You’ve just finished a session. The clinical work was solid. Now you’re staring at your billing screen, unsure which code covers what you did, whether you can bill both services, and whether your documentation is audit-proof. That uncertainty costs mental health practices thousands of dollars every year—not from fraud, but from confusion. This guide covers every mental health CPT code you need in 2026: what each code means, who can bill it, exact time thresholds, 2026 Medicare rates, documentation requirements, and the most expensive errors to avoid. Whether you’re a psychiatrist, LCSW, psychologist, PMHNP, group practice owner, or billing staff member, you’ll finish this guide knowing precisely which code to use—and why.
Table of Contents
What Are Mental Health CPT Codes and Why Do They Matter?
Mental health CPT codes are five-digit identifiers maintained by the American Medical Association (AMA) that describe every service you provide to a patient. They’re the HIPAA-mandated billing language between your clinical work and insurance reimbursement. Without them, no payer—Medicare, Medicaid, or commercial—can process your claim.
What is a CPT code in mental health? It’s the standardized code that communicates what treatment you provided, for how long, and under what clinical circumstances. CPT codes are the financial backbone of every behavioral health practice: they determine your revenue per session, your audit exposure, and your parity law compliance.
Mental health coding is structurally different from most medical coding. Surgical codes describe a procedure. Mental health codes are time-based—the difference between 90834 and 90837 is 53 minutes. They require documented start and stop times, precise alignment with clinical complexity, and linkage to ICD-10-CM diagnoses to establish medical necessity. Add behavioral health carve-outs (where insurers separately administer mental health benefits through organizations like Optum or Beacon Health), and compliance requirements under the Mental Health Parity and Addiction Equity Act (MHPAEA), and you have a billing ecosystem that punishes imprecision.
Every provider type uses these codes differently. Psychiatrists and PMHNPs bill E/M codes for medication management, evaluation codes for intakes, and add-on psychotherapy codes for combined visits. LCSWs, LPCs, LMFTs, and psychologists bill standalone psychotherapy codes and evaluation codes. BCBAs use behavior identification and intervention codes. Each scope, each payer, each code has its own rules—and getting them wrong means denied claims, recoupments, or audit exposure.
The sections ahead walk through every code category: evaluations, psychotherapy, add-ons, group and family therapy, crisis intervention, interactive complexity, health behavior codes, collaborative care, telehealth modifiers, NP billing, and modifier codes—plus 2026 Medicare rates and the billing errors that cost practices the most.
Psychiatric Evaluation Codes — CPT 90791 and 90792 Explained
The first session sets the tone—clinically and financially. CPT 90791 and 90792 are the gateway to an entire episode of care.
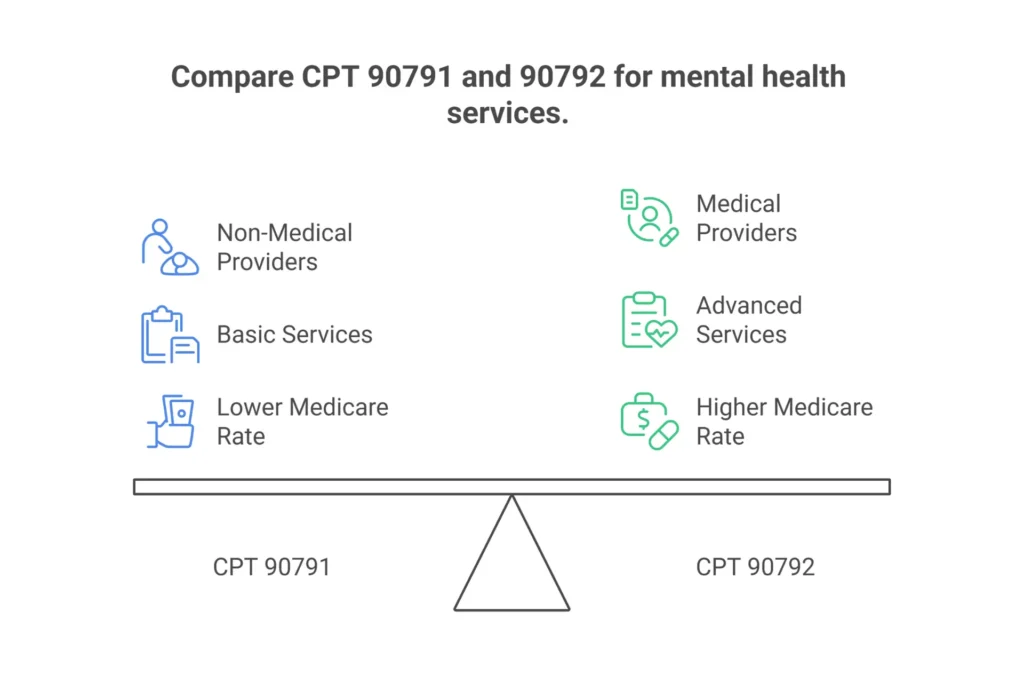
What is CPT code 90791 used for? CPT 90791 is a comprehensive psychiatric diagnostic evaluation performed without medical services. It includes taking a full psychiatric history, conducting a mental status examination (MSE), developing a diagnostic formulation, and documenting a treatment plan. Non-prescribing providers use it—psychologists, LCSWs, LPCs, LMFTs. There’s no mandatory minimum time, but thorough documentation of all required elements is expected. 2026 Medicare national average: $174.50 in non-facility settings.
What is the difference between 90791 and 90792? The single word “medical” separates them. 90791 is a diagnostic evaluation without medical services—no prescribing, no medication review, no physical exam components. 90792 includes medical services: medication review, prescribing decisions, lab orders, or physical assessment elements. Only prescribers—psychiatrists (MD/DO), psychiatric NPs (PMHNPs), and physician assistants—can bill 90792. The 2026 Medicare rate is approximately $202.08, about $27 higher than 90791, reflecting the additional medical complexity.
Can a psychiatric NP bill 90792? Yes. PMHNPs with prescriptive authority and Medicare enrollment can bill 90792 independently. Documentation must demonstrate medical services: medication review, prescribing rationale, and any physical assessment elements performed. When billing under their own NPI, NPs receive 85% of the physician fee—approximately $171.77.
Can 90791 and 90837 be billed on the same day? Yes, if the services are distinct. The evaluation establishes diagnosis and treatment plan; the therapy session provides separate therapeutic intervention with its own clinical content and time. Document each independently—separate sections or separate notes with distinct time allocations. No NCCI edit prohibits this pairing, but auditors will scrutinize same-day billing; cloned content across notes is the fastest way to trigger a review.
Documentation requirements for 90791/90792: The note must include a comprehensive psychiatric history, mental status examination (appearance, speech, mood, affect, thought process, thought content, cognition, insight, judgment), suicide and violence risk screening, diagnostic impression with supporting ICD-10-CM codes (F32.x for MDD, F41.1 for GAD, F90.x for ADHD), and a treatment plan specifying recommended frequency and modality.
Frequency limits: Medicare permits 90791/90792 once every six months per episode, with documentation of new clinical necessity for re-evaluation. Commercial payers typically limit to once per year. Billing more frequently without documented justification of a new episode is the type of pattern that triggers Targeted Probe and Educate (TPE) audits.
Before your evaluation codes can generate revenue, you must be properly credentialed. Our credentialing services help mental health providers get paneled with payers efficiently so nothing delays your first clean claim.
Psychotherapy CPT Codes — 90832, 90834, and 90837: Time Rules, Documentation, and Reimbursement
These three codes generate the majority of revenue for outpatient mental health—and they’re also the most common source of billing errors. A single minute makes the difference between 90834 and 90837, and billing the wrong one is either leaving money on the table or inviting an audit.
What is the difference between 90832, 90834, and 90837? All three are individual psychotherapy codes for insight-oriented, behavior-modifying, or supportive therapy. The only distinction is face-to-face session time, governed by the AMA midpoint rule. 90832 covers 16–37 minutes. 90834 covers 38–52 minutes. 90837 covers 53 minutes or more. Bill the code whose time range your documented session falls within—not the code closest to how long you intended the session to be.
| Code | Time Range | 2026 Medicare Rate | Most Common Use Case |
|---|---|---|---|
| 90832 | 16–37 minutes | $92.15 | Brief check-ins, medication follow-up |
| 90834 | 38–52 minutes | $134.25 | Standard weekly therapy session |
| 90837 | 53+ minutes | $172.80 | Intensive therapy, trauma work, complex cases |
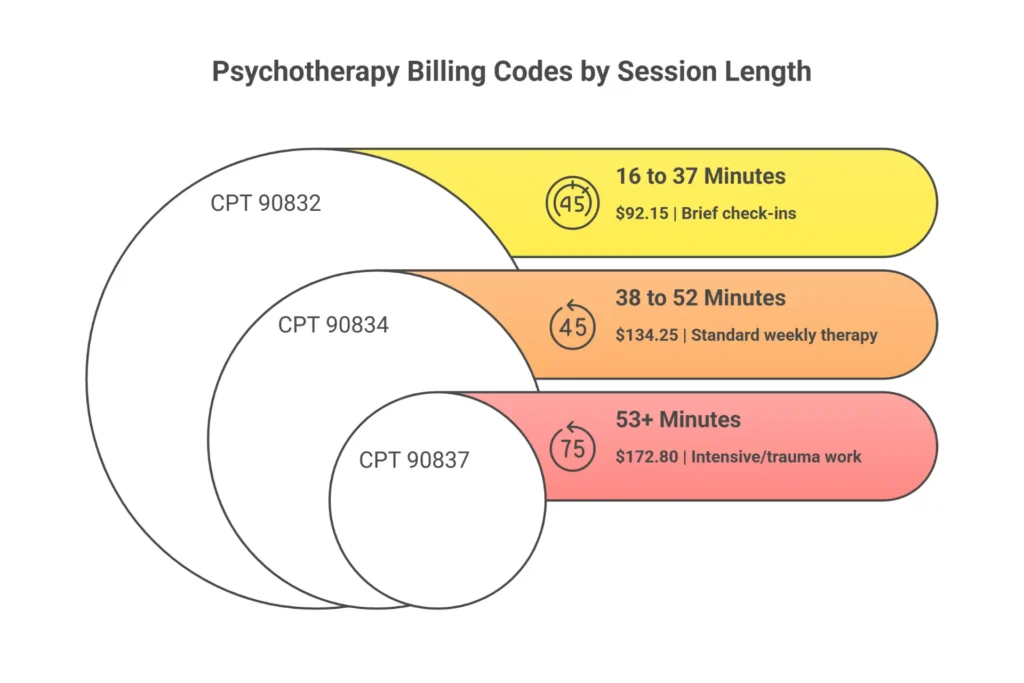
What is the time range for CPT code 90834? The official time range is 38 to 52 minutes of face-to-face psychotherapy. If a session ends at 37 minutes, bill 90832. If it reaches 53 minutes, bill 90837. The midpoint that gives 90834 its “45-minute” reputation is just the center of its range—not a requirement. What matters is that your documented time falls between 38 and 52 minutes.
Can I bill 90837 for a 50-minute session? No. A 50-minute session falls squarely in the 38–52 minute range. Billing 90837 requires 53+ minutes. The traditional “50-minute hour” is not a billing threshold—it’s a clinical convention. Billing 90837 for 50-minute sessions is upcoding. Auditors and payer AI systems flag this pattern routinely: if your notes consistently show 50-minute sessions but every claim is 90837, expect a recoupment demand.
What CPT code is used for a 45-minute therapy session? That’s 90834. The code covers sessions from 38 to 52 minutes, and 45 minutes is the natural midpoint. It’s the most frequently billed outpatient mental health code.
How much is CPT 90834 reimbursement? The 2026 Medicare national average is approximately $134.25 in non-facility settings. Geographic GPCI adjustments apply—urban practices in New York or Los Angeles may see $155+, rural practices somewhat less. Commercial payers typically reimburse 130–250% of Medicare, so $175–$335 depending on your contract. NPs billing under their own NPI receive 85%: approximately $114.11.
Documentation that survives audits: Record exact start and stop times (e.g., “Session: 2:05 PM – 2:51 PM, 46 minutes”), the therapeutic modality (CBT, DBT, supportive therapy), specific interventions, patient response, mental status observations, risk assessment, and progress toward treatment goals linked to an ICD-10 diagnosis. Notes that say “client discussed childhood trauma” without specifying modality, goals, or response are audit vulnerabilities.
Telehealth billing for 90832, 90834, 90837: All three codes are telehealth-eligible. Use modifier 95 for synchronous audio-video, modifier 93 or FQ for audio-only, and POS 10 when the patient is at home. More detail in Section 10.
For help ensuring your practice captures every dollar from psychotherapy codes, our mental health billing services are built for this exact revenue cycle.
Add-On Psychotherapy Codes — 90833, 90836, 90838: When and How to Append to E/M
A psychiatrist or PMHNP doing both medication management and psychotherapy in a single visit has two distinct services—and two distinct codes. The add-on psychotherapy codes exist specifically for this. Failing to bill them is walking away from significant revenue.
90833 is psychotherapy, 30 minutes (16–37 minutes), performed with an evaluation and management (E/M) service. The “+” symbol in the CPT manual means it’s an add-on—it must accompany a primary E/M code. 90836 covers 38–52 minutes of psychotherapy with E/M. 90838 covers 53+ minutes.
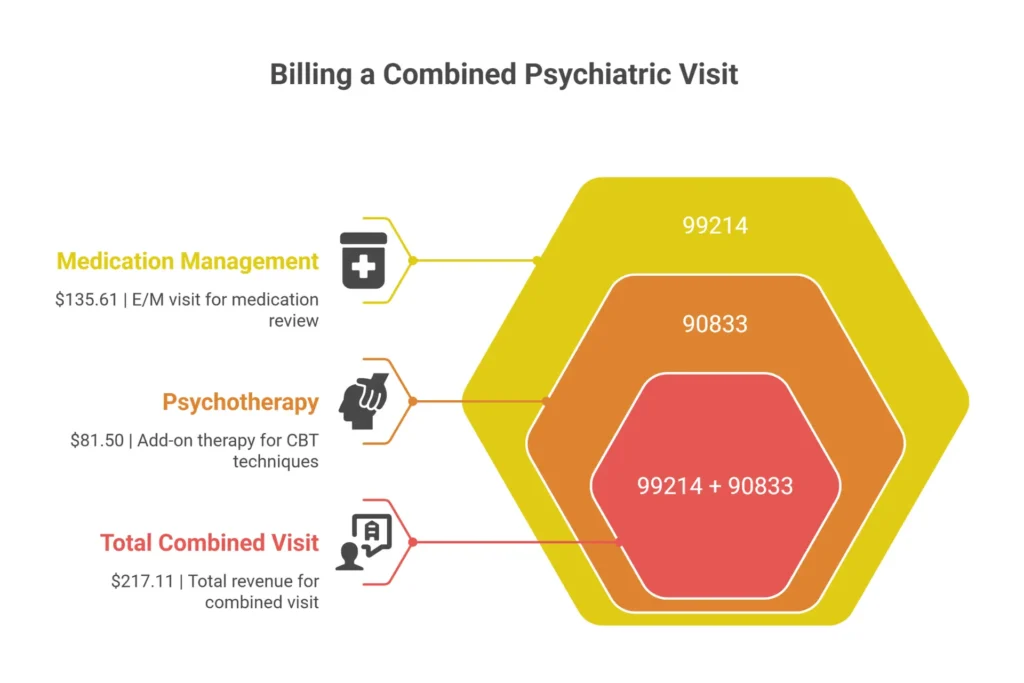
Can CPT code 99214 and 90833 be billed together? Yes. This is the foundational combined-visit scenario. A psychiatric prescriber spends 20 minutes on medication management—reviewing symptoms, adjusting dosage, checking for side effects, updating the medication plan (99214, moderate-complexity E/M). Then spends 20 minutes on CBT techniques targeting the same patient’s depression (90833, 30-minute psychotherapy add-on). Both are documented separately and billed together. Total 2026 Medicare: $135.61 (99214) + $81.50 (90833) = $217.11—versus $172.80 for 90837 alone.
A real example: A psychiatrist sees a patient with bipolar disorder for a 45-minute visit. The first 20 minutes covers medication review, labs, and prescribing decision (99214). The remaining 25 minutes involves structured cognitive behavioral techniques for mood regulation (90833). The note separates both components with distinct time entries and clinical content. The claim has two codes—both paid.
What is the difference between 90832 and 90833? 90832 is standalone 30-minute psychotherapy—used when the session involves only therapy, no E/M. 90833 is the add-on version—used when psychotherapy accompanies an E/M service. You cannot bill both 90832 and an E/M code on the same day. The correct pairing for a combined medication management and therapy visit is the E/M code plus the appropriate add-on (90833, 90836, or 90838).
Can you bill 90833 alone? No, ever. 90833 is designated as an add-on code. Without a primary E/M code, it auto-denies. The primary codes that 90833, 90836, and 90838 require are the office/outpatient E/M codes: 99202–99205 (new patient) and 99212–99215 (established patient).
What does CPT code 90836 mean? 90836 is the 45-minute psychotherapy add-on (38–52 minutes of psychotherapy time) performed alongside an E/M service. It’s appropriate when the therapy portion of a combined visit takes 38–52 minutes. 2026 Medicare: $103.21. With 99214, that’s $238.82 total.
Who can bill these codes: Only prescribing providers—psychiatrists, PMHNPs, PAs. Psychologists, LCSWs, LPCs, and LMFTs cannot bill E/M codes, so they cannot bill add-on codes. They use standalone 90832, 90834, or 90837 instead.
Documentation requirement: The note must clearly separate the E/M component (medication review, MDM, history, ROS) from the psychotherapy component (modality, interventions, patient response, time allocation for therapy). A single blended note that doesn’t distinguish the two invites denial. Structure it as two sections: “Psychiatric Evaluation and Management” and “Psychotherapy.”
For precise documentation review and coding support, our medical coding services include retrospective chart audits and staff training.
Group Therapy and Family Therapy CPT Codes — 90846, 90847, 90849, 90853
These codes shift focus from the individual to relationships. The rules change based on who is in the room—and the per-patient billing mechanics of group therapy catch new providers off guard.
CPT 90853 — Group psychotherapy is for sessions with two to twelve unrelated individuals addressing mental health concerns through group dynamics—peer support, universality, interpersonal learning. Is CPT 90853 billed per patient or per group? Per patient. Always. If eight patients attend, you submit eight separate claims—one for each patient using their own insurance. Billing one claim for the group underbills by 87%. The 2026 Medicare rate is $30.39 per patient. Eight patients at $30.39 = $243.12 for a 60-minute group—more than a single 90837.
Each claim requires individualized documentation: a global group note covering theme, interventions, and total time, plus a patient-specific paragraph documenting that individual’s participation, mood, and progress toward their unique treatment goals. Cloned notes—identical progress paragraphs across all group members—are the top audit trigger for 90853.
CPT 90847 — Family psychotherapy with patient present is conjoint therapy involving the identified patient and family members working through relational dynamics together. Time-based: 26+ minutes required (50-minute session typical). 2026 Medicare rate: $145.60. The patient must actually be in the room (or on the video call).
CPT 90846 — Family psychotherapy without patient present covers collateral sessions—coaching parents, educating a spouse, supporting caregivers—when the identified patient is absent. The session must directly benefit the patient’s treatment. 2026 Medicare rate: $118.75. Common denial pitfall: overuse raises questions about medical necessity. Another denial cause: payers classifying family work as “marriage counseling” under Z63.0, which is often a plan exclusion. Use the patient’s F-code diagnosis as the primary ICD-10 to establish medical necessity.
CPT 90849 — Multiple-family group psychotherapy is for sessions where multiple family units meet together—three sets of parents and their respective children, for example. Common in partial hospitalization and substance use programs. Billed per session, not per family. 2026 Medicare rate approximately $35.00.
Interactive Complexity Add-On Code 90785 — The Most Underused Code in Mental Health
Fewer than 5% of eligible claims include this code. For pediatric, autism, high-conflict, and forensic practices, that gap represents $15,000–$30,000 in uncaptured annual revenue—for work you’re already doing.
CPT 90785 is an add-on for sessions made significantly more complex by communication barriers or third-party dynamics. You append it to the primary code to capture the extra clinical effort those circumstances require.
What are the criteria for billing CPT code 90785? The APA and AMA specify four qualifying factors, and your session must meet at least one:
- Maladaptive communication: High anxiety, hostility, reactivity, or disagreement among participants that requires de-escalation or redirection
- Caregiver emotions or behaviors: Caregiver interference that prevents them from understanding or supporting the treatment plan
- Third-party involvement: Legally authorized representatives (guardians, probation officers, case managers) whose presence requires complex management during the session
- Non-verbal communication tools: Use of play equipment, drawings, tablets, or visual tools for patients who cannot communicate through typical language (children, autism, selective mutism)
Append 90785 to: 90791, 90792, 90832–90838, 90847, 90853. Do not append to: 90846 (no patient present), 90839/90840 (complexity is already built into crisis codes), or E/M codes without psychotherapy.
Documentation must include: which criterion applied, how it affected the session, and what clinical intervention you used. Example: “Interactive complexity present—high parental conflict (criterion 2) prevented patient’s verbal participation; required structured turn-taking and de-escalation over 15 minutes to restore session focus.” Documentation that simply says “session was complex” without specifics will be denied.
2026 Medicare rate: $14.50. Modest per session—but substantial in aggregate. A pediatric practice with 20 eligible sessions per week generates $15,080 annually in add-on revenue. Commercial payers pay $20–$35. For more guidance on this code, the APA psychotherapy code resources provide authoritative criteria.
Crisis Intervention CPT Codes — 90839 and 90840
When a scheduled session becomes a response to imminent danger, the clinical work changes—and so does the code. Crisis codes aren’t for emotionally intense sessions. They’re for acute, life-threatening situations.
CPT 90839 is psychotherapy for crisis, first 60 minutes. It covers 30–74 minutes of face-to-face crisis intervention. CPT 90840 is the add-on for each additional 30 minutes beyond 74 minutes.
Time arithmetic: 30–74 minutes = 90839 only. 75–104 minutes = 90839 + one unit of 90840. 105–134 minutes = 90839 + two units of 90840. Minimum 30 minutes required—a brief 15-minute phone crisis call doesn’t qualify.
What qualifies as a psychiatric crisis for billing? Active suicidal ideation with plan or intent, homicidal ideation, acute psychosis with severe decompensation, grave disability, or imminent hospitalization evaluation. Not sufficient: a patient crying harder than usual, chronic suicidal ideation with no new plan, or intense but manageable distress. The session must involve urgent stabilization—safety planning, de-escalation, mobilizing emergency resources—not routine therapeutic processing.
What is the difference between 90839 and 90837? 90837 is scheduled, recurring psychotherapy for ongoing treatment. 90839 is urgent, often unplanned intervention for imminent risk. The documentation requirements are fundamentally different: 90837 needs progress toward treatment goals; 90839 needs a crisis precipitant, explicit risk statement, MSE, safety intervention, and disposition. You cannot bill both on the same day for the same patient—NCCI edits prohibit it.
Documentation requirements per CMS Local Coverage Article A57480: crisis precipitant, specific risk assessment (suicide/violence screening with documented clinical reasoning), mental status examination, interventions performed (de-escalation, safety plan, contact with ER or family), total time, and disposition. Documentation that references “patient in crisis” without specifics will not survive audit scrutiny.
2026 Medicare rates: 90839 $152.40, 90840 $75.20 per unit. Telehealth: permanent. Use modifier 95 (video) or 93/FQ (audio-only) with POS 10 for home-based sessions.
Health Behavior Assessment and Intervention Codes — 96156, 96158, 96159, 96164, 96165
These codes serve a specific, underused niche: patients with chronic medical conditions who need behavioral support but don’t have a mental health diagnosis. They’re the bridge between behavioral health and primary care.
Critical distinction: Health behavior codes require a primary physical health diagnosis. You’re addressing biopsychosocial factors affecting a medical condition—not treating a psychiatric disorder. A psychologist working with a cancer patient on chemotherapy adherence and nausea coping bills 96158 under C50.9, not 90834 under F41.1.
The codes:
- 96156 — Health behavior assessment or re-assessment (untimed, once per episode). 2026 Medicare: $125.30
- 96158 — Individual intervention, first 30 minutes. $72.40
- 96159 — Individual add-on, each additional 15 minutes. $33.00
- 96164 — Group intervention, first 30 minutes. $50.00
- 96165 — Group add-on, each additional 15 minutes. $18.00
ICD-10 coding requirement: Primary diagnosis must be a physical health code—E11.9 (Type 2 diabetes), I25.10 (coronary artery disease), C50.919 (breast cancer), G89.4 (chronic pain). F-codes are secondary or excluded. Using an F-code as primary triggers psychotherapy billing rules and likely denial.
Who can bill: Psychologists, LCSWs, LPCs, LMFTs—any licensed mental health professional addressing physical health behaviors within scope. These codes bill under the patient’s medical benefit, bypassing behavioral health carve-outs and session caps.
You cannot bill 96158 and 90837 on the same day for the same patient. Choose the code that matches the primary clinical focus: physical health adherence (96158) or mental health treatment (90837).
Collaborative Care Management CPT Codes — 99492, 99493, 99494, and 99484
Collaborative Care (CoCM) is evidence-based, primary care–based behavioral health integration. These are monthly bundled codes—you bill once per month per patient based on total care team time.
The model requires three players: a billing practitioner (PCP, NP, or PA who oversees care and bills the codes), a behavioral health care manager (LCSW, psychologist, RN who tracks patients and delivers brief interventions), and a psychiatric consultant (psychiatrist who reviews the caseload weekly and advises on complex cases without seeing patients directly).
CPT 99492 — Initial psychiatric collaborative care management, first 70 minutes in the initial calendar month. Activities: assessment, care plan, patient outreach, medication reconciliation, registry setup, psychiatric consultation. 2026 Medicare: $165.20
CPT 99493 — Subsequent months, at least 60 minutes. Ongoing monitoring, plan adjustment, psychiatric caseload consultation. $142.80
CPT 99494 — Each additional 30 minutes beyond 99492/99493 threshold (add-on). $71.40
CPT 99484 — General behavioral health integration (BHI), at least 20 minutes per calendar month of non-face-to-face coordination. No psychiatric consultant required. The simpler entry point. $55.60
Documentation requirements: Registry tracking with validated measures (PHQ-9 for depression, GAD-7 for anxiety), monthly summary of care manager time and activities, evidence of psychiatric consultation (documented notes, emails, or call logs), treatment plan with measurable goals.
Note on 99484 vs. 99492/99493: You cannot bill both for the same patient in the same month. If your team has the infrastructure—psychiatric consultant contract, registry, care manager—go with 99492/99493. The revenue difference is significant: $165 vs. $55.
Coverage: Medicare covers fully. Commercial adoption is accelerating—approximately 80% of major commercial plans accept CoCM as of 2026. Medicaid varies by state. Our RCM services include CoCM billing setup and monthly management.
Telehealth Mental Health CPT Codes — Modifiers 95, GT, FQ, and 93 Explained
Telehealth for mental health is permanently extended as of 2026. No geographic restrictions. Home is a valid originating site. Audio-only is covered. The challenge isn’t whether you can bill telehealth—it’s which modifier combination to use.
As of 2026: No in-person visit required before initiating telehealth (waived through 2027). All psychotherapy and evaluation codes are telehealth-eligible. Audio-only is permanently available for mental health with appropriate documentation.
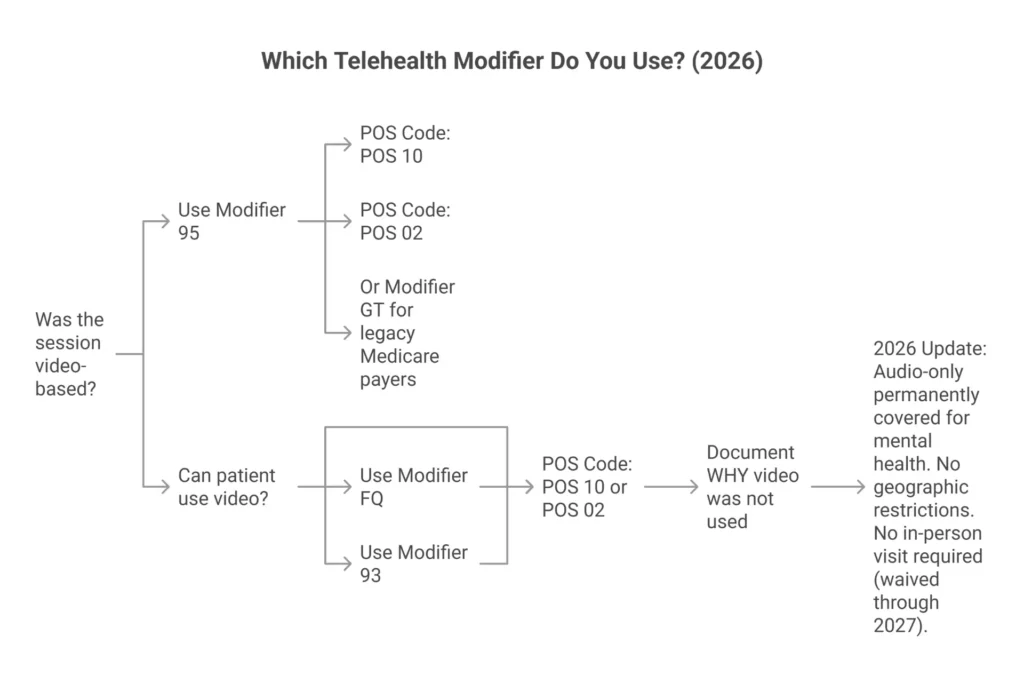
| Modifier | Meaning | When to Use | POS Code |
|---|---|---|---|
| 95 | Synchronous telehealth, audio-video | Most video sessions; standard for commercial and Medicare | POS 10 (home) or 02 (elsewhere) |
| GT | Interactive audio-video (legacy) | Some commercial payers still prefer this; Medicare accepts | Varies by payer |
| FQ | Audio-only (PHE context) | Medicare audio-only when patient can’t or won’t use video | POS 02 |
| 93 | Audio-only telephone (CMS 2026) | Ongoing audio therapy when video isn’t feasible | POS 10 or 02 |
What is the difference between POS 02 and POS 10? POS 10 means the patient is receiving telehealth at home—this pays the higher non-facility rate. POS 02 means the patient is receiving telehealth from any other location (clinic, school, office). The payment difference is roughly 5–10% per claim. For most outpatient mental health telehealth, POS 10 is correct and pays more.
Can therapists bill for phone-only sessions? Yes. Use standard CPT codes (90832–90837, 90791) with modifier 93 (for ongoing audio therapy in 2026) or modifier FQ (Medicare, PHE context). Document why video wasn’t used (patient technology barriers, patient refusal of video, documented in the note) and patient’s consent to audio-only treatment. Missing this documentation is a top denial cause for audio-only claims.
Documentation for all telehealth: Patient location (home, confirmed), start/stop times, technology platform (Doxy.me, Zoom for Healthcare, SimplePractice—HIPAA-compliant platforms only), and consent for telehealth on file.
For telehealth authorization and payer eligibility verification before sessions, our insurance eligibility service confirms telehealth coverage in real time.
Psychiatric NP Billing Codes — 99213, 99214, 99204, 99205 and How PMHNPs Bill
PMHNPs are the only mental health providers who can wear both hats: prescriber and therapist. That flexibility creates complexity in code selection.
Code decision matrix for PMHNPs:
- New patient with prescribing → 90792
- Established patient, medication management only → 99213 (low complexity, 20–29 min) or 99214 (moderate, 30–39 min)
- Established patient, medication management + psychotherapy → 99214 + 90833 (or 90836/90838 depending on therapy time)
- Psychotherapy only → 90834 or 90837
What are billing codes for psychiatric nurse practitioners? PMHNPs use: 90792 (initial psychiatric evaluation with medical services), 99213–99215 (established patient E/M for medication management), 99204–99205 (new patient E/M), 90832–90837 (standalone psychotherapy), and 90833/90836/90838 (psychotherapy add-ons to E/M).
Can a psychiatric nurse practitioner bill 90792? Yes. PMHNPs with prescriptive authority enrolled with Medicare and commercial payers can bill 90792 independently. Documentation must include medical services: medication review, prescribing decision, any physical assessment elements. 2026 Medicare rate at 85%: approximately $171.77.
What is the difference between 90791 and 90792? 90791 is evaluation without medical services (therapists and non-prescribers). 90792 includes medical services—prescribing, lab review, physical assessment. PMHNPs doing initial evaluations with medication management should use 90792. Using 90791 when you prescribed is downcoding.
The 85% Medicare rule: NPs billing under their own NPI receive 85% of the physician fee schedule. Example: 99214 pays physicians $135.61; NPs receive $115.27. To receive 100%, use incident-to billing—but requirements are strict: the physician must have established the care plan, the physician must be immediately available (virtual supervision is acceptable in 2026), and no new problems can be addressed.
2026 NP Medicare rates:
| CPT | Physician Rate | NP Rate (85%) |
|---|---|---|
| 99213 | $95.19 | $80.91 |
| 99214 | $135.61 | $115.27 |
| 99215 | $188.42 | $160.16 |
| 99204 | $177.36 | $150.76 |
| 99205 | $236.81 | $201.29 |
| 90792 | $202.08 | $171.77 |
State scope of practice matters: 27 states including New York, Washington, Colorado, and Massachusetts grant full practice authority—PMHNPs bill independently without physician oversight. Reduced and restricted states require collaborative agreements or supervision. Our credentialing services help navigate state-specific enrollment requirements.
Mental Health Billing Modifier Codes — GT, 95, HO, HN, HE, U1-U9 Explained
Modifiers are a two-character instruction set that tells payers who delivered the service, how it was delivered, and whether something unusual applies. Missing a required modifier means a denied claim.
Telehealth modifiers (covered in depth in Section 10): 95 (synchronous audio-video, standard), GT (legacy interactive audio-video), FQ (Medicare audio-only PHE context), 93 (audio-only 2026).
Medicaid credential modifiers (HCPCS Level II) are state-required indicators of the provider’s degree level or program type. Medicare doesn’t require them, but many state Medicaid programs will deny without them:
- HO — Master’s degree level clinician. Required by California, Illinois, and Missouri Medicaid for LCSWs, LPCs, LMFTs billing psychotherapy. Append to the CPT code: 90837-HO.
- HN — Bachelor’s degree level clinician. Used in Texas and Illinois for tiered reimbursement.
- HE — Mental health program indicator. Required by Colorado and Missouri to distinguish mental health from substance abuse services.
- HF — Substance abuse program. Required in Texas, Georgia, and North Carolina for SUD billing.
- U1–U9 — State-specific modifiers (Ohio, Missouri, others) indicating provider credential, supervision level, or treatment intensity. Ohio uses U4 for LSW, U5 for LMFT, U9 for Licensed Psychologist. Meanings vary by state—always verify your state Medicaid manual.
CPT modifiers:
- Modifier 25 — Required when an E/M service (99214) is billed on the same day as another procedure (90833, 96127). Append to the E/M code to signal it was significant and separately identifiable from the procedure. Missing modifier 25 causes bundling—the procedure gets paid, the E/M doesn’t.
- Modifier 52 — Reduced services. When a session is cut short—patient left early, acute symptom interruption—document why the full session wasn’t completed.
- Modifier 22 — Unusual procedural services requiring substantially more work. For crisis sessions with interpreters or extraordinary complexity.
The Medicare vs. Medicaid distinction on modifiers is critical: Medicare typically doesn’t require HO/HN credential modifiers, but Medicaid programs in most states do. Maintain separate billing profiles and modifier checklists per payer type.
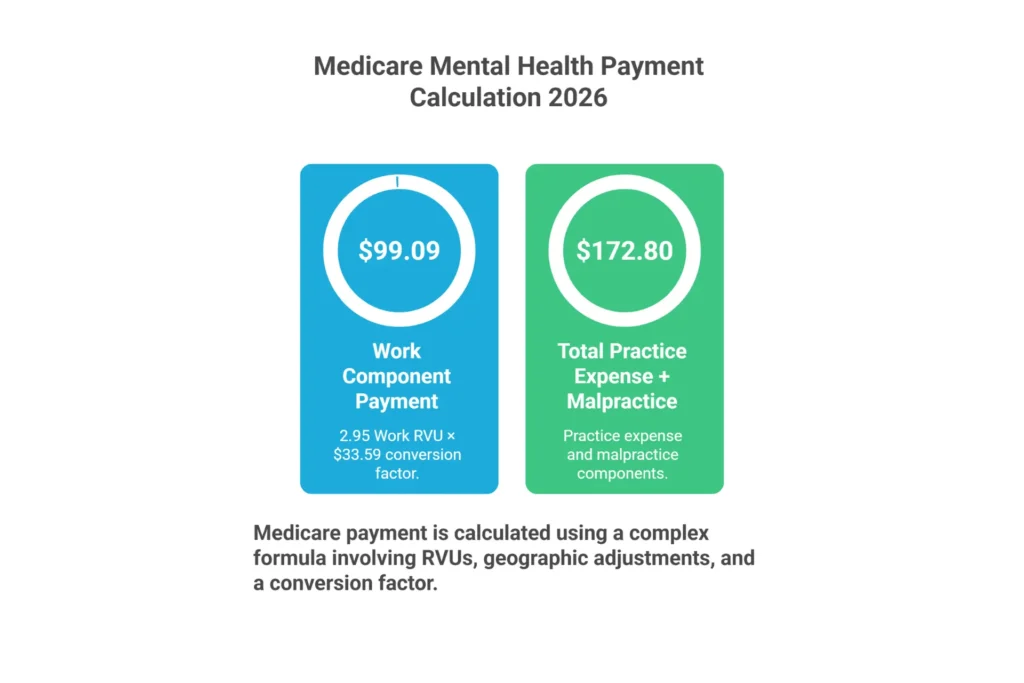
2026 Medicare Reimbursement Rates for Mental Health CPT Codes
Medicare rates are calculated using the RBRVS formula: (Work RVU × GPCI_work + Practice Expense RVU × GPCI_PE + Malpractice RVU × GPCI_MP) × Conversion Factor. The 2026 conversion factor is $33.59, a 3.7% increase from 2025’s $32.35. Rates below are national non-facility averages—actual payment varies by geographic GPCI location.
Commercial payers typically reimburse 120–250% of Medicare. Use these rates as a negotiation floor: if a commercial payer is offering less than 120% of current-year Medicare for a code, you’re being underpaid and have documented grounds to renegotiate. Medicaid rates vary significantly by state—California’s 90837 rate is approximately $180, Texas approximately $140.
| CPT Code | Description | Time | 2026 Medicare Rate | Telehealth Eligible? |
|---|---|---|---|---|
| 90791 | Psych diagnostic eval w/o medical | Untimed | $174.50 | Yes |
| 90792 | Psych diagnostic eval w/ medical | Untimed | $202.08 | Yes |
| 90832 | Psychotherapy 30 min | 16–37 min | $92.15 | Yes |
| 90833 | Psychotherapy add-on 30 min w/ E/M | 16–37 min | $81.50 | Yes |
| 90834 | Psychotherapy 45 min | 38–52 min | $134.25 | Yes |
| 90836 | Psychotherapy add-on 45 min w/ E/M | 38–52 min | $103.21 | Yes |
| 90837 | Psychotherapy 60 min | 53+ min | $172.80 | Yes |
| 90838 | Psychotherapy add-on 60 min w/ E/M | 53+ min | $125.45 | Yes |
| 90839 | Crisis psychotherapy, first 60 min | 30–74 min | $152.40 | Yes |
| 90840 | Crisis add-on, each additional 30 min | +30 min | $75.20 | Yes |
| 90785 | Interactive complexity add-on | N/A | $14.50 | Yes |
| 90846 | Family therapy without patient | Untimed | $118.75 | Yes |
| 90847 | Family therapy with patient | 26+ min | $145.60 | Yes |
| 90853 | Group psychotherapy (per patient) | Per patient | $30.39 | Yes |
| 99213 | Office E/M established, low | 20–29 min | $95.19 | Yes |
| 99214 | Office E/M established, moderate | 30–39 min | $135.61 | Yes |
| 99492 | CoCM initial month | 70 min | $165.20 | No |
| 99493 | CoCM subsequent month | 60 min | $142.80 | No |
| 99484 | General BHI | 20+ min | $55.60 | No |
To look up your exact GPCI-adjusted rates, use the CMS Medicare Physician Fee Schedule lookup tool with your locality code. A psychiatrist in Manhattan may see 90837 at ~$195; a therapist in rural Wyoming may see ~$155 for the same service.
If commercial payers are consistently paying below these benchmarks, our denial management services include underpayment identification and payer dispute support.
Most Common Mental Health CPT Code Billing Errors and How to Avoid Them

Mental health claims deny at 15–20%—more than double the rate of general medical claims. Most of these denials are preventable.
Error #1: Time-code mismatch
What it is: Billing 90837 for sessions under 53 minutes.
Why it happens: Therapists round up from 50-minute sessions out of habit.
Financial impact: Audit recoupment of $38 per session (difference between 90837 and 90834); pattern flagging of all prior claims.
Prevention: Document exact start/stop times. Build EHR reminders showing midpoint thresholds: under 37 min = 90832, 38–52 min = 90834, 53+ min = 90837.
Error #2: Add-on code standalone billing
What it is: Submitting 90833, 90836, or 90838 without a primary E/M code.
Why it happens: Misunderstanding of add-on code requirements.
Financial impact: 100% denial—$81.50–$125.45 lost per claim.
Prevention: Pre-submission checklist: Is a primary E/M code on this claim? Is the billing provider a prescriber? Both must be true before submitting add-on codes.
Error #3: Medical necessity documentation gaps
What it is: Notes lacking ICD-10 linkage, treatment goals, interventions, or patient response.
Why it happens: Template fatigue, copy-paste habits, time pressure.
Financial impact: Audit recoupment of all related claims, sometimes spanning multiple years.
Prevention: Structured templates requiring: diagnosis → functional goal → intervention → response → plan. Random monthly audit of 10% of notes. Review CMS Article A57480 for documentation expectations.
Error #4: Modifier errors
What it is: Missing modifier 95 on telehealth claims, wrong POS code, missing HO on Medicaid.
Why it happens: Payer-specific modifier requirements vary and aren’t centralized.
Financial impact: 100% denial until corrected—often requiring resubmission and timely filing risk.
Prevention: Maintain a payer-specific modifier matrix. Automate EHR flags for modifier requirements by payer and service type.
Error #5: Group therapy per-group billing
What it is: Billing one unit of 90853 for a 10-patient group instead of 10 claims.
Why it happens: New providers assume group = one claim.
Financial impact: 90% underpayment—billing $30.39 instead of $303.90 for the same session.
Prevention: Bill per patient. Maintain signed attendance roster. Individual patient-specific paragraphs in group notes.
Error #6: 90791/90792 frequency overuse
What it is: Billing psychiatric evaluation codes more frequently than payer allows.
Why it happens: Not tracking last evaluation date per patient per payer.
Financial impact: Second evaluation denied; if pattern found on audit, all evals reviewed.
Prevention: EHR flag on last evaluation date. Justify re-evaluations with new episode documentation.
Error #7: Credentialing and eligibility lapses
What it is: Billing payers before effective credentialing date or after enrollment expiration.
Why it happens: Credentialing timelines are long and expiration dates easy to miss.
Financial impact: 100% denial for all claims during lapse period with no appeal rights.
Prevention: Real-time eligibility verification before every session. Credentialing expiration calendar with 90-day advance alerts.
Error #8: Timely filing violations
What it is: Submitting claims after the payer’s filing deadline (Medicare: 12 months; most commercial: 90–180 days).
Why it happens: Claims get stuck in a queue, rejected for unrelated reasons, then forgotten.
Financial impact: 100% denial with no recovery option.
Prevention: Submit within 48 hours of service. Weekly aging reports to identify stalled claims approaching deadlines.
If your practice is seeing denial rates above 5%, our denial management services can identify the systemic cause and get revenue flowing. The Quick Reference Table below consolidates every code—bookmark it as your daily companion.
Complete Mental Health CPT Codes Quick-Reference Table 2026
Use this table when you need a fast answer at the point of billing. All rates are 2026 national Medicare non-facility averages before GPCI adjustment. Commercial rates typically range 120–250% of Medicare. NP rates are 85% of the listed rates when billing under own NPI.
For a downloadable PDF version of this table—formatted for printing with additional documentation tips and an audit-proof phrase bank for crisis and interactive complexity documentation
📄 Free Download: 2026 Mental Health CPT Codes Cheat Sheet
Formatted for printing · 27 codes · 2026 Medicare rates · Telehealth modifiers · Audit-proof documentation phrase bank for 90785 and 90839
⬇ Download Free PDFFree for all mental health providers. No sign-up required.
| CPT Code | Plain-English Description | Time/Duration | Provider Types | 2026 Medicare Rate | Telehealth Modifiers |
|---|---|---|---|---|---|
| 90791 | Psychiatric evaluation (no medications) | Untimed | LCSW, LPC, LMFT, Psychologist, Psychiatrist | $174.50 | 95, 93 |
| 90792 | Psychiatric evaluation (with medications) | Untimed | Psychiatrist, PMHNP | $202.08 | 95 |
| 90832 | Therapy session, 30 min | 16–37 min | All licensed MH providers | $92.15 | 95, 93 |
| 90833 | Therapy add-on 30 min (with med management) | 16–37 min | Psychiatrist, PMHNP | $81.50 | 95 |
| 90834 | Therapy session, 45 min | 38–52 min | All licensed MH providers | $134.25 | 95, 93 |
| 90836 | Therapy add-on 45 min (with med management) | 38–52 min | Psychiatrist, PMHNP | $103.21 | 95 |
| 90837 | Therapy session, 60 min | 53+ min | All licensed MH providers | $172.80 | 95, 93 |
| 90838 | Therapy add-on 60 min (with med management) | 53+ min | Psychiatrist, PMHNP | $125.45 | 95 |
| 90839 | Crisis intervention, first 60 min | 30–74 min | All licensed MH providers | $152.40 | 95, 93 |
| 90840 | Crisis add-on, each additional 30 min | +30 min | All licensed MH providers | $75.20 | 95, 93 |
| 90785 | Interactive complexity (add-on) | N/A | All licensed MH providers | $14.50 | 95 |
| 90846 | Family therapy (patient absent) | Untimed | All licensed MH providers | $118.75 | 95 |
| 90847 | Family therapy (patient present) | 26+ min | All licensed MH providers | $145.60 | 95 |
| 90849 | Multiple-family group | Untimed | All licensed MH providers | $35.00 | 95 |
| 90853 | Group therapy (per patient) | Untimed | All licensed MH providers | $30.39 | 95 |
| 96156 | Health behavior assessment | Untimed | Psychologist, LCSW, LPC, LMFT | $125.30 | 95 |
| 96158 | Health behavior intervention, first 30 min | 30 min | Psychologist, LCSW, LPC, LMFT | $72.40 | 95 |
| 96159 | Health behavior intervention, add-on 15 min | +15 min | Psychologist, LCSW, LPC, LMFT | $33.00 | 95 |
| 99213 | Medication management, low complexity | 20–29 min | Psychiatrist, PMHNP | $95.19 | 95 |
| 99214 | Medication management, moderate complexity | 30–39 min | Psychiatrist, PMHNP | $135.61 | 95 |
| 99204 | New patient E/M, moderate complexity | 45–59 min | Psychiatrist, PMHNP | $177.36 | 95 |
| 99205 | New patient E/M, high complexity | 60–74 min | Psychiatrist, PMHNP | $236.81 | 95 |
| 99492 | Collaborative care, initial month | 70 min/month | Primary care MD/NP/PA | $165.20 | No |
| 99493 | Collaborative care, subsequent month | 60 min/month | Primary care MD/NP/PA | $142.80 | No |
| 99494 | Collaborative care add-on, 30 min | +30 min | Primary care MD/NP/PA | $71.40 | No |
| 99484 | General behavioral health integration | 20+ min/month | Primary care MD/NP/PA | $55.60 | No |
Want to keep this at your desk all year? Download the free 2026 Mental Health CPT Codes PDF Cheat Sheet—includes this full table formatted for printing, plus documentation tips, modifier legend, and an audit-proof phrase bank for 90785 and 90839.
🖨️ Want to Keep This at Your Desk All Year?
Download the free 2026 Mental Health CPT Codes PDF Cheat Sheet — includes this full table formatted for printing, plus a documentation tips guide, modifier legend, and an audit-proof phrase bank for 90785 and 90839.
⬇ Download Free PDF →PDF · Free · No sign-up required · Optimized for printing
Frequently Asked Questions About Mental Health CPT Codes
What is the difference between CPT codes 90832, 90834, and 90837?
All three are individual psychotherapy codes distinguished solely by session length. CPT 90832 covers 16–37 minutes (the 30-minute code). CPT 90834 covers 38–52 minutes (the standard 45-minute code). CPT 90837 covers 53 minutes or longer (the 60-minute code). You bill the code whose time range matches your documented face-to-face session time. The AMA midpoint rule means you must meet the lower threshold of each range to bill that code.
Can I bill CPT 90791 and 90837 on the same day?
Yes, if the services are clinically distinct and separately documented. The evaluation (90791) establishes the patient’s diagnosis and treatment plan. The therapy session (90837) provides separate therapeutic work with its own clinical content, interventions, and time. Document each independently with different clinical focus and time allocation. No NCCI edit prohibits this pairing, but auditors will scrutinize same-day billing—ensure each note stands completely on its own.
Can I bill 90837 for a 50-minute session?
No. A 50-minute session falls within the 38–52 minute range and must be billed as CPT 90834. CPT 90837 requires 53 minutes or more of face-to-face psychotherapy. The traditional “50-minute therapy hour” is a clinical convention, not a billing threshold. Billing 90837 for 50-minute sessions constitutes upcoding and triggers audit risk. Always document exact start and stop times.
What is the difference between 90791 and 90792?
The distinction is medical services. CPT 90791 is a psychiatric diagnostic evaluation without medical services—used by non-prescribing providers (LCSWs, LPCs, LMFTs, psychologists) for comprehensive intake assessments when no medication management or prescribing occurs. CPT 90792 includes medical services such as medication review, prescribing, physical exam elements, or lab orders—used only by psychiatrists and PMHNPs. CPT 90792 reimburses approximately $27 more than 90791.
Can a psychiatric NP bill CPT 90792?
Yes. Psychiatric Nurse Practitioners with prescriptive authority and Medicare enrollment can bill 90792 independently for comprehensive psychiatric evaluations that include medical services. Documentation must include medication review, prescribing rationale, and any physical assessment components. When billing under their own NPI, NPs receive 85% of the physician rate—approximately $171.77 in 2026.
What CPT code should I use for a 45-minute therapy session?
Use CPT 90834, which covers sessions lasting 38 to 52 minutes. The code is commonly called the “45-minute therapy code” because 45 minutes falls in the center of its time range. All licensed mental health providers can bill 90834 for face-to-face or telehealth individual psychotherapy. Document exact start and stop times.
Can CPT code 99214 and 90833 be billed together?
Yes. This is the standard combined medication management and psychotherapy visit for prescribers. CPT 99214 covers the E/M component (medication review, MDM). CPT 90833 covers 16–37 minutes of separately documented psychotherapy. Both components need distinct documentation. Append modifier 25 to 99214 if your payer requires it. Total 2026 Medicare value: approximately $217.
Can you bill 90833 without an E/M code?
No. CPT 90833 is an add-on code (marked with “+” in the CPT manual) and requires a primary E/M code (99202–99205 for new patients, 99212–99215 for established patients). Submitting 90833 without a primary E/M results in immediate automatic denial. Only psychiatrists, PMHNPs, and PAs can bill 90833 because only they can bill the required primary E/M.
What is the difference between 90833 and 90832?
CPT 90832 is standalone 30-minute individual psychotherapy—used when the session involves only therapy, no medication management. CPT 90833 is the add-on version of 30-minute psychotherapy—used only when psychotherapy is performed alongside a separate E/M service in the same visit. The two cannot be used interchangeably: 90832 is for therapists in therapy-only sessions; 90833 is for prescribers in combined med management and therapy visits.
What billing codes do psychiatric nurse practitioners use?
PMHNPs use: 90792 for initial psychiatric evaluations with medical services; 99213–99215 for established patient medication management; 99204–99205 for new patient visits; 90832–90837 for standalone psychotherapy sessions; and 90833/90836/90838 as add-on codes to E/M when combining medication management with psychotherapy in the same visit.
What CPT code is used for group therapy?
CPT 90853 is the standard group psychotherapy code. The most important billing rule: it’s billed per patient, not per group. If 10 patients attend, you submit 10 separate claims—one per patient using their individual insurance. The 2026 Medicare rate is $30.39 per patient. Each claim requires individualized documentation of that patient’s participation and response.
What is the difference between 90839 and 90837?
CPT 90837 is routine 60-minute individual psychotherapy for scheduled, ongoing mental health treatment. CPT 90839 is crisis psychotherapy—urgent intervention for patients experiencing imminent risk of harm, acute psychosis, grave disability, or life-threatening psychiatric emergencies. 90839 requires crisis-specific documentation (risk assessment, safety planning, disposition) and cannot be billed on the same day as 90837 per NCCI edits.
What is the 50-minute rule for 90837?
There is no 50-minute rule for 90837. The threshold is 53 minutes. Sessions ending at 50 minutes must use 90834. The confusion stems from the traditional “50-minute therapy hour,” but CPT time ranges are absolute: 38–52 minutes = 90834, 53 or more minutes = 90837. Rounding up from 50 to qualify for 90837 is upcoding.
Can interns or trainees bill CPT codes?
Interns and pre-licensed trainees can bill through incident-to billing under a supervising licensed provider. Three requirements must be met: the supervisor established the initial treatment plan, the supervisor is immediately available during the session (virtual supervision is acceptable in 2026), and services are within the intern’s scope. Document supervisor availability in every note. Independent billing requires full licensure.
What modifier is required for telehealth therapy in 2026?
Use modifier 95 for video-based sessions (synchronous audio-video) with most commercial payers, Medicaid, and Medicare. For audio-only sessions, use modifier 93 (CMS 2026 standard for ongoing audio therapy) or modifier FQ (Medicare, PHE context). Always pair with POS 10 if the patient is receiving telehealth at home—this pays the higher non-facility rate.
Can 90846 and 90847 be billed in the same week?
Yes, as long as both services are medically necessary and separately documented. 90847 (family therapy with patient present) and 90846 (collateral session without patient) serve different clinical purposes. However, frequent use of 90846 without corresponding 90847 may raise questions about why the identified patient is consistently excluded from their own family treatment.
Your Mental Health Billing Shouldn’t Be This Hard
Mental health CPT codes are intricate, payer rules shift annually, and a single documentation gap can turn a clean claim into a denial—or an audit. You’ve done the clinical work. Getting paid for it accurately and consistently is a systems problem, not a personal failing.
Elite Med Financials is a specialized mental health billing company. We handle coding, claim submission, denial management, and appeals so your practice captures every dollar it earns. Our clients achieve 98%+ clean claim rates and measurably faster payment cycles.
We’ll review your last 10 claims, identify missed revenue and coding errors, and show you exactly where money is leaking—at no cost. Or call us directly: +1 (307) 243-8064

