
Last Updated: February 2026 | Elite Med Financials Clinical Billing Team
Here’s something that surprises most wound care providers when they first hear it: the majority of Medicare wound care denials aren’t caused by doing the wrong procedure — they’re caused by the wrong paperwork. Specifically, the wrong code, the wrong modifier, or documentation that doesn’t match the bill that was sent.
I’ve reviewed claims from wound care practices across multiple MAC jurisdictions, seen the aftermath of TPE audits, and helped recover revenue that was sitting dormant in AR because no one knew how to write a Level 1 Redetermination letter. The patterns are predictable. The fixes are learnable. But they require knowing the difference between what a coder does and what a biller does — and why wound care is genuinely one of the most complex specialties either of them will ever work in.
This guide covers both disciplines from the ground up.
Wound Care Billing vs. Wound Care Coding: Two Different Jobs, One Revenue Goal
Practices that treat billing and coding as interchangeable terms are the ones calling us after an audit. Let’s be precise.
Medical coding is the interpretive phase. Your certified coder reads the provider’s clinical note — wound depth, tissue type removed, measurements, instruments — and translates all of that into standardized CPT and ICD-10 codes. Their question is: What was done, and how do we capture its clinical complexity in alphanumeric language?
Medical billing is the transactional phase. Once the codes are assigned, the biller takes them, verifies payer rules, applies the correct modifiers, scrubs for NCCI edits, and submits the claim via CMS-1500. Their question is: Will the payer accept this, and if not, what stops it?
When these two functions don’t communicate — when a coder selects CPT 97597 and CPT 29580 without flagging the NCCI bundle to the biller, or when a biller submits an E11.621 claim without knowing that a second ICD-10 code is required — you get denials that feel mysterious but actually have a documented explanation in NCCI Chapter 4 or LCD Group 1.
What makes wound care harder than most specialties:
Depth-based CPT selection. CPT codes 11042–11047 are not selected by procedure name or wound type. They’re selected by the deepest layer of tissue that was actually removed — subcutaneous fat (11042), muscle or fascia (11043), or bone (11044). If the clinical note says “debridement performed to healthy tissue” without specifying depth, the coder is guessing. Guessing in wound care leads to either upcoding (OIG audit risk, up to $10,000 per false claim) or downcoding (lost revenue, no appeal possible).
Dual ICD-10 for diabetic ulcers. Medicare requires an etiology-manifestation pair. E11.621 (Type 2 diabetes with foot ulcer) alone fails medical necessity. You need the L97.5xx series specifying site and depth — L97.516 for right foot with bone involvement, L97.522 for midfoot with fat exposed, and so on. General coders routinely miss the second code. The denial is CO-97, and about half of them are never appealed.
NCCI bundling. The National Correct Coding Initiative flags services considered integral to each other and bundles them. Compression bandaging with debridement on the same limb, selective debridement with surgical debridement on the same wound, ultrasound therapy with any debridement on the same site — these are all automatic prepayment edits with modifier indicators that tell you exactly whether a modifier bypass is allowed. Many billers don’t know which indicator is 0 (no bypass) versus 1 (XS or 59 allowed).
MAC-specific LCD compliance. Your Local Coverage Determination isn’t the same as your colleague’s in a different state. Noridian’s A58565 Revision 11 (effective January 1, 2026), CGS’s A55909, and Palmetto’s A55818 each maintain their own “Group 1” ICD-10 code lists. Your ICD-10 code might be technically correct and still not appear on your MAC’s approved list — automatic denial.
The financial split between general RCM firms and specialized wound care billing and coding services consistently runs 15–30% denial rate versus under 5%. On a practice billing $600,000 annually, that’s the difference between $54,000 in permanent revenue leakage and $1,400. The math speaks for itself.
If that gap sounds familiar, our wound care billing services are built specifically to close it.
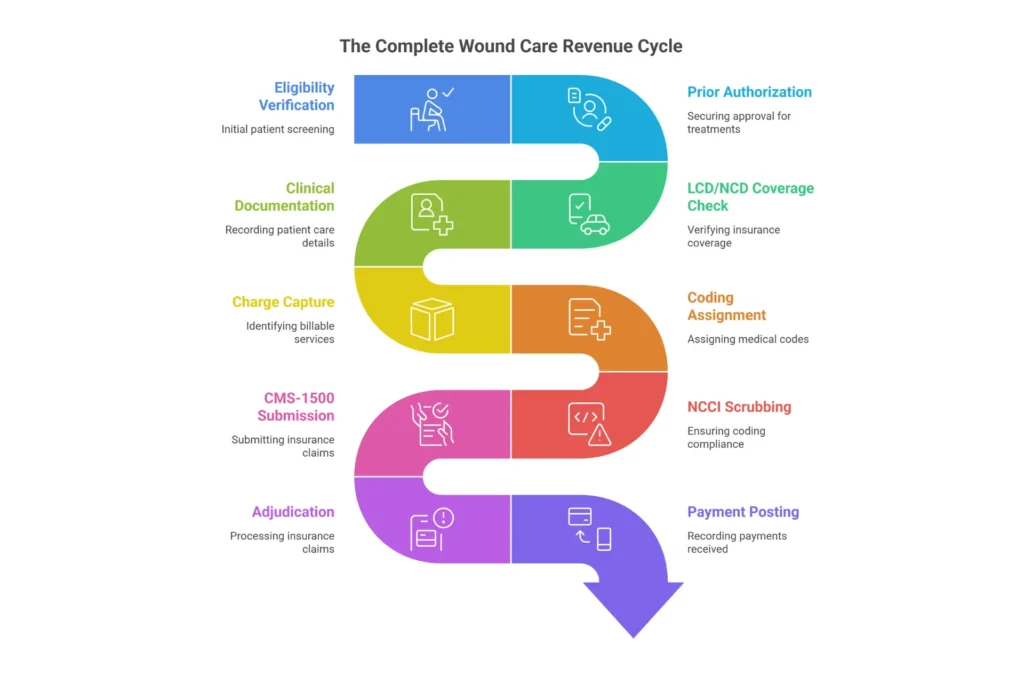
The Complete Wound Care Revenue Cycle
Wound care revenue doesn’t just move through a billing system — it moves through a series of checkpoints where clinical precision and administrative compliance either align or break down. Here’s what that lifecycle actually looks like under 2026 CMS requirements.
Front-End: Before the Patient Arrives
Eligibility verification isn’t just checking active insurance. For wound care, it means confirming Medicare Part B coverage, checking that the planned procedure aligns with the patient’s active LCD, and verifying therapy caps if PT or OT is involved. Miss this and you may provide a service with zero coverage.
Prior authorization has become non-negotiable for high-value wound care therapies. Most commercial payers and Medicare Advantage plans require documented proof of 30 days of failed conservative care before authorizing cellular tissue products (CTPs). NPWT rental pumps require authorization through the DME MAC. HBOT typically needs Wagner Grade documentation and vascular assessment. Missed prior auth means $1,500–$4,000 per skin substitute application is gone — retroactive approval is rare.
Mid-Cycle: The Encounter and Translation
Charge capture is where most practices lose invisible money. I’ve audited practices that consistently forget the add-on codes — +11045, +11046, +11047 — for every additional 20 sq cm of debridement beyond the first. They miss MIST therapy (97610) on days it qualifies as separately billable. They don’t capture modifier -25 when a significant, separately identifiable evaluation occurs alongside the procedure. Each missed service is $80–$200 per visit, and it compounds weekly.
Coding assignment must follow the deepest-tissue-removed rule for 11042–11047, the surface-area rule for 97597–97598, and full ICD-10 specificity for every diagnosis linked on the claim. CMS-1500 Box 21 lists etiology first (E11.621) followed by manifestation (L97.511). Box 24E links each CPT code to the specific supporting diagnosis. Get this backward, or use the wrong number of linked diagnoses, and adjudication fails.
Claim scrubbing runs NCCI edits, MUE limits, and LCD validation before the claim ever leaves your system. In 2026, this step can’t be manual.
Back-End: Collections and Follow-Up
Wound care AR averages 45–60 days — measurably longer than general medicine’s 30–40 days. That’s because wound care claims have more complexity, more denial reasons, and more documentation requirements on appeal. You need tiered follow-up: 30-day reminders, 60-day payer calls, 90-day escalation for high-dollar claims. AR left to age past 90 days in wound care has roughly a 40% recovery rate. Under 30 days, that’s 85%+.
The KPIs that define a healthy wound care revenue cycle:
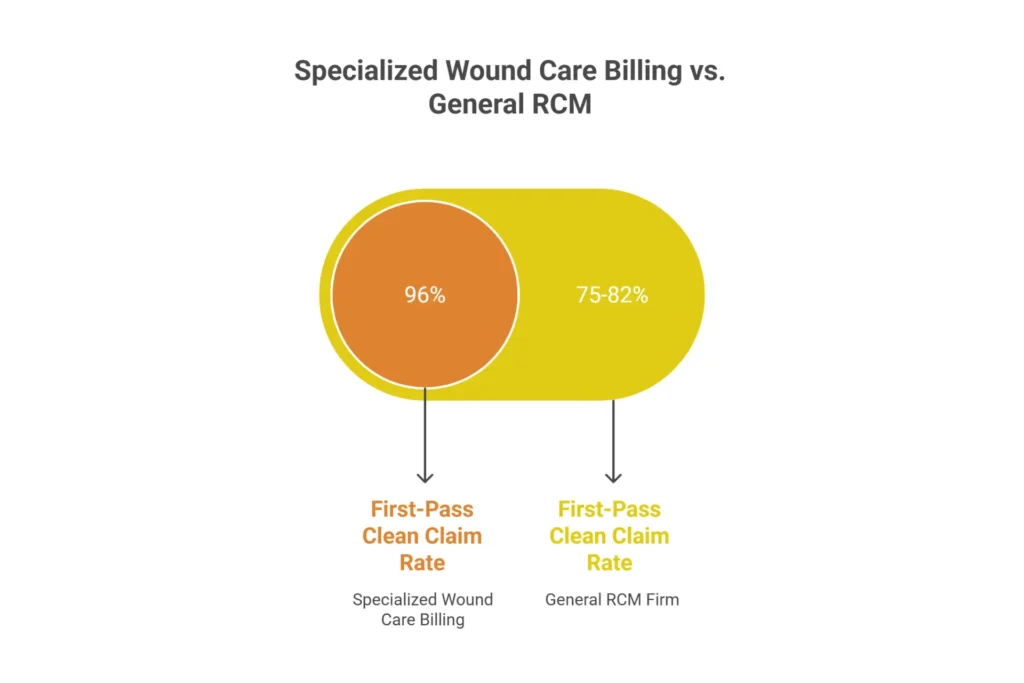
- First-pass clean claim rate: Target >95% (industry wound care average is 75–82%)
- Denial rate: Target <5% (most general RCM firms run 15–30%)
- Days in AR: Target <35 (average is 45–60)
- Net collection rate: Target >98%
Our revenue cycle management services track these KPIs weekly and report them to your inbox — not just when something goes wrong.
What Certified Wound Care Coders Actually Do
The CWCC (Certified Wound Care Coder) credential from AAPC isn’t an elective specialty. It’s what separates a coder who can assign 97597 from one who knows to query the provider about undermining depth and cross-check the MAC LCD before submitting.
Here are six specialized tasks a certified wound care coder performs that general coders consistently miss:
1. Capture add-on units accurately. A 45 sq cm debridement isn’t just one code. It’s 11042 for the first 20 sq cm, plus add-on +11045 for the next 20, plus a note that the remaining 5 sq cm was included in the second unit. Generalists bill one code and call it done.
2. Query the provider before submission. When the note says “debrided to viable tissue” without depth specificity, a certified coder doesn’t guess 11042. They query the provider — “Was subcutaneous tissue exposed? Did you reach muscle?” — and document that query in the chart. The answer determines the code. The query protects the practice during audit.
3. Sequence dual ICD-10 for diabetic ulcers. E11.621 + L97.529 (or the site-specific code) in that order, linked correctly in Box 24E. Not E11.621 alone. Not the L97 code alone.
4. Cross-check MAC LCD Group 1 lists by jurisdiction. Before submitting a claim for a patient in Noridian’s JE territory, a certified coder verifies the ICD-10 against the 1,173 Group 1 codes in A58565 Revision 11. A code not on that list = automatic denial regardless of clinical appropriateness.
5. Apply X-series modifiers over generic -59. CMS now explicitly prioritizes XS (separate structure), XE (separate encounter), XP (separate practitioner), and XU (unusual non-overlapping service) over the catch-all -59. A certified coder knows which scenario maps to which modifier.
6. Monitor the annual update cycle. CPT descriptors update January 1. ICD-10-CM updates October 1. NCCI edits update quarterly. MAC LCDs revise on unpredictable schedules. A certified wound care coder subscribes to MAC listservs, attends AAPC wound care CEU sessions, and reads AHIMA Coding Clinics. A general coder finds out about changes when claims start denying.
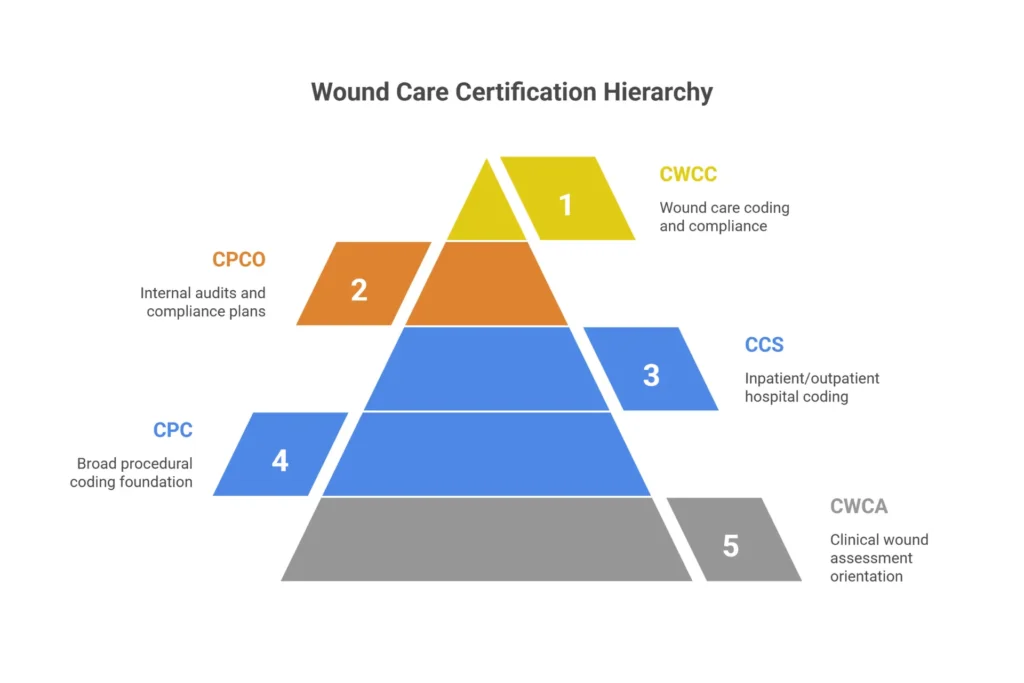
Certifications that matter in wound care:
| Credential | Issuer | What It Validates | When You Need It |
|---|---|---|---|
| CWCC | AAPC | Wound CPT/ICD-10, debridement, skin substitutes, NCCI, LCD compliance | Outpatient wound care — your minimum standard |
| CPC | AAPC | Broad procedural coding foundation | Good baseline, insufficient alone for wound care |
| CCS | AHIMA | Inpatient/outpatient hospital coding and DRGs | Hospital-based wound centers, inpatient dehiscence coding |
| CWCA | ABWM | Entry-level wound assessment | Clinical orientation — not coding-specific |
| CPCO | AAPC | Compliance oversight, internal audits, OIG plan management | Compliance officer role — audit defense |
Ask to verify credentials through the AAPC credential verification tool or AHIMA’s portal. Don’t take marketing language at face value.
Our medical coding services are staffed exclusively by AAPC-certified wound care coders. Not “experienced billers who do coding.” Certified specialists.
The 8 Most Common Wound Care Coding Errors
These aren’t hypothetical. They’re pulled from OIG 2025 Work Plan data, CMS CERT reports, and patterns I’ve seen in real practice claim audits. Each one includes the specific code, the fix, and the financial exposure.
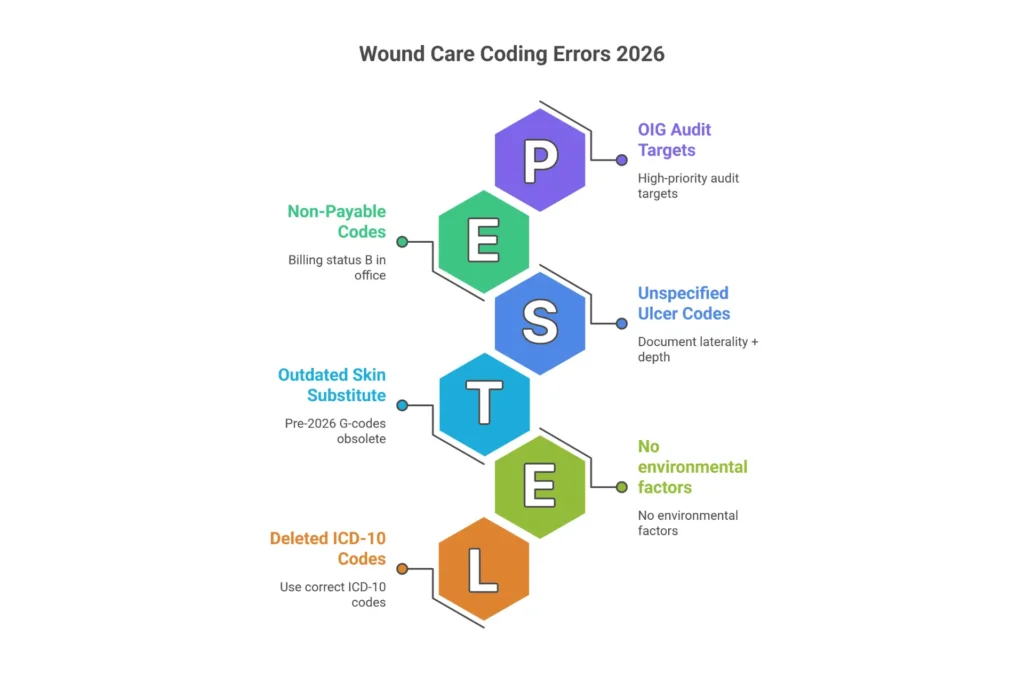
Error 1 — Upcoding debridement depth Billing 11044 (bone) when the note says “wound with visible bone” but doesn’t document that bone was actually removed. The deepest tissue removed determines the code — not the deepest tissue seen. Fix: Documentation must state “bone tangibly debrided to viable margins” or equivalent. Not “bone visible.” Risk: High OIG exposure. False Claims Act penalties up to $10,000+ per claim. Denial code: CO-97 (medical necessity) on post-payment review.
Error 2 — Using deleted ICD-10 code T81.32XA after October 2024 T81.32XA was deleted effective October 1, 2024. Approximately 25% of practices still have it active in their charge systems per 2026 MAC audit data. Fix: Update to T81.320A (disruption of deep internal surgical wound), T81.321A (superficial), or T81.329A (other). Use A for initial treatment, D for subsequent, S for sequela. Denial code: CO-16 (invalid/obsolete code).
Error 3 — Missing dual ICD-10 for diabetic foot ulcers E11.621 alone without a corresponding L97.5xx code triggers CO-97 on nearly every MAC. The etiology-manifestation pair is required for medical necessity validation. Fix: Always pair E11.621 with the specific ulcer code. L97.516 (right foot, bone without necrosis), L97.522 (left midfoot, fat exposed), etc. The specificity of the L97 code must match what the provider documented. Appeal success rate: ~50% on resubmission with added L97 code.
Error 4 — Billing 97597 + 11042 on the same wound, same day NCCI PTP edit bundles selective debridement (97597) with surgical debridement (11042) on the same wound. Modifier indicator 0 — no bypass allowed. These are procedure variants for the same service. Fix: Select the code that best captures the work. If different wounds were treated, use modifier XS with documentation of separate anatomic sites. Loss: ~$400 per claim, with less than 20% recovery rate on appeal.
Error 5 — Billing 97602 separately in office settings CPT 97602 (non-selective debridement — wet-to-moist dressings) has Status B in the Medicare Physician Fee Schedule Database. In physician offices, it’s bundled into the primary service. Not separately payable. Fix: Don’t bill it in POS 11. Physical and occupational therapists in SNF/HHA settings can bill it under a therapy plan of care with GP or GO modifier. Loss: ~$150 per claim, non-appealable.
Error 6 — Unspecified ulcer codes that fail LCD Group 1 match L97.909 (unspecified chronic ulcer of unspecified lower leg) doesn’t appear on most MAC Group 1 approved lists. L97.516 (right foot, specific depth) does. Fix: Provider documentation must specify laterality, location within the foot, and depth indicators (skin only, fat, muscle, bone). Query if missing. Reimbursement drop: Average 30% reduction in reimbursement for non-covered ICD-10 codes.
Error 7 — Outdated skin substitute coding after January 1, 2026 The November 2025 CMS Physician Fee Schedule Final Rule reclassified most CTPs to incident-to supplies at a flat rate of approximately $127.14 per sq cm. Old Q41xx G-code structures and size-based add-ons no longer apply. Fix: Use the current Q41xx series for the product and CPT 15271–15278 for application. No separate add-ons for size. Verify with your specific MAC’s updated LCD. Loss: $500–$1,000 per application if you bill with pre-2026 logic.
Error 8 — Missing 7th character (encounter designator) on injury and complication codes S-codes (traumatic wounds) and T-codes (complications like post-surgical dehiscence) require a 7th character: A (initial/active treatment), D (subsequent/routine follow-up), S (sequela). Defaulting to X (placeholder) or omitting it entirely triggers CO-4. Fix: Use A for every visit where active wound treatment is ongoing. Switch to D when treatment is routine maintenance. S only for late effects after healing.
The OIG 2025 Work Plan explicitly targeted errors 1, 3, 4, and 7 as high-priority review areas. If you’re seeing patterns of these denials, that’s not bad luck — that’s a systematic documentation or coding gap that needs to be addressed before a Targeted Probe and Educate letter arrives.
Bundling Rules Every Wound Care Biller Must Know
NCCI edits are automated prepayment filters that run before a claim adjudicates. Understanding them isn’t optional — it’s baseline competency for anyone billing wound care.
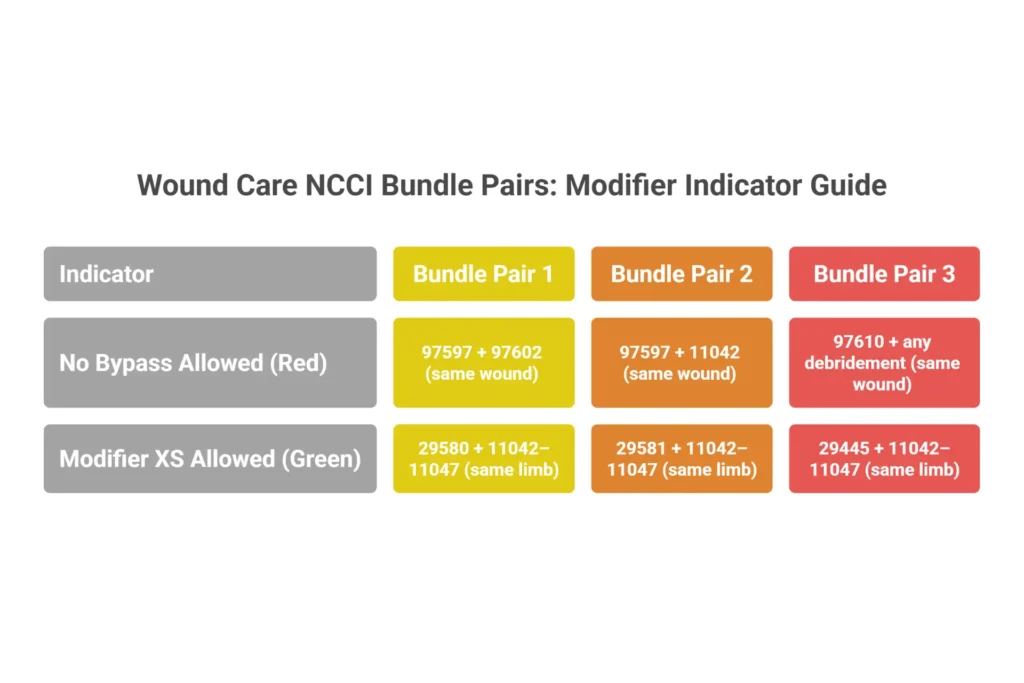
The core bundle pairs, with modifier indicators:
| Bundle Pair | Modifier Indicator | What It Means |
|---|---|---|
| 97597 + 97602 (same wound) | 0 — no bypass | Always bundled; no modifier works |
| 97597 + 11042 (same wound) | 0 — no bypass | Procedure variants; choose one |
| 97610 + any debridement (same wound) | 0 — no bypass | MIST bundles with all debridement on same wound |
| 29580 + 11042–11047 (same limb) | 1 — XS allowed | Different limb requires modifier XS + documentation |
| 29581 + 11042–11047 (same limb) | 1 — XS allowed | Same rule; document separate anatomic sites |
| 29445 + 11042–11047 (same limb) | 1 — XS allowed | Total contact cast; XS if contralateral limb |
Status B for 97602. This code isn’t just bundled with specific codes — it’s bundled with the visit itself in physician office settings. Status B in the MPFSDB means non-payable in that setting, period. No modifier overrides it for physicians in POS 11.
The 2022 Chapter 4 Section G update (NCCI Version 28.0) was the formal codification of the casting/strapping + debridement bundle rule. Before 2022, practices sometimes got away with billing both. After January 2022, the edit went live and retroactive audits followed. The OIG had documented 15–20% improper payments specifically from this practice.
MUE limits for 2026:
- 97597: 4 units per day (override requires separate wound documentation and photos)
- 11042: 6 units per day (document separate sites and depth of each)
- 11044: 2 units per day (high scrutiny; bone exposure proof required for each unit)
- 97605 NPWT: 1 unit per day
Dressing bundling. Routine wound cleansing, irrigation, and dressing changes are considered integral to debridement under CMS Active Wound Care billing guidelines. Don’t bill them separately. There’s no modifier that makes them independently payable alongside debridement on the same wound.
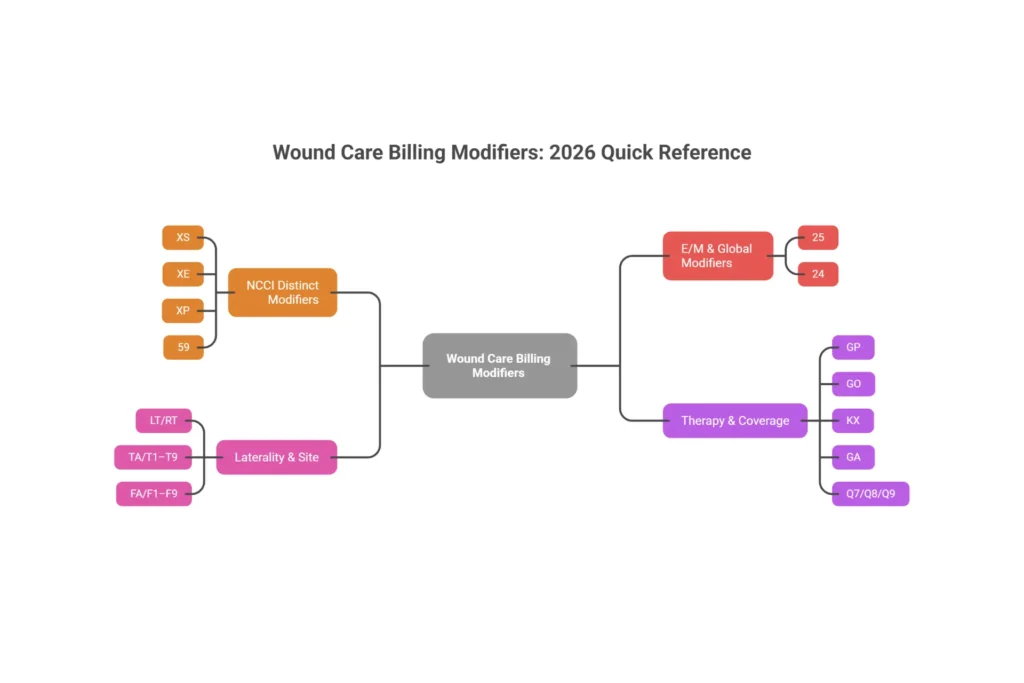
Modifier Usage in Wound Care Billing
Modifiers are what tell the payer’s adjudication system why two codes on the same claim aren’t redundant. In 2026, CMS guidance prioritizes X-series modifiers over the generic -59. Here’s every modifier wound care billers need.
| Modifier | Use Case | Documentation Required |
|---|---|---|
| XS — Separate structure | Left heel + right shin debridement | Wound locations, sizes, separate necessity per site |
| XE — Separate encounter | Morning debridement + afternoon assessment | Time-stamped notes showing distinct sessions |
| XP — Separate practitioner | MD debridement + PT evaluation same day | Provider signatures, separate roles documented |
| XU — Unusual non-overlapping | Service not integral to primary procedure | Clinical rationale in documentation |
| 59 — Distinct procedural service | Last resort when XS/XE/XP/XU don’t apply | Site-specific documentation |
| 25 — Separately identifiable E/M | New infection diagnosis + scheduled debridement | Complete E/M note beyond the procedure |
| LT/RT — Laterality | Any limb procedure | Explicit anatomic site in note |
| TA/T1–T9 — Toe | Toe wound debridement | Digit-specific location |
| FA/F1–F9 — Finger | Finger wound debridement | Digit-specific location |
| GP — PT plan of care | Physical therapist wound services | Certified POC, progress notes, 90-day recert |
| GO — OT plan of care | OT wound services | Same requirements as GP |
| KX — Therapy threshold | >$2,330 annual therapy cap | Measurable functional improvement documented |
| GA — ABN on file | Non-covered service with patient liability | Signed ABN in chart |
| Q7/Q8/Q9 — Routine foot care | Diabetic nail/callus care | Class A, B, or C findings on examined foot |
Why XS, not 59. CMS NCCI policy directs billers to use the most specific X-modifier available before defaulting to -59. Overuse of -59 is one of the top audit flags for wound care claims because it’s the modifier historically used to improperly unbundle services. XS, by contrast, is documentation-specific and harder to abuse.
Modifier 25 — the most scrutinized in wound care. Here’s how it breaks down:
- Supported: Patient presents for scheduled debridement; you also diagnose new cellulitis extending beyond the wound margin, adjust antibiotics, and document a full evaluation separately. Two distinct services.
- Not supported: “Evaluated wound and performed debridement.” That’s one service.
- Borderline: New-onset pain in the contralateral foot noted during the visit. If you examine and document the contralateral issue separately — history, assessment, plan — that supports modifier 25.
Therapy modifiers under MM10176. GP and GO must appear on every therapy claim line. KX is required when the patient exceeds the annual cap. CQ (PTA) and CO (OTA) trigger a 15% reimbursement reduction when assistants perform more than 10% of the service — bill them incorrectly and you’ll face post-payment audits.
Wound Care Coding Accuracy Estimator
Estimate how much revenue your practice may be losing to coding errors and denials.
Why Specialized Wound Care Billing and Coding Services Outperform General RCM
General RCM firms aren’t incompetent — they’re just calibrated for general medical billing. Wound care has specific technical requirements that don’t transfer from general practice, and six knowledge gaps in particular consistently cost practices six figures annually.
Gap 1: Depth vs. surface area logic. General billers apply a size-based mental model to all wound care. Specialists know surgical debridement (11042–11047) is billed by deepest tissue removed, while active wound management (97597–97598) is billed by surface area. The same wound, treated two different ways, produces two completely different code families.
Gap 2: The ZZZ add-on trap. Skin substitute applications carry add-on codes for the product units. Generalists bill only the application CPT and miss the HCPCS Q41xx codes for the graft material. The product cost passes to the practice with no reimbursement for the product.
Gap 3: 12/360 frequency monitoring. Medicare limits certain procedures. Specialists flag the 13th application with documentation supporting continued medical necessity and generate the ABN. Generalists submit it cold, receive an unappealable automatic denial, and often don’t even know why.
Gap 4: The diabetic “E + L” rule. Generalists link debridement to the ulcer code. Specialists know the etiology (E11.621) must precede the manifestation (L97.5xx) on the claim, both codes must be present, and each must link to the CPT in Box 24E. One missing link = CO-97.
Gap 5: MIST therapy unbundling. CPT 97610 (low-frequency non-contact ultrasound) is bundled with debridement on the same wound same day — modifier indicator 0. But it’s separately billable when debridement is not performed. Generalists let their software bundle it by default. Specialists capture it when it qualifies, at $100+ per visit.
Gap 6: LCD Group 1 fluency. A technically correct ICD-10 code that isn’t on the MAC’s approved list fails the LCD check. Specialists either know the Group 1 lists by MAC or run pre-submission LCD validation. Generalists learn about coverage gaps through denied claims.
The ROI calculation. A $600,000 annual wound care practice with a 15% denial rate loses $90,000 to denials. If 60% are recovered, permanent leakage is $36,000. With specialized billing at a 4% denial rate and 94% recovery, leakage drops to $1,440. Net annual gain after service fees: often $45,000–$50,000. The ROI on specialization consistently exceeds 900%.
Eight questions to ask before you sign with any billing service:
- Do your coders hold CWCC certification? (Verify through AAPC.)
- Which MAC articles do you work with — A58565, A55909, A55818?
- How do you track the 12/360 frequency limit for skin substitutes?
- What is your first-pass clean claim rate for wound care claims in POS 11?
- What is your denial recovery rate above 90 days?
- Do you use modifier XS or default to -59 for separate wound sites?
- How do you handle ABN generation for frequency exceptions?
- What was the financial impact of the 2026 skin substitute flat-rate change on your clients?
A billing service that can’t answer questions 2, 4, and 6 specifically doesn’t have the depth you need for wound care.
Learn more about what questions to ask and what to expect from our outsource wound care billing guide, or talk to us directly about whether specialized billing is right for your practice.
How Elite Med Financials Handles Wound Care Billing and Coding

No black boxes. Here’s exactly what happens to a wound care claim in our system.
Pre-service: Insurance eligibility verification before the patient arrives. LCD/NCD coverage check for the planned procedure. Prior authorization management for CTPs, NPWT, and HBO therapy — we handle the documentation of conservative care failure, the submission, and the follow-up.
Within 24 hours of the encounter: Our CWCC-certified coders audit the provider’s note. We check wound measurements, depth documentation, tissue types, and progress compared to the previous visit. If the note says “debrided to healthy tissue” without specifying the layer, we query the provider before coding — not after the claim denies.
Coding and claim build: ICD-10 dual coding for diabetic ulcers. Depth-based debridement code selection with add-ons calculated per 20 sq cm. NCCI PTP and MUE checks. Modifier assignment (XS before 59, always). CMS-1500 Box 21/24E linkage validated. Claims submitted electronically via EDI within 48 hours.
Tracking and denial management: Claim status dashboards with auto-alerts at 14 days. Technical denials (CO-16, CO-4) corrected and resubmitted same day. Clinical denials (CO-97) appealed at Level 1 Redetermination with documentation packages built from the LCD’s own medical necessity language.
AR follow-up: 30-day reminders, 60-day payer calls, 90-day escalation with weekly payer contact. We don’t let wound care claims age out.
Compliance monitoring built in:
- 8-application skin substitute cap alerts
- 12/360 debridement frequency flags with ABN auto-generation
- 30-day wound progress prompts for CTP medical necessity
- Daily OIG/SAM exclusion screening
- Quarterly internal coding audits on 5–10% of claims with 95% accuracy standard
KPIs delivered weekly: First-pass rate, denial rate by payer and reason code, days in AR, net collection rate, skin substitute flat-rate underpayment tracking.
We also offer Medicare credentialing services to get new wound care providers enrolled and billing without the 60–90 day gap that costs most practices their first quarter of revenue. And for practices looking at the full picture — billing, credentialing, digital presence, and IT infrastructure — our end-to-end practice management services cover every dimension of practice growth.
Request a Coding Accuracy Assessment →
Certifications to Look For in Wound Care Billing Professionals
Credentials in wound care billing aren’t branding — they’re the difference between a coder who can assign a code and one who can defend it during an ADR audit.
CWCC (Certified Wound Care Coder — AAPC) is the standard you should require. It covers depth-based debridement coding, skin substitute applications, NCCI edits, LCD Group 1 compliance, and dual diabetic ulcer coding. Holders earn 15–25% more than general CPCs and statistically carry lower denial rates.
CPC (Certified Professional Coder — AAPC) provides the procedural coding foundation but doesn’t include wound-specific content. A coder with CPC only is a starting point, not an endpoint, for wound care practices.
CCS (Certified Coding Specialist — AHIMA) is the credential for inpatient and facility billing. If your practice includes hospital-based wound centers or inpatient post-surgical dehiscence management, CCS holders who understand ICD-10-PCS and DRG logic are valuable.
CPCO (Certified Professional Compliance Officer — AAPC) is what makes the difference when an OIG Work Plan targets wound care. They manage internal audit programs, respond to ADRs, write rebuttal letters, and build the documentation that protects practices during MAC medical reviews.
Verifying what you’re told. Don’t accept “we have certified coders” as sufficient. Use the AAPC credential verification tool — enter the coder’s member ID and last name. Ask for a redacted sample of their denial analysis for a current wound care client. If they understand 2026 skin substitute coding, T81.320A replacement logic, and modifier XS priority, they’ll answer specific questions specifically.
From specialized coding and billing certifications to CPCO oversight of compliance programs, the credentials behind your billing team represent your first line of defense against revenue leakage and your last line of defense in an audit.
In 2026, with OIG wound care scrutiny at an all-time high and CMS implementing the most significant reimbursement restructuring wound care has seen in decades, trusting your revenue cycle to generalists isn’t a cost-saving decision. It’s a risk-assumption decision.
What is wound care billing and coding?
Wound care coding translates clinical documentation — wound depth, tissue removed, measurements — into CPT and ICD-10 codes. Wound care billing takes those codes, applies modifiers, checks NCCI edits, and submits claims to payers. Both require wound-specific expertise to avoid denials under Medicare and commercial payer rules.
What CPT codes are used for wound care?
The most common codes are 11042–11047 for surgical debridement (selected by deepest tissue removed), 97597–97598 for selective debridement (by surface area), 15271–15278 for skin substitute applications, 97610 for low-frequency ultrasound therapy, and 97605–97608 for negative pressure wound therapy.
How do you code a diabetic foot ulcer?
Diabetic foot ulcer coding requires two ICD-10 codes: E11.621 (Type 2 diabetes with foot ulcer) followed by a site and depth-specific code from the L97.5xx series, such as L97.516 for right foot with bone involvement without necrosis. Both codes must be present and linked to the relevant CPT in Box 24E of the CMS-1500.
What certifications do wound care coders need?
The CWCC (Certified Wound Care Coder) from AAPC is the specialty standard. It covers depth-based debridement, skin substitutes, NCCI edits, and LCD compliance. CPC provides the foundational credential, but CWCC is required for wound-specific accuracy.
How do you bill Medicare for wound debridement?
Submit CMS-1500 with the correct depth-based CPT (11042 for subcutaneous, 11043 for muscle, 11044 for bone), link it to a covered ICD-10 code on your MAC’s Group 1 list, include laterality modifiers (LT/RT), and verify LCD compliance before submission. Add-on codes apply for every 20 sq cm beyond the first.
What is the most common wound care billing error?
Missing dual ICD-10 coding for diabetic foot ulcers — billing E11.621 alone without the corresponding L97.5xx code. This triggers CO-97 medical necessity denials and appears in nearly every CMS CERT report for wound care as a top source of improper payments.
Frequently Asked Questions About Wound Care Billing and Coding Services
What is the difference between wound care billing and wound care coding?
Coding is the interpretive phase — a certified coder reads clinical documentation and assigns CPT and ICD-10 codes based on wound depth, tissue type, and surface area. Billing is the transactional phase — a biller applies modifiers, checks NCCI edits, and submits the claim to the payer for reimbursement. Both require wound-specific expertise; general RCM staff typically lack the depth needed for either.
What CPT codes are most commonly used in wound care billing?
The primary codes are 11042–11047 for surgical debridement (depth-based), 97597–97598 for selective debridement (surface-area-based), 15271–15278 for skin substitute application, 97610 for MIST therapy, 97605–97608 for negative pressure wound therapy, and 29580/29581 for compression bandaging. Each has specific documentation requirements and NCCI bundling rules.
Can I bill CPT 97597 and 11042 on the same wound on the same day?
No. These codes are bundled by NCCI with modifier indicator 0 — no bypass allowed. They’re considered procedure variants for the same debridement service. If both debridement types were performed on different wounds at different anatomic sites, use modifier XS with documentation supporting separate locations and medical necessity.
What certifications should a wound care coding service have?
The minimum standard is CWCC (Certified Wound Care Coder) from AAPC, which validates wound-specific CPT/ICD-10 accuracy, NCCI compliance, and LCD adherence. CCS (AHIMA) adds value for hospital or inpatient billing. CPCO oversight adds compliance and audit defense capability. Verify credentials through AAPC’s or AHIMA’s online verification tools before signing any contract.
How does the 2026 skin substitute flat-rate payment affect wound care coding?
Effective January 1, 2026, most cellular tissue products are reclassified as incident-to supplies under a flat rate of approximately $127.14 per sq cm under the CMS Physician Fee Schedule Final Rule. Old G-codes and size-based add-ons are obsolete. Current coding uses Q41xx HCPCS codes for the product and CPT 15271–15278 for application. Practices that haven’t updated their coding approach are currently losing $500–$1,000 per application.
What ICD-10 codes support medical necessity for wound debridement?
Medical necessity requires a specific, covered diagnosis code. For diabetic ulcers: E11.621 + L97.5xx. For pressure ulcers: L89.xxx with stage and site specificity (Stage 2 through unstageable — Stage 1 is non-covered). For post-surgical wounds: T81.320A–T81.329A (after October 2024; T81.32XA is deleted). Unspecified codes like L97.909 typically fail LCD Group 1 matching.
Why do wound care claims have higher denial rates than other specialties?
Wound care combines three complexity factors that most specialties don’t: depth-based code selection requiring clinical specificity, mandatory dual ICD-10 coding for diabetic ulcers, and MAC-specific LCD lists that vary by jurisdiction. General RCM services typically run 15–30% denial rates in wound care because their staff lack the wound-specific knowledge for these requirements. Specialized services hold under 5%.
What should I look for when outsourcing wound care billing?
Ask specifically about MAC jurisdiction expertise (can they cite A58565 and A55909?), NCCI edit scrubbing with quarterly updates, CWCC-certified coders, 12/360 frequency monitoring, denial recovery rates above 90%, and their approach to the 2026 skin substitute flat-rate change. A service that can’t answer these questions precisely doesn’t have the wound care depth you need.
Conclusion: Build Your Revenue on Compliant, Specialized Wound Care Billing
Three things should stay with you from this guide.
Billing and coding are different disciplines — and both require wound care specialization. Your coder needs to understand depth-based CPT selection, dual ICD-10 requirements, MAC LCD Group 1 lists, and the 2026 skin substitute coding overhaul. Your biller needs to understand modifier hierarchy, NCCI bundling indicators, MUE limits, and what each MAC’s article actually says about documentation requirements. These aren’t interchangeable skill sets.
The eight coding errors in this article account for the majority of wound care revenue leakage. Every one of them is preventable, every one has a specific documentation fix, and most of them appear in OIG and CERT audit findings year after year. The practices with low denial rates aren’t lucky — they’ve closed these gaps.
Certified coders, specialized billers, and compliance monitoring together equal your audit defense. The 2025 OIG Work Plan flagged wound care as a priority audit area. CMS CERT data consistently shows wound care as an above-average source of improper payments. If an ADR arrives, the practices that respond successfully are the ones with certified professionals who know the MAC’s own LCD language and can demonstrate medical necessity using the documentation standards the auditor is applying.
At Elite Med Financials, we’ve structured every element of our wound care billing and coding services around these principles — from CWCC-certified coders and NCCI-enabled claim scrubbers to quarterly internal audits and 24-hour documentation review. We don’t just process wound care claims — we protect wound care revenue.
Ready to see what compliant wound care billing looks like? Request your free Coding Accuracy Assessment today. We’ll review a sample of your recent claims, identify your specific leakage points, and show you the path to under 5% denials and over 98% net collection.
Request Your Free Coding Accuracy Assessment →
Related Reading: Wound Care Billing Codes Reference | Medicare Wound Care Billing Guide | Wound Care Billing Guidelines 2026 | How to Improve Revenue Cycle Management | Revenue Cycle Management Process
Disclaimer: This article reflects CMS published rules, NCCI edits, and MAC billing articles as of February 2026. Always verify current LCDs and coding guidance in the CMS Medicare Coverage Database before submitting claims, as policies are subject to change.

