PA requirements.
What is the 40 trip rule for Medicare ambulance?
The “40 trip rule” refers to Medicare RSNAT thresholds. When a beneficiary receives 40 or more round trips (or 80 one-way trips) within a 60-day period for scheduled, non-emergency ambulance transport, prior authorization becomes mandatory for all subsequent ambulance services. Before reaching this threshold, PA isn’t required, but a Physician Certification Statement is always required for ambulance billing.
Quick Reference Tables
HCPCS Codes and PA Requirements
| HCPCS | Service | PA Required | PCS Required |
|---|---|---|---|
| A0080 | Ambulatory/Sedan | Rarely | No |
| A0100 | Taxi/Non-Medical Vehicle | Rarely | No |
| A0130 | Wheelchair Van | Conditional | Yes (most states) |
| T2005 | Stretcher Van | Always | Yes |
| A0428 | BLS Ambulance | Always | Yes |
| A0426 | ALS Ambulance | Always | Yes |
| A0430 | Fixed-Wing Air | Always | Yes |
| A0431 | Rotary-Wing Air | Always | Yes |
Denial Codes Quick Reference
| Code | Meaning | Primary Cause | Prevention |
|---|---|---|---|
| CO-197 | No prior authorization | PA not obtained before service | Verify PA before dispatch |
| PR-19 | Inactive eligibility | Coverage lapsed | Run 270/271 check 48 hrs prior |
| CO-4 | Incorrect modifier | Wrong service level coded | Match modifier to transport mode |
| CO-16 | Missing information | Incomplete claim data | Complete all required fields |
| CO-50 | Non-covered service | Service not in benefit plan | Verify coverage before scheduling |
State Portal Quick Reference
| State | Portal | Urgent PA Contact |
|---|---|---|
| TX | tmhp.com | 512-514-4200 |
| CA | medi-cal.ca.gov | 833-701-0051 (fax) |
| NY | emedny.org | Regional HRA offices |
| PA | promise.dpw.state.pa.us | County MATP |
| IN | in.gov/ihcp | Verida: 866-809-8889 |
| FL | ahca.myflorida.com | MTM portal |
| OH | medicaid.ohio.gov | 800-686-1516 |
Conclusion: Building a PA-Compliant Operation
Non-emergency medical transport prior authorization is no longer optional—it is a core compliance requirement that protects reimbursement, improves patient access, and aligns providers with 2026 CMS expectations. The providers who thrive in this environment treat PA not as an administrative burden but as a revenue protection system.
Key Takeaways
The fundamentals of NEMT prior authorization success come down to consistent execution of basic processes:
Verify early: Run eligibility verification (EDI 270/271) at scheduling, not dispatch.
Document thoroughly: PCS accuracy and ICD-10 code alignment eliminate preventable denials.
Match transport level: Request ambulance, stretcher, or wheelchair based on documented medical need—not patient preference.
Submit before service: Avoid CO-197 denials and retroactive uncertainty by confirming PA exists before dispatch.
Track expirations: PAs lapse at 60-365 days depending on state and condition—proactive renewal prevents gaps.
Provider organizations can reduce denial rates from 20%+ to below 10% by using state-approved templates, submitting clean PA packets the first time, and tracking approvals in digital systems. The return on this investment—measured in recovered revenue and reduced administrative rework—compounds with every trip.
2026 Industry Direction
The regulatory and operational landscape continues to evolve. Providers should prepare for:
- 7-day nationwide PA decision standards under CMS-0057-F
- 72-hour expedited timeline requirements for urgent requests
- FHIR-based ePA APIs rolling out across Medicaid and Medicare Advantage
- Continued broker and technology consolidation
- AI triage tools reducing manual administrative burden by up to 80%
When to Consider Professional Billing Support
Managing prior authorization internally makes sense for smaller operations with straightforward payer mixes. However, as complexity increases, many providers find that professional medical transportation billing services deliver better outcomes than in-house teams stretched thin across multiple responsibilities.
Consider professional support when:
- Operating in multiple states with different requirements
- Managing more than 500 trips per month
- Denial rates exceeding 15%
- Staff turnover disrupts billing continuity
- PA backlogs delay patient services
Professional billing partners bring dedicated expertise, established payer relationships, and technology infrastructure that most individual providers can’t justify building internally. For providers ready to launch or scale their transportation operations, partnering with experienced billing specialists accelerates the path to profitability.
Provider Resources
Bookmark these essential resources for ongoing reference:
- 42 CFR § 431.53 — Federal transportation assurance requirements
- CMS RSNAT guidance — Available through MAC portals (CGS, Novitas, Noridian)
- State Medicaid transportation manuals — State-specific PA rules and forms
- ModivCare/Verida/MTM provider academies — Broker-specific training
- American Ambulance Association (ambulance.org) — Industry best practices
For patients navigating the system from the other side, understanding how to schedule and prepare for medical transportation helps ensure smooth service delivery and reduces no-shows that impact provider revenue.
Success in NEMT requires mastering prior authorization. The providers who build robust PA systems—verifying eligibility, documenting necessity, submitting complete requests, and tracking approvals—protect their revenue while serving patients who depend on medical transportation access. This guide provides the foundation; implementation determines results.
This guide is provided for informational purposes by Elite Med Financials, a healthcare revenue cycle management company specializing in medical transportation billing. Need help with prior authorization management or NEMT billing? Contact our team for a free consultation. Consult state Medicaid manuals and payer-specific documentation for authoritative requirements—regulations change frequently.

