
I’ve spent the better part of fifteen years watching Medicare wound care billing transform from a relatively straightforward process into what can only be described as a compliance minefield. And 2026? This year takes the complexity to an entirely new level.
Between the site-neutral skin substitute payment overhaul, the WISeR prior authorization model, and LCD consolidations happening across multiple jurisdictions, providers who aren’t paying attention are leaving serious money on the table—or worse, setting themselves up for devastating audits.
Here’s what I know after reviewing thousands of wound care claims: the difference between practices that thrive and those that struggle almost always comes down to understanding Medicare’s rules inside and out. Not the surface-level stuff you can Google in five minutes, but the nitty-gritty details that determine whether your claim gets paid or lands in denial limbo.
This guide covers everything—from basic coverage questions that trip up even experienced billers, to the specific CPT code decisions that can make or break your reimbursement. Whether you’re a wound care specialist wondering why your debridement claims keep getting rejected, a medical biller trying to navigate Part A versus Part B coverage, or a practice manager concerned about compliance, you’ll find actionable answers here.
Let’s get into it.
Table of Contents
Does Medicare Cover Wound Care?
Yes, Medicare covers medically necessary wound care services under both Part A and Part B. But here’s where most people get tripped up—Medicare draws a hard line between skilled wound care and routine maintenance.
Think of it this way: if your grandmother could change the dressing after watching a YouTube video, Medicare isn’t paying for it. But if the wound requires professional assessment, debridement of necrotic tissue, or management of complications like infection—that’s a different story entirely.
The Centers for Medicare & Medicaid Services (CMS) spells this out clearly in the Medicare Benefit Policy Manual, Chapter 15. Medical necessity isn’t just a buzzword—it’s the foundation of every covered service.
What Makes Wound Care “Medically Necessary”?
According to CMS guidelines, wound care qualifies as medically necessary when:
- The wound is chronic and hasn’t responded to at least 30 days of standard treatment
- Skilled clinical judgment is required to assess wound progression
- The treatment prevents deterioration or promotes healing
- A physician has documented why the care requires professional intervention
The documentation piece is where I see practices fail most often. Saying “wound care provided” in your notes won’t cut it. You need objective measurements, tissue descriptions, and clear medical necessity statements. Every single time.
Covered vs. Non-Covered Wound Care Services
What Medicare Covers:
| Service | CPT Codes | Coverage Notes |
|---|---|---|
| Selective debridement | 97597, 97598 | Removing necrotic tissue, biofilm, slough with scissors, forceps, waterjet |
| Surgical debridement | 11042-11047 | Deep tissue removal to subcutaneous, muscle, fascia, or bone |
| NPWT (wound vac) | 97605-97608 | After 30-day standard care failure documented |
| MIST ultrasound therapy | 97610 | For painful wounds failing conventional debridement |
| Surgical dressings | A6196-A6266 | Alginates, foams, hydrocolloids, collagen, hydrogels |
| Skin substitutes/CTPs | Q4100 series | Strict LCD criteria apply; 2026 flat-rate payment |
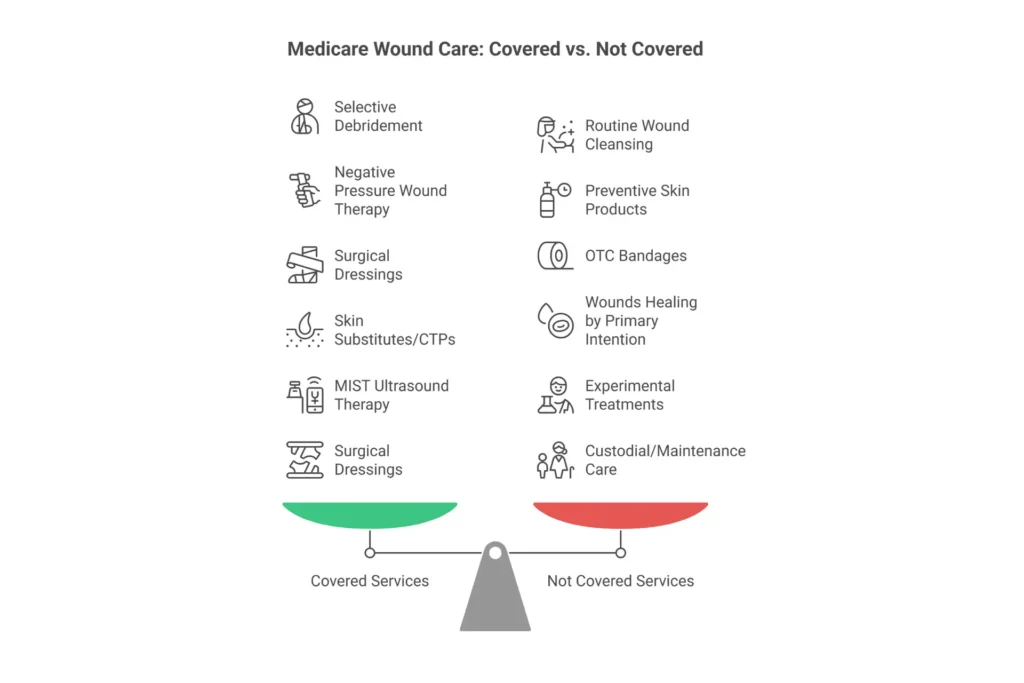
What Medicare Does NOT Cover:
- Routine wound cleansing without debridement
- Preventive skin products (moisturizers, barrier creams)
- Convenience items for caregivers
- Wounds healing normally by primary intention
- Experimental treatments without established efficacy
- Hyperbaric oxygen therapy beyond specific NCD criteria
- OTC equivalents of prescription dressings
- Non-sterile gauze used alone
The Bottom Line: Medicare pays for skilled care that promotes healing. It doesn’t pay for maintenance that any caregiver could perform. Understanding this distinction is fundamental to every wound care billing decision you’ll make.
If your wound care claims keep getting denied for medical necessity, the issue is almost always documentation. Consider working with specialists who understand Medicare wound care billing requirements to identify gaps in your current processes.
Medicare Part A vs Part B Wound Care Coverage
This distinction causes more billing errors than almost anything else I see. Understanding when wound care falls under Part A versus Part B—and when both apply simultaneously—is fundamental to getting paid correctly.
Part A Coverage: The Institutional Bundle
Under Part A, wound care gets bundled into facility payments. You don’t bill per procedure—everything rolls into a single payment.
Inpatient Hospital (POS 21)
Medicare pays hospitals through MS-DRGs (Medicare Severity Diagnosis Related Groups). A patient with a Stage IV pressure ulcer might fall into DRG 592-594, and that single payment covers everything—debridement, dressings, nursing time, NPWT supplies, the works.
The key exception: physicians still bill their professional services separately under Part B. The hospital gets the facility payment; the doctor bills for E/M visits (99221-99223 for initial, 99231-99233 for subsequent) and any surgical debridement they personally perform.
Skilled Nursing Facility (POS 31)
Under PDPM (Patient-Driven Payment Model), wound care drives reimbursement through two components:
- Nursing Component – Complex wounds place patients in higher-paying nursing categories
- Non-Therapy Ancillary (NTA) Component – Wounds provide “points” that boost the NTA score
A Stage IV pressure ulcer with infection can add significant points to the NTA component, increasing daily payments by $50-200 depending on the patient’s overall acuity.
But here’s the critical rule: Consolidated Billing. During a Part A covered stay, the SNF bills for almost everything. Physician professional services are “carved out”—meaning doctors can still bill Part B for E/M visits (99304-99310) and surgical debridement (11042-11047).
Home Health (Part A)
Under PDGM (Patient-Driven Groupings Model), agencies receive 30-day episode payments. Wounds fall into the “Wounds” clinical group—specifically “Post-Op Wound Aftercare and Skin/Non-Surgical Wound Care”—which carries the highest case-mix weight in the model.
Everything bundles into the episode payment: nursing visits, supplies, therapy services. The agency absorbs those costs within the 30-day payment.
Part B Coverage: Professional and Outpatient Services
Part B is where you bill per procedure, per visit. Payment comes from the Physician Fee Schedule (PFS) at 80% after the deductible.
| Setting | POS Code | Payment Method | Key Considerations |
|---|---|---|---|
| Physician Office | 11 | PFS rates | 11043-11047 frequently denied here |
| Hospital Outpatient | 22 | OPPS/APC + PFS | Facility + professional fees separate |
| Ambulatory Surgical Center | 24 | Procedure-based | Limited approved code list |
| SNF (physician services) | 31 | PFS | Part B carve-out during Part A stay |
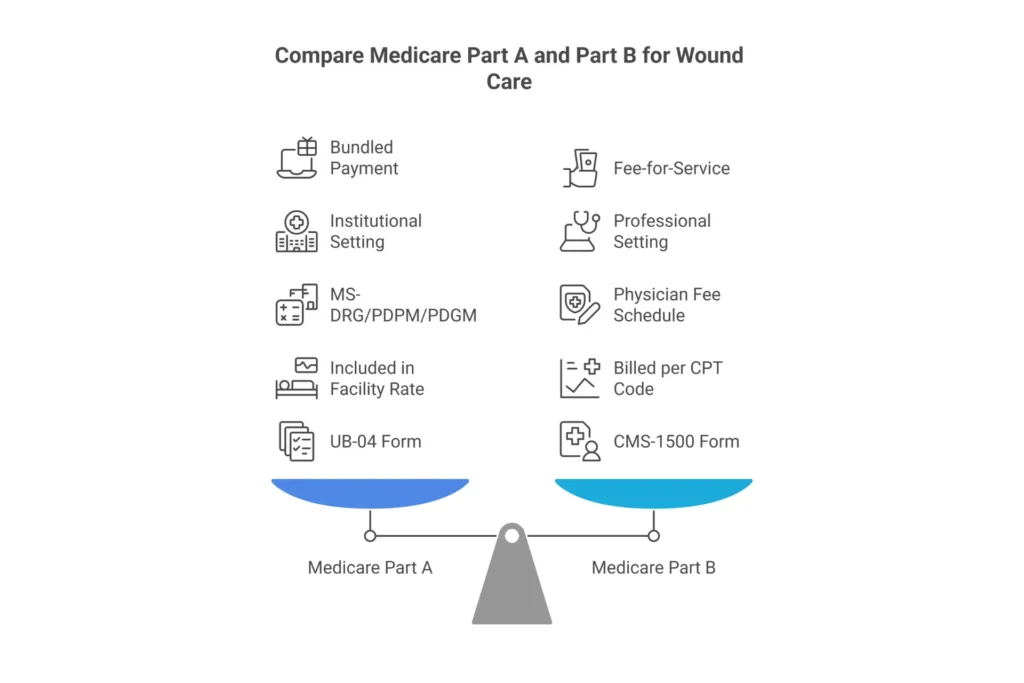
When Both Apply: Split Billing Scenarios
Here’s a scenario you’ll encounter regularly: A patient in a SNF Part A stay needs physician-performed surgical debridement.
- The facility bills Part A (UB-04 form)
- The physician bills Part B (CMS-1500 form)
This is split billing, and it’s perfectly legitimate. Just make sure you’re using POS 31 on the physician claim, not POS 11. Billing the office place of service while the patient is in a SNF? That’s an automatic denial under Consolidated Billing rules.
The complexity of Part A versus Part B billing is one of the most common reasons practices seek comprehensive RCM services. Getting this wrong doesn’t just cost you one claim—it can trigger audit reviews of your entire wound care billing pattern.
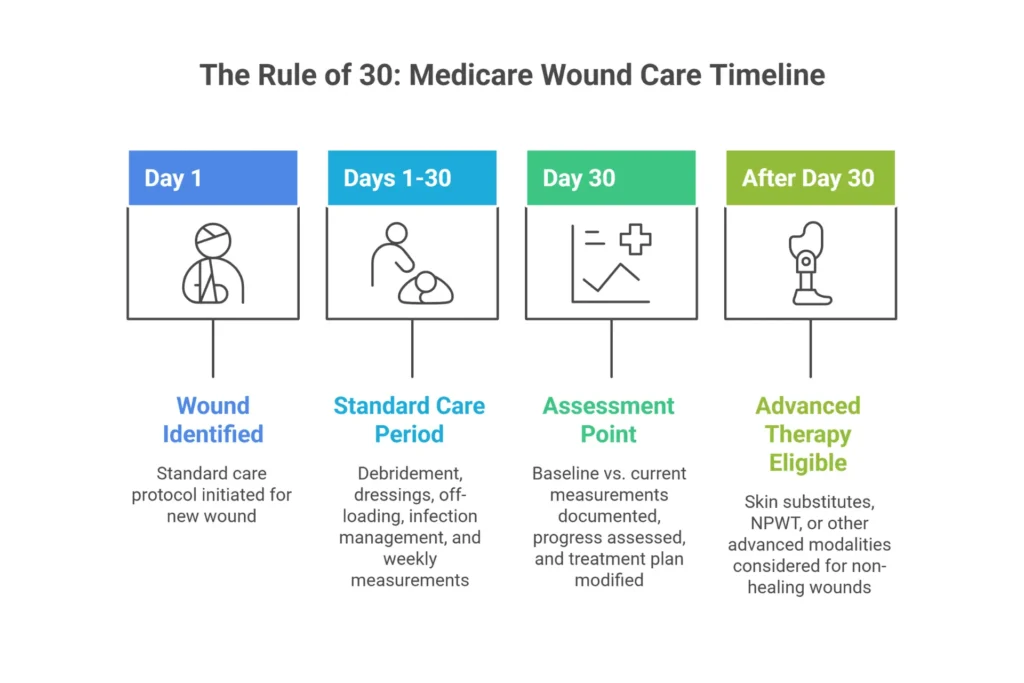
The Rule of 30 in Wound Care
If there’s one concept that separates compliant wound care billing from audit disasters, it’s the Rule of 30. And surprisingly, many experienced billers still don’t fully understand it.
What is the Rule of 30 in wound care?
The Rule of 30 is a Medicare guideline requiring that a wound shows no measurable improvement after at least 30 days of standard treatment before advanced therapies like skin substitutes, cellular and tissue-based products (CTPs), or NPWT are considered medically necessary and covered. It’s embedded in LCDs like L38904 (Noridian) and L35125 (Novitas).
Why It Exists
The Rule of 30 stems from clinical evidence showing that wounds failing to respond to 30 days of appropriate standard care are unlikely to heal without intervention. It establishes the clinical threshold for “chronic wound” status—the prerequisite for advanced therapy coverage.
Standard care includes:
- Appropriate wound bed preparation
- Debridement of necrotic tissue and biofilm
- Moisture management with appropriate dressings
- Off-loading (for DFUs)
- Compression therapy (for VLUs)
- Infection management
- Nutritional optimization
- Vascular assessment and treatment
What You Must Document at 30 Days
Your 30-day progress note is your audit defense. It should include:
- Comparative measurements – Baseline vs. current (LxWxD in centimeters)
- Surface area calculation – Percentage change from baseline
- Tissue type percentages – “60% granulation, 30% slough, 10% epithelial”
- Exudate characteristics – Type (serous, serosanguinous, purulent) and amount
- Wound bed changes – Increased/decreased necrosis, granulation progression
- Factors affecting healing – Infection status, nutritional labs, vascular studies
- Modified plan of care – What you’re changing and clinical rationale
- Physician signature – On the reassessment, not just a cosign
Common Rule of 30 Documentation Failures
I see these mistakes constantly in audit reviews:
- No baseline measurements to compare against
- Subjective descriptions without quantifiable metrics (“wound looks better”)
- Continuing the same treatment without documented justification for why
- Missing tissue type percentages—just saying “necrotic tissue present”
- No physician input on the 30-day reassessment
- Cloned notes that are identical to week 1
When wounds aren’t improving, auditors expect to see documented reasoning. “Continued current treatment plan” without explanation is a red flag. If you’re struggling with medical necessity denials, our denial management services can help identify patterns and fix documentation gaps before they become audit findings.
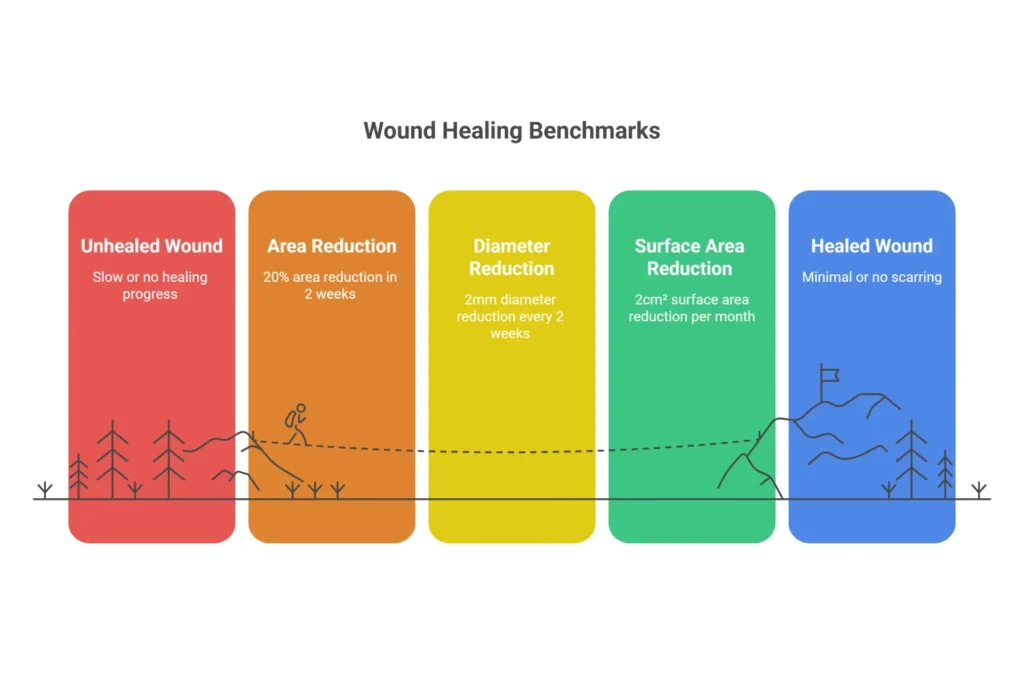
The 2-2-2 Rule in Medicare Wound Care
While the Rule of 30 establishes chronicity, the 2-2-2 Rule monitors whether your treatment is actually working. Think of them as complementary benchmarks—one for entry into advanced treatment, one for ongoing justification.
What is the 2-2-2 Rule in Medicare wound care?
The 2-2-2 Rule is a clinical benchmark stating that a wound should show approximately 20% reduction in surface area within 2 weeks, approximately 2mm diameter reduction every 2 weeks, or approximately 2cm² area reduction per month to demonstrate appropriate healing trajectory. It predicts healing success and justifies continued treatment.
Clinical Application
Research shows that wounds failing to achieve 20% area reduction in the first two weeks have significantly lower probability of healing by week 12. This isn’t arbitrary—it’s based on clinical trial data and wound healing biology.
The 2-2-2 Rule gives you an early warning system. If a wound isn’t meeting these benchmarks, you need to:
- Reassess for barriers (infection, biofilm, vascular insufficiency)
- Modify the treatment approach
- Document why you believe the new approach will work
- Consider whether the wound is healable at all
Expected Healing Timeline:
| Timeframe | Expected Progress | Action If Not Met |
|---|---|---|
| 2 weeks | ~20% area reduction | Reassess treatment plan |
| 4 weeks | ~50% area reduction | Modify approach, document barriers |
| 8 weeks | Continued improvement | Document comorbidities |
| 12+ weeks | Near closure or justified continuation | Detailed rationale required |
Billing Implications of the 2-2-2 Rule
Here’s what matters for reimbursement: You can still bill if the wound isn’t meeting the 2-2-2 benchmark—but you must document:
- Why the wound isn’t progressing as expected
- What factors are impeding healing (comorbidities, infection, vascular issues, non-compliance)
- What you’re changing in the treatment plan
- Why continued treatment is medically necessary despite lack of progress
Billing the same treatment on a non-improving wound without documented justification? That’s the fastest path to a CO-50 denial for lack of medical necessity.
2-2-2 Rule Exceptions
The rule doesn’t apply to:
- Palliative wounds where healing isn’t the goal
- Malignant wounds
- Wounds on limbs with documented arterial insufficiency (ABI <0.5)
- Patients with documented contraindications to healing (immunosuppression, ESRD)
If you’re treating these wound types, document the exception clearly. Reference comorbidities and explain why standard healing benchmarks don’t apply.
Medicare Wound Care Documentation Requirements
Let me be direct: in 2026, documentation is your only defense against takebacks. CMS isn’t looking for notes—they’re looking for data-driven clinical evidence that justifies every dollar paid.
The Comprehensive Error Rate Testing (CERT) program and Recovery Audit Contractors (RACs) are actively reviewing wound care claims. Your documentation must stand on its own, without you there to explain it.
Mandatory Elements of Every Wound Assessment
Anatomical location – Be precise. “Right medial malleolus, posterior aspect” not “right leg.” Laterality matters for ICD-10 coding.
Size – Length × Width × Depth in centimeters. Every. Single. Time.
- Length: Longest head-to-toe axis
- Width: Widest perpendicular axis
- Depth: Deepest point, measured with sterile probe
Stage/Classification – NPUAP stages I-IV, Unstageable, or DTI for pressure ulcers. Wagner or University of Texas scale for diabetic ulcers. Document consistently.
Tissue types – Document by percentage. “50% granulation tissue (beefy red, moist), 40% slough (yellow, stringy), 10% epithelial tissue (pink, advancing from edges).” Be specific about what you see.
Exudate – Type (serous, serosanguinous, sanguinous, purulent) and amount (scant, small, moderate, large/copious).
Edges and periwound – Attached, rolled (epibole), undermined; macerated, erythematous, indurated, denuded.
Tunneling/Undermining – Use clock method. “Undermining from 2 to 5 o’clock, 2.5cm depth at 3 o’clock.”
Infection signs – Erythema extending >2cm, warmth, edema, purulent drainage, foul odor, friable granulation tissue.
Pain assessment – 0-10 scale, quality (burning, sharp, aching), timing (constant, with dressing changes).
Documentation Template for Wound Care
Here’s a copy-paste template I’ve refined over years of audit reviews:
WOUND ASSESSMENT - [DATE]
Location: [Anatomical site with laterality]
Wound Type: [Pressure ulcer Stage IV / DFU Wagner 2 / VLU / Surgical]
Etiology: [Pressure, diabetes, venous insufficiency, surgical]
MEASUREMENTS:
Length: [X] cm (head-to-toe)
Width: [X] cm (perpendicular)
Depth: [X] cm (deepest point)
Surface Area: [X] cm²
Comparison to Baseline: [X]% change ([increased/decreased])
TISSUE BED:
Granulation: [X]% - [description: beefy red, friable, pale pink]
Slough: [X]% - [description: yellow, stringy, adherent]
Eschar: [X]% - [description: black, brown, soft, hard]
Epithelial: [X]% - [description: pink, advancing margins]
Necrotic: [X]% - [description if present]
EXUDATE:
Type: [Serous/Serosanguinous/Sanguinous/Purulent]
Amount: [Scant/Small/Moderate/Large]
WOUND EDGES: [Attached/Rolled/Undermined/Epithelializing]
PERIWOUND SKIN: [Intact/Macerated/Erythematous/Indurated/Denuded]
TUNNELING: [None / Location by clock, depth]
UNDERMINING: [None / Location by clock, depth]
INFECTION SIGNS: [Present/Absent] - [If present: specify findings]
PAIN: [0-10 scale] - [Quality, timing]
ODOR: [None/Faint/Moderate/Foul]
PROCEDURE PERFORMED:
[Description including tissue type removed, method, instruments, anesthesia]
Pre-procedure tissue: [Description]
Tissue removed: [Quantify - e.g., "4.0 cm² necrotic slough"]
Deepest layer reached: [Epidermis/Dermis/Subcutaneous/Muscle/Bone]
Hemostasis: [Method achieved]
Post-procedure bed: [Description]
MEDICAL NECESSITY STATEMENT:
[Why skilled care is required - chronic wound, necrotic tissue present, risk of infection/deterioration, caregiver cannot perform]
TREATMENT PLAN:
Primary dressing: [Type, size]
Secondary dressing: [Type, size]
Frequency: [Daily/Every other day/Three times weekly]
Goals: [Quantifiable - e.g., "20% reduction in 14 days"]
Follow-up: [Date/timeframe]
Provider Signature: _________________ Date: _________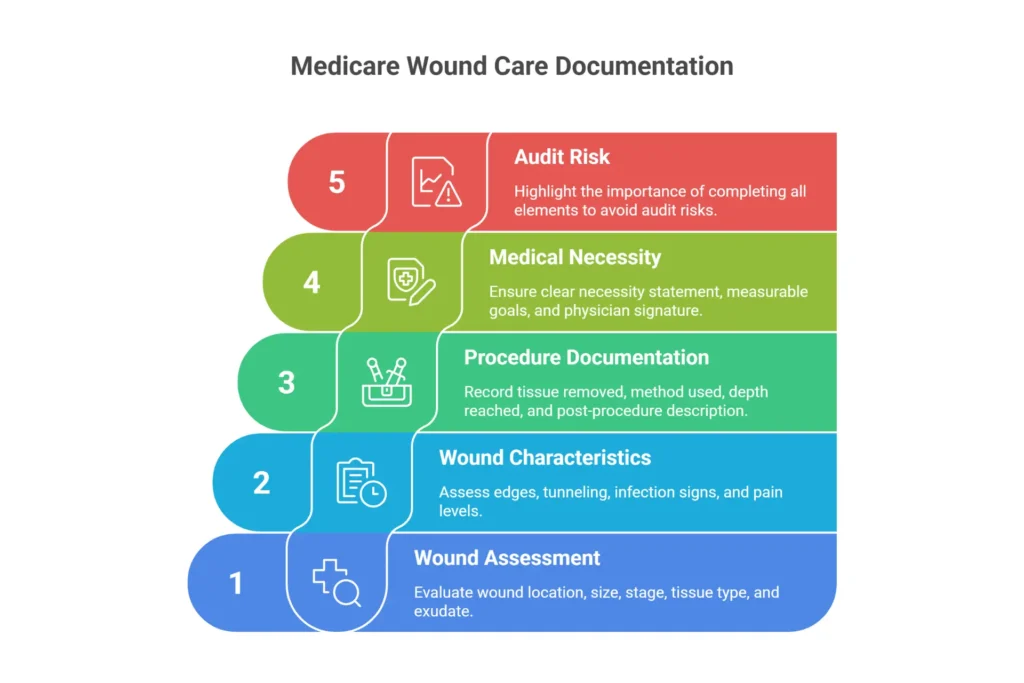
Documentation Red Flags That Trigger Audits
- Cloned notes – Identical assessments across visits are an immediate audit trigger
- Missing serial measurements – No comparison to baseline means no proof of progress
- Vague language – “Wound looks better” without supporting data
- Debridement without necrotic tissue documented – Why are you debriding healthy tissue?
- Missing 30-day failure documentation – Especially before advanced therapies
- No plan modification – Same treatment for 8 weeks with no documented rationale
- Inconsistent staging – Stage 3 one week, Stage 2 the next without explanation
Proper documentation isn’t just about compliance—it’s about protecting your revenue. If you’re dealing with frequent documentation-related denials, our medical coding specialists can help identify exactly where your notes are falling short.
CPT Codes for Medicare Wound Care Billing
This is where revenue lives or dies. Choosing the wrong code—or billing from the wrong place of service—can tank an otherwise solid claim. I’ve seen practices lose tens of thousands of dollars annually from coding errors that were completely preventable.
Active Wound Care Codes (97597-97610)
| Code | Description | 2026 Payment (Est.) | Key Requirements |
|---|---|---|---|
| 97597 | Selective debridement, ≤20 cm² | ~$75-100 | Scissors, forceps, waterjet; remove non-viable only |
| 97598 | Each additional 20 cm² | ~$40-60 | Add-on code to 97597 |
| 97602 | Non-selective debridement | Bundled (Status B) | NOT separately payable under PFS |
| 97605 | NPWT, ≤50 cm² | ~$200-250 | Requires 30-day failure; chronic wound |
| 97606 | NPWT, >50 cm² | ~$250-300 | Requires 30-day failure; chronic wound |
| 97607 | Disposable NPWT, ≤50 cm² | ~$180-220 | Same requirements as 97605 |
| 97608 | Disposable NPWT, >50 cm² | ~$220-280 | Same requirements as 97606 |
| 97610 | MIST ultrasound | ~$150 | Cannot bill same day as debridement |
Critical note on 97602: This code is Status B under the Physician Fee Schedule—meaning it’s bundled into E/M and not separately payable in office settings. It IS separately payable under OPPS in hospital outpatient departments. I see practices billing 97602 from POS 11 constantly, and it denies every time.
Surgical Debridement Codes (11042-11047)
| Code | Tissue Depth | POS Allowed | 2026 Payment (Est.) |
|---|---|---|---|
| 11042 | Subcutaneous, first 20 cm² | 11, 21, 22, 24, 31 | ~$135 |
| 11043 | Muscle/fascia, first 20 cm² | 21, 22, 24 only | ~$262 |
| 11044 | Bone, first 20 cm² | 21, 22, 24 only | ~$425 |
| 11045 | SubQ add-on, each additional 20 cm² | 11, 21, 22, 24, 31 | ~$68 |
| 11046 | Muscle add-on, each additional 20 cm² | 21, 22, 24 only | ~$122 |
| 11047 | Bone add-on, each additional 20 cm² | 21, 22, 24 only | ~$180 |
Critical Place of Service Restrictions
This is the single most common denial reason I see for wound care claims.
CPT codes 11043, 11044, 11046, and 11047 are excluded from POS 11 (Office). Medicare’s position is that deep debridement to muscle or bone requires the sterile environment and anesthesia capability of a facility setting.
Bill 11043 from your office? Automatic denial. No appeal will save you—you performed the service in the wrong setting according to Medicare policy. Either reclassify the service (if it was actually subcutaneous depth) or perform deep debridements in an appropriate facility.
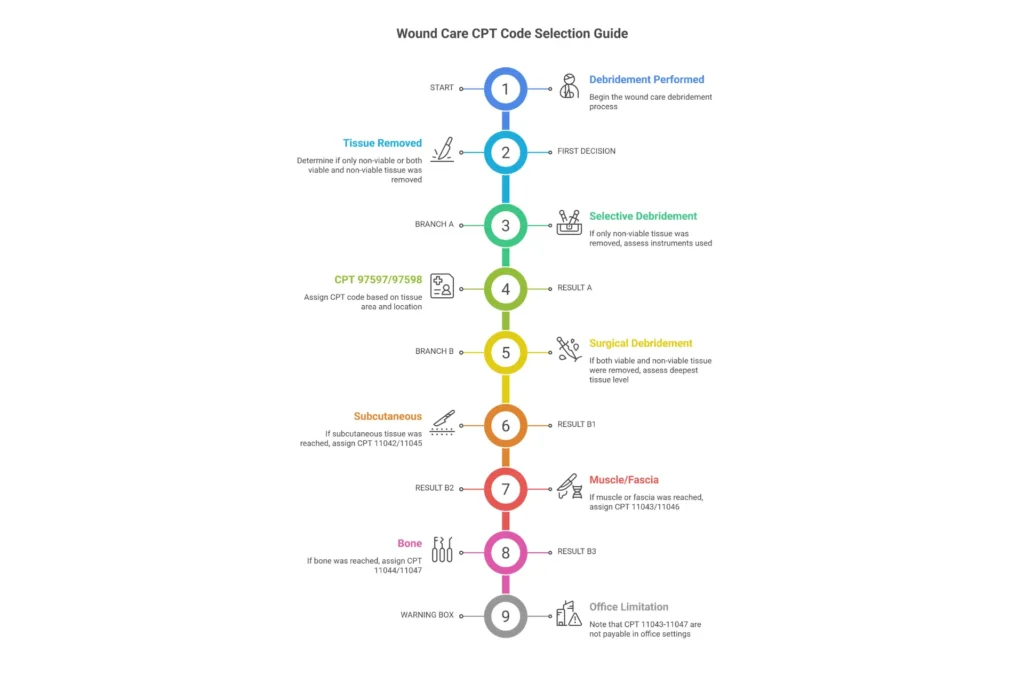
Code Selection: 97597 vs 11042—The Decision Framework
This question comes up constantly. Here’s how to decide:
Use 97597 (Selective Debridement) when:
- You’re removing non-viable tissue only
- Using scissors, forceps, curette, or high-pressure waterjet
- Working within epidermis or dermis
- Preserving all viable tissue
- The wound is superficial
Use 11042 (Surgical Debridement) when:
- You’re performing surgical excision with scalpel
- Removing both viable and non-viable tissue to reach clean margins
- Working down to subcutaneous tissue or deeper
- The wound requires aggressive wound bed preparation
The key distinction: Selective debridement removes only non-viable tissue. Surgical debridement removes tissue (including viable margins) to achieve a clean wound bed—it’s excisional.
You cannot bill both on the same wound. They’re mutually exclusive per NCCI edits. Pick the code that best represents your work.
Essential Modifiers for Wound Care
| Modifier | When to Use | Example |
|---|---|---|
| 25 | Significant, separately identifiable E/M same day | E/M + 11042 when E/M addresses separate issue |
| 59/XS | Distinct service, separate structure | Multiple wounds on different anatomical sites |
| XE | Separate encounter | Morning and afternoon procedures |
| LT/RT | Laterality | Right vs left lower extremity |
| T1-T9, F1-F9 | Specific digits | Toe or finger wounds |
| KX | Medical policy requirements met | Exceeding frequency limits with documentation |
| GP | Physical therapy plan of care | When PT performs 97597 |
NCCI Edits to Know
These code combinations will deny automatically:
- 97597 + 11042 same wound = Denial (mutually exclusive)
- 97602 + 97597 same wound = Denial (bundled)
- 97610 + debridement same wound same day = Denial
- 11042 + 11045 without proper documentation = Denial
For complex coding questions, especially involving multiple wounds or same-day procedures, consulting with specialists who understand wound care billing codes inside and out can prevent costly errors.
Local Coverage Determinations (LCDs) for Wound Care
If you’re billing Medicare for wound care, LCDs are your rulebook. And they vary significantly by where you practice. What flies in California might get denied in Florida.
What Are LCDs and Why Do They Matter?
Local Coverage Determinations are region-specific policies issued by Medicare Administrative Contractors (MACs). They define the specific coverage criteria, documentation requirements, and utilization limits for services like debridement, NPWT, and skin substitutes.
Here’s the hierarchy:
- NCD (National Coverage Determination) – Federal law, applies nationwide
- LCD – State/regional policy, can be stricter than NCD
- Billing Article (LCA) – Contains specific CPT/ICD-10 code requirements
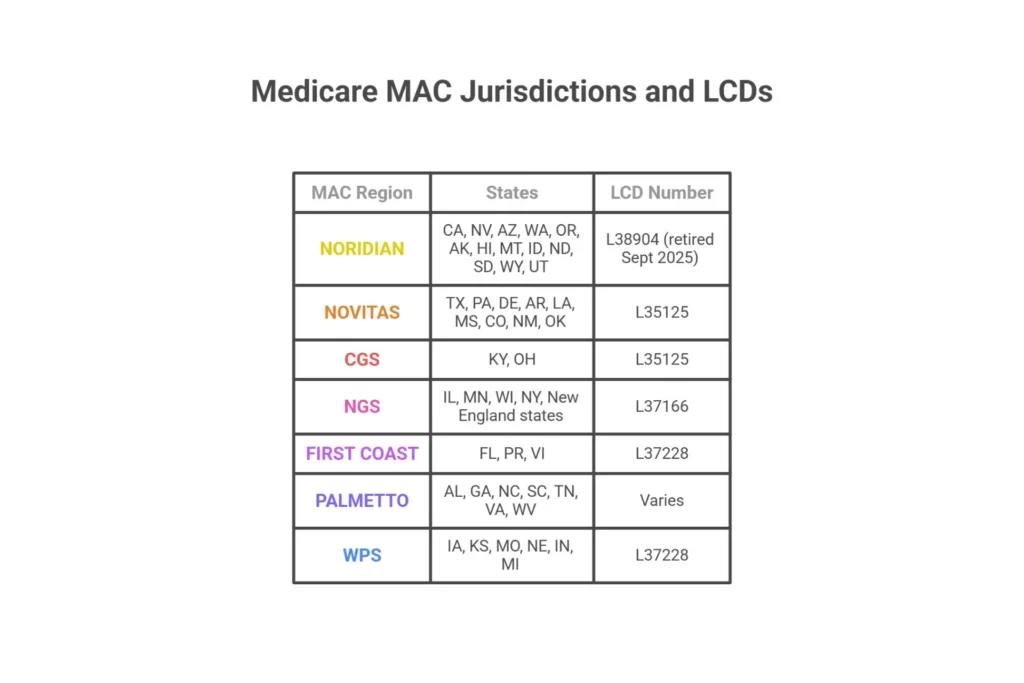
Key Wound Care LCDs by MAC Jurisdiction
| MAC | Jurisdiction | States | Primary LCD |
|---|---|---|---|
| Noridian | JE, JF | CA, NV, AZ, WA, OR, AK, HI, MT, ID, ND, SD, WY, UT | L38904 (retired Sept 2025) |
| Novitas | H, JL | TX, PA, DE, AR, LA, MS, CO, NM, OK | L35125 |
| CGS | J6, JK | KY, OH | L35125 |
| NGS | J6, JK | IL, MN, WI, NY, New England | L37166 |
| First Coast | JN | FL, PR, VI | L37228 |
| Palmetto | JJ, JM | AL, GA, NC, SC, TN, VA, WV | Varies |
| WPS | J5, J8 | IA, KS, MO, NE, IN, MI | L37228 |
What LCDs Typically Require
Most wound care LCDs share common requirements:
- 30-day standard care failure before advanced modalities
- Serial wound measurements at each visit (LxWxD in cm)
- Measurable progress documentation (percentage change)
- Physician reassessment at regular intervals (usually every 30 days)
- Specific tissue type documentation (percentages)
Utilization Limits You Must Know
- Debridement: Usually ≤4 selective (97597) per month, ≤12 surgical (11042-11044) per year
- Skin substitutes: Typically ≤8 applications per 12-week episode
- KX modifier: Required when exceeding limits with documented justification
2026 LCD Changes: What’s Different
L38904 (Noridian) retired September 2025 – Check for replacement policy L35125 (Novitas/CGS) revised January 2026 – New skin substitute criteria Unified Skin Substitute LCD withdrawn December 2025 – Each MAC sets own policy
How to Find Your LCD
- Go to the Medicare Coverage Database
- Select “LCDs”
- Filter by your state/MAC
- Search “wound care” or specific CPT code
- Check “Associated Documents” for the Billing Article
Understanding your specific MAC’s requirements is essential for compliance. If you’re operating across multiple jurisdictions, comprehensive medical billing services can help ensure you’re meeting each region’s distinct criteria.
What Wound Care Products Are Covered by Medicare?
Product coverage falls under two categories: DMEPOS (home use) and Part B incident-to supplies (clinic use). Getting this right affects both coverage and reimbursement.
Surgical Dressings Covered by Medicare
| Category | HCPCS Range | Clinical Use |
|---|---|---|
| Alginate | A6196-A6199 | High exudate wounds, promotes autolytic debridement |
| Foam | A6206-A6215 | Moderate to heavy drainage, pressure redistribution |
| Hydrocolloid | A6216-A6233 | Light to moderate exudate, self-adherent |
| Hydrogel | A6234-A6241 | Dry wounds, sloughy wounds, promotes autolysis |
| Collagen | A6021-A6024 | Chronic wounds, promotes granulation tissue |
| Transparent film | A6251-A6256 | Superficial wounds, moisture vapor permeable |
| Wound fillers | A6257-A6259 | Deep cavities, tunneling, undermining |
| Contact layers | A6266 | Prevents dressing adherence to wound bed |
| Specialty absorptive | A6242-A6248 | Heavy drainage, superabsorbent polymers |
Skin Substitutes/CTPs: 2026 Payment Overhaul
The biggest change in 2026: site-neutral, flat-rate payment effective January 1, 2026.
- Office rate: ~$127.28 per cm²
- HOPD rate: ~$127.14 per cm²
- Wastage payments: Eliminated
- Maximum applications: 8 per 12-week episode
- Requirement: 30-day standard care failure documented; 50% area reduction not achieved at week 4
This represents a fundamental shift from the previous high/low bundle system. The flat rate applies regardless of which product you choose, making clinical selection—not reimbursement optimization—the primary driver.
Medicare Coverage for Wound Care Graft Products
Medicare Part B covers amniotic membrane allografts and cellular and tissue-based products (CTPs) — including dehydrated and cryopreserved amniotic membrane grafts — under CPT codes 15271–15278 for the application procedure and product-specific Q-codes (Q4100–Q4255) for the graft itself. As of January 1, 2026, CMS reimburses most skin substitute products at the flat rate of ~$127.14 per cm², regardless of which product is used.
Coverage is subject to Local Coverage Determination (LCD) requirements specific to your MAC jurisdiction. To qualify, the wound must have failed at least 30 days of documented standard-of-care treatment, and medical necessity must be established through serial wound measurements, tissue type documentation, and physician assessment. The product applied must have a confirmed Q-code assignment — and that Q-code must match the product’s FDA documentation exactly on the claim.
✓ Medicare Part B Coverage Requirements
- ✓ 30 consecutive days of failed standard wound care documented
- ✓ Wound type: DFU, VLU, or pressure injury (per LCD)
- ✓ Serial wound measurements (LxWxD) at each visit
- ✓ Confirmed Q-code matching product FDA documentation
- ✓ Prior authorization per MAC jurisdiction where required
- ✓ Maximum 8 applications per 12-week episode (2026 rule)
⚠ The #1 Graft Claim Risk Most Providers Miss
An unverified graft product — one without pre-confirmed FDA HCT/P documentation, correct NDC numbers, and the right Q-code assignment — is the leading cause of Medicare skin substitute claim denials and RAC audit flags.
The Q-code on your claim must match the product in your hands. If your supplier has not pre-loaded and confirmed the correct Q-code before shipment, you are billing blind — and Medicare auditors know it.
Quick Reference — Wound Care Graft Billing Codes
We Supply DermaBind Grafts with Triple-Verified Medicare Coverage
Provider credentials verified. FDA documentation pre-loaded. Patient insurance confirmed before every application. Every enrolled account backed by 6-Year Claims Protection.
NPWT (Wound Vac) Coverage
- Pump (E2402): Capped rental for up to 4 months
- Supplies (A6550, A7000): Dressing kits and canisters covered while pump is medically necessary
- Qualifying wounds: Stage III/IV pressure ulcers, DFUs, VLUs, non-healing surgical wounds post-30 days
Standard Written Order (SWO) Requirements
Any surgical dressing requires a compliant SWO including:
- Patient name and MBI (Medicare Beneficiary Identifier)
- Order date (within 120 days of service)
- Detailed product description (HCPCS or brand/size)
- Quantity and frequency
- Wound diagnosis and anatomical location
- Physician signature (handwritten or compliant e-signature)
What’s NOT Covered
- OTC equivalents (standard adhesive bandages)
- Non-sterile gauze used alone
- Wound cleansers (bundled into procedure)
- Cosmetic products (scar reduction)
- Intact skin barriers (prevention products)
- Experimental treatments
- Products without HCPCS codes
Skilled Nursing Facility (SNF) Wound Care Billing
SNF billing is uniquely complex because you’re navigating PDPM, Consolidated Billing rules, and limited Part B carve-outs simultaneously.
PDPM: How Wound Care Drives SNF Reimbursement
Under the Patient-Driven Payment Model, wounds contribute to reimbursement through:
Nursing Component: Complex wounds (Stage III/IV pressure ulcers, multiple wounds, surgical wounds) place patients in higher-paying nursing case-mix groups.
NTA Component: Wounds earn “points” that boost the Non-Therapy Ancillary score. A Stage IV pressure ulcer can add significant daily revenue—especially during the first 3 days when the 3x NTA multiplier applies.
What’s Bundled into Part A Per Diem
All of these services are included in the SNF’s daily rate—the facility cannot bill them separately:
- Nursing-performed debridement (selective, non-surgical)
- All supplies and dressings
- NPWT supplies
- Topical medications
- Assessments and dressing changes
Part B Carve-Outs: What Physicians CAN Bill
Only physician/NPP professional services are carved out:
- E/M visits (99304-99310, 99315-99316)
- Surgical debridement (11042-11047) performed by physician
- Podiatry services (per NCD 70.2 criteria)
Critical rule: Therapy codes like 97597 performed by PT or OT are bundled into Part A. The SNF absorbs that cost. If your physical therapist performs selective debridement during a Part A stay, you cannot bill it to Part B.
MDS Documentation for PDPM
Section M (Skin Conditions) drives PDPM payment:
- M1300: Risk Assessment
- M1306-M1311: Pressure ulcer staging and count
- M1320-M1324: Stasis ulcers
- M1330-M1350: Surgical wounds
Accurate MDS coding directly impacts facility reimbursement. Inaccurate staging—either over or under—is a primary target for OIG audits.
Home Health Wound Care Medicare Billing
The home health setting has its own eligibility requirements and payment model. Understanding PDGM is essential for both agencies and referring physicians.
Does Medicare Cover Daily Wound Care at Home?
Yes—but only temporarily and under strict conditions. Coverage requires the patient to be homebound, need skilled nursing for an unstable wound (heavy drainage, infection signs, post-debridement care), and have a physician-certified plan of care. Daily visits are typically approved for 1-3 weeks for complex wounds. Once the wound stabilizes and a caregiver can manage dressing changes, daily visits are no longer covered. Routine maintenance is excluded.
Eligibility Requirements
Homebound status: Leaving home requires considerable and taxing effort. Examples:
- Patients who need ambulance transport
- Those who can only leave with assistance of another person
- Leaving home is medically contraindicated
Skilled nursing need: The wound care must be so complex that only a licensed nurse can safely perform it:
- Sharp debridement requiring clinical judgment
- NPWT management and troubleshooting
- Assessment for signs of systemic infection
- Teaching caregivers aseptic technique
Physician certification: Required initially and for recertification every 60 days.
Face-to-face encounter: Within 90 days prior or 30 days after start of care.
PDGM Payment Model
Home health agencies receive 30-day episode payments. Wounds fall into the highest case-mix weight clinical group (“Wounds”). The payment bundles:
- All nursing visits
- All routine supplies (dressings, gauze, tape)
- Therapy services
OASIS Documentation
The OASIS assessment drives payment. Key wound items:
- M1300-M1309: Pressure ulcer staging
- M1322-M1324: Stasis ulcers
- M1330-M1350: Surgical wounds
Accurate OASIS coding is essential—it directly determines the 30-day payment amount.
Common Medicare Wound Care Denials and Appeals
Denials happen. Understanding why—and how to fight back effectively—protects your revenue.
Top Denial Codes for Wound Care
| Code | Meaning | Common Trigger | Solution |
|---|---|---|---|
| CO-50 | Medical necessity not established | Missing 30-day failure, vague documentation | Add measurements, tissue types, necessity statement |
| CO-4 | Procedure/modifier inconsistent | Missing Modifier 25 or 59 | Review modifier requirements; resubmit with correction |
| CO-97 | Bundled service | 97597 + 11042 same wound | Pick appropriate single code |
| CO-16 | Missing information | No measurements, missing signature | Complete documentation and resubmit |
| CO-11 | Diagnosis inconsistent | Stage 2 ulcer with bone debridement | Verify staging matches procedure depth |
| CO-18 | Duplicate claim | Same service rebilled | Check for prior payment |
| M76 | Place of service issue | 11043 from POS 11 | Perform in facility or recode to 11042 |
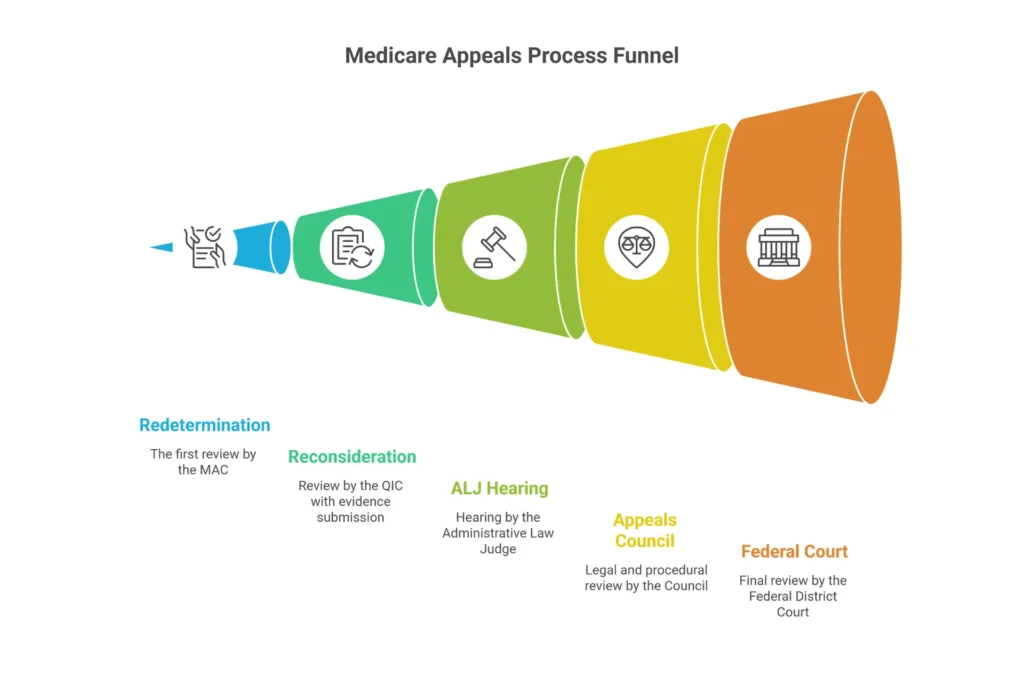
The 5-Level Medicare Appeals Process
Level 1: Redetermination (MAC)
- Deadline: 120 days from denial
- Format: Written request with supporting documentation
- Success rate: ~15-20%
Level 2: Reconsideration (QIC)
- Deadline: 180 days from Level 1 decision
- Important: Cannot add new evidence after this level
- Success rate: ~25-30%
Level 3: ALJ Hearing
- 2026 Amount in Controversy: $200 minimum
- Format: Usually video or telephone hearing
- Success rate: ~60% (highest success level)
Level 4: Medicare Appeals Council
- Written review of ALJ decision
- Focuses on legal/procedural errors
Level 5: Federal District Court
- 2026 Amount in Controversy: $1,960 minimum
- Judicial review
Building a Winning Appeal Package
Your appeal should include:
- Full procedure notes with all measurements
- Dated photographs with ruler visible
- Medical necessity statement referencing LCD criteria
- Timeline showing wound progression (comparison table)
- Peer-reviewed literature supporting necessity
- Coding rationale with CPT guidelines
- Physician attestation letter
If denials are eating into your revenue, our specialized wound care billing services include comprehensive denial management and appeals support with documented success rates.
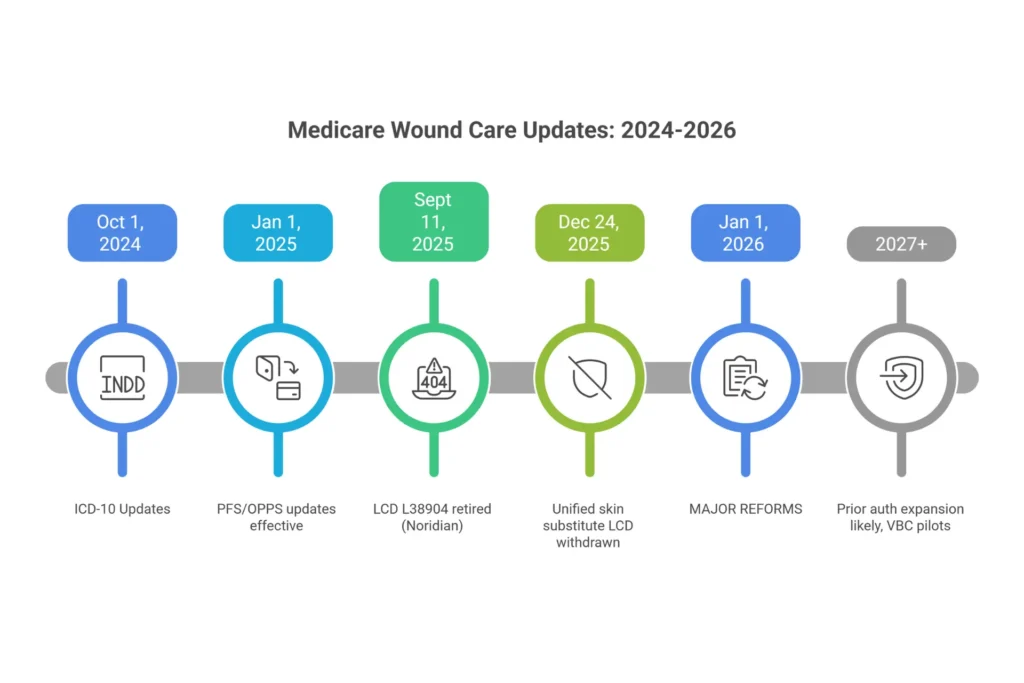
2024-2026 Medicare Wound Care Updates
The last three years have brought the most significant changes to wound care reimbursement in decades. Here’s what you need to know.
2026: The Year of Major Reform
Skin Substitute Reimbursement Overhaul (Effective January 1, 2026)
- Site-neutral, flat-rate payment: ~$127 per cm²
- Wastage payments eliminated—paid only for amount used
- CTPs classified as “incident-to” supplies
- 8-application maximum per 12-week episode
- KX modifier required after application 4
WISeR Model Launch
- Wasteful and Inappropriate Service Reduction (WISeR) prior authorization pilot
- Mandatory in selected states for skin substitutes
- Targeting high-volume CTP utilization patterns
Physician Fee Schedule Changes
- Dual conversion factors: $33.57 (QPs) / $33.40 (non-QPs)
- Efficiency adjustment: -2.5% for many procedure codes
- Debridement codes saw modest rate reductions
2025 LCD Changes
- L38904/A58567 retired September 2025 (Noridian)
- L35125/A53001 revised January 2026 (Novitas/CGS)
- Unified national skin substitute LCD proposed then withdrawn December 2025
2024 ICD-10 Updates
New codes for surgical wound disruption (effective October 1, 2024):
- T81.320A-S (superficial disruption)
- T81.321A-S (deep disruption)
- T81.328A-S (other/unspecified)
- Old code T81.32XA deleted
What’s Coming: 2027 and Beyond
- Prior authorization expansion likely for CTPs and NPWT
- Value-Based Care pilots for wound care
- AI photo analysis and RPM codes gaining traction
- Outcomes-based reimbursement experiments
Staying current with these changes is challenging for any practice. Working with an end-to-end revenue cycle management partner ensures your practice adapts to regulatory shifts without missing revenue opportunities.
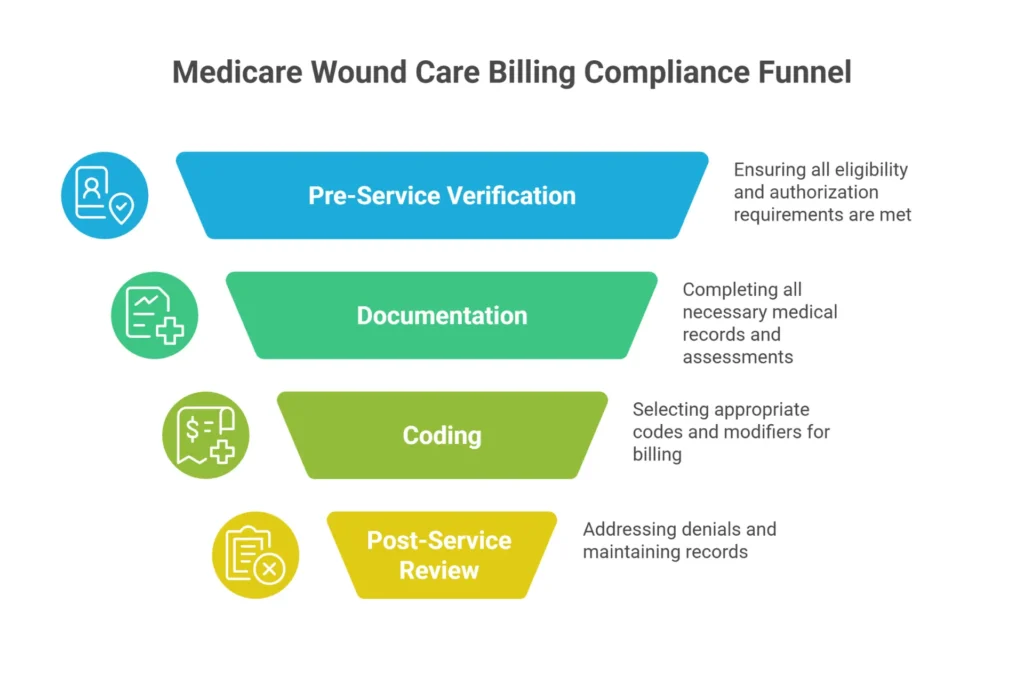
Medicare Wound Care Billing Compliance Checklist
Use this checklist before every claim submission. Print it, laminate it, put it next to every workstation.
Pre-Service Verification
- Verify Medicare eligibility and coverage
- Confirm medical necessity (30-day failure documented if applicable)
- Check LCD requirements for your MAC jurisdiction
- Obtain prior authorization if required (CTPs, NPWT in some MACs)
- Verify provider enrollment and credentialing status
- Confirm patient is homebound (for home health)
Documentation Checklist
- Complete wound assessment with LxWxD measurements in centimeters
- Document anatomical location with laterality
- Record wound stage/classification
- Document tissue type percentages (granulation, slough, eschar, epithelial)
- Record exudate type and amount
- Document edges, periwound condition, tunneling/undermining
- Note infection signs (present or absent with findings)
- Include pain assessment
- Record procedure method, instruments, tissue removed
- Quantify tissue removed (cm²)
- State medical necessity clearly
- Document measurable goals and treatment plan
- Include photographs with ruler (recommended)
- Physician signature on assessment and orders
Coding Verification
- Select CPT based on deepest tissue removed
- Verify POS matches code requirements (11043-11047 only in facility)
- Link appropriate ICD-10 codes (specific laterality, stage)
- Apply correct modifiers (25, 59/XS, KX, LT/RT)
- Check NCCI edit conflicts
- Verify no duplicate billing
- Confirm frequency limits not exceeded (or KX applied with justification)
Post-Service Review
- Review remittance advice for denials
- Address denials within 120 days
- Maintain records 7+ years
- Update treatment plan at 30-day intervals
- Track wound progression against benchmarks
Get a Free Medicare Wound Care Billing Compliance Review →
Frequently Asked Questions (FAQ)
Does Medicare cover daily wound care?
Yes, under the Home Health Part A benefit when the patient is homebound and requires skilled nursing for wound care that a caregiver cannot safely perform. Daily visits are typically approved for 1-3 weeks for unstable wounds with heavy drainage, signs of infection, or post-debridement care requirements. Once the wound stabilizes and a caregiver is trained in dressing changes, daily visits are no longer covered. Routine maintenance dressing changes are excluded from coverage.
What wound care products are covered by Medicare?
Medicare covers surgical dressings including alginates (A6196-A6199), foams (A6206-A6215), hydrocolloids (A6216-A6233), hydrogels (A6234-A6241), collagen dressings (A6021-A6024), transparent films (A6251-A6256), and wound fillers (A6257-A6259) for wounds resulting from surgery or debridement. Skin substitutes/CTPs are covered after documented 30-day standard care failure, with 2026 flat-rate payment of approximately $127 per cm². NPWT supplies (E2402 pump, A6550 dressing kits, A7000 canisters) are covered for qualifying Stage III/IV pressure ulcers, diabetic foot ulcers, and non-healing surgical wounds. All dressing orders require a physician Standard Written Order with diagnosis and wound description.
What is the Rule of 30 in wound care?
The Rule of 30 requires a wound to show no measurable improvement after at least 30 consecutive days of standard treatment before advanced therapies like skin substitutes or NPWT are covered by Medicare. Standard care includes appropriate debridement, dressings, off-loading, compression (for venous ulcers), and infection management. At the 30-day mark, you must document baseline versus current measurements, lack of progress in wound size or tissue quality, reassessment of healing barriers (infection, nutrition, vascular status), and modifications to the treatment plan. This establishes the wound as “chronic” and eligible for advanced therapy coverage.
What is the 2-2-2 Rule in Medicare wound care?
The 2-2-2 Rule is a clinical benchmark stating that a wound should demonstrate approximately 20% surface area reduction within 2 weeks of treatment, approximately 2mm diameter reduction every 2 weeks, or approximately 2cm² area reduction monthly. This formula measures healing trajectory and predicts whether a wound will likely close by week 12. Failure to meet this benchmark requires documented reassessment and treatment plan modification. You can still bill services if the benchmark isn’t met, but documentation must explain why progress is lacking (comorbidities, infection, vascular disease) and what changes you’re implementing.
Can you bill E/M and debridement on the same day?
Yes, with Modifier 25 appended to the E/M code. The E/M service must be significant and separately identifiable from the wound procedure—meaning it addresses a distinct clinical issue beyond the wound itself. For example, if you evaluate new fever, adjust diabetes medications, or address an unrelated complaint during the same visit, that qualifies. Document both services with separate medical necessity statements. The E/M portion should stand on its own as a justified service.
How often can you bill for wound debridement?
Most LCDs allow up to 4 selective debridements (97597) per month and up to 12 deep surgical debridements (11043-11047) per year. Exceeding these limits requires the KX modifier plus documented evidence of progress (such as 20% size reduction) and physician reassessment. Without this justification, claims exceeding frequency limits will be denied automatically. The key is documenting that continued debridement is medically necessary—not just routinely scheduled.
Is CPT 97602 payable under Medicare?
CPT 97602 (non-selective debridement) has Status B under the Physician Fee Schedule—meaning it’s bundled into E/M services and NOT separately payable in office settings (POS 11). It IS separately payable under OPPS in hospital outpatient departments (POS 22). If you’re billing 97602 from your office, it will deny. This is one of the most common billing errors I see in wound care.
Do I need prior authorization for wound care?
For Original Medicare, prior authorization is not required for routine debridement or surgical dressings. However, skin substitutes/CTPs require prior authorization in many MAC jurisdictions, especially for applications beyond standard frequency limits (typically after 4 applications). The WISeR Model, launching in 2026, implements mandatory prior authorization for skin substitutes in selected states. Medicare Advantage plans frequently require prior authorization for most advanced wound therapies. Always verify requirements with your specific MAC and payer before providing advanced services.
What documentation is needed for skin substitutes?
For Medicare coverage of skin substitutes/CTPs, you must document: (1) 30 consecutive days of standard care that failed to produce measurable improvement; (2) baseline wound measurements and weekly measurements thereafter; (3) 50% area reduction not achieved by week 4; (4) diagnosis of diabetic foot ulcer (DFU) or venous leg ulcer (VLU)—most LCDs limit CTP coverage to these wound types; (5) physician attestation of medical necessity; and (6) prior authorization if required by your MAC or for applications beyond the standard limit.
How do I bill wound care under Medicare?
Bill wound care using CPT codes based on the deepest tissue removed during debridement. Use 97597 and 97598 for selective debridement with scissors, forceps, or waterjet. Use 11042 through 11047 for surgical debridement with scalpel, selecting the code based on depth—subcutaneous, muscle, or bone. Document wound measurements in centimeters, tissue types by percentage, and medical necessity for skilled care. Always verify your place of service allows the code you’re billing—11043 through 11047 are only payable in facility settings, not physician offices.
What documentation does Medicare require for wound debridement?
Medicare requires wound measurements including length, width, and depth in centimeters at every visit. You must document tissue type percentages for granulation, slough, eschar, and epithelial tissue. The procedure note must describe tissue removed, instruments used, and the deepest layer reached. Include exudate type and amount, periwound condition, and signs of infection. A clear medical necessity statement explaining why skilled care is required is essential. Include photographs with a ruler when possible for audit defense.
How long does Medicare pay for wound care treatment?
Medicare pays for wound care as long as it remains medically necessary with documented progress. Wounds must show measurable improvement every 30 days. If no improvement occurs, you must document barriers to healing and modifications to the treatment plan. Advanced therapies like skin substitutes typically have episode limits—usually 8 applications per 12-week episode. There’s no absolute time limit, but continued treatment requires ongoing justification through serial measurements and documented clinical necessity.
Why was my wound care claim denied by Medicare?
Common denial reasons include missing medical necessity documentation, billing deep debridement codes 11043 through 11047 from a physician office instead of a facility, exceeding frequency limits without KX modifier and justification, billing mutually exclusive codes on the same wound such as 97597 with 11042, incomplete wound assessments without measurements, and missing physician signature. Check your remittance advice denial code—CO-50 indicates medical necessity issues, CO-4 indicates modifier problems, and CO-97 indicates bundling violations.
What qualifies as a chronic wound for Medicare coverage?
Medicare considers a wound chronic when it fails to show measurable improvement after 30 consecutive days of appropriate standard care. Standard care includes debridement of necrotic tissue, appropriate moisture-management dressings, off-loading for diabetic foot ulcers, compression therapy for venous leg ulcers, infection management, and nutritional optimization. You must document baseline measurements, the 30-day treatment history, lack of progress in wound size or tissue quality, and reassessment of healing barriers before a wound qualifies as chronic for advanced therapy coverage.
Does Medicare cover wound vac therapy at home?
Yes, Medicare covers Negative Pressure Wound Therapy at home under the DME benefit. The NPWT pump is billed under HCPCS code E2402 as a capped rental for up to 4 months. Supplies including dressing kits and canisters are covered under codes A6550 and A7000 while the pump remains medically necessary. Qualifying wounds include Stage III and IV pressure ulcers, diabetic foot ulcers, venous and arterial ulcers, and non-healing surgical wounds after 30 days of documented standard care failure.
How much does Medicare pay for wound debridement?
Medicare payment for wound debridement varies by code and setting. In 2026, CPT 97597 pays approximately $75 to $100 in non-facility settings. CPT 11042 for subcutaneous debridement pays approximately $135. Deep debridement codes 11043 for muscle and 11044 for bone pay approximately $262 and $425 respectively, but are only payable in facility settings. Actual payment depends on your geographic locality adjustment and whether you’re billing facility or professional fees. Check the Medicare Physician Fee Schedule lookup tool for your specific area.
What is the difference between selective and surgical debridement?
Selective debridement, coded as CPT 97597 and 97598, removes only non-viable tissue using instruments like scissors, forceps, curettes, or high-pressure waterjet while preserving healthy tissue. It’s typically performed within the epidermis and dermis layers. Surgical debridement, coded as CPT 11042 through 11047, is excisional—removing both viable and non-viable tissue with a scalpel to achieve clean wound margins. The depth of the deepest tissue removed determines the specific 11042 series code. You cannot bill both on the same wound during the same session.
Conclusion
Medicare wound care billing in 2026 demands precision. The rules are more complex than ever—from the 30-day chronicity requirement to the 2-2-2 healing benchmarks, from place of service restrictions on deep debridement codes to the new flat-rate skin substitute payments that have fundamentally changed CTP economics.
But here’s what I’ve learned after fifteen years in this space: the practices that thrive aren’t the ones with the fanciest EHR systems or the highest patient volume. They’re the ones that understand Medicare’s rules and document accordingly. Every measurement you record, every tissue type you describe, every medical necessity statement you write—these aren’t just checkboxes. They’re the foundation of your reimbursement and your audit defense.
The providers who struggle are invariably the ones who view documentation as a burden rather than a business necessity. They’re the ones who assume their clinical skill alone will protect them when auditors come calling. It won’t. Only documentation will.
If there’s one takeaway from this guide, it’s this: Medicare wound care billing is a system. Learn the system—the rules, the benchmarks, the LCD requirements, the coding nuances—and you’ll protect your revenue while providing excellent patient care. Ignore the system, and you’ll spend more time on appeals than on patients.
The complexity isn’t going away. If anything, 2027 will bring more prior authorization requirements, more documentation scrutiny, and more audit activity. The practices that invest in compliance infrastructure now will be the ones that thrive. The ones that don’t? They’ll be writing refund checks.
Ready to Get Your Medicare Wound Care Billing Right?
At EliteMed Financials, we’ve spent over 15 years helping wound care providers navigate Medicare’s complex reimbursement landscape. We’ve seen every denial code, fought every appeal level, and helped practices recover hundreds of thousands in lost revenue.
Our wound care billing specialists understand:
- LCD requirements across all MAC jurisdictions
- CPT code selection for maximum compliant reimbursement
- Documentation standards that pass audit scrutiny
- The 2026 regulatory changes and how to adapt
Our Services for Wound Care Providers
Wound Care Billing Services – Complete claim submission, denial management, and appeals support
Medical Coding Services – Expert code selection to maximize compliant reimbursement
RCM Services – End-to-end revenue cycle management from charge capture to collection
Medicare Credentialing – Get enrolled and maintain compliant enrollment status
End-to-End Practice Management – Comprehensive financial services including billing, credentialing, and practice optimization
📞 Call (307) 243-8064 for a Free Medicare Wound Care Billing Compliance Review
Let us identify gaps in your current process and show you exactly where you’re leaving money on the table—or exposing yourself to audit risk.

Related Resources:
- Wound Care Billing Codes: Complete 2026 Guide
- Revenue Cycle Management Best Practices
- How to Improve Revenue Cycle Management
- Healthcare Revenue Cycle Fundamentals
- Revenue Cycle Management Process
Last updated: February 2026 | This guide reflects current CMS regulations, LCD requirements, and 2026 fee schedule rates. Medicare policies change frequently—always verify current requirements with your MAC and the Medicare Coverage Database.

