Wound care coding isn’t like other medical billing. One wrong digit in a debridement code—billing 11044 when you should have used 97597—and you’re looking at audit flags, clawbacks, and denial rates that can cripple your revenue cycle.
Here’s the reality: wound care billing codes are responsible for more claim denials and compliance issues than almost any other specialty. Between depth-based surgical debridement (11042-11047), selective wound management (97597-97598), and the maze of ICD-10 diagnosis codes (L89, L97, E11.621), the margin for error has completely vanished.
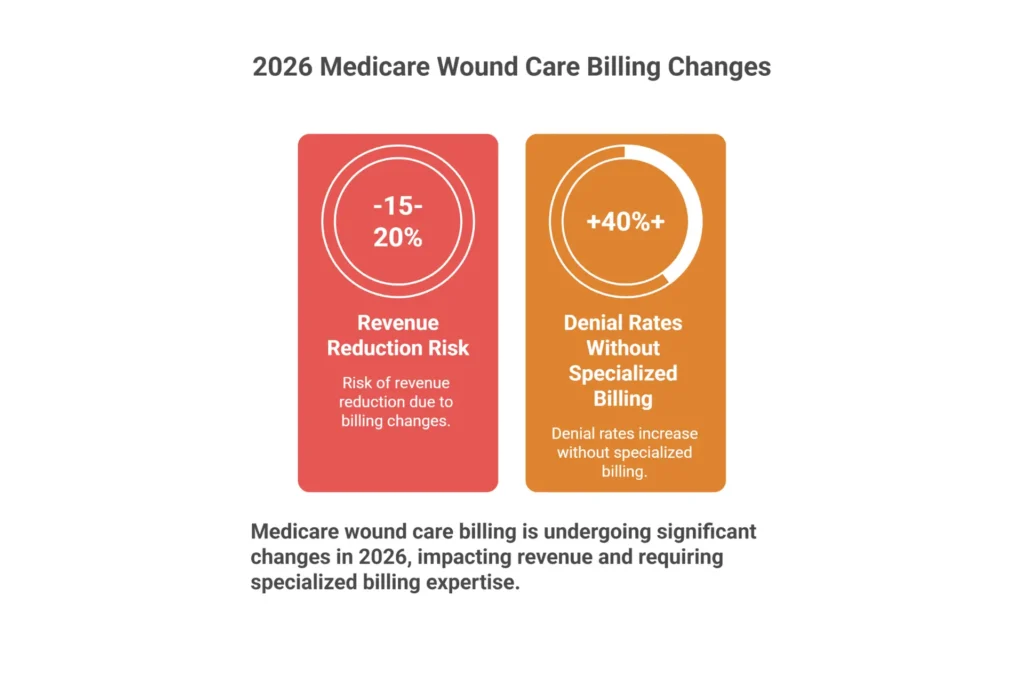
And 2026 made everything harder. The new Medicare skin substitute flat-rate payments, increased OIG scrutiny on debridement coding, and MAC-specific LCD requirements mean the old “close enough” approach to wound care coding no longer works.
This guide breaks down every wound care CPT code, ICD-10 diagnosis code, and Medicare compliance requirement you need to know. Whether you’re a coder looking to sharpen your skills, a practice manager trying to reduce denials, or a clinician who wants to understand why documentation matters—this is your complete reference.
Bookmark this page. You’ll be coming back to it.
Table of Contents
What Are Wound Care Billing Codes?

Wound care billing codes are the specialized CPT, ICD-10, and HCPCS codes used to report wound treatment procedures and establish medical necessity for reimbursement. Unlike general medical coding, wound care coding requires precision across three interconnected code sets that must work together perfectly—or claims get denied.
Here’s why wound care coding is uniquely challenging:
Three Code Sets Working Together
Every wound care claim requires codes from multiple systems:
- CPT codes (97597-97598, 11042-11047, 15271-15278) describe WHAT procedure was performed
- ICD-10 codes (L89.xxx, L97.xxx, E11.621) describe WHY treatment was medically necessary
- HCPCS codes (Q4101, A6021, E2402) describe WHICH supplies and equipment were used
Miss one element—or sequence them incorrectly—and the claim fails.
Depth-Based Coding Complexity
The surgical debridement codes (11042-11047) are based on the deepest tissue layer removed, not the wound depth itself. This single distinction causes more audit problems than any other coding issue in wound care. We’ll cover this in detail in the CPT codes section.
Diagnosis Specificity Requirements
ICD-10 wound codes demand anatomic site, laterality, AND severity/stage. Using unspecified codes (ending in 9) when documentation supports specific codes triggers denials and leaves money on the table.
Payer-Specific Rules
Medicare’s Local Coverage Determinations (LCDs) vary by MAC region. A wound care claim that gets paid in Texas might get denied in California using identical coding—because the LCD requirements differ.
Mastering wound care coding and billing means understanding not just what codes exist, but how they interact, when to use each one, and what documentation supports each selection.
→ Not sure if your current billing setup is optimized? Get a free revenue leakage assessment
Why Specialized Wound Care Billing Matters
Let me paint you a picture that happens every single day in practices across the country.
Your biller—who’s actually pretty good at general medical coding—is looking at a debridement note. The physician documented: “Debrided necrotic tissue from left heel wound, down to bone exposure.”
The biller, applying perfectly logical reasoning, selects CPT 11044 for bone debridement. After all, the note says “down to bone,” right?
Wrong. And this mistake just triggered an audit flag.
If the clinician removed biofilm and necrotic tissue from the surface of exposed bone but didn’t actually excise cortical bone tissue itself, that’s not 11044. That’s 97597 or 97598 for selective debridement. Billing 11044 when the documentation describes wound depth rather than tissue removal depth is textbook upcoding—the kind auditors actively hunt.
This is the kind of coding error that happens every day—and it’s why wound care billing codes require specialized knowledge.
The 2026 regulatory environment has fundamentally changed the game:
| Regulatory Change | What It Means for Your Practice |
|---|---|
| Skin substitute flat-rate payment ($127.14/cm²) | High-cost grafts that exceed this rate now lose money on every application |
| 2.5% efficiency reduction to non-time-based work RVUs | Your debridement payments just got cut |
| Dual conversion factors (APM vs. non-APM) | 3.8% gap based on your participation status |
| Increased OIG skin substitute scrutiny | $10 billion in 2024 spending means audits are coming |
These coding complexities explain why wound care claims have denial rates 2-3x higher than general medical claims. Without deep knowledge of wound care CPT codes and their documentation requirements, even experienced coders make costly mistakes.
The good news? Once you understand the principles—especially the depth rule for debridement and the sequencing rules for ICD-10—these codes become manageable. The rest of this guide breaks down exactly what you need to know.
Quick Knowledge Check: Can you explain the difference between billing 11044 vs. 97597 when bone is visible in a wound? If that question makes you pause, keep reading—we cover this in detail below.
The Complete Wound Care Code System: How CPT, ICD-10, and HCPCS Work Together

Understanding wound care billing codes requires seeing how the three code systems connect. Here’s how each piece fits together:
CPT Codes: What Procedure Was Performed
CPT codes tell payers exactly what treatment you provided. In wound care, these fall into four main categories:
Active Wound Care (97597-97610)
- Selective debridement of devitalized tissue
- Negative pressure wound therapy (NPWT)
- Non-selective debridement techniques
Surgical Debridement (11042-11047)
- Excisional debridement by tissue depth
- Coded by deepest tissue REMOVED (critical distinction)
- Add-on codes for wounds exceeding 20 sq cm
Skin Substitute Application (15271-15278)
- Application procedure codes (separate from product)
- Anatomic site determines code selection
- Size thresholds at 25 sq cm and 100 sq cm
Evaluation & Management (99202-99215)
- Often billed with wound care procedures
- Modifier 25 required for separate E/M on same day
ICD-10 Codes: Why Treatment Was Necessary
ICD-10 diagnosis codes establish medical necessity. Without proper diagnosis coding, even perfectly coded procedures get denied.
Pressure Ulcers (L89.xxx)
- Six-character codes specifying site, laterality, and stage
- Stage must match current wound status (not historical)
Diabetic Ulcers (E10.xxx, E11.xxx)
- Diabetes code sequenced FIRST as primary diagnosis
- Ulcer manifestation code follows as secondary
Chronic Ulcers (L97.xxx)
- Lower extremity ulcers with severity indicators
- Six characters required for full specificity
HCPCS Codes: What Supplies and Equipment Were Used
HCPCS codes capture supplies, drugs, and equipment not covered by CPT.
Q-Codes for Skin Substitutes
- Q4101-Q4255 for specific products
- Now reimbursed at flat rate ($127.14/cm²) for most products
A-Codes for Dressings
- A6021-A6233 for wound dressings by type
- Quantity and size documentation required
E-Codes for Equipment
- E2402 for NPWT pumps and supplies
- Rental vs. purchase distinctions apply
The Connection That Makes or Breaks Claims
A complete wound care claim requires all three elements aligned:
| Element | Example | Purpose |
|---|---|---|
| CPT | 11043 (muscle debridement) | What was done |
| ICD-10 | L89.154 (Stage 4 sacral pressure ulcer) | Why it was necessary |
| HCPCS | A6021 (collagen dressing) | What supplies were used |
If the ICD-10 code indicates a Stage 2 ulcer but the CPT code is for muscle-depth debridement, the claim gets denied—the diagnosis doesn’t support that level of treatment.
This alignment is what separates clean claims from denials.
→ Need expert wound care coding support? Explore our medical coding services
Wound Care CPT Codes: Complete Reference Guide [2026]

If you only master one thing about wound care billing, let it be this: CPT codes are not interchangeable, and using the wrong one isn’t a minor error—it’s revenue loss and potential compliance exposure.
Active Wound Care Codes (97597-97610)
| CPT Code | Description | Billing Unit | Key Considerations |
|---|---|---|---|
| 97597 | Active debridement, first 20 sq cm | Per wound, per session | Selective removal—biofilm, slough without going to surgical depth |
| 97598 | Active debridement, each additional 20 sq cm | Add-on to 97597 | Cannot be billed without 97597 primary |
| 97602 | Non-selective debridement | Per session | Wet-to-dry, whirlpool—rarely covered separately |
| 97605 | NPWT, durable pump, ≤50 sq cm | Per session | Facility setting, reusable equipment |
| 97606 | NPWT, durable pump, >50 sq cm | Per session | Size threshold documentation critical |
| 97607 | NPWT, disposable pump, ≤50 sq cm | Per session | Home care, single-use systems |
| 97608 | NPWT, disposable pump, >50 sq cm | Per session | Size threshold documentation critical |
Surgical Debridement Codes (11042-11047)
| CPT Code | Description | Critical Rule |
|---|---|---|
| 11042 | Subcutaneous tissue, first 20 sq cm | Deepest tissue removed—not wound depth |
| 11043 | Muscle/fascia, first 20 sq cm | Must document muscle tissue excision |
| 11044 | Bone, first 20 sq cm | Requires actual bone removal—not just exposure |
| 11045 | Add-on for 11042 | Each additional 20 sq cm |
| 11046 | Add-on for 11043 | Each additional 20 sq cm |
| 11047 | Add-on for 11044 | Each additional 20 sq cm |
Skin Substitute Application Codes (15271-15278)
| CPT Code | Description | Application |
|---|---|---|
| 15271 | Trunk/arms/legs, first 25 sq cm, ≤100 sq cm total | Application only—product billed separately |
| 15272 | Each additional 25 sq cm, ≤100 sq cm total | Add-on code |
| 15273 | Trunk/arms/legs, first 100 sq cm, >100 sq cm total | Large wound threshold |
| 15274 | Each additional 100 sq cm | Add-on for large wounds |
| 15275 | Face/scalp/eyelids/hands/feet/genitalia, first 25 sq cm | Premium anatomic sites |
| 15276-15278 | Additional units and large wound variants | Site-specific add-ons |
The Depth Rule That Causes Most Audit Problems
Code based on the deepest layer of tissue REMOVED—not the depth of the wound itself.
This single principle causes more coding errors than everything else combined. If a wound tunnels to bone but the physician only debrided subcutaneous tissue, you bill 11042. If you bill 11044 because bone was visible in the wound—but no bone tissue was actually excised—that’s upcoding. It’s the distinction between visualizing bone and removing bone with a rongeur.
Your documentation must explicitly describe what tissue was removed, not just what was visible.
CPT Code Selection: Real-World Scenarios
Understanding the codes is one thing—applying them correctly is another. Here are five common scenarios with the correct coding approach:
Scenario 1: Sharp Debridement of Diabetic Foot Ulcer
A physician uses a scalpel to remove slough and biofilm from a 15 sq cm diabetic foot ulcer. The wound base shows healthy granulation tissue after debridement. No subcutaneous tissue was excised.
✅ Correct Code: 97597 (selective debridement, first 20 sq cm)
❌ Common Error: 11042 (surgical debridement—but no tissue was excised, only devitalized material removed)
Scenario 2: Excisional Debridement with Bone Exposure
A wound care specialist derides a sacral pressure ulcer. The wound extends to bone, and the physician documents removing necrotic subcutaneous tissue with a curette. Bone is visible but not debrided.
✅ Correct Code: 11042 (subcutaneous tissue debridement)
❌ Common Error: 11044 (bone debridement—but no bone tissue was actually removed)
Scenario 3: Large Wound Requiring Multiple Debridement Units
A patient presents with a 65 sq cm venous leg ulcer requiring excisional debridement of subcutaneous tissue.
✅ Correct Codes: 11042 + 11045 + 11045 (first 20 sq cm + two additional 20 sq cm units)
❌ Common Error: Billing only 11042 (missing 45 sq cm of billable work)
Scenario 4: NPWT Application in Office Setting
A physician applies negative pressure wound therapy using a reusable pump on a 40 sq cm wound in the office.
✅ Correct Code: 97605 (NPWT, ≤50 sq cm, durable equipment)
❌ Common Error: 97607 (disposable pump code—wrong equipment type)
Scenario 5: Skin Substitute on Foot Wound
A 30 sq cm cellular tissue product is applied to a diabetic foot ulcer.
✅ Correct Codes: 15275 (first 25 sq cm, foot) + 15276 (additional 5 sq cm) + Q4xxx (specific product)
❌ Common Error: Using 15271 (trunk/arms/legs code for a foot wound)
Common CPT Coding Mistakes to Avoid
| Mistake | Why It Happens | How to Fix It |
|---|---|---|
| Using 11044 when bone is visible but not removed | Confusion between wound depth and tissue removal depth | Always ask: “What tissue was EXCISED?” |
| Missing add-on codes for large wounds | Rushing through coding, not calculating wound size | Document and calculate wound area for every visit |
| Wrong NPWT code (97605 vs 97607) | Not distinguishing durable vs. disposable equipment | Verify equipment type in documentation |
| Using trunk codes for hands/feet | Not checking anatomic site distinctions | 15271-15274 = trunk/arms/legs; 15275-15278 = face/hands/feet |
| Billing 97597 with 11042-11047 | Assuming you can bill both selective and surgical debridement | These are mutually exclusive—bill the highest level performed |
ICD-10 Codes for Wound Care: Complete Diagnosis Coding Guide
Perfect CPT coding means nothing if your ICD-10 selections don’t establish medical necessity. The diagnosis code tells the story of why treatment was required—and payers scrutinize this connection closely.

Pressure Ulcer Coding (L89.xxx)
Pressure ulcer codes demand specificity. The sixth character indicates stage, and “unspecified” codes invite denials.
| Anatomical Site | Stage 2 | Stage 3 | Stage 4 | Unstageable | Deep Tissue Injury |
|---|---|---|---|---|---|
| Sacrum | L89.152 | L89.153 | L89.154 | L89.150 | L89.156 |
| Right Heel | L89.612 | L89.613 | L89.614 | L89.610 | L89.616 |
| Left Heel | L89.622 | L89.623 | L89.624 | L89.620 | L89.626 |
Critical sequencing rule: When a pressure ulcer heals from Stage 4 to Stage 3, you code the current stage. You don’t retroactively change historical staging.
Diabetic Ulcer Coding (E10.621, E11.621)
This is where sequencing trips up even experienced coders. For a diabetic foot ulcer:
- E11.621 (Type 2 diabetes with foot ulcer) — PRIMARY diagnosis
- L97.5xx (Specific ulcer site and severity) — SECONDARY
- Z79.4 or Z79.84 — Insulin or oral hypoglycemic use status
The diabetes code comes first. Always. It’s the etiology; the ulcer is the manifestation.
Chronic Ulcer Severity (L97.xxx)
The sixth character tells you severity:
- 1 = Limited to skin breakdown
- 2 = Fat layer exposed
- 3 = Necrosis of muscle
- 4 = Necrosis of bone
- 5 = Muscle necrosis without bone involvement
- 6 = Bone necrosis without muscle involvement
Using unspecified severity codes (ending in 9) when documentation supports specific staging leaves money on the table and invites audit questions.
ICD-10 Wound Care Coding: Common Scenarios
Scenario 1: Type 2 Diabetic with Heel Ulcer
Patient has Type 2 diabetes on insulin with a right heel ulcer exposing fat layer.
✅ Correct Sequence:
- E11.621 (Type 2 diabetes with foot ulcer) — PRIMARY
- L97.412 (Non-pressure chronic ulcer right heel, fat layer exposed) — SECONDARY
- Z79.4 (Long-term insulin use) — ADDITIONAL
❌ Common Error: Putting L97.412 as primary (diabetes etiology must come first)
Scenario 2: Hospital-Acquired Pressure Injury
Patient develops Stage 3 pressure ulcer on right hip during hospital stay.
✅ Correct Codes:
- L89.213 (Pressure ulcer of right hip, Stage 3)
- Y95 (Nosocomial condition) — if hospital-acquired
Scenario 3: Wound Improving from Stage 4 to Stage 3
A sacral pressure ulcer that was previously Stage 4 now shows granulation tissue filling the wound bed, effectively presenting as Stage 3.
✅ Correct Code: L89.153 (Stage 3 sacral pressure ulcer)
❌ Common Error: Continuing to code L89.154 (Stage 4) because “it was Stage 4 originally”
Rule: Always code the CURRENT stage, not the historical worst stage.
ICD-10 Coding Mistakes That Cause Denials
| Mistake | Result | Prevention |
|---|---|---|
| Unspecified codes (L89.90, L97.909) | Automatic denial or reduced payment | Always document site, laterality, stage/severity |
| Wrong sequencing for diabetic ulcers | Denial for improper etiology reporting | Diabetes code ALWAYS primary |
| Using resolved wound codes | Denial—no medical necessity | Only code active wound conditions |
| Missing laterality | Claim rejection | Specify right, left, or bilateral |
| Staging mismatch with CPT | Medical necessity denial | Stage 2 ulcer cannot support 11044 debridement |
Wound Care Coding Decision Trees: Step-by-Step Code Selection
One of the biggest challenges with wound care billing codes is knowing which code to select when multiple options seem applicable. These decision trees walk you through the logic for the most common scenarios.
Decision Tree 1: Debridement Code Selection
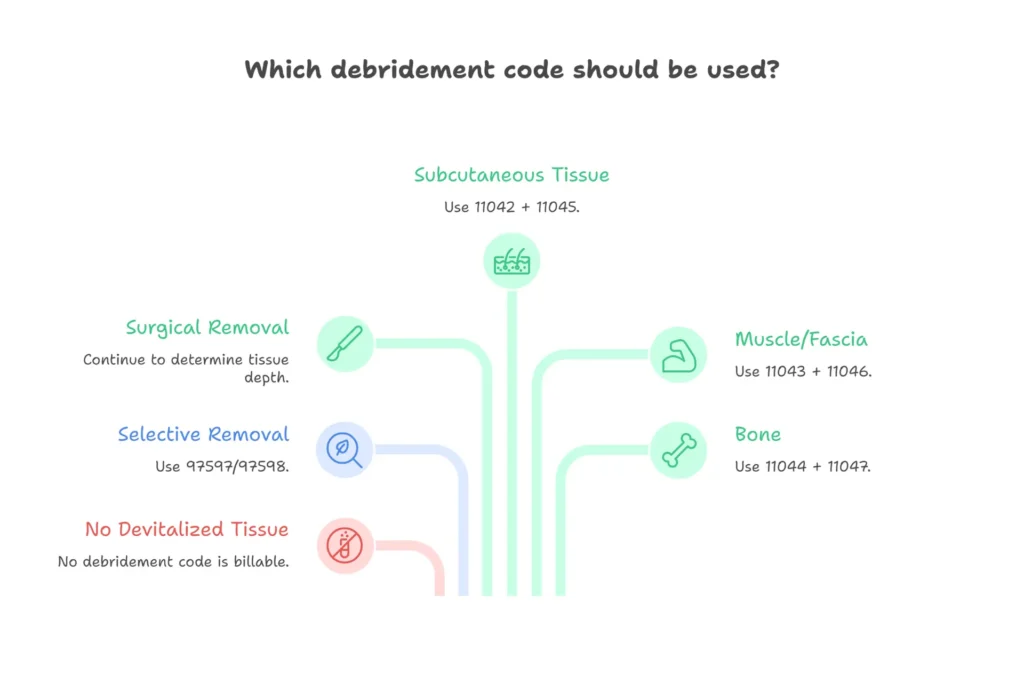
Step 1: Was devitalized tissue removed?
- No → No debridement code billable
- Yes → Continue to Step 2
Step 2: Was the removal selective or surgical?
- Selective (biofilm, slough removed without cutting viable tissue) → 97597/97598
- Surgical (viable tissue was excised/cut away) → Continue to Step 3
Step 3: What was the deepest tissue layer REMOVED?
- Epidermis/dermis only → 97597 (not surgical depth)
- Subcutaneous tissue → 11042 (+ 11045 for each additional 20 sq cm)
- Muscle/fascia → 11043 (+ 11046 for each additional 20 sq cm)
- Bone → 11044 (+ 11047 for each additional 20 sq cm)
Critical Check: Does documentation explicitly state what tissue was excised? If it only describes wound depth, you cannot code surgical debridement.
Decision Tree 2: Skin Substitute Code Selection
Step 1: Where is the wound located?
- Trunk, arms, or legs → Use 15271-15274 series
- Face, scalp, hands, feet, or genitalia → Use 15275-15278 series
Step 2: What is the total wound size?
For trunk/arms/legs (15271-15274):
- ≤100 sq cm total: 15271 (first 25 sq cm) + 15272 (each additional 25 sq cm)
- >100 sq cm total: 15273 (first 100 sq cm) + 15274 (each additional 100 sq cm)
For face/hands/feet (15275-15278):
- ≤100 sq cm total: 15275 (first 25 sq cm) + 15276 (each additional 25 sq cm)
- >100 sq cm total: 15277 (first 100 sq cm) + 15278 (each additional 100 sq cm)
Step 3: Add the product Q-code
- Identify the specific skin substitute product used
- Bill appropriate Q-code (Q4101-Q4255) with quantity in sq cm
Decision Tree 3: ICD-10 Wound Diagnosis Selection
Step 1: What is the wound etiology?
- Pressure/immobility → L89.xxx (pressure ulcer codes)
- Diabetes-related → E10/E11.621 + L97.xxx (diabetes primary, ulcer secondary)
- Venous insufficiency → I87.2 + L97.xxx
- Arterial disease → I70.xxx + L97.xxx
- Trauma/surgical → L89.xxx or appropriate injury code
- Unknown/non-specific → L97.xxx with documented severity
Step 2: Identify anatomic site and laterality
- Specify exact location (sacrum, heel, ankle, etc.)
- Include right, left, or bilateral designation
Step 3: Determine severity/stage
- Pressure ulcers: Stage 1-4, unstageable, or deep tissue injury
- Chronic ulcers: Severity 1-6 based on tissue involvement
Step 4: Check sequencing
- Diabetes codes (E10/E11) always come BEFORE manifestation codes
- Multiple wounds = multiple diagnosis codes in order of clinical significance
Quick Reference: Code Selection by Clinical Scenario
| Clinical Scenario | CPT Code | ICD-10 Code | Key Documentation |
|---|---|---|---|
| Sharp debridement of slough, no tissue excision | 97597 | Per wound type | Tissue removed: biofilm/slough |
| Surgical debridement to subcutaneous level | 11042 | Per wound type | “Excised subcutaneous tissue” |
| NPWT application, office, 35 sq cm wound | 97605 | Per wound type | Wound size, equipment type |
| Skin substitute to 40 sq cm leg ulcer | 15271 + 15272 | Per wound type | Site, size, product used |
| Stage 3 sacral pressure ulcer, diabetic patient | — | L89.153 + E11.9 | Stage, site, comorbidity |
| Diabetic foot ulcer with muscle exposure | — | E11.621 + L97.413 | Diabetes first, severity 3 |
Documentation Phrases That Support Correct Coding
For Surgical Debridement (11042-11047):
- ✅ “Excised necrotic subcutaneous tissue using curette”
- ✅ “Sharply debrided nonviable muscle tissue”
- ✅ “Removed cortical bone fragments with rongeur”
- ❌ “Debrided wound down to bone” (describes depth, not removal)
- ❌ “Cleaned wound bed” (suggests selective, not surgical)
For Active Debridement (97597-97598):
- ✅ “Selectively removed biofilm and adherent slough”
- ✅ “Debrided devitalized tissue from wound surface”
- ✅ “Removed non-viable tissue without excising viable structures”
For Skin Substitutes (15271-15278):
- ✅ “Applied [Product Name], 30 sq cm, to wound bed after preparation”
- ✅ “Cellular tissue product placed on debrided wound surface”
- Documentation must include: product name, size applied, wound location
This decision-tree approach ensures you select the right code every time—and have the documentation to support it.
Medicare Wound Care Billing: LCD Rules & Compliance Requirements [2026]
If 2025 was the warning shot, 2026 is the full regulatory assault. Understanding what’s changed—and what it means for your practice—is survival-critical.
The Skin Substitute Payment Overhaul
Effective January 1, 2026, CMS fundamentally restructured how skin substitutes get paid. The familiar ASP+6% model is dead for most products.
The New Reality:
- Flat national rate: $127.14 per square centimeter for most products
- Products now classified as “incident-to supplies”
- Separate payment for application codes (15271-15278) and product codes (Q-codes)
- Only biologicals licensed under PHS Section 351 remain on ASP methodology
If your practice uses high-cost grafts exceeding $127.14/cm², you are now losing money on every application unless you’ve renegotiated supplier contracts or shifted to different products.
Your Graft Product Source Directly Impacts Your Q-Code Eligibility and Claim Success Rate
If your practice applies amniotic membrane or skin substitute grafts, the product source directly impacts your Q-code eligibility and claim success rate. An unverified product — one without confirmed FDA HCT/P documentation, correct NDC numbers, and pre-loaded Q-code assignment — is one of the leading causes of skin substitute claim denials and Medicare RAC audit flags.
Our 3-Step IVR verified graft program ensures your product documentation, provider credentials, and patient insurance coverage are all confirmed before every application — so the Q-code on your claim matches the product in your hands, every single time. Every enrolled practice also receives 6-Year Claims Protection against Medicare audits and retroactive denials.
What Is the Rule of 30 in Wound Care?
This question comes up constantly, and the answer involves two distinct requirements:
Conservative Care Requirement: Advanced therapies like skin substitutes are only covered when the wound has failed standard wound care for at least 30 days. Documentation must prove appropriate offloading, infection control, moisture balance management, and nutritional assessment occurred before escalating treatment.
Debridement Volume Guideline: Debridement generally shouldn’t exceed 30% of the total wound area in a single session without documented justification. Exceeding this threshold without proper documentation raises medical necessity questions.
No documented conservative care trial? No coverage. This is one of the most common denial reasons in wound care billing.
LCD Compliance Across MAC Jurisdictions
In a surprise December 2025 move, CMS withdrew the Final LCDs that would have created a strict skin substitute formulary. But don’t mistake that withdrawal for relaxed scrutiny—existing LCDs remain in force, and auditors are watching closely.
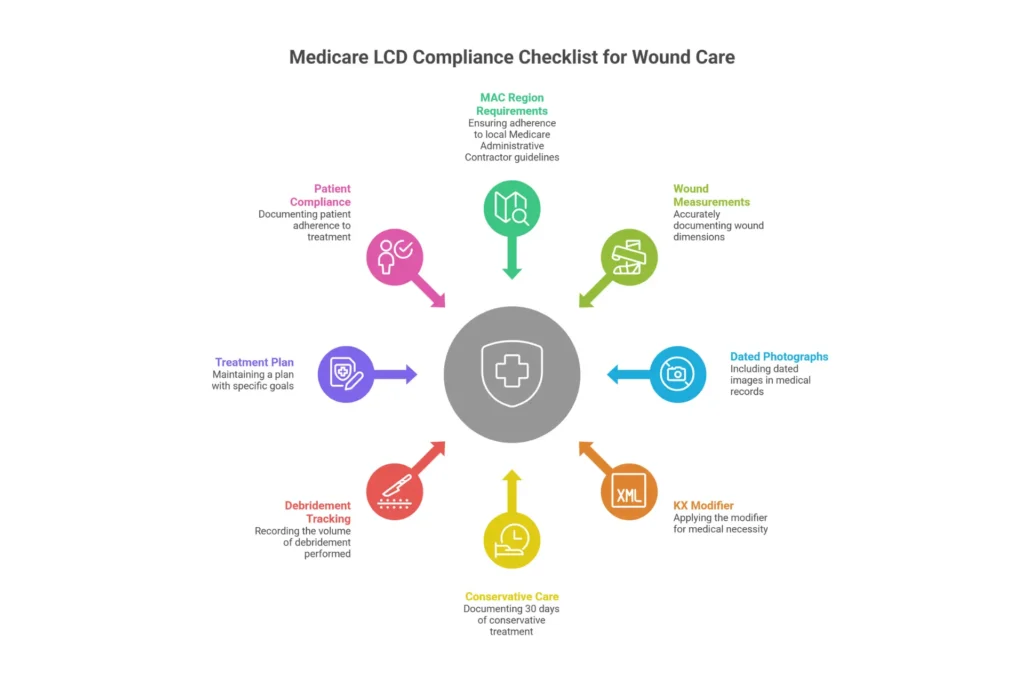
Your compliance checklist:
- ☐ Identified which LCD applies to your MAC region
- ☐ Wound measurements are objective (ruler measurements, not “walnut-sized”)
- ☐ Photographs include measurement tools in frame
- ☐ KX modifier present when required for skin substitutes
- ☐ 30-day conservative care failure documented before CTPs
→ Stay compliant with Medicare requirements. Explore our credentialing services
When to Consider Professional Wound Care Billing Help
Even with a complete understanding of wound care billing codes, many practices struggle with implementation. The coding knowledge exists, but the execution falls short due to volume, complexity, or staffing limitations.
Here are the signs that your wound care coding may need professional support:
Warning Signs Your Coding Needs Help:
- Denial rates exceeding 15% on wound care claims
- Frequent requests for additional documentation from payers
- Uncertainty about 2026 Medicare skin substitute payment changes
- Staff spending more time on appeals than initial coding
- Audit notices or RAC reviews targeting wound care claims
When these issues persist despite training, it may be time to evaluate professional wound care billing partners.
Expertise You Can’t Replicate In-House
Your billing staff—who’s also covering front desk and scheduling—simply cannot keep pace with:
- 2026 flat-rate skin substitute payment calculations
- The 3.8% APM vs. non-APM conversion factor gap
- New ICD-10 codes for non-pressure chronic ulcers
- MAC-specific LCD updates that drop without warning
A specialized wound care billing company employs certified coders whose singular focus is staying current on wound-specific regulations. You’re not funding their continuing education—you’re just benefiting from it.
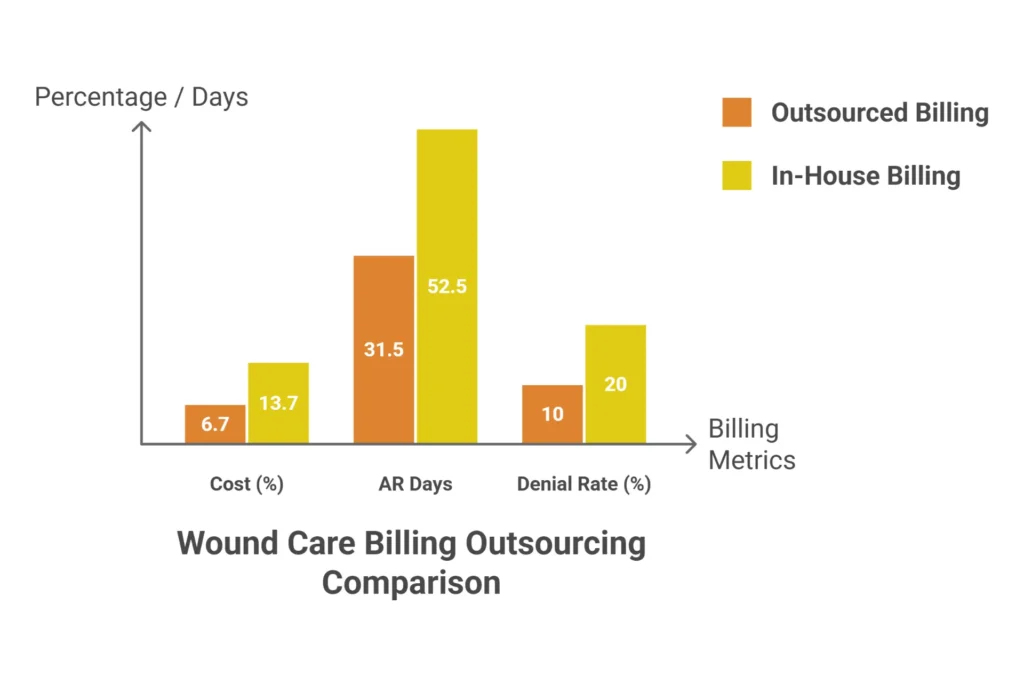
Faster Revenue Cycles
Average wound care claim AR with in-house billing: 45-60 days. Specialized partners routinely achieve 28-35 days. The difference? Dedicated denial management teams working aging reports daily rather than “when we have time.”
Reduced Audit Exposure
When OIG investigators come knocking—and with $10 billion in skin substitute spending, they will—do you want your part-time biller defending your coding decisions? Or a team that understands exactly what auditors look for and builds compliant claims from day one?
The ROI Calculation
Here’s what a typical mid-sized wound care practice sees after transitioning to specialized billing:
- Direct cost savings: 30-40% reduction in billing expenses
- Revenue increase: 15-25% from better coding and denial recovery
- AR acceleration: 20-30% reduction in Days in AR
- Denial rate reduction: From 25-35% to under 10%
The compound effect? Year-one ROI typically exceeds 200%.
→ Get a Free Coding Accuracy Assessment
How to Evaluate Wound Care Billing and Coding Partners
Selecting the right billing partner is high-stakes. Here’s how to make that decision with confidence.
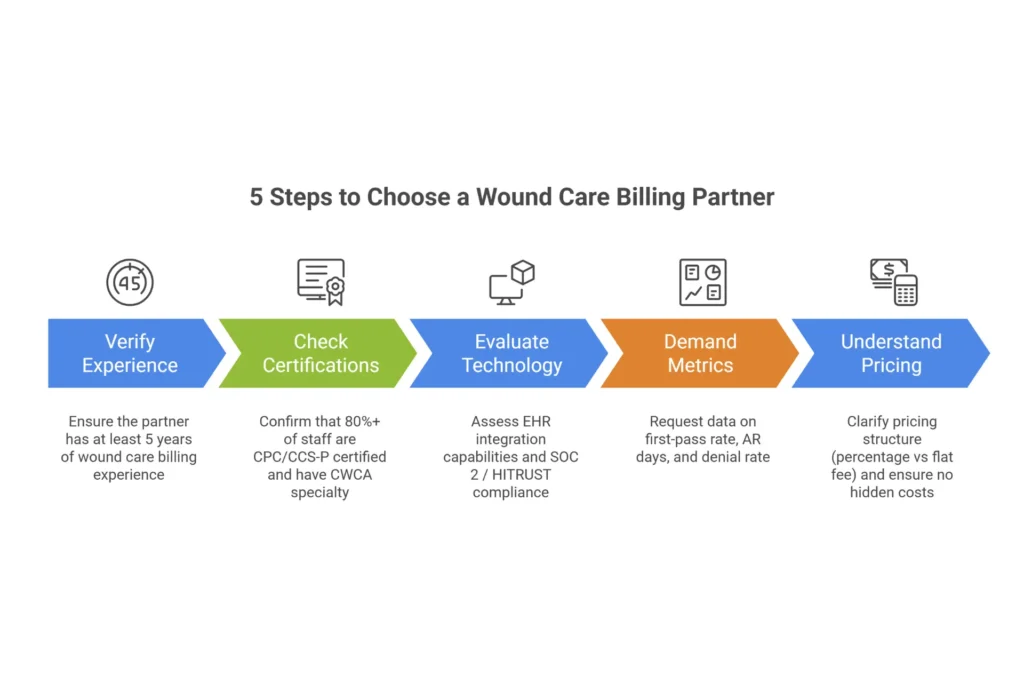
Verify Wound-Specific Experience
This requirement is non-negotiable. You need a partner with minimum five years of documented wound care billing experience—not general medical billing experience with some wound claims mixed in.
Questions that separate specialists from generalists:
- “What percentage of your claims involve debridement codes 11042-11047?”
- “How do you handle KX modifier requirements for skin substitutes across different MAC regions?”
- “Can you walk me through coding a wound where depth reaches muscle but only subcutaneous tissue was removed?”
Demand Credentialing Verification
At least 80% of the coding team should hold relevant certifications:
- CPC (Certified Professional Coder)
- CCS-P (Certified Coding Specialist—Physician)
- CWCA (Certified Wound Care Associate) or CWS (Certified Wound Specialist)
Evaluate Technology Integration
The best partners offer:
- Direct EHR integration (no manual exports)
- Real-time claim status visibility
- AI-assisted denial prediction
- SOC 2 Type II or HITRUST certification for security
Scrutinize Performance Guarantees
A reputable partner publishes their benchmarks and backs them contractually:
- First-pass acceptance rate: 95%+
- Clean claim rate: 98%+
- Denial rate: under 10%
- Days in AR: under 45
- Net collection rate: 95%+
If they won’t provide these numbers or won’t put them in an SLA, walk away.
Understand Pricing Models
| Model | Typical Range | Best For |
|---|---|---|
| Percentage of collections | 6-8% | Practices with $1M+ revenue |
| Per-claim | $6-12 | High-volume, lower complexity |
| Flat monthly | $3,000-8,000 | Predictable claim volume |
Red flags: Guarantees of “100% collection” (impossible), pressure toward multi-year contracts without performance SLAs, or setup fees exceeding $5,000.
Common Wound Care Coding Errors and How to Fix Them
Let’s get tactical about the problems that drain revenue—and exactly how to fix them.
Challenge 1: Missing Wound Measurements
Why it happens: Clinicians are focused on healing, not billing documentation. Time pressure leads to notes like “wound improving” without dimensions.
The fix: Implement mandatory measurement fields in your EHR that won’t allow visit closure without documented length, width, and depth. Consider AI-assisted wound imaging that auto-calculates measurements from smartphone photos. Pre- and post-debridement photographs with rulers in frame should be standard protocol.
Challenge 2: Debridement Depth Coding Errors
Why it happens: Confusion between wound depth and tissue removed depth.
The fix: Decision tree training for all coding staff. If documentation says “bone visible” but doesn’t describe bone tissue removal with rongeur or similar instrument, it’s 97597—not 11044. This single distinction prevents six-figure audit liabilities.
Challenge 3: Modifier Misuse
Why it happens: Lack of understanding about when distinct procedural services qualify for unbundling.
The fix: Hard-stop edits in billing software. For skin substitutes, if KX modifier is missing and the MAC requires it, the claim shouldn’t be submittable. For debridement, modifier 59/XS should require documentation review before application.
Challenge 4: LCD Non-Compliance
Why it happens: Policy updates happen faster than in-house training cycles.
The fix: Partner with specialists who monitor MAC policy changes daily. When CMS withdrew the Final LCDs in December 2025, specialized vendors pivoted within 24 hours. In-house teams typically take weeks to catch up—by which time claims have already been denied.
Challenge 5: AR Aging Beyond 90 Days
Why it happens: Manual claim status follow-up is tedious and gets deprioritized.
The fix: Automation. Modern tools check claim status on thousands of claims simultaneously, flagging only those needing human intervention. What was a 40-hour weekly manual process becomes 4 hours of exception management.
The Cost of Wound Care Coding Errors: Understanding the Financial Impact
Understanding the financial impact of coding errors helps justify investment in proper training, tools, or professional support.
What Coding Errors Actually Cost
| Error Type | Direct Cost | Indirect Cost |
|---|---|---|
| Undercoding (using 97597 instead of 11042) | $150-400 per claim | Cumulative revenue loss |
| Upcoding (using 11044 incorrectly) | Full claim recoupment + penalties | Audit exposure, reputation damage |
| Missing add-on codes | $75-200 per claim | Pattern of lost revenue |
| Documentation gaps causing denials | Full claim value | Staff time on appeals |
| LCD non-compliance | Claim denial | Potential fraud investigation |
Sample Annual Impact: Mid-Size Wound Care Practice
For a practice processing 500 wound care claims monthly:
| Metric | Poor Coding | Accurate Coding | Difference |
|---|---|---|---|
| First-pass acceptance | 75% | 95% | +20% |
| Average reimbursement per claim | $285 | $340 | +$55 |
| Annual wound care revenue | $1.71M | $2.04M | +$330,000 |
| Appeals staff time (hours/month) | 80 | 20 | -60 hours |
The $330,000 difference comes from:
- Correct code selection (not undercoding)
- Complete documentation supporting higher-level codes
- Fewer denials requiring rework
- Proper use of add-on codes for large wounds
Investment vs. Return
Whether you invest in staff training, coding software, or professional billing support, the ROI math is straightforward:
If your improvement in clean claims and proper code selection exceeds your investment cost, it’s worth it.
Most practices see positive ROI within 90-120 days of implementing systematic coding improvements.
Next Steps: Improving Your Wound Care Coding
Now that you understand wound care billing codes, here’s how to put this knowledge into practice.
Immediate Actions (This Week)
1. Audit Your Current Coding
Pull your last 30 wound care claims and check:
- Are you using add-on codes when wound size exceeds 20 sq cm?
- Do your ICD-10 codes include full specificity (site + laterality + stage)?
- Are debridement codes based on tissue removed, not wound depth?
2. Create a Code Quick-Reference
Print or bookmark the CPT and ICD-10 tables from this guide. Post them where coders can reference during claim entry.
3. Review Your Denial Patterns
What are the top 3 denial reasons for wound care claims? Target those specific issues first.
Short-Term Improvements (Next 30 Days)
1. Documentation Template Update
Ensure your EHR templates capture:
- Wound measurements (L × W × D) with units
- Tissue type present and removed
- Conservative care history (for skin substitute claims)
- Pre/post debridement wound status
2. Coder Training Session
Schedule a focused training on the depth rule for debridement coding. This single concept prevents most audit issues.
3. LCD Compliance Check
Verify your documentation meets your MAC region’s specific LCD requirements.
Long-Term Excellence (90+ Days)
1. Track Key Metrics
Monitor: First-pass acceptance rate, denial rate by code, average reimbursement per wound care claim
2. Regular Code Updates
Subscribe to CMS updates and AAPC coding newsletters to stay current on changes
3. Consider Professional Review
If denial rates remain above 15% despite improvements, a professional coding audit can identify blind spots
Free Resources to Continue Learning
- CMS Medicare Claims Processing Manual, Chapter 12 — Official wound care billing guidance
- AAPC Wound Care Coding Resources — Training and certification information
- Your MAC’s LCD Database — Regional coverage requirements
→ Get Your Free Wound Care Coding Cheat Sheet + Denial Prevention Checklist
Frequently Asked Questions
What is the difference between 97597 and 11042?
97597 is for selective debridement (removing devitalized tissue like slough or biofilm without excising viable tissue). 11042 is for surgical/excisional debridement where subcutaneous tissue is actually cut away and removed. The key distinction: 97597 = cleaning the wound; 11042 = surgically removing tissue.
How do I code debridement when bone is visible?
Code based on what tissue was REMOVED, not what’s visible. If bone is exposed but only subcutaneous tissue was debrided, use 11042. Only use 11044 if bone tissue itself (cortical bone) was actually excised with instruments like a rongeur.
What ICD-10 codes are used for diabetic foot ulcers?
Use E11.621 (Type 2 diabetes with foot ulcer) as the PRIMARY diagnosis, followed by L97.xxx (specific ulcer site and severity) as SECONDARY. Always sequence the diabetes code first—it’s the etiology.
How do I code pressure ulcers that are healing?
Always code the CURRENT stage, not the original worst stage. If a Stage 4 ulcer has granulated and now presents as Stage 3 depth, code it as Stage 3 (L89.xx3). Document the healing progress.
What is the Rule of 30 for wound care billing?
Two components: (1) Advanced therapies require 30 days of documented failed conservative care before Medicare covers them. (2) Single-session debridement generally shouldn’t exceed 30% of wound area without documented justification.
When do I use modifier 59 with wound care codes?
Use modifier 59 (or X modifiers) when performing distinctly separate procedures that would otherwise be bundled. Example: Debridement of two anatomically separate wounds on different extremities during the same session.
How are skin substitute codes structured?
Application codes (15271-15278) are separate from product codes (Q4xxx). Bill the application code based on anatomic site and size, plus the Q-code for the specific product used. Note: 2026 changed most products to flat-rate reimbursement at $127.14/cm².
What documentation is required to support wound care CPT codes?
Essential elements: Wound location, measurements (L × W × D), tissue types present, tissue removed (for debridement), wound bed description before and after treatment, and medical necessity statement. For surgical debridement, explicitly document WHAT tissue was excised.
What CPT codes are used for wound debridement?
Active debridement uses 97597-97598 for selective removal. Surgical debridement uses 11042 (subcutaneous), 11043 (muscle), or 11044 (bone) based on the deepest tissue actually removed—not the wound depth.
How do I code a Stage 4 pressure ulcer?
Use L89.xx4 where “xx” indicates the anatomic site. For example, L89.154 for Stage 4 sacral pressure ulcer. Include laterality when applicable (right hip = L89.214).
What is the difference between 11042 and 11044?
11042 is debridement of subcutaneous tissue. 11044 is debridement of bone. The difference is which tissue layer was surgically removed—not how deep the wound extends.
How do you bill for NPWT wound therapy?
Use 97605-97606 for durable pump equipment (reusable) or 97607-97608 for disposable pumps. Size threshold is 50 sq cm. Also bill E-codes for supplies and equipment as applicable.
What ICD-10 code for diabetic foot ulcer?
E11.621 for Type 2 diabetes with foot ulcer (primary), followed by L97.xxx for specific ulcer location and severity (secondary). Always sequence diabetes first.
What is wound care coding Rule of 30?
Two rules: Advanced therapies need 30 days of failed conservative care documentation, and debridement shouldn’t exceed 30% of wound area per session without justification.
How to code skin substitute application?
Use 15271-15274 for trunk/arms/legs or 15275-15278 for face/hands/feet. Code is based on wound size (25 sq cm and 100 sq cm thresholds). Bill separately for the product using Q-codes.
What documentation needed for wound care billing?
Required: Wound measurements (L × W × D), tissue type documentation, description of treatment performed, tissue removed (for debridement), and for advanced therapies, proof of 30-day conservative care failure.
Conclusion: Your 2026 Action Plan
Mastering wound care billing codes is no longer optional—it’s essential for financial survival in 2026 and beyond. The complexity of CPT depth-based coding, ICD-10 specificity requirements, and Medicare LCD compliance means the margin for error has disappeared.
This guide covered everything you need to know about wound care coding and billing:
- CPT Codes: 97597-97598 for active debridement, 11042-11047 for surgical debridement (remember: code tissue REMOVED), 15271-15278 for skin substitutes
- ICD-10 Codes: L89.xxx for pressure ulcers, L97.xxx for chronic ulcers, E11.621 for diabetic ulcers (always sequenced first)
- Medicare Compliance: 2026 flat-rate payments, Rule of 30, LCD requirements by MAC region
- Common Errors: Depth coding confusion, missing add-on codes, unspecified diagnosis codes, documentation gaps
Bookmark this guide and return to it whenever you’re coding wound care claims. The reference tables, scenario examples, and compliance checklists are designed to be used in daily practice.
Want to take your wound care coding further?
Download our free resources:
- Wound Care CPT/ICD-10 Cheat Sheet (PDF) — Print-ready quick reference
- Denial Prevention Checklist — Pre-submission verification tool
If your practice needs hands-on coding support, EliteMed Financials offers expert medical coding services with certified wound care specialists. Our team handles the complexity so you can focus on patient care.
→ Request a Free Coding Accuracy Assessment
→ Book Your Free Revenue Leakage Audit — Find out exactly where your current wound care billing process is losing revenue, and get a customized roadmap to fix it.
Related Reading: