
Table of Contents
What is Mental Health Billing? The Complete Beginner’s Guide [2026]
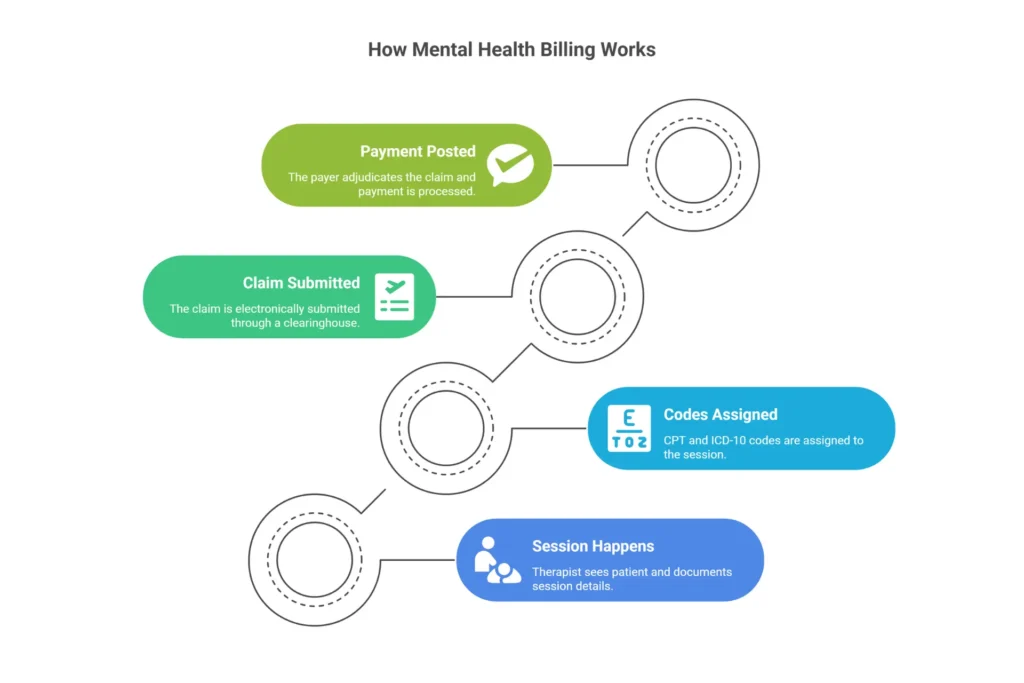
Mental health billing is how therapists and psychiatrists get paid for their clinical work. It’s the process of translating a 50-minute therapy session into the specific codes and forms insurance companies require to cut a check. When done right, it’s invisible. When done wrong, it consumes your evenings, drains your revenue, and puts your practice at audit risk.
If you’re new to private practice or just tired of denials, this guide walks you through everything — from basic definitions to the seven most common mistakes, and finally, how to know if you should handle billing yourself or bring in help.
Let’s start at the very beginning.
What Is Mental Health Billing?
Mental health billing is the process of submitting claims to insurance companies for therapy, psychiatric evaluations, and counseling services using specialized CPT and ICD-10 codes.
It involves documenting exactly what happened in a session — how long it lasted, what diagnosis it addressed, and why it was medically necessary — then formatting that information so payers like Medicare, Blue Cross, or Cigna will reimburse you.
Unlike general medical billing, mental health billing is time-based. You’re not billing for a procedure with hard data like a blood test or X-ray. You’re billing for a conversation, which means your documentation has to prove that conversation was worth paying for.
Mental Health Billing Definition
The Centers for Medicare and Medicaid Services (CMS) defines mental health billing as the submission of claims for covered services including diagnostic interviews, individual and group psychotherapy, crisis interventions, and psychiatric evaluations provided by qualified professionals under Medicare Part B. These services require compliance with state licensure, documentation standards, and medical necessity criteria.
In plain English: it’s how you prove to an insurance company that you did your job so they’ll send you money.
Who Performs Mental Health Billing?
A wide range of clinicians bill for mental health services, each with slightly different rules depending on their license and the payer.
Psychiatrists (MD/DO) bill for both therapy and medication management, often using E/M codes (99213–99215) with psychotherapy add-ons like +90833.
Psychologists (PhD/PsyD) bill for diagnostic evaluations (90791), psychological testing (96130–96133), and therapy sessions.
Licensed Clinical Social Workers (LCSWs) are the backbone of therapy billing, routinely using 90834 and 90837. Under Medicare, they bill at 75% of the psychologist rate but cannot bill for diagnostic evaluations requiring medical services.
Licensed Professional Counselors (LPCs) and Licensed Marriage and Family Therapists (LMFTs) gained Medicare billing authority in 2024, finally putting them on equal footing with LCSWs for psychotherapy services.
Psychiatric Mental Health Nurse Practitioners (PMHNPs) bill for both medication management and therapy, often using the same E/M plus add-on combinations as psychiatrists, though state practice acts vary on independence.
Board Certified Behavior Analysts (BCBAs) use a different coding system entirely — HCPCS codes like H0031 for assessments and 97151–97158 for treatment, billed in 15-minute increments.
Billing specialists are the unsung heroes who submit the claims, track payments, and fight denials. Most practices either employ them in-house or outsource to a dedicated mental health billing service.
What Services Does Mental Health Billing Cover?
Mental health billing covers a broad spectrum of services, each with its own CPT code family:
- Psychiatric diagnostic evaluations (90791) — The initial intake, typically 60–90 minutes, without medical services.
- Individual psychotherapy — 90832 (30 minutes), 90834 (45 minutes), 90837 (60+ minutes). These account for roughly 63% of all mental health claims.
- Psychotherapy with E/M services — Add-on codes 90833, 90836, and 90838 for sessions combining therapy with medication management.
- Family and group therapy — 90846 (family without patient), 90847 (family with patient), 90853 (group).
- Crisis intervention — 90839 for the first 30–74 minutes, +90840 for each additional 30.
- Health behavior interventions — 96156–96171 for services targeting physical health conditions with psychological components.
- Collaborative care management — 99492–99494 for integrated care between primary care and psychiatry.
- Telehealth services — Same codes as in-person, with POS 10 (patient’s home) and modifier 95 or 93 appended.
Mental Health Billing vs. Medical Billing — 7 Key Differences
If you’ve ever tried to bill a 60-minute therapy session the same way you’d bill a strep test, you already know: mental health billing lives in its own world. The rules are different, the denial rates are higher, and the documentation has to tell a story, not just report a result.
| Aspect | Mental Health Billing | Medical Billing |
|---|---|---|
| Primary Coding Method | Time-based CPT codes (90832–90837) with strict midpoint rule | Procedure-based and E/M codes tied to medical decision-making |
| Documentation Type | Narrative progress notes proving medical necessity; DAP format; PHQ-9 scores | SOAP notes; objective findings; lab values; imaging results |
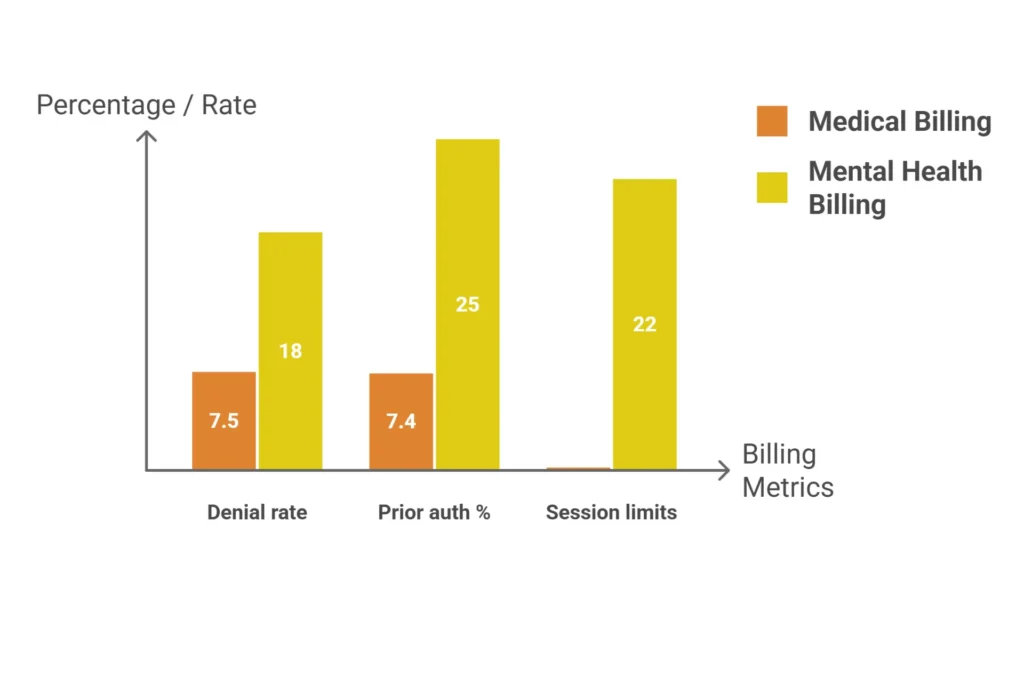
| Prior Authorization Frequency | 20–30% of claims; ongoing therapy often flagged after 6–12 sessions | ~7.4% of Medicare Advantage claims |
| Denial Rates | 16–20% average — double the medical average | 5–10% average |
| Top Denial Reasons | CO-16 (incomplete docs), CO-50 (not medically necessary), missing prior auth | CO-16 (missing info), CO-97 (bundled service), CO-50 (non-covered) |
| Session/Visit Limits | 18–26 outpatient sessions per year common across many plans | Rare for office visits |
| Telehealth Rules (2026) | Permanent; no geographic limits; audio-only covered; POS 10 standard | Temporary for most specialties; audio-only generally not covered |
| Behavioral Health Carve-Outs | Common — UHC → Optum; BCBS → Carelon; separate payer IDs | Essentially non-existent in medical billing |
1. Time-Based vs. Procedure-Based Coding
Medical billing loves hard data. Did you remove a mole? Bill 11400. Did you read an EKG? Bill 93000. There’s a code for the thing you did.
Mental health doesn’t work that way. You’re billing for time spent, not tasks performed. A 45-minute session using CBT for anxiety gets the same 90834 as a 45-minute session using EMDR for trauma. The code doesn’t care about your modality — only your minutes.
This is where the midpoint rule comes in. For 90834 (45 minutes), the time range is 38–52 minutes. For 90837 (60 minutes), it’s 53 minutes or more. Bill 90837 for a 50-minute session, and you’ve created an audit trail. Payers can — and do — go back three years demanding repayment for upcoded claims, plus interest and potential False Claims Act penalties.
2. Documentation: Narrative vs. Objective
A medical note can document a cough, a negative chest X-ray, and a prescription. That’s sufficient. There’s objective proof the visit happened.
A therapy note has to convince a reviewer who never met your patient that this hour of conversation was medically necessary. You need the diagnosis, the functional impairment, the treatment goals, the interventions used, and the patient’s response. Every session.
Psychotherapy notes (your private process notes) are not the same as progress notes (the record shared with insurers). Psychotherapy notes carry special HIPAA protection under 45 CFR 164.524 and cannot be required for payment. But your progress notes must be detailed enough to justify every minute billed.
3. Prior Authorization Burden
In medical billing, you might need prior auth for an MRI or surgery. In mental health, you often need it just to keep seeing a patient after their 12th session. About 20–30% of mental health claims require prior authorization, and for ongoing therapy, that number can hit 50%. Miss it, and you get CO-16: your claim is denied and rarely recoverable.
4. Denial Rates: Twice as High
Medical claim denials average 5–10%. Mental health runs 16–20%, with intensive outpatient programs sometimes exceeding 30%. Because medical necessity in mental health is subjective, your documentation has to leave no room for interpretation by a reviewer who has never seen your patient.
5. Carve-Outs: The Payer Within a Payer
A patient might hand you a UnitedHealthcare card, but their mental health benefits are actually managed by Optum. Or Blue Cross, but Carelon Behavioral Health handles therapy claims. These behavioral health carve-outs have their own payer IDs, prior auth rules, and fee schedules. Bill the primary insurer directly, and your claim vanishes. This complexity is almost entirely absent from medical billing.
6. Session Limits
Most medical services have no annual visit caps. Mental health plans routinely cap therapy at 20–26 sessions per year. Exceed the limit without authorization, and the overage is unrecoverable. Our eligibility verification services catch these limits before they become problems.
7. Telehealth: Permanent vs. Temporary
CMS made most mental health telehealth flexibilities permanent in 2026. You can see patients at home (POS 10) via audio-only (modifier 93) or video (modifier 95), with no geographic restrictions. Other specialties lost these advantages after the COVID-era extensions expired. Mental health kept them.
The Mental Health Billing Process — Step by Step
Mental Health Billing for Dummies — 3 Rules to Live By
- Verify before you see. Check insurance 48 hours before every appointment. Coverage that was active last month may have changed.
- Document the minutes. Write start and stop times. “60 minutes” is a claim. “1:00 PM – 1:55 PM” is evidence.
- Submit within 72 hours. The longer you wait, the closer you get to a timely filing denial.
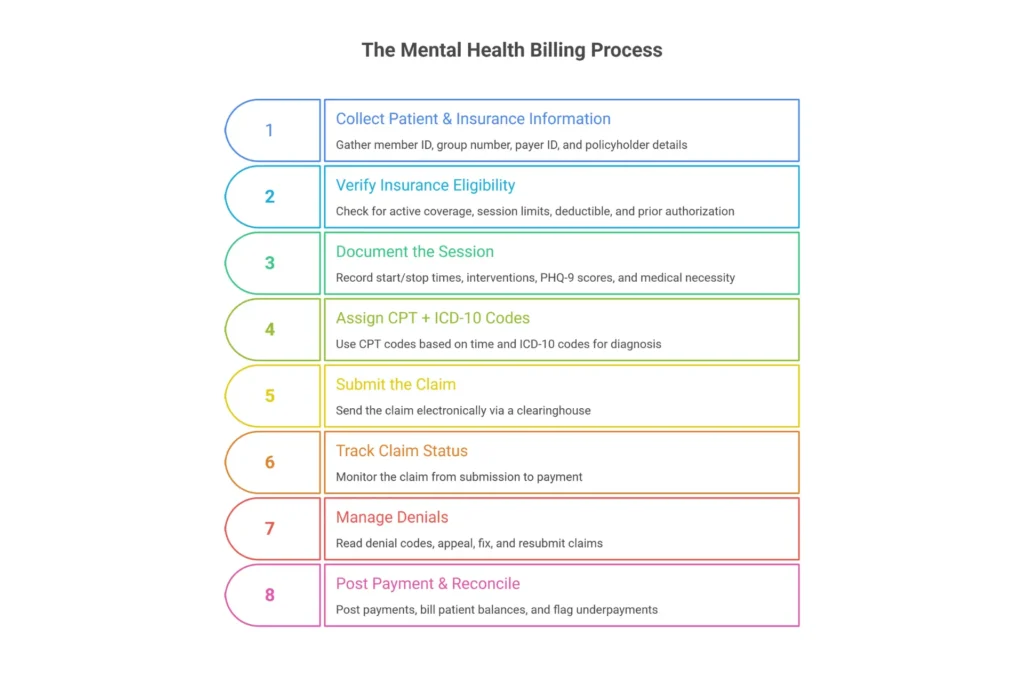
Step 1: Collect Patient and Insurance Information
Get the insurance card — front and back. Record:
- Member ID exactly as shown (no typos; “Bob” vs. “Robert” rejects claims)
- Group number and payer ID
- Policyholder name and date of birth
- Coverage effective and termination dates
Step 2: Verify Insurance Eligibility
Run a real-time eligibility check through your EHR or a clearinghouse like Availity before the first session. Confirm: Is the policy active? How many therapy sessions are covered annually? What is the deductible and copay? Is prior authorization required? Is this a behavioral health carve-out?
Q: How do I verify insurance eligibility for mental health services?
Use your EHR’s built-in eligibility tool or a clearinghouse to run a real-time 270/271 transaction. Verify the member ID, active dates, session limits, deductible, copay, and prior authorization requirements. Do this 48 hours before every appointment — coverage changes monthly.
Free Download: 2026 Mental Health Billing Verification Checklist
48-point pre-session checklist used by billing specialists. Covers eligibility, prior auth, CPT code selection, documentation, and timely filing — one sheet per patient, per session.
WHAT’S INSIDE
✓ Prior authorization tracking (6 items)
✓ CPT code selection guide (midpoint rule)
✓ ICD-10 documentation requirements
✓ Timely filing deadline reference by payer
✓ Common denial codes + instant fixes
✓ Telehealth modifier guide (POS 10, 95, 93)
Free for all mental health providers · PDF · Print-ready · No sign-up required
Step 3: Document the Session
Your note must include: date of service, start and stop times, presenting problem, interventions used (CBT, EMDR, DBT, supportive therapy), patient response, risk assessment where indicated, and why the session was medically necessary. Include standardized assessment scores when relevant — PHQ-9 for depression, GAD-7 for anxiety. Payers respond to numbers. Our medical coding services ensure notes translate into billable claims.
Step 4: Assign CPT and ICD-10 Codes
Select the CPT code based on total face-to-face time:
- 90832: 16–37 minutes
- 90834: 38–52 minutes
- 90837: 53+ minutes
Pair it with the most specific ICD-10 code the documentation supports. Use F41.1 (generalized anxiety disorder) rather than F41.9 (unspecified anxiety) when the record supports it. Sequence the primary diagnosis — the main reason for treatment — first.
For a complete breakdown of every mental health CPT code, 2026 Medicare rates, and telehealth modifiers, see our Mental Health CPT Codes Complete Guide →
Step 5: Submit the Claim
Most claims go electronically as an 837P file through a clearinghouse. The clearinghouse scrubs for errors — missing NPI, invalid modifiers, mismatched codes — before forwarding to the payer. Electronic claims pay in 14–30 days. Paper CMS-1500 forms take 30–60 and have higher rejection rates. Stop using paper.
Q: What is the golden rule of medical billing? “If it isn’t documented, it didn’t happen.” Every service you bill must have corresponding documentation proving it occurred and was medically necessary. In mental health, progress notes must show session time, interventions, patient response, and how the service addressed the active diagnosis.
Step 6: Track the Claim
Watch for the claim to move from submitted to accepted to paid. If it’s been 21 days without movement, follow up. Payers lose claims. A follow-up call often finds them.
Step 7: Manage Denials
Read the denial reason code and act accordingly:
- CO-16: Missing prior authorization or information → get retroactive auth or submit missing data
- CO-50: Not medically necessary → appeal with stronger documentation
- CO-96: Non-covered service → verify benefit language and appeal with parity act arguments
- PR-49: Incorrect coding → correct the code and resubmit
Q: What are the top 5 denials in mental health billing? The top five are: (1) CO-16 (missing prior auth or documentation), (2) CO-50 (not medically necessary), (3) incorrect CPT or ICD codes, (4) CO-27 (expired eligibility), and (5) timely filing violations. Together they account for 70–80% of all mental health denials. Our denial management services resolve these systematically.
Step 8: Post Payments and Reconcile
When payment arrives as an ERA 835 or paper EOB, post it to the patient’s account. Write off contractual adjustments. Bill the patient for remaining deductibles, copays, or coinsurance. Then reconcile: does the payment match what you expected? Underpayments are common and often recoverable through our AR follow-up process.
Mental Health Billing Terminology — The Complete Glossary
CPT Code — Current Procedural Terminology codes maintained by the AMA. In mental health, primarily time-based: 90832 (30 min), 90834 (45 min), 90837 (60+ min). Includes add-ons like 90833 for therapy with medication management.
ICD-10 Code — Diagnosis codes from the International Classification of Diseases. Mental health uses F-codes mapped from DSM-5 (e.g., F32.9 for major depressive disorder, F41.1 for GAD). Must be as specific as possible to prove medical necessity.
Add-On Code — A CPT code with a “+” symbol billed only alongside a primary code. Examples: +90833 (30-min therapy with E/M), +90836 (45-min with E/M), +90838 (60-min with E/M). Used when a psychiatrist provides both medication management and therapy in one visit.
Modifier — Two-character codes adding context to a claim. Common in mental health: 95 (synchronous video telehealth), 93 (audio-only telehealth), 25 (significant, separately identifiable E/M same day as another service).
Place of Service (POS) Code — Two-digit codes indicating where service occurred. POS 11 = office. POS 02 = telehealth from non-home location. POS 10 = telehealth from patient’s home (standard for mental health in 2026).
NPI (National Provider Identifier) — Your unique 10-digit ID required on every claim. Type 1 is for individuals. Type 2 is for organizations. Both appear on group practice claims.
ERA (Electronic Remittance Advice) — The 835 file showing what was paid, denied, or adjusted. Auto-posts to your EHR when configured correctly.
EOB (Explanation of Benefits) — The patient-friendly version of the ERA. Shows what insurance paid and what the patient owes.
BAA (Business Associate Agreement) — A HIPAA-required contract between you and any vendor handling protected health information. Non-negotiable for billing companies.
CMS-1500 Form — The paper claim form (or its electronic equivalent, the 837P). Contains all patient, provider, and service information.
Clearinghouse — The middleman that scrubs your claims for errors and routes them to payers. Availity, Change Healthcare, and Waystar are the most common in mental health.
EDI (Electronic Data Interchange) — The standard format for electronic healthcare transactions. 837P for claims, 835 for payments, 270/271 for eligibility.
Allowed Amount — The maximum a payer will pay for a service. You write off anything above it per your network contract.
Deductible — What the patient pays before insurance covers services. Must be tracked and collected.
Copay vs. Coinsurance — Copay is a fixed fee per visit (e.g., $25). Coinsurance is a percentage of the allowed amount (e.g., 20%).
Out-of-Pocket Maximum — The annual cap on patient costs. Once met, insurance pays 100%.
Prior Authorization (PA) — Pre-approval from an insurer before providing certain services. Required for ongoing therapy beyond session limits in many plans.
Timely Filing — The deadline to submit claims. Medicare: 365 days. Aetna: 90 days. United: 90–120 days. Cigna: 180 days. Missing it permanently forfeits payment.
Medical Necessity — Clinical justification that a service is required to diagnose or treat a condition. Proved through documentation linking diagnosis, functional impairment, and treatment response.
Superbill — A detailed receipt for out-of-network patients to submit to their own insurance. Includes all coding information plus provider NPI and charges.
HIPAA — The Health Insurance Portability and Accountability Act. Sets privacy and security standards for all health information.
Credentialing / Paneling — The process of getting approved to join insurance networks. Takes 90–120 days. No billing until complete. Learn more about our credentialing services.
Incident-To Billing — Services by a non-physician billed under a supervising physician’s NPI at 100% of the physician rate. Requires direct supervision and an established treatment plan.
RCM (Revenue Cycle Management) — The end-to-end financial process from patient scheduling to final payment collection. Our full RCM services cover every step.
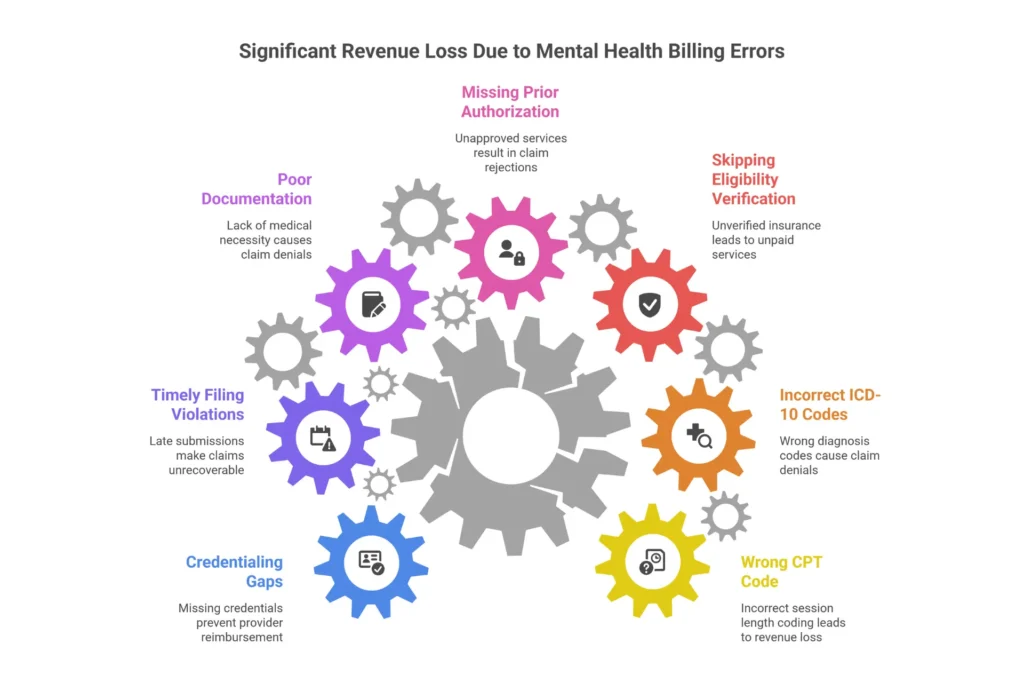
Why Mental Health Billing Fails — The 7 Most Common Mistakes
💡 Is your practice making any of these 7 mistakes right now?
Our free billing audit analyzes your last 90 days of claims, identifies exactly where revenue is leaking, and compares your metrics against industry benchmarks — at no cost and no obligation.
Get My Free Billing Audit →Mistake 1: Wrong CPT Code for Session Length
What it is: Billing 90837 (60-minute code) for a 50-minute session.
Why it happens: Therapists estimate, or assume a few minutes of difference won’t matter. It does.
Financial impact: A single 90837 downcoded to 90834 costs $35–$50. Multiply by 20 sessions weekly over a full year, and you’re either leaving $48,000 on the table or facing an audit for upcoding.
Prevention: Write start and stop times. 38 minutes = 90834. 53 minutes = 90837. No exceptions.
Mistake 2: Incorrect ICD-10 Codes
What it is: Using unspecified codes (F32.9) when more specific ones are available (F32.1 for mild depression, F32.2 for severe). Or wrong sequence — billing relationship stress before the primary diagnosis.
Why it happens: Intake forms are vague, and diagnoses don’t get updated as patients progress or improve.
Financial impact: 15–20% of denials trace back to diagnosis errors. Unspecified codes for long-term ongoing therapy flag automatic reviews.
Prevention: Review diagnoses every 90 days. Update to the most specific code the documentation supports. Sequence the primary treatment reason first.
Mistake 3: Skipping Eligibility Verification
What it is: Assuming last month’s insurance is still active.
Why it happens: It’s tedious to check before every session, so it gets skipped.
Financial impact: One unverified patient seen for six sessions before a denial costs $900+ in unrecoverable revenue. Solo practices lose an average of $18,000 per year to this single mistake.
Prevention: Run eligibility checks 48 hours before every appointment. Automate it through your EHR.
Mistake 4: Missing Prior Authorization
What it is: Providing services without insurer pre-approval when required.
Why it happens: Providers assume session 13 works the same as session 1. It doesn’t for many plans.
Financial impact: 20–30% of mental health claims require prior auth. Without it, the denial is final. Practices lose $25,000–$50,000 per provider annually to auth denials.
Prevention: Check auth requirements during every eligibility verification. Track session counts. When a patient hits session 10, begin the auth process for the next block.
Mistake 5: Poor Documentation — Missing Medical Necessity
What it is: Session notes that don’t justify why the visit was clinically required.
Why it happens: You know why the session was needed — you were there. But the reviewer was not. Your note has to make the case for them.
Financial impact: This is the top denial driver, accounting for 25–35% of all rejected claims. In an audit, vague notes can trigger six-figure repayment demands.
Prevention: Every note should answer: What is the diagnosis? How does it impair function? What interventions were used? How did the patient respond? What is the treatment plan going forward?
Mistake 6: Timely Filing Violations
What it is: Submitting claims after the payer’s deadline.
Why it happens: Workflow gets disrupted. Corrected claims take time. The filing window closes before anyone notices.
Financial impact: 10–15% of claims die this way. Once the window closes, you cannot bill the patient. The revenue is permanently gone.
Prevention: Submit within 72 hours of every session. Know your deadlines: Medicare (365 days), Aetna (90), United (90–120), Cigna (180). Flag anything approaching 60 days unsubmitted.
Mistake 7: Credentialing Gaps
What it is: Treating patients before your effective date is confirmed with a payer.
Why it happens: The patient needs help now, and you want to see them. But payers do not pay for services rendered before your credentialing effective date — regardless of when you submitted the application.
Financial impact: A 90-day credentialing gap can cost $30,000 per provider in unrecoverable revenue.
Prevention: Begin credentialing 120 days before you plan to see patients on that plan. Track application status weekly. Confirm effective dates in writing before scheduling insured patients.
Is Mental Health Billing Easy? The Honest Answer
No. Mental health billing is technically demanding, administratively heavy, and constantly changing. Most therapists who manage their own billing spend 12–15 hours a week on it — time they could spend with patients. Denial rates are double those in medical specialties, and the rules that govern authorization, documentation, and coding shift without warning.
But “hard” doesn’t mean impossible. It means the right systems, the right training, or the right partner make a significant difference.
The 5 Reasons Mental Health Billing Is Harder Than It Looks
1. Time-based coding is unforgiving. One minute can cost you an entire code tier. The midpoint rule — 38 minutes for 90834, 53 for 90837 — leaves no room for rounding, guessing, or estimating.
2. Medical necessity is subjective. You’re not just documenting what happened; you’re making a case to a stranger that it was worth paying for. That requires a different skill than clinical work.
3. Payers change rules constantly. Insurance companies update policies, modifier requirements, and authorization rules without notice, sometimes mid-year. Keeping up is effectively a second job.
4. Behavioral health carve-outs multiply complexity. One patient can have different payer IDs for medical, mental health, and pharmacy benefits. Bill the wrong one, and the claim disappears with no explanation.
5. The emotional labor compounds everything. Therapists chose this field to help people — not to argue with insurance reviewers. The adversarial nature of denial management creates real burnout.
Q: What is the hardest part of medical billing and coding? Keeping up with constant payer rule changes — what billing specialists call payer rule drift. Insurers update medical necessity criteria, modifier requirements, and prior authorization rules without notice. In mental health, proving necessity through subjective narrative documentation adds a layer of complexity that specialties with objective test results simply do not face.
Stop spending 15 hours a week on billing. Start spending it on patients.
EliteMed Financials handles the entire mental health billing cycle — from eligibility verification to denial appeals — with a 98%+ clean claim rate and an average of 25–35 days in AR.
In-House vs. Outsourced Mental Health Billing — Side-by-Side Comparison
If you’re deciding whether to manage billing in-house or bring in a specialized service, the answer isn’t philosophical — it’s mathematical. Here is what the numbers actually show:
| Metric | In-House Billing | Outsourced (Specialized RCM) |
|---|---|---|
| Direct Annual Cost | $55,000–$75,000 salary + benefits + software | 5–8% of collections |
| Cost Per Claim | $25–$40 | $5–$15 |
| Denial Rate | 15–20% | 4–7% |
| Days in AR | 50–60 days | 25–35 days |
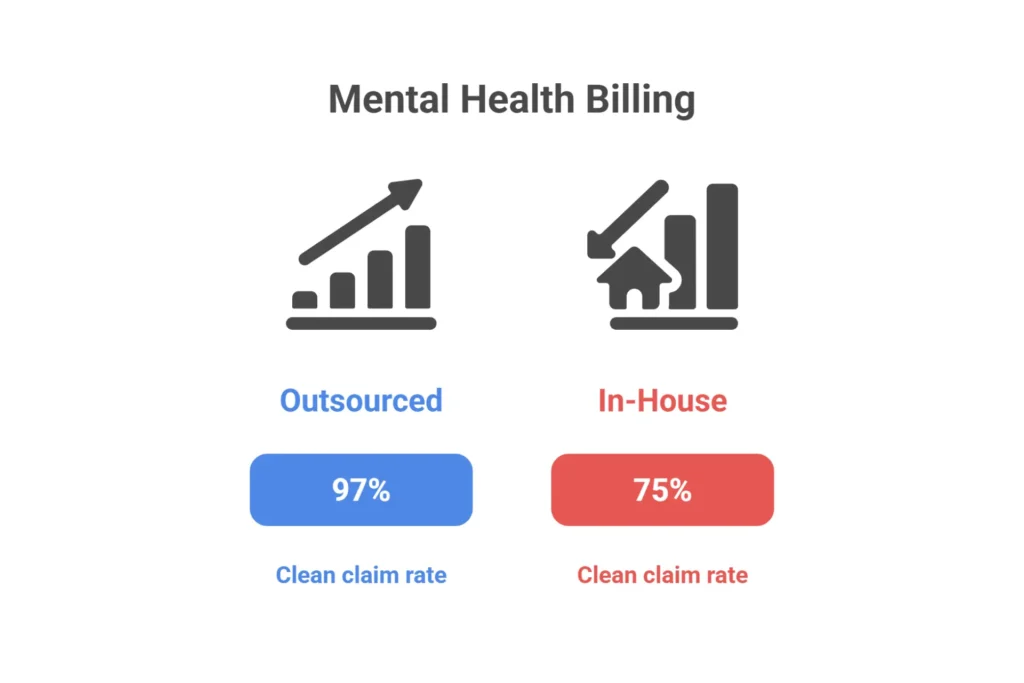
| Clean Claim Rate | 70–80% | 96–98% |
| Collection Rate | 75–85% | 95–98% |
| Provider Time Burden | 10–15 hours/week | Under 2 hours/week (report review) |
| Scalability | Requires hiring for growth | Scales automatically with volume |
| HIPAA Risk | Internal — depends on training and policy | Shared — billing company assumes liability via BAA |
When In-House Makes Sense
If you’re a solo practitioner with under $100,000 in annual collections and a simple, one or two-payer mix, you can manage billing yourself with solid EHR tools. You’ll spend 10–15 hours weekly and leave some revenue on the table, but you’ll avoid the service fee.
When Outsourcing Is the Better Call
If you collect more than $100,000 annually, manage multiple payers, deal with carve-outs, or simply value your clinical hours above the fee — outsourcing wins clearly.
The math for a solo therapist: paying 6% on $120,000 ($7,200/year) recovers 10 clinical hours weekly. At $150/hour, that’s $75,000 in potential revenue — a net gain approaching $68,000. For a 5-provider group, denial rates dropping from 18% to under 5% typically recover an additional $50,000+ annually on top of the fee paid.
Q: What are the benefits of outsourcing mental health billing? Outsourcing reduces denial rates from 15–20% to under 5%, cuts AR days from 50–60 to 25–35, and returns 10–15 clinical hours weekly to providers. Specialized companies handle prior authorizations, credentialing, and carve-outs while achieving 95–98% collection rates.
Q: How much does mental health billing outsourcing cost? Most mental health billing companies charge 5–8% of collected revenue. A solo practitioner collecting $100,000 annually pays $500–$700 monthly. Group practices pay $2,000–$5,000 monthly for 3–5 providers, with volume discounts for larger clinics.
How to Choose a Mental Health Billing Company [2026 Checklist]
Not all billing companies are created equal. A generalist medical billing company that also handles mental health as a sideline is not the same as a specialist. Use these eight questions to separate the right partners from the wrong ones.
1. “What is your first-pass clean claim rate for mental health clients?” Target: over 95%. EliteMed Financials achieves 98%+. Every percentage point below 95% translates directly into rework cost and delayed cash flow.
2. “What is your current denial rate and appeal success rate?” Target: denial rate under 5%; appeal success rate above 92%. The industry average runs 16–20%. Your partner should cut that by at least 60%.
3. “How many years of mental health-specific experience do your coders have?” Target: 5+ years minimum. They must understand the midpoint rule, add-on codes, behavioral health carve-outs, and telehealth modifiers — not just general billing concepts.
4. “What is your average Days in AR for mental health clients?” Target: under 30 days. The industry average runs 50–60. Every day claims sit unpaid is cash flow your practice cannot use.
5. “Can you provide 3–5 client references from practices similar to mine?” Target: at least two solo practitioners and two group practices. Call them. Ask specifically what changed after outsourcing.
6. “What technology do you use for claim scrubbing, denial prediction, and reporting?” Target: AI-powered scrubbing, predictive analytics, real-time dashboards. Manual processes catch some errors. Technology prevents them before they reach the payer.
7. “What is your exact pricing model, and what is included?” Target: transparent 5–8% with coding, claims, denials, appeals, eligibility verification, and patient follow-up included in the base fee.
8. “Will you sign a HIPAA Business Associate Agreement and include performance guarantees?” Target: yes to both. BAA is legally required. Performance guarantees — clean claim rate, denial rate, AR days — with service credits for misses show a company confident in its own work.
Red Flags That Should Send You Looking Elsewhere
- No mental-health-specific case studies or client references
- Clean claim rate below 90%
- Pricing above 8% with hidden add-on fees
- Refusal to sign a BAA
- Claims of “guaranteed 100% collections” (not possible and a warning sign)
- Large upfront setup fees over $5,000
- No certified coders on staff
What a 98%+ Clean Claim Rate Actually Means for Your Revenue
At the industry average of 92%, a $500,000 practice spends approximately $40,000 annually chasing denials and resubmitting claims. At 98%, that drops to roughly $10,000. The $30,000 difference flows directly to your bottom line — without seeing a single additional patient.
More importantly, a 98% rate means errors are caught before they reach the payer, not weeks later when a denial arrives. That’s the difference between proactive billing and reactive firefighting.
Ready to Stop Losing Revenue to Billing Errors?
EliteMed Financials specializes exclusively in mental health and behavioral health billing. Our certified coders have 10+ years of specialty experience, and we back every engagement with a written performance guarantee.
- ✓ 98%+ first-pass clean claim rate
- ✓ Denial rate under 4% (vs. 16–20% industry average)
- ✓ Average 25–35 days in AR (vs. 50–60 industry average)
- ✓ Full mental health billing: coding, submission, denials, appeals, credentialing
- ✓ HIPAA BAA included — always
Get Your Free Billing Audit →
No pressure. No commitment. Just data showing exactly what your practice is leaving on the table.
Or call us directly: +1 (307) 243-8064
Mental Health Billing FAQ
What is mental health billing?
Mental health billing is the process of submitting insurance claims for therapy and psychiatric services using specialized CPT and ICD-10 codes. It involves documenting session time, diagnosis, and medical necessity to receive reimbursement from payers like Medicare, Blue Cross, or Cigna.
How is mental health billing different from medical billing?
Mental health billing uses time-based codes (90832–90837) and requires extensive narrative documentation to prove medical necessity. It has higher denial rates (16–20% vs. 5–10%), more prior authorization requirements, and often involves behavioral health carve-outs where mental health benefits are managed by separate companies with different payer IDs and fee schedules.
Is mental health billing easy to learn?
It typically takes 6–12 months to reach working proficiency due to complex time-based coding rules, payer-by-payer variations, and documentation requirements. Therapists who self-bill spend 12–15 hours weekly on administrative tasks, and 68% report billing as their top practice burden.
What CPT codes are used in mental health billing?
The most-used codes are 90791 (diagnostic evaluation), 90832 (30-minute therapy), 90834 (45-minute therapy), 90837 (60-minute therapy), 90847 (family therapy with patient present), 90853 (group therapy), and add-ons like 90833 for therapy combined with medication management. All psychotherapy codes follow the midpoint rule for accurate time-based selection.
What is the golden rule of medical billing?
If it isn’t documented, it didn’t happen. Every service you bill must have corresponding documentation proving it occurred and was medically necessary. In mental health, progress notes must include session start and stop times, the interventions used, patient response, and how the service addressed the active diagnosis.
What causes mental health insurance claims to be denied?
The top five reasons are: poor documentation or missing medical necessity (25–35% of denials), incorrect CPT or ICD-10 codes (20%), missing prior authorization (20%), eligibility issues such as inactive coverage or exhausted session limits (15%), and timely filing violations (10%). Together these account for 70–80% of all mental health claim denials.
How long does it take to get paid from a mental health insurance claim?
Electronic claims pay in 14–30 days; paper claims take 30–60. Medicare targets 21 days for clean electronic claims. Average days in accounts receivable for mental health practices runs 45–60 days due to denial rates and rework. Outsourcing to a specialized billing company can consistently reduce that to 25–35 days.
Can a therapist do their own billing?
Yes — about 51% of solo therapists self-bill using EHRs like TherapyNotes or SimplePractice. The upside is saving the 5–8% billing service fee. The downside is that self-billing typically produces 15–25% revenue loss from preventable errors, approximately $30,000 per year per provider, and consumes 10–15 hours of clinical time weekly.
What is a superbill in mental health billing?
A superbill is a detailed receipt for cash-pay or out-of-network patients to submit to their own insurance. It includes patient info, date of service, CPT codes, ICD-10 diagnosis codes, charges, provider NPI, and diagnosis pointers. The patient pays you at the time of service, then uses the superbill to seek reimbursement from their insurer directly.
How does telehealth billing work for mental health in 2026?
Use POS 10 for sessions where the patient is at home, and append modifier 95 for video or modifier 93 for audio-only. CMS made mental health telehealth flexibilities permanent — no geographic restrictions, no in-person visit requirement through 2027, and audio-only coverage when video is unavailable. This is a permanent advantage mental health has over virtually all other specialties.
What is incident-to billing in mental health?
Incident-to billing allows services by a non-physician (such as an LCSW under supervision) to be billed under a supervising psychiatrist’s NPI at 100% of the Medicare physician rate rather than the therapist’s 75% rate. It requires direct on-site supervision, an established treatment plan from the physician, and that the physician saw the patient initially. Most private payers now require clinicians to use their own NPI regardless.
What is the hardest part of medical billing and coding?
Keeping up with constant payer rule changes — what billing specialists call payer rule drift — is the biggest ongoing challenge. Insurers update medical necessity criteria, modifier requirements, and prior authorization rules without notice, often mid-year. In mental health, proving necessity through subjective narrative documentation adds complexity that specialties using lab values and imaging do not face.
How often can you bill 90837?
As often as clinically necessary — typically weekly — provided sessions are at least 53 minutes and each note fully documents medical necessity, interventions, and patient response. Payers may flag providers who bill 90837 for more than 80% of sessions, which can trigger a medical necessity audit. Accurate documentation is your protection.
What is the 8 minute rule for therapy billing?
The 8-minute rule applies to timed physical and occupational therapy codes like 97110, not to mental health psychotherapy codes. Mental health uses the midpoint rule instead: 16–37 minutes = 90832, 38–52 minutes = 90834, 53 or more minutes = 90837. The 8-minute rule may occasionally apply to health behavior intervention codes (96156–96171) billed by mental health providers targeting physical conditions.
What is the difference between a claim denial and a claim rejection?
A rejection occurs before the payer processes the claim — typically a formatting error like an invalid NPI, missing required field, or duplicate claim. Rejections can be corrected and resubmitted immediately, often the same day. A denial occurs after the payer has adjudicated the claim and refused payment. Denials require a formal appeal, supporting documentation, or a corrected claim and take significantly longer to resolve.
What are the benefits of outsourcing mental health billing?
Outsourcing reduces denial rates from 15–20% to under 5%, cuts accounts receivable days from 50–60 to 25–35, and returns 10–15 clinical hours per week to providers. Specialized companies handle prior authorizations, credentialing, telehealth modifiers, and complex carve-outs while consistently achieving 95–98% collection rates — compared to 75–85% for in-house billing.
What are the 5 C’s of mental health?
Connection, Coping, Calmness, Care, and Compassion are clinical elements therapists work to build with and for their clients. While these are not billing terms, documenting patient progress toward these therapeutic goals in session notes helps establish medical necessity for ongoing treatment, which directly supports continued insurance reimbursement.
Quick Voice Search Answers
🎙 “What is mental health billing?”
Mental health billing is how therapists and psychiatrists submit insurance claims for sessions using CPT and ICD-10 codes to get reimbursed by Medicare, Medicaid, or private insurance.
🎙 “Is mental health billing easy?”
No. Mental health billing is significantly harder than general medical billing because of time-based coding rules, high denial rates, prior authorization requirements, and behavioral health carve-outs that vary by payer.
🎙 “What is the golden rule of medical billing?”
If it isn’t documented, it didn’t happen. Every service you bill must have matching notes proving it occurred, was medically necessary, and addressed the patient’s active diagnosis.
🎙 “Can a therapist do their own billing?”
Yes, but most lose 15–25% of revenue to billing errors and spend 10–15 hours weekly on paperwork. Outsourcing costs 5–8% of collections but typically recovers far more than that in reduced denials.
🎙 “How does therapy billing work?”
You verify insurance, document the session with the correct CPT code based on session length, submit an electronic claim through a clearinghouse, then track payment and manage any denials that come back.
🎙 “What is prior authorization for mental health?”
Prior authorization is pre-approval from an insurer before providing ongoing therapy. Most plans require it after 12–20 sessions. Without it, claims get denied with CO-16 and are rarely reversible.
🎙 “What is a superbill in therapy?”
A superbill is a detailed receipt with CPT codes, ICD-10 codes, and provider info that out-of-network patients use to claim reimbursement from their own insurance after paying you directly.
🎙 “What is a BAA in healthcare?”
A Business Associate Agreement is a HIPAA-required contract with any vendor that handles patient data. Every billing company must sign one before touching your patient records. It is legally non-negotiable.
EliteMed Financials provides specialized mental health and behavioral health billing services with a 98%+ clean claim rate. We are not a law firm and this guide is for informational purposes only. For legal or compliance questions, consult a qualified healthcare attorney.
External references: CMS Behavioral Health Integration | Mental Health Parity and Addiction Equity Act

