
By a 15-Year Veteran of Healthcare Revenue Cycle Management
If you’re reading this, chances are you’ve got a stack of denied claims for debridement procedures gathering dust, your accounts receivable is creeping past that 45-day mark you swore you’d never hit, and the 2026 CMS changes to skin substitute reimbursement have your head spinning. I’ve been there. Not as a consultant looking in—but as a billing manager who lived through the chaos of the 2020s, watching practices hemorrhage revenue because they couldn’t keep up with the breakneck pace of regulatory change.
Here’s the truth I’ve learned after 15 years in wound care revenue cycle management: the margin for error has vanished. With CMS now paying a flat $127.28 per square centimeter for skin substitutes and AI-powered audit programs like WISeR (Wound Integrity & Searchable Reporting) scrutinizing every debridement claim, you can no longer afford a “good enough” billing operation.
This guide is everything I wish someone had handed me when I was making the outsourcing decision for my own practice. We’ll cover the real costs, the hidden traps, the questions your vendors hope you won’t ask, and the exact metrics that separate industry leaders from “claim pushers.”
Let’s get your revenue cycle where it needs to be.
Table of Contents
Why Healthcare Providers Outsource Wound Care Billing
In my first year managing billing for a multi-specialty group, I remember a podiatrist walking into my office with a stack of 50 denials. “I debrided the wound,” he said. “Why won’t they pay?” I had to explain—gently—that “debridement” isn’t a single service. There’s selective debridement (CPT 97597), surgical debridement of subcutaneous tissue (CPT 11042), and a dozen variations in between. And if his documentation didn’t specify depth? Denied. If he didn’t measure the wound? Denied. If he used a skin substitute without tracking the exact square centimeter wastage? You guessed it—denied.
That moment taught me something that’s only become more true in 2026: wound care billing isn’t like other billing. It sits at the intersection of surgical coding, supply chain management, and physical therapy documentation. And this year, with the new bundled payment model for cellular and tissue-based products (CTPs), the complexity has peaked.
The Growing Complexity of Wound Care Billing in 2026
Let me paint you a picture of what your billing team is up against right now.
The Debridement Hierarchy Problem
CPT 97597 (selective debridement) and CPT 11042 (surgical debridement of subcutaneous tissue) look similar on paper. But in practice, they represent fundamentally different procedures with different documentation requirements. Your biller needs to know that if the provider removed devitalized tissue from the surface, it’s 97597. But if they went deeper—into subcutaneous tissue—it’s 11042. And if they did both on the same wound? You only bill the deepest layer. Miss that nuance, and you’re either leaving money on the table or inviting an audit from the Office of Inspector General (OIG).
I’ve seen practices lose $50,000 in a single quarter because their in-house team consistently coded 11042 when 97597 was appropriate—triggering automatic scrutiny from Centers for Medicare & Medicaid Services.
The 2026 Skin Substitute Shift
This is the big one. In 2026, CMS finalized the transition of skin substitutes from a “buy-and-bill” Average Sales Price (ASP) model to a bundled payment system. The flat rate is now approximately $127.28 per square centimeter, paid as an incident-to supply.
What does this mean operationally? Your billing team must now:
- Track exact square centimeter usage per application
- Document wastage precisely
- Verify that the product used aligns with your MAC’s Local Coverage Determination (LCD)
- Understand that different Medicare Administrative Contractors (MACs) like Novitas Solutions vs. Palmetto GBA have different frequency limits—some automatically flag more than 8 debridements in a 12-week period unless specific “healing trajectory” documentation exists
I recently consulted for a clinic that lost $420,000 in a Medicare clawback because their billing firm kept billing skin substitutes at the old ASP+6% rate, unaware that the rules had changed. The firm’s defense? “We were just following the provider’s superbill.” The practice’s defense? None. The money was gone.
The Documentation Trinity
Here’s a phrase I want you to remember: Measurement, Tissue Type, Medical Necessity. Every wound care claim must satisfy all three.
- Measurement: Length, width, depth—updated weekly, not just at the initial visit
- Tissue Type: Percentage of eschar, slough, or granulation tissue
- Medical Necessity: Why this treatment over a less invasive option? If the wound isn’t showing 20% reduction in size over 4 weeks, many payers will deny continued treatment
In-house teams—especially generalist billers—rarely have the training to catch documentation gaps at this level. They see a superbill with a code, they submit it. The denial comes 45 days later. By then, the provider barely remembers the patient.
Top 8 Benefits of Outsourcing Wound Care Billing
After a decade and a half in this industry, I’ve compiled the metrics that actually matter. Here’s what specialized wound care billing services deliver:
1. Denial Rate Reduction: 40-60%
In-house teams average 12-18% denial rates. Specialized wound care outsourcers? Under 5%. That’s not a marginal improvement—that’s the difference between a profitable practice and one that’s bleeding cash.
2. Clean Claim Rate: 95-98%
Compare that to the 72-78% in-house average. Clean claims get paid in weeks. Dirty claims take months—if they get paid at all.
3. Days in AR: 28-34 days
In-house averages 45-55 days. The math is simple: faster AR means better cash flow means you can actually pay your staff and invest in growth.
4. Net Revenue Uplift: 10-15%
This isn’t just cost savings—it’s capturing revenue you’re currently leaving on the table. Missed modifiers, unbundled procedures, incorrectly coded depth—specialized coders find these errors and fix them.
5. 40-60% Overall Cost Savings
When you factor in salary, benefits, software licenses, training, and the hidden cost of turnover, in-house billing costs 10-15% of collections. Outsourcing at 5-8% is simply cheaper.
6. Regulatory Compliance Without the Headache
LCDs change. MAC frequency limits shift. In 2026, staying current requires dedicated monitoring. Outsourcing firms have teams whose only job is tracking these updates.
7. AI-Driven Claim Scrubbing
Top firms use tools like Waystar and Optum360 that flag missing measurements, incorrect modifiers, and documentation gaps BEFORE submission. In-house teams often can’t afford these tools.
8. Cybersecurity Protection
With healthcare data breaches at an all-time high, shifting liability to a SOC2-compliant partner isn’t just smart—it’s essential.
Access to Medicare-Covered Graft Products with Built-In Billing Support — No Separate Supplier Needed
Most wound care billing companies handle your claims. Most graft suppliers handle your products. None of them do both — except Elite Med Financials. As an authorized representative for DermaBind amniotic wound care grafts (Medicare Part B covered, TL and FM product lines), we are the only billing partner that supplies the graft product and manages the complete claim cycle for that product — under one roof, with one point of accountability.
When you outsource billing to a standard company and order grafts from a separate supplier, you create a dangerous gap: the supplier has no visibility into your billing, and your billing company has no visibility into product compliance. That gap is where Q-code mismatches, documentation failures, and audit flags live. When your graft supplier and billing partner are the same company, that gap disappears entirely.
Provider credentials, FDA documentation, and patient insurance confirmed before every application
The only graft program in the market that backs every verified claim with 6-year audit defense — at no extra cost
DermaBind TL & FM billed under CPT 15271–15278 + pre-loaded Q-codes, with ~$127.14/cm² 2026 flat-rate compliance built in
The result: one outsourced partner handles your graft supply, your graft billing, and your graft audit defense. No coordination overhead. No finger-pointing between vendor and billing company when a claim is denied.
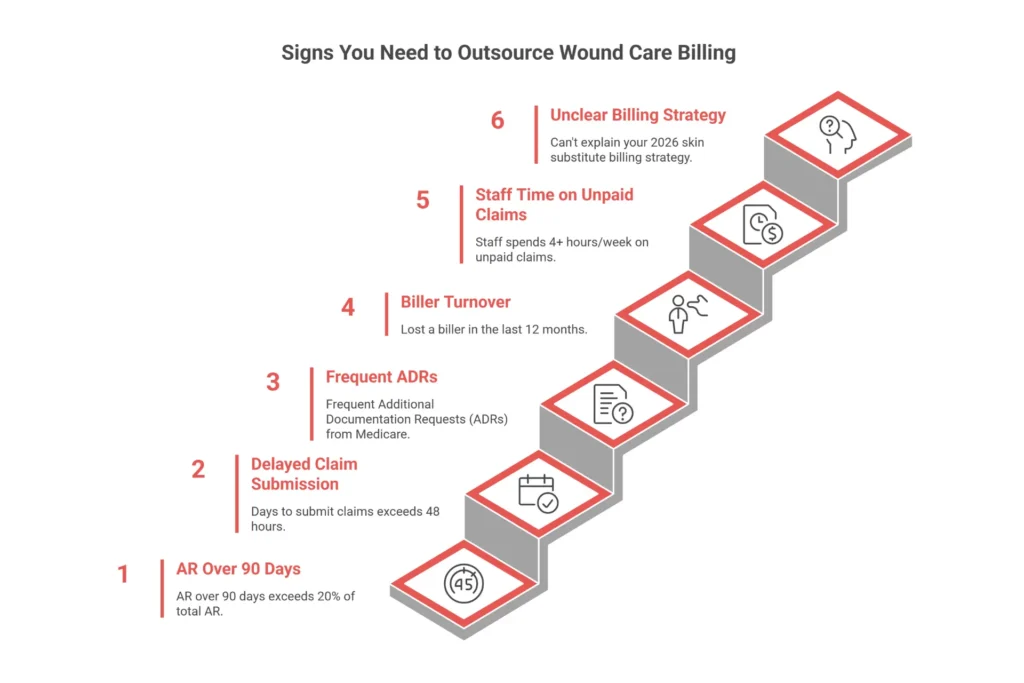
See our graft program →Warning Signs Your Practice Needs to Outsource
How do you know if you’re a candidate? I use a simple diagnostic with every practice I advise. If any of these apply, you need help.
🚩 Your AR over 90 days exceeds 20% of total AR. That’s not “slow-paying insurance.” That’s revenue you’ll never see.
🚩 Your “Days to Submit” (time from encounter to claim filing) exceeds 48 hours. Every hour you delay is an hour your cash flow is strangled.
🚩 You’re receiving frequent Additional Documentation Requests (ADRs) from Medicare. This means your claims are raising red flags.
🚩 You’ve lost a biller in the last 12 months. The knowledge drain from turnover costs an average of 15% of revenue.
🚩 Your staff spends more than 4 hours a week discussing unpaid claims instead of patient care. The administrative burden has exceeded your capacity.
🚩 You can’t explain your 2026 skin substitute billing strategy. If you don’t know how you’re handling the flat-rate bundle, you’re already behind.
In my experience, the practices that wait until they’re in crisis mode lose the most. If you’re nodding along to even two of these, it’s time to start the conversation.
Ready for a personalized assessment of your current billing health? Contact our wound care billing specialists for a complimentary 30-minute consultation.
In-House vs Outsourced Wound Care Billing: Complete Comparison
I’ve run in-house billing departments. I’ve managed outsourced relationships. I’ve cleaned up the mess when practices switched from one to the other. Here’s the unvarnished truth: neither option is inherently right or wrong—it depends on your volume, your complexity, and your tolerance for risk.
But in 2026, with the new CMS rules in full effect, the scales have tipped dramatically toward outsourcing for most practices.
Cost Comparison: The Real Numbers
Let’s start with the numbers. I’ve modeled this for a mid-sized wound care practice collecting $2 million annually—roughly 1,000-1,200 claims per month.
| Cost Component | In-House (Annual) | Outsourced (Annual) |
| Staffing (2 billers @ $58,000 + 30% benefits) | $150,800 | $0 |
| Billing Software / EMR Seats | $12,000 | Included |
| Clearinghouse Fees | $3,600 | Included |
| Training & Compliance (CPT updates, CEUs) | $8,500 | Included |
| Overhead (Space, Equipment, IT) | $10,000 | $0 |
| Total Annual Cost | $184,900 | $120,000-$140,000 |
| Cost as % of Collections | 9.2% | 6-7% |
Based on $2M annual collections. In-house costs vary by region and benefit structure.
But here’s where the math gets interesting. The table above only shows direct costs. It doesn’t account for revenue leakage—the money you lose from denials, undercoding, and slow payments.
When I audit in-house billing operations, I typically find:
- Denial rates of 12-18% vs. outsourced benchmarks of 3-5%
- Clean claim rates of 78-84% vs. outsourced 95-98%
- Days in AR of 45-55 vs. outsourced 28-34
That 10-15% higher denial rate on a $2M practice represents $200,000-$300,000 in lost revenue annually. Suddenly, the “cheaper” in-house option doesn’t look so cheap.
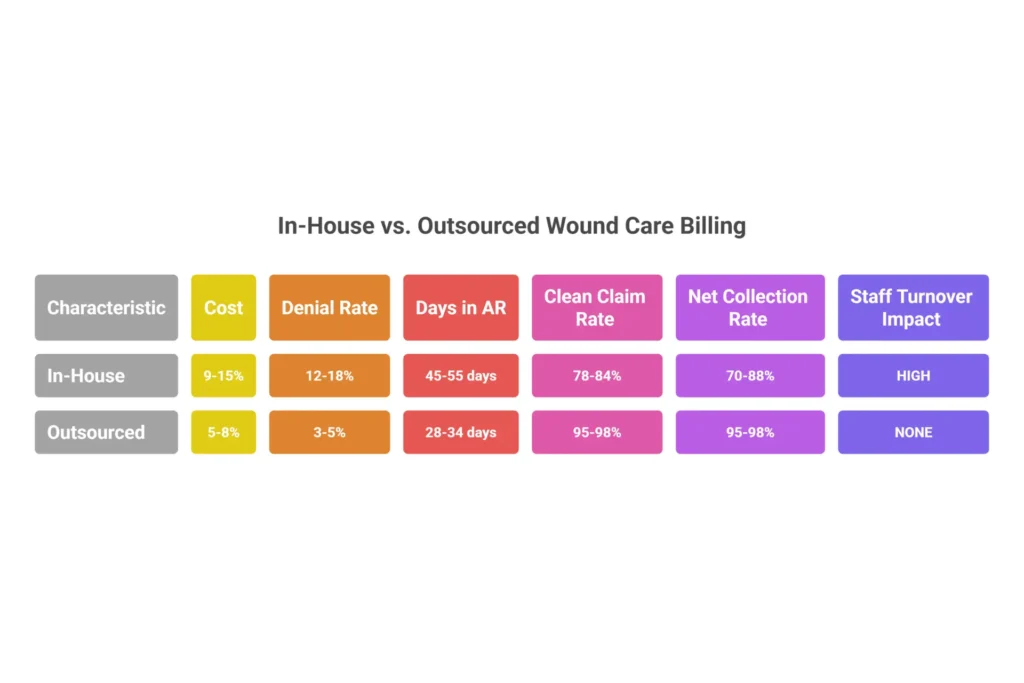
Performance Benchmarks: In-House vs. Specialized Outsourced
| Metric | In-House Average | Outsourced Specialist | Improvement |
| Clean Claim Rate | 78-84% | 95-98% | +15-20% |
| First-Pass Acceptance | 82-90% | 96-98% | +8-12% |
| Days in AR | 45-55 | 28-34 | 15-20 days faster |
| Denial Rate | 12-18% | 3-5% | 60-75% reduction |
| Net Collection Rate | 70-88% | 95-98.5% | +10-20 points |
| Staff Turnover Impact | High (20% rate) | None (vendor-managed) | Eliminated |
Expertise and Quality Differences
In-House Reality:
Your biller might have 2-5 years of experience. They might be certified (CPC). But unless they’ve spent those years exclusively in wound care, they’re missing the nuances. Wound care billing requires understanding:
- The difference between CPT 97597 and 11042 at a clinical level, not just a code level
- MAC-specific frequency limits (some regions flag more than 8 debridements in 12 weeks)
- The 2026 bundled payment rules for skin substitutes
- How to document “healing trajectory” to justify continued treatment
When your in-house biller quits—and with 20% annual turnover in medical billing, they will—that knowledge walks out the door. You spend months hiring and training a replacement, during which your AR balloons and your denials spike.
Outsourced Reality:
Specialized wound care billing firms have teams of 10-50 certified coders, many with CWCA (Certified Wound Care Assistant) or WCC (Wound Care Certified) credentials. They see claims from dozens or hundreds of practices. When a new payer edit appears, they know within days—not months. Their technology flags missing documentation before claims are submitted. Their appeal success rates are higher because they’ve fought the same battles before.
I’ve seen outsourced teams achieve 98-100% coding accuracy and near 100% audit pass rates because they’re proactive, not reactive.
When In-House Makes Sense
Let me be clear: I’m not anti-in-house. In three scenarios, I still recommend keeping billing internal:
- Massive Volume (> $10M Annual Revenue): At this scale, you can afford a dedicated Director of Revenue Cycle Management and a specialized audit team.
- Extremely Niche Procedures: If you’re performing experimental wound care treatments that require constant clinician-biller dialogue, in-house may be necessary.
- You’re Already Hitting 97%+ Clean Claims: If your in-house team is already performing at “best-in-class” levels, don’t fix what isn’t broken. But be honest with yourself about your actual metrics.
When Outsourcing Is the Better Choice
For everyone else—and that’s most practices—outsourcing wins. Specifically:
- High Staff Turnover: If you’ve lost a biller in the last 12 months, you’re already feeling the knowledge drain
- Scaling Practices: Adding providers? Opening a new location? Outsourcing scales without hiring
- High Denial Rates (>10%): You’re leaving six figures on the table
- AR Days >45: Your cash flow is strangled
- Under $5M Annual Revenue: You can’t afford the fully-loaded cost of a specialized in-house team
Want to calculate your own break-even point? Our team at Elite Med Financials provides customized ROI analysis for practices considering the switch.
How Much Does It Cost to Outsource Wound Care Billing?
This is the question I get most often, and it’s the one with the most variable answer. In 2026, you’ll encounter four primary pricing models. Let me break them down with the numbers you actually need.
Common Pricing Models Explained
1. Percentage of Collections (Most Common)
- Typical Range: 4-10% of net collections
- Wound Care Average: 5.4-8% (higher than general medicine due to complexity)
- Volume Discounts: Rates drop to 4-6% for collections above $2M annually
- Best For: Most practices, because incentives align—your vendor only gets paid when you do
2. Per-Claim / Encounter-Based Pricing
- Typical Range: $4-$12 per claim
- Wound Care Average: $8-$10 per claim (simple dressing changes at lower end, complex grafts at higher end)
- Best For: Practices with predictable, stable claim volume who want fixed costs
- Caveat: Often excludes denial management and appeals—those are extras
3. Flat Monthly Fee
- Typical Range: $2,000-$8,000+ per month
- Small Practice: $3,000-$5,000/month
- Medium Practice: $5,000-$8,000/month
- Large Practice: $8,000+/month
- Best For: Practices that want predictable budgeting and have stable revenue
4. Hybrid Models (Base + Percentage)
- Structure: $500-$1,500 per provider/month + 2-4% of collections
- Best For: Balancing predictable base revenue with performance incentives
- Growing in Popularity: Gives you the best of both worlds

What’s Included vs. What Costs Extra
Understanding what’s bundled in your base fee versus what triggers additional charges is crucial. Here’s what I typically see:
Usually Included in Base Fee:
- Charge capture and CPT/ICD-10 coding
- Electronic claim submission
- Basic denial management and appeals
- Payment posting
- Standard weekly/monthly reporting
- AR follow-up for claims under 90 days
Often Extra (Ask Specifically):
- Setup/Onboarding Fees: $1,500-$5,000 (red flag if over $5K; many firms waive with 24-month contract)
- Credentialing: $300-$500 per provider
- Technology Integration: $1,000-$3,000 (should be one-time)
- Custom Reporting: $100-$500/month
- Complex Appeals: $25-$50 each
- Patient Statements: $0.25-$0.50 each
- Old AR Cleanup: 15-20% contingency fee
ROI Calculator: Is Outsourcing Worth It?
💰 Wound Care Billing ROI Calculator
See how much you could save by outsourcing your billing
Your total yearly collections
Industry average: 12-18%
Salary + benefits + software + overhead
Typical range: 5-8%
Specialists typically achieve 3-5%
📊 Your ROI Analysis
Ready to capture this revenue? Our wound care billing specialists can help.
Get Your Free Assessment →*This calculator provides estimates based on industry averages. Actual results may vary based on practice specifics, payer mix, and documentation quality. Contact us for a personalized analysis.
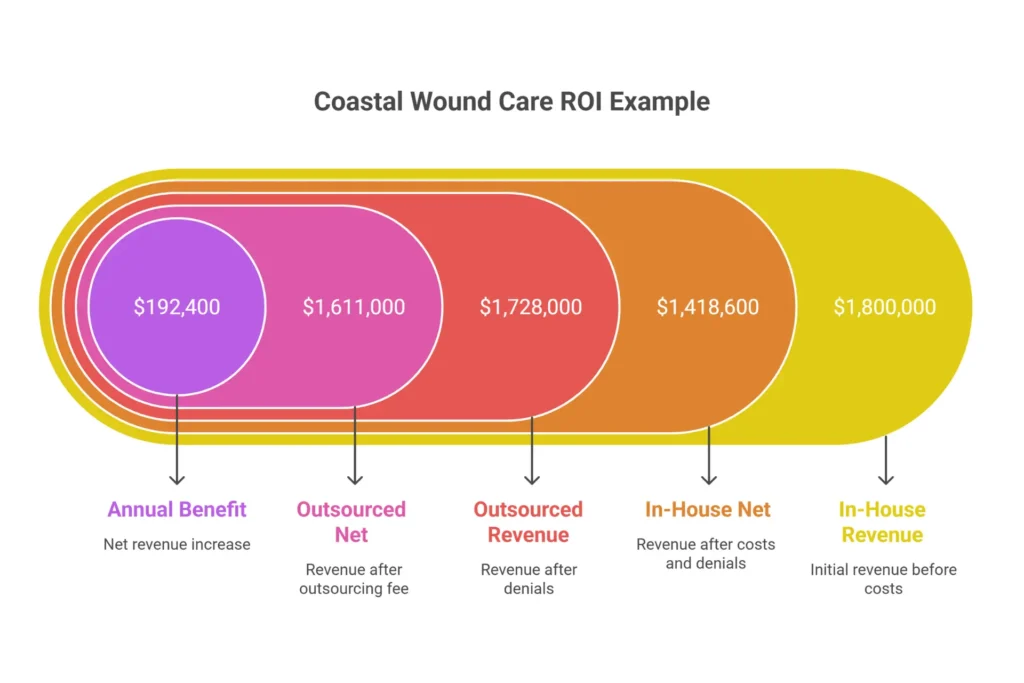
Here’s a real example from a practice I worked with last year. Let’s call them Coastal Wound Care—$1.8M annual collections, in-house billing, 14% denial rate, 52 days in AR.
Pre-Outsourcing Reality:
| Category | Annual Cost |
| Staffing (1.5 FTE) | $113,100 |
| Software/Clearinghouse | $7,800 |
| Training/Compliance | $2,500 |
| Space/Overhead | $6,000 |
| Total In-House Cost | $129,400 (7.2%) |
| Revenue Lost to Denials (14%) | $252,000 |
Post-Outsourcing (6.5% fee, 4% denial rate):
| Category | Annual Result |
| Outsourcing Fee | $117,000 |
| Revenue After Denials (96% collection) | $1,728,000 |
| Net After Fee | $1,611,000 |
The Math:
- In-House Net Revenue (after costs and denials): $1,800,000 – $129,400 – $252,000 = $1,418,600
- Outsourced Net Revenue: $1,611,000
Annual Benefit: $192,400
ROI: 164% ($192,400 gain / $117,000 fee)
That’s not cost savings—that’s profit transformation.
Hidden Costs to Watch For
I’ve seen too many practices sign contracts based on a quoted percentage, only to discover a minefield of add-on fees. Here’s what to ask about upfront:
The “Bottom-Feeder” Red Flag: If a firm quotes under 4% for wound care, run. They’re either “claim pushers” who don’t work denials, or they’ll hit you with hidden fees that make the effective rate much higher.
Understanding the real cost of medical billing services requires looking beyond the headline percentage.
What to Look for in a Wound Care Billing Company
After 15 years of evaluating billing partners, I’ve developed a mental checklist that separates pretenders from performers. Here’s what matters—and what doesn’t.
Essential Qualifications and Certifications
At the Individual Level:
- CPC (Certified Professional Coder) or CCS (Certified Coding Specialist) — non-negotiable baseline
- CWCA (Certified Wound Care Assistant) or WCC (Wound Care Certified) — the mark of true specialization
- 5+ years wound care experience for at least 50% of the team assigned to your account
At the Company Level:
- HIPAA compliance with a signed Business Associate Agreement (BAA)
- SOC 2 Type II audit (this verifies their security controls—don’t accept less)
- HBMA (Healthcare Billing and Management Association) or AAAMD affiliation
- 30-50%+ wound care clients — if wound care is less than a third of their book, you’re not a priority
Technology and EHR Integration Requirements
In 2026, manual billing processes are a liability. Your partner must offer:
- Bidirectional EHR Integration: They should sync with your system via API—whether you’re on Epic, Cerner, athenahealth, or wound-specific platforms like NetHealth, Healogics, Swift Skin & Wound, or WoundExpert
- AI-Powered Claim Scrubbing: Tools like Waystar or Optum360 that flag missing measurements, incorrect modifiers, and documentation gaps BEFORE submission
- Real-Time Dashboard: You should be able to log in 24/7 and see your AR aging, denial trends, and payer mix—not wait for a monthly PDF
- Predictive Analytics: Top firms now flag “failing wounds” (less than 20% area reduction over 4 weeks) to alert providers before payers deny continued treatment
- Audit-Ready Portal: Can they pull a “Clinical Justification Report” bundling wound photo, measurements, and CPT code for a specific date of service in one click?

Performance Metrics That Matter
When a vendor shows you their “average performance,” ask for your specialty’s numbers. Here’s what best-in-class looks like for wound care:
| Metric | Benchmark |
| First-Pass Clean Claim Rate | 95-98% |
| Days in AR | <30 days |
| Denial Rate | <5% |
| Net Collection Rate | 95%+ |
| Client Retention Rate | 95%+ |
| Appeal Success Rate | >80% on meritorious claims |
| Response Time | <24 hours |
Wound Care-Specific Experience Indicators
Here’s how I test a potential partner’s wound care knowledge. If they stumble on these, they’re not ready.
The Debridement Scenario:
“We performed a subcutaneous debridement of 14 cm² on the left foot and 12 cm² on the right foot, both at the same depth. How do you bill it?”
Correct Answer: “Sum the area (26 cm²) and bill 11042 (first 20 cm²) and 11045 (additional 6 cm²).”
Red Flag Answer: “Bill 11042 twice with a modifier.”
The 97597 vs. 11042 Distinction:
“What’s the difference?”
Correct Answer: “97597 is for non-excisional debridement—removing slough or fibrin. 11042 requires excisional removal of subcutaneous tissue. We need documentation of depth to choose correctly.”
The 2026 Skin Substitute Question:
“How are you adjusting your billing for skin substitutes given the $127.28/cm² flat rate?”
Good Answer: “We’re tracking the threshold against invoice cost to flag margin risk, and we’ve updated our claim scrubber to ensure wastage is documented and unit counts are precise.”
Bad Answer: “We still bill them as ASP+6% biologics.”
For more details on coding best practices, see our comprehensive guide to wound care billing codes.
Red Flags When Choosing a Billing Partner
I’ve seen practices make every mistake in the book. Here are the warning signs I wish they’d recognized earlier.
The Expertise Illusion
🚩 “We handle all specialties.”
Translation: We’re generalists who don’t know wound care.
🚩 Can’t explain LCD frequency limits.
If they don’t know that your MAC flags more than 8 debridements in 12 weeks, they’ll keep billing until you get an ADR—and then an audit.
🚩 Client portfolio <20% wound care.
You’re not their specialty. You’re their experiment.
🚩 Cannot explain debridement depth hierarchy.
CPT 11042, 11043, 11044, 11045, 11046, 11047—if they can’t recite these and explain the documentation requirements, they’re not ready for wound care.
The Price Trap
🚩 Rates under 4% for full-service billing.
Mathematically impossible if they’re actually working denials. They’re cherry-picking clean claims and letting your difficult AR rot.
🚩 “Free setup” but $50 per appeal.
The hidden fees will eat you alive. Ask for an all-inclusive rate.
🚩 Long-term contracts without performance outs.
If they won’t let you leave if they underperform, they’re not confident in their performance.
The Opaque Operation
🚩 Monthly PDF reports only.
In 2026, waiting 30 days for data means you’re managing by looking in the rearview mirror. Demand a real-time dashboard.
🚩 No AI claim scrubbing.
If they’re not using tools like Waystar, they’re missing errors you’ll pay for later.
🚩 Can’t demonstrate EHR integration.
“If you can send us a spreadsheet…” is not integration. It’s a recipe for data entry errors.
The Compliance Time Bomb
🚩 Vague about offshore operations.
If they use offshore coders without SOC 2 certification for those facilities, your data is at risk. I’ve seen “copy-paste” documentation errors from offshore teams trigger systemic audit failures.
🚩 Weak BAA or won’t share it.
A Business Associate Agreement isn’t a formality—it’s your legal protection. If they’re casual about it, walk.
🚩 Can’t explain 2026 skin substitute rules.
This is the biggest red flag of all. If they don’t understand the single biggest regulatory change in wound care billing this decade, they’ll cost you money—and potentially trigger a clawback.
🚩 No OIG/SAM exclusion screening.
They should be checking monthly that their staff aren’t excluded from federal programs. If they’re not, you could be liable.
Concerned about a vendor you’re evaluating? Our team has helped dozens of practices avoid these traps. Contact us for a second opinion.
15 Questions to Ask Before Outsourcing
Don’t go into vendor interviews unprepared. Use these questions—and listen carefully to the answers.
Experience & Expertise Questions
1. “What percentage of your clients are wound care practices, and can you share 3-5 case studies with specific metrics?”
- Good Answer: “40% of our 200 clients are wound care. Here are three case studies showing denial reductions from 15% to 4%, 12% to 3%, and 18% to 5%.”
- Red Flag: “We serve all specialties. Our clients are happy.”
2. “Walk us through coding a debridement to muscle depth using CPT 11044—how do you document for medical necessity?”
- Good Answer: “We require clinical notes to explicitly state ‘removal of muscle tissue.’ We verify depth documentation before coding.”
- Red Flag: “We code based on what’s on the superbill.”
3. “What certifications do your coders hold, and how many have 5+ years in wound care?”
- Good Answer: “90% are CPC-certified, and 60% have CWCA credentials. Our lead coder has 12 years in wound care.”
- Red Flag: “Everyone’s certified. We don’t track years by specialty.”
4. “Describe your ongoing training for 2026 CMS skin substitute changes.”
- Good Answer: “We subscribe to CMS updates and AAWC webinars. We’ve already updated our scrubber to flag any claim missing wastage documentation.”
- Red Flag: “We’re aware of the changes.”
Performance Metrics Questions
5. “What are your average first-pass rate, AR days, denial rate, and collection rate for wound care clients?”
- Good Answer: “First-pass 96%, AR 28 days, denial rate 4.2%, net collection 97%.”
- Red Flag: “It varies. We have great results.”
6. “Can you provide 6-12 months of anonymized performance data from similar practices?”
- Good Answer: “Absolutely. Here’s data from three wound care practices your size.”
- Red Flag: “We don’t share client data.”
7. “How do your denial rates break down (medical necessity vs. coding vs. auth) for wound claims?”
- Good Answer: “About 40% medical necessity, 35% coding, 25% authorization. Here’s our root-cause analysis process.”
- Red Flag: “We don’t track it that granularly.”
Operations & Support Questions
8. “Who is our dedicated account manager, their experience, and what’s the response time SLA?”
- Good Answer: “Jane Smith, 8 years wound care experience. Email response within 4 hours, phone within 24.”
- Red Flag: “You’ll have a team. We don’t do dedicated managers.”
9. “What is your staff turnover rate, and how do you mitigate billing disruptions?”
- Good Answer: “12% annually. We cross-train all staff and have a 2-week knowledge transfer protocol.”
- Red Flag: “We’re growing fast. Turnover happens.”
Technology & Integration Questions
10. “Which EHRs and clearinghouses do you integrate with?”
- Good Answer: “We integrate with Epic, Cerner, NetHealth, and Healogics via API. Clearinghouses include Availity and Change Healthcare.”
- Red Flag: “We can work with anything. You’ll send us reports.”
11. “What claim scrubbing tools ensure accuracy?”
- Good Answer: “We use Waystar with custom rules for wound care—flagging missing measurements, depth mismatches, and frequency limits.”
- Red Flag: “Our coders review everything manually.”
Contract & Pricing Questions
12. “Detail your pricing: percentage range, what’s included, and volume discounts.”
- Good Answer: “6.5% for your volume, includes everything except credentialing. Drops to 5.8% at $200K monthly collections.”
- Red Flag: “Our standard rate is 7%. We can discuss.”
13. “What are termination terms, notice period, and data return process?”
- Good Answer: “30-day notice. We’ll return all your data in CSV format within 2 weeks at no cost.”
- Red Flag: “Standard 90-day notice. Data export may incur fees.”
14. “Define ‘net collections’ and what performance guarantees you offer.”
- Good Answer: “Net collections is total payments after contractual adjustments but before bad debt. We guarantee 95% or we credit fees.”
- Red Flag: “We track gross collections. Guarantees are tricky.”
Transition Questions
15. “What is your onboarding timeline and support during the first 90 days?”
- Good Answer: “4-6 weeks. We’ll do a 2-week parallel run and provide daily calls for the first month.”
- Red Flag: “Usually 60-90 days. We’ll get you set up.”
The Complete Transition Process
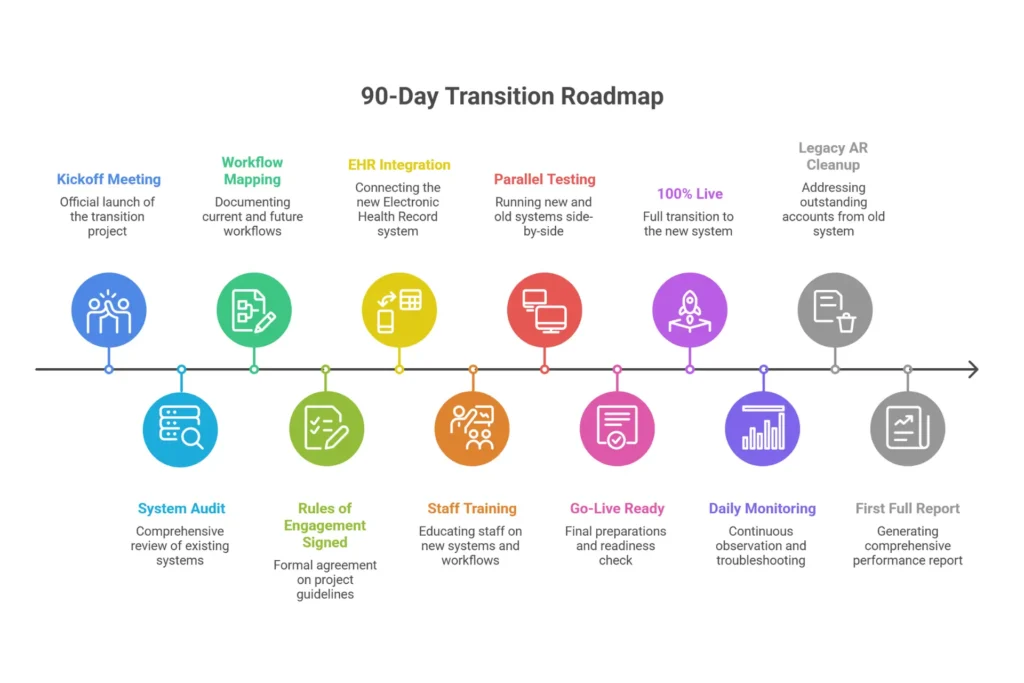
Switching billing vendors feels like performing open-heart surgery on your practice. Do it right, and revenue flows smoothly. Do it wrong, and you’ll be explaining cash flow gaps to your lenders.
I’ve overseen dozens of transitions. Here’s the roadmap that works.
Phase 1: Discovery & Planning (Weeks 1-4)
Week 1: Kickoff
- Appoint an internal Transition Lead—someone with authority and institutional knowledge
- Vendor assigns your Account Manager and Implementation Specialist
- Establish weekly check-in calls
Week 2: System Audit
- Grant vendor “Read-Only” access to your EHR for the last 90 days of claims
- They’ll audit your coding patterns, documentation gaps, and denial reasons
- This identifies problems BEFORE they start billing
Week 3: Workflow Mapping
- Document how a patient moves from check-in to debridement to billing
- Identify where documentation often fails (missing measurements? wrong depth?)
- Create “Rules of Engagement” document
Week 4: Milestone
- Signed Rules of Engagement document
- Complete list of payer contracts and fee schedules
- Current credentialing roster (NPIs, PTANs, Tax IDs)
Phase 2: Technical Integration (Weeks 5-8)
Week 5: EHR Integration
- Establish API or HL7 bridges for automated data transfer
- This is where FHIR (Fast Healthcare Interoperability Resources) APIs shine—real-time wound measurement syncing
- Test connection with sample data
Week 6: Staff Training
- Vendor trains your front desk on new insurance verification portals
- Clinicians learn what documentation the vendor needs (and when)
- Your billing staff learns their new oversight role
Week 7: Parallel Testing (Critical)
- Vendor submits a “shadow batch” of claims alongside your current process
- Compare results: match rates should exceed 95%
- Identify and resolve discrepancies before go-live
Week 8: Milestone
- Credentialing confirmed active in all payer systems
- Clearinghouse EDI/ERA links tested and verified
- Green light for go-live
Phase 3: Go-Live & Stabilization (Weeks 9-12)
Week 9: Go-Live
- Vendor takes over 100% of new date-of-service claims
- Your team shifts focus to legacy AR cleanup
- Daily 15-minute “scrums” to resolve missing information flags
Week 10: Monitoring
- Track claim lag time (target: <48 hours from DOS to submission)
- Monitor first-pass acceptance (target: >95%)
- Watch for credentialing rejections (indicates setup errors)
Week 11: Legacy AR Transition
- Begin handing off aging reports for claims billed before go-live
- Prioritize >90-day AR first
- Vendor assigns “Tiger Team” to high-balance accounts
Week 12: Milestone
- First full billing cycle report generated and reviewed
- AR trending toward 30-day target
- Denial rate below 5%
Tips for Smooth Transition
- Clean your data first. Resolve all “unbilled encounters” older than 60 days before transition
- Communicate with staff early. Hold a town hall: “This frees you for patient care”
- Keep 1-month operating reserve. Temporary 5-10% revenue dips happen
- Run parallel for 2 weeks minimum. If a vendor pushes to go live without parallel testing, they’re overconfident or underprepared
- Monitor daily for first 30 days. This isn’t micromanagement—it’s risk management
For a deeper dive into optimizing your revenue cycle, see our guide on how to improve revenue cycle management.
Outsourced Wound Care Billing Services: What’s Included

When you sign with a wound care billing partner, what exactly are you getting? The answer varies dramatically between “claim pushers” and true partners. Here’s my breakdown of standard vs. premium services.
Front-End Services (Patient Access Layer)
Standard (Included):
- Patient registration and demographics entry
- Real-time insurance eligibility verification
- Benefits verification
- Prior authorization tracking for standard procedures
Premium (May Be Extra):
- Dedicated “Pre-Cert Specialists” for high-cost skin substitutes
- Deep patient financial counseling
- Complex authorization appeals
Coding Services (Clinical-Financial Bridge)
Standard (Included):
- CPT coding for debridement (97597/97598, 11042-11047)
- CPT coding for Negative Pressure Wound Therapy (97605-97608)
- ICD-10 coding (L97.xx and related wound diagnoses)
- HCPCS supply coding (A6021, etc.)
- Modifier application (-25, -59, LT/RT)
- Documentation review for medical necessity
Premium (Value-Add):
- Clinical Documentation Improvement (CDI) audits
- Modifier compliance audits
- Coding scenario training for clinicians
Wound-Specific Nuances:
- Debridement hierarchy validation (selective vs. surgical)
- Skin substitute unit tracking ($127.28/cm² cap management)
- NPWT reimbursement differentiation (DME-owned vs. disposable)
- Healing trajectory analysis
Our medical coding services team specializes in these exact nuances.
Claim Management (Submission Engine)
Standard (Included):
- Electronic claim submission (99%+)
- AI-driven claim scrubbing (98%+ accuracy)
- Clearinghouse management (Availity, Change Healthcare, etc.)
- Real-time claim tracking
- Resubmissions
May Be Extra:
- Paper claim processing ($2-5 each)
Denial Management (Revenue Recovery)
Standard (Included):
- Automated denial identification
- Root-cause analysis (coding vs. auth vs. medical necessity)
- Appeal drafting and submission
- Payer communication and negotiation
- Monthly denial trend reporting
Premium (Strategic):
- High-volume complex appeals
- Predictive denial analytics
- AI-powered appeal engines
AR Management (Cash Flow Engine)
Standard (Included):
- Weekly payer follow-up calls
- Aging AR prioritization (90+ days first)
- Secondary claim billing
- Patient collection support
- Write-off recommendations (<1% goal)
May Be Extra:
- Old AR cleanup (15-20% contingency fee)
- Aggressive agency collections
Reporting & Analytics (Visibility Layer)
Standard (Included):
- Weekly AR aging reports
- KPI dashboards (first-pass rate, denial rate, collections)
- Denial trend analysis
- Monthly financial reviews
Premium (Strategic):
- Custom reports ($100-500/month)
- Margin analysis per cm² of skin substitute
- Benchmarking against industry peers
Infrastructure Services (Compliance Layer)
Standard (Included):
- Credentialing maintenance (CAQH updates, re-credentialing)
- Basic compliance monitoring
May Be Extra:
- New provider/payer enrollments ($300-500 each)
- Audit defense (TPE/RAC representation)
- Formulary optimization consulting
- Staff training on 2026 documentation requirements
For comprehensive credentialing support, explore our Medicare credentialing services.
HIPAA Compliance and Legal Considerations
Let me be direct: outsourcing your billing is legal, but you remain on the hook. The HITECH Act made Business Associates directly liable for HIPAA violations, but as the Covered Entity, you’re still responsible for oversight.

Is It Legal to Outsource Medical Billing?
Yes—with a BAA. HIPAA explicitly permits outsourcing as long as you have a signed Business Associate Agreement (BAA) in place before any PHI is disclosed.
The legal framework includes:
- HIPAA Privacy Rule: PHI safeguards
- HIPAA Security Rule: ePHI administrative, physical, technical safeguards
- HIPAA Breach Notification Rule: 60-day notification requirement (but negotiate this down)
- False Claims Act: “Reckless disregard” for billing accuracy creates joint liability
- State Laws: California CCPA, Texas Medical Privacy Act—some require 72-hour breach notification
Business Associate Agreement Requirements
A generic BAA isn’t enough in 2026. You need a Precision BAA addressing:
Essential Provisions:
- Permitted uses limited to billing—no data mining
- Subcontractor flow-down (written consent for offshore work)
- Breach notification: negotiate 24-48 hours, not 60 days
- Audit rights: you can review their SOC 2, penetration tests, breach logs
- Data return/destruction: machine-readable export (CSV/JSON) at no cost upon termination
- Data sovereignty: PHI remains subject to U.S. laws even if processed offshore
Sample Language to Demand:
“Upon termination, Business Associate shall provide Covered Entity with a machine-readable, structured data export of all claim history, payment records, and audit logs within 30 days at no cost.”
Data Security Standards
Technical Controls to Verify:
- Encryption: AES-256 at rest, TLS 1.3 in transit
- Access Controls: Multi-factor authentication (MFA) for every user
- Audit Logs: Can they tell you exactly who viewed a specific patient’s record and when?
- Zero-Trust Architecture: Assume breach, verify everything
Certifications to Request:
- SOC 2 Type II (within 12 months)
- HITRUST CSF (gold standard)
- ISO 27001 (international security standard)
Insurance Requirements:
- Cyber Liability: Minimum $5M per occurrence
- Errors & Omissions (E&O): Minimum $2M per occurrence
- Require being named as “Additional Insured”
Offshore Considerations
Offshoring is legal, but risky. If your vendor uses offshore coders:
- Require SOC 2 reports for offshore facilities
- Demand written data sovereignty policy
- Verify no-data-retention outside U.S.
- Watch for “copy-paste” documentation errors (common with offshore teams)
For authoritative guidance on HIPAA compliance, refer to the HHS HIPAA website.
Outsourcing for Small Practices
If you’re a solo provider or a 2-3 provider practice, you face a unique challenge: you’re too big for a part-time biller, but too small for a full RCM team. I call this the Efficiency Gap.

Why Small Practices Benefit Most
The Numbers Don’t Lie:
- Small practice revenue: $500K-$1.5M annually
- In-house cost: $80K-$150K/year (10-15% of collections)
- Outsourced cost: $3K-$6K/month (5-7% of collections)
- Net savings: 40-50%
Beyond Cost Savings:
- Turnover Protection: One biller quitting can cripple your cash flow for months. Outsourcing eliminates this risk
- Big-Practice Technology: Get AI claim scrubbing and real-time dashboards for a fraction of in-house cost
- Compliance Burden: LCD tracking, 2026 skin substitute rules—outsourcing transfers this headache
- Scalability: Add providers without hiring
Budget-Friendly Options for Small Wound Care Practices
Full-Service Outsourcing:
- 5-7% of collections
- End-to-end RCM
- Best long-term value
Flat Monthly Fee:
- $3,000-$5,000/month
- Predictable budgeting
- Good for stable revenue
Per-Claim Pricing:
- $6-$10 per claim
- Pay only for what you use
- Ideal for low-volume practices
Hybrid Models:
- Base $2,000/month + 3% of collections
- Balances predictability and incentive
Partial Outsourcing:
- Denial-only service: ~$1,000/month
- Back-end AR follow-up: ~$1,000/month
- Test the waters before full commitment
The “Pure Growth” Negotiation Tactic
Here’s a strategy I’ve used successfully for small practices:
Offer a higher percentage for the first 90 days (e.g., 8%) that automatically drops to 6% once monthly collections exceed $100K. This aligns incentives—they help you grow to earn more.
Success Story: Solo Podiatrist
Dr. Martinez, a solo podiatrist with a wound care focus, was spending 15 hours a week on billing. Denial rate: 15%. AR days: 58.
After switching to outsourced billing:
- Time on billing: 2 hours/week oversight
- Denial rate: 4%
- AR days: 28
- Net revenue increase: $120,000/year
The outsourcing fee? $84,000/year. Net gain: $36,000 plus 13 hours weekly of her time back.
Ready to explore options for your practice? Our medical billing services for small practices are specifically designed for providers like you.
Case Study: How Coastal Wound Care Added $192K in Annual Profit
Let me share a real example (name changed, numbers real).
Practice Profile
- Type: Multi-provider podiatry and wound care center
- Size: 5 providers, 1,200 claims/month
- Annual Revenue: $1,800,000
- EHR: eClinicalWorks
- Pre-Outsourcing State: 2 in-house billers, 52 days AR, 14% denial rate, constant staff turnover
The Challenge (Before)
When I first met with Coastal’s owner, she was exhausted. Her lead biller had quit three months ago—the third in two years. The replacement was still learning. Unbilled encounters were stacking up. Medicare had sent two ADRs in six months, and she’d spent $15,000 on a consultant to prepare for an audit that hadn’t happened yet.
Baseline Metrics:
| Metric | Before |
| Denial Rate | 14% |
| Days in AR | 52 |
| Net Collection Rate | 78% |
| AR >90 Days | 22% |
| Staff Turnover | 2 billers in 24 months |
| Clinician Time on Admin | 12 hours/week |
The Solution
We moved to a specialized wound care billing partner with:
- CPC and CWCA-certified coders
- AI-driven documentation scrubbing (flagged missing measurements before submission)
- Hard-coded 2026 flat-rate reimbursement limits ($127.28/cm²)
- “Tiger Team” assigned to clean up 400+ backlogged claims >90 days
- Weekly KPI reviews with dedicated account manager
Transition Timeline:
- Weeks 1-4: Discovery, data cleanup, workflow mapping
- Weeks 5-8: EHR integration, parallel testing
- Week 9: Go-live
- Weeks 10-12: Daily scrums, legacy AR cleanup begins
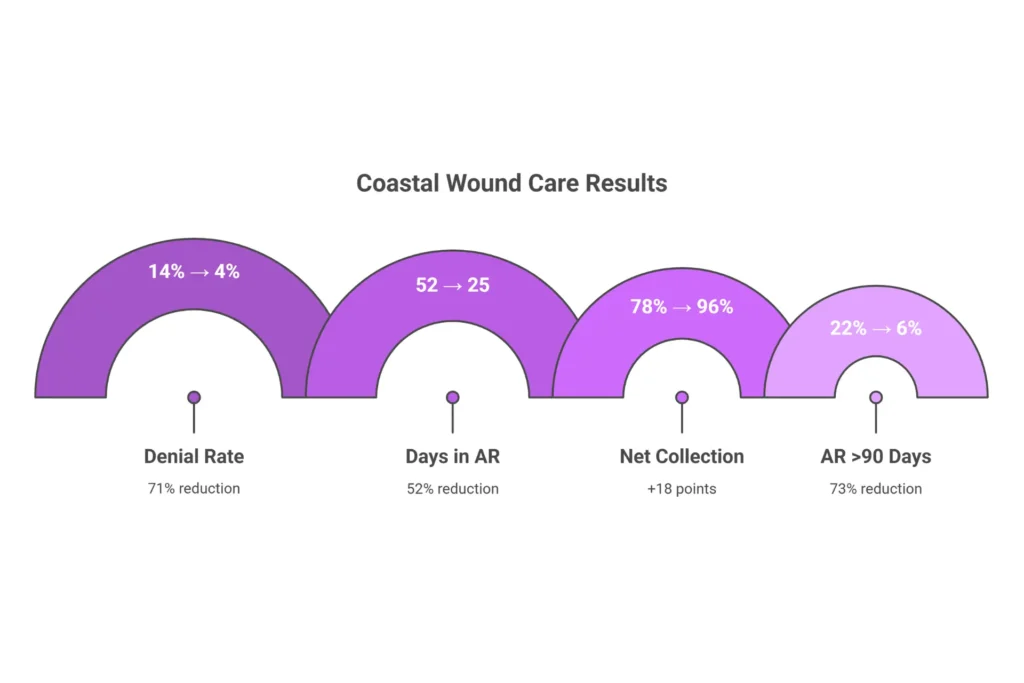
The Results (6 Months Post-Transition)
| Metric | Before | After | Improvement |
| Denial Rate | 14% | 4% | 71% reduction |
| Days in AR | 52 | 25 | 52% reduction |
| Net Collection Rate | 78% | 96% | +18 points |
| AR >90 Days | 22% | 6% | 73% reduction |
| Monthly Cash Flow | Baseline | +$24,000 | Significant |
| Clinician Admin Time | 12 hrs/week | 2 hrs/week | 10 hrs saved |
Financial Impact:
- In-House Cost (pre): $129,400 + $252,000 denial loss = $381,400 total cost of billing
- Outsourcing Fee: $117,000
- Net Gain: $192,400 annual profit increase
The Audit Win:
Six months after transition, Coastal received a CMS “Probe and Educate” audit. The vendor assembled documentation—wound photos, measurements, depth notes—in one click. Error rate: 0.5%. The practice passed with flying colors.
Owner’s Quote:
“I was terrified of losing control. Instead, I gained visibility. I can see my AR in real-time, I don’t dread Monday mornings, and I’ve reclaimed 10 hours a week to actually see patients. The ROI was undeniable.”
Key Success Factors
- Pre-transition AR audit: We didn’t carry garbage to the new vendor
- Dedicated wound coders: They caught depth documentation gaps our in-house team missed for years
- Weekly KPI checks: Problems were identified and fixed in days, not months
- Staff pivot: Our former lead biller became the internal auditor, reviewing notes for 2026 compliance before submission
For more on optimizing your revenue cycle management process, see our detailed breakdown.
Frequently Asked Questions
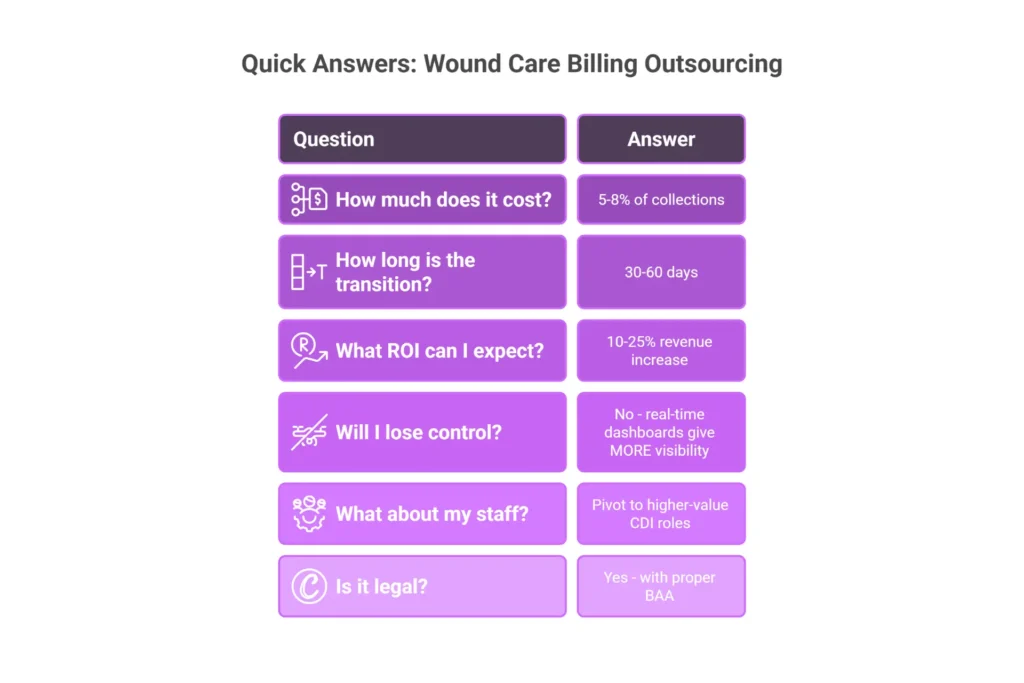
Is outsourcing medical billing a good idea?
Yes, for most wound care practices—especially small ones facing high denials from complex coding—outsourcing boosts revenue 10-25% while cutting costs 30-50% net. It reduces denial rates from 15% to under 5%, accelerates AR from 50 to 25 days, and ensures compliance with 2026 CMS skin substitute rules.
How much does it cost to outsource medical billing?
For wound care billing, expect to pay 5-8% of collections (average 6%), $8-12 per claim, or a flat fee of $3,000-$6,000/month for small practices. Volume discounts apply above $1M in annual collections. Hidden costs may include setup fees ($2,000-$5,000) and per-appeal charges ($25-$50). In 2026, don’t focus on the “cost”—focus on the Net Collection Rate. A 7% firm that collects 98% is cheaper than a 5% firm that collects 90%.
What is the golden rule of medical billing?
“If it isn’t documented, it didn’t happen.” Every CPT code must be supported by clinical evidence—wound measurements (L x W x D), tissue types, and debridement depth. In 2026, this rule has expanded to include precise documentation of skin substitute usage (exact cm² and wastage) under the new bundled payment model. If an auditor reviews a claim for subcutaneous debridement (11042) but the note only describes “cleaning slough” (97597), the claim will be denied.
How long does the transition to outsourced billing take?
A standard transition takes 30 to 60 days for wound care practices. Phases: Weeks 1-2 (planning/audit), 3-4 (setup/integration), 5-6 (go-live/parallel testing), 7-8 (stabilization). Expect an initial 5-10% revenue lag as systems synchronize. Clean up old AR beforehand to avoid delays. Start at least 60 days before a major staff departure or contract renewal to avoid cash flow gaps.
Will I lose control of my billing?
No—with proper contracts, you retain full oversight via real-time dashboards, weekly reports, and quarterly audits. Top firms provide more visibility than in-house teams through AI analytics and 24/7 portals showing exactly where every dollar is in the revenue cycle. Proximity is not control; transparency is control. Demand SLAs with <24-hour response times and schedule monthly performance calls.
What happens to my current billing staff?
Most practices transition internal staff into “Clinical Documentation Integrity” (CDI) or “Patient Experience” roles. Your current biller knows your patients and clinical quirks—they can “scrub” notes for 2026 compliance before the vendor sees them, acting as an internal auditor to prevent denials. This approach reduces billing-related turnover and frees 10-15 provider hours per week previously lost to administrative tasks.
Can I outsource only part of my billing?
Yes—hybrid models are popular in 2026. Common options include “Old AR Clean-up” (vendor works claims >90 days) or “Back-End Only” (you handle coding/submission; they handle denials/appeals). Costs range from $1,000-$2,000/month for partial services. This is an excellent low-risk way to test vendor relationships.
What if I’m unhappy with the service?
Contracts typically allow 30-90 day termination with data return. Build performance KPIs directly into your contract—first-pass rate >95%, Days in AR <35 days, denial rate <5%. If these are breached for two consecutive months, you should have termination-for-cause rights without penalty. Ensure your contract includes a “data portability” clause requiring the vendor to return all your data in machine-readable format at no cost upon termination.
How do I choose a wound care billing company?
Look for firms with 30%+ wound care clients, certified wound coders (CPC/WCC), and proven metrics: 95%+ clean claims, <5% denials, and real-time dashboards. Avoid generic companies dodging specifics or charging under 4%. Get 5 references from similar practices and check SOC 2 Type II compliance. Test their knowledge with scenario questions about debridement coding and 2026 skin substitute rules.
Is it legal to outsource medical billing?
Yes, outsourcing medical billing is fully legal under U.S. federal law when proper safeguards are in place. A signed Business Associate Agreement (BAA) is mandatory before any PHI disclosure. The provider remains the “covered entity” with ultimate liability, but risks are mitigated through robust contracts, SOC 2 certified vendors, and cyber liability insurance. Offshore billing is also legal if BAA-compliant, but requires extra scrutiny.
What are the cons of outsourcing medical billing?
The main cons include less direct, day-to-day control over billing staff, potential communication delays if not managed well, data trust concerns requiring robust BAAs, and a transition period that may temporarily disrupt cash flow (5-10% for 30-60 days). These are manageable through proper contracts, dedicated account managers, real-time dashboards, and thorough vendor selection.
What is the average denial rate for wound care billing?
In-house teams average 12-18% denial rates. Specialized wound care billing services achieve under 5%—often 3-4%. The most common denial reasons are: medical necessity documentation gaps (40%), coding errors (35%), and authorization issues (25%). The 2026 skin substitute bundling rules have increased documentation-related denials significantly.
How do I outsource my wound care billing?
Outsourcing your wound care billing is a straightforward four-step process. First, audit your current AR and denial rates to see where you’re losing money. Second, get quotes from three to five specialized wound care firms—look for certified wound coders and real-time dashboards. Third, sign a Business Associate Agreement and integrate your EHR with their system—modern APIs make this fast. Fourth, transition through 30-60 days of testing and go-live. Most practices complete this with no revenue disruption and see a 10-25% revenue boost within 90 days.
What does outsourced wound care billing cost?
Most wound care billing companies work on a performance basis—they only get paid when you do. Typically, they’ll take 5-8% of what they collect. For a specialty like wound care, this is a huge win because the extra revenue they find by catching coding errors usually covers their entire fee. Small practices might pay a flat fee around $3,000 to $6,000 a month. You might see a one-time setup fee of $2,000 to $5,000. The bottom line? Outsourcing typically saves practices 40% compared to keeping billing in-house.
How do I choose a wound care billing company?
When choosing a partner, specialty expertise is everything. You don’t want a generalist—you want someone who knows the 2026 rules for skin substitutes and debridement like the back of their hand. Ask if they have certified wound care coders—look for CPC or CWCA certifications. Make sure they offer a real-time dashboard so you can see your money at any time, not just a monthly PDF. A huge red flag is any company that tries to lock you into a long-term contract without a trial period. Always ask for five references from practices similar to yours and check for SOC 2 certification.
What’s the best medical billing company for wound care?
The best company depends on your practice size and needs. Look for firms where at least 30% of clients are wound care practices. Top-rated wound care billing services specialize in high-complexity cases and act as audit defense partners, not just claim processors. When evaluating, ask them how they handle the 2026 bundled payments for skin substitutes—if they can’t explain the $127 per square centimeter rule clearly, they aren’t the right fit. Small practices benefit from companies offering no-minimum-volume deals and flat monthly fees.
How long does it take to outsource billing?
Plan for about two months to get everything running perfectly. The first couple of weeks are technical—getting your EHR talking to their billing system. Then you’ll spend a few weeks in a “shadow period” where they test claims alongside your team to make sure coding is accurate. By the second month, you’re usually fully live. It’s designed to make sure your cash flow doesn’t skip a beat. Most practices start seeing real results—faster payments, fewer denials—within 90 days of going live.
Can I outsource just my denial management?
Yes, absolutely. In fact, hybrid models are becoming really popular for practices that want to test the waters. You can outsource just your denial management—let’s say you’re running a 15% denial rate—for about $1,000 to $2,000 a month. The vendor will work on appealing those denied claims and clearing up your old accounts receivable while your team keeps handling the front-end. It’s a great low-risk way to bring in expert help for your biggest pain points without handing over everything at once.
What happens to my billing staff if I outsource?
Most smart practices don’t fire their staff—they pivot them into more valuable roles. Your current biller knows your patients and your clinical quirks better than anyone. Many become Clinical Documentation Integrity specialists, where they review the doctor’s notes before they go to the outsourced vendor, catching documentation gaps that would cause denials. It’s a win-win: your staff gets more strategic, interesting work, and your practice gets an extra layer of audit protection. Plus, it frees up about 10 to 15 hours a week for your clinicians to focus on patients instead of paperwork.
Is outsourcing medical billing legal?
Yes, it’s completely legal, but you have to follow strict rules to protect patient data. The most important document is called a Business Associate Agreement, or BAA, which you must sign before any patient information is shared. This contract spells out exactly how they can use the data and what they have to do if there’s a breach. You also want to make sure they have cyber insurance—at least $5 million—and a security certification like SOC 2 Type II. Offshore billing is legal too, but you need extra safeguards to ensure data stays protected across borders.
Conclusion: Your Revenue Cycle Transformation Starts Now
After 15 years in this industry, I’ve seen every billing disaster imaginable. I’ve watched practices lose hundreds of thousands to clawbacks because they didn’t understand the 2026 skin substitute rules. I’ve seen owners burn out trying to manage billing themselves. And I’ve seen the relief on their faces when they finally partner with experts who actually know wound care.
Here’s my honest advice: if your AR is over 40 days, if your denial rate is over 10%, if you’ve lost a biller in the last year, or if you’re lying awake at night worrying about audits—you need help. Not next year. Now.
The 2026 CMS changes aren’t going away. The scrutiny on debridement coding isn’t easing. The margin for error isn’t coming back.
Your Decision Framework
- Audit your current numbers (AR days, denial rate, clean claim rate)
- Calculate your true cost-to-collect (salary + benefits + software + overhead + lost revenue)
- Interview 3-5 specialized vendors using the questions in this guide
- Run the numbers (use the ROI framework we’ve outlined)
- Make the call
Take Action Today
Your revenue cycle is the engine of your practice. Don’t let it run on fumes.
Ready to transform your wound care billing? Here’s how we can help:
- Wound Care Billing Services — Specialized coding, denial management, and compliance monitoring
- Comprehensive RCM Services — End-to-end revenue cycle management
- Medicare Credentialing — Get enrolled and stay enrolled
- Medical Coding Services — Expert coders who understand wound care
Additional Resources:
- Wound Care Billing Codes Guide
- Medicare Wound Care Billing Guide
- Revenue Cycle Management Overview
- Healthcare Revenue Cycle Fundamentals
For authoritative reference:
This guide is updated for 2026 CMS regulations. Specific reimbursement rates and policies may vary by MAC and payer. Always verify current requirements with your Medicare Administrative Contractor.

