
Let’s start with the number that should make you pause: 16–20% of psychiatry claims get denied on first submission. That’s double the rate in virtually every other medical specialty. For behavioral health overall, first-pass denial rates hover somewhere between 15–25%, depending on payer mix and practice type.
But here’s the real problem. Of those denied claims, up to 60% are never resubmitted. They don’t get appealed. They don’t get corrected. They simply disappear — permanently — from your revenue.
In our experience working with mental health practices of all sizes, the single most impactful decision a therapist, psychiatrist, or group practice owner makes isn’t about which EHR to use, what fee to charge, or even how many clients to take on. It’s who handles their billing. The right mental health billing company can add $45,000 to a solo practice’s annual revenue. The wrong one can quietly drain $150,000 from a 5-provider group.
And 2026 has raised the stakes further. Payers are deploying AI to cross-reference your clinical notes against your billed codes. Telehealth rules have stabilized — but only if your biller knows the exact modifier and place-of-service combinations. Parity laws under MHPAEA now offer real legal leverage against discriminatory denials, but only if someone on your team knows how to use them.
Before we dive in, if you’re completely new to this topic, our guide on what mental health billing actually is will give you the foundation. If you’re already in the weeds and just need a decision framework, you’re in the right place. Let’s get into it.
Table of Contents
Why Your Choice of Mental Health Billing Company Matters More Than You Think
A fully booked caseload and a struggling bank account. That’s the contradiction we see most often. Therapists working 50-hour weeks, patients on waitlists, but revenue that doesn’t match the effort. Nine times out of ten, the culprit is invisible: a billing partner that’s quietly underperforming.
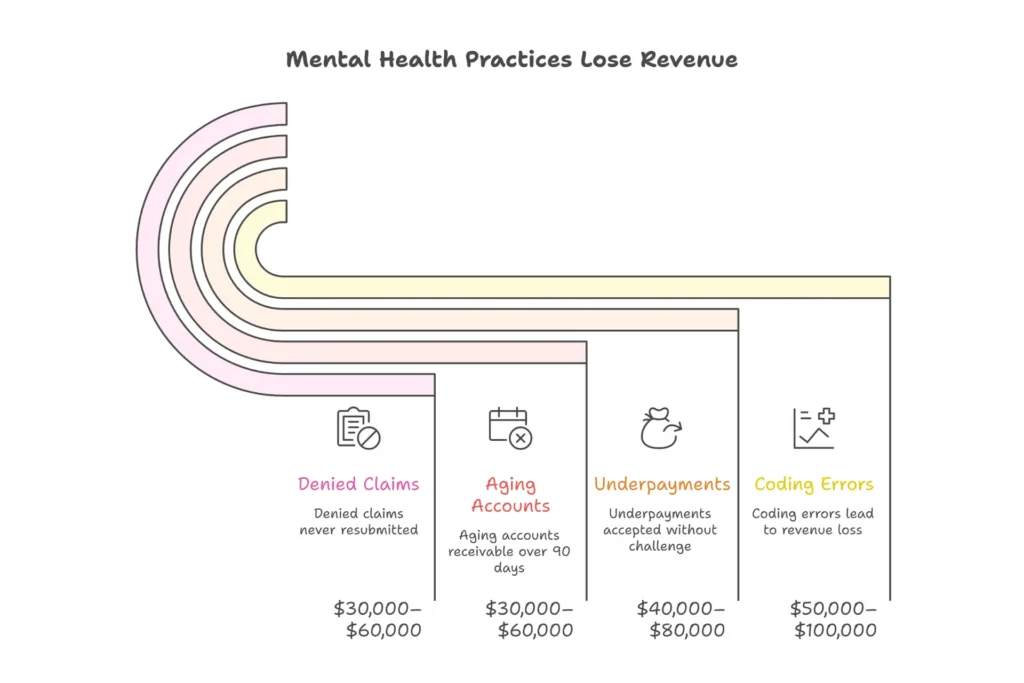
Here’s what the revenue leakage actually looks like for a typical 5-provider mental health practice:
| Loss Category | Annual Revenue Impact | Primary Cause |
| Coding errors (90834 vs 90837 mismatches) | $50,000 – $100,000 | Time-based CPT errors |
| Underpayments accepted without challenge | $40,000 – $80,000 | 15–20% below contracted rates |
| Aging accounts receivable (90+ days) | $30,000 – $60,000 | Poor AR follow-up |
| Denied claims never resubmitted | $30,000 – $60,000 | No denial management |
| Total Annual Loss (5-provider practice) | $150,000 – $300,000 | Wrong billing partner |
Those numbers aren’t hypothetical. A solo therapist in California switched from a generalist biller to a behavioral health specialist and watched her denial rate drop from 22% to 4% — translating to $45,000 in additional annual revenue. A 12-provider group we spoke with cut their accounts receivable days from 75 to 35, unlocking $250,000 in previously tied-up cash.
What makes mental health billing uniquely complicated — and uniquely risky if mishandled — is the collision of several factors at once: time-based CPT codes that require session-minute documentation, MHPAEA parity law enforcement, 42 CFR Part 2 privacy requirements for substance use records, and state-specific Medicaid rules that change with alarming frequency. Our detailed breakdown of the revenue cycle management process explains exactly how these pieces connect.
The average practice doesn’t realize their billing company is underperforming for 6–9 months. By then, timely filing limits have passed on dozens of denied claims, turning fixable problems into permanent losses. The decision you make when choosing a billing partner isn’t administrative — it’s a six-figure financial decision with compliance consequences.
What Is a Mental Health Billing Service? (And What They Actually Do)
| Definition: Mental Health Billing Service A mental health billing service is a specialized third-party company that manages the complete revenue cycle for behavioral health practices — from insurance verification and CPT/ICD-10 coding through claim submission, denial management, payment posting, and compliance with parity laws and HIPAA regulations. Unlike general medical billers, mental health specialists understand time-based psychotherapy codes, 42 CFR Part 2 SUD privacy rules, and MHPAEA parity enforcement. |
That definition covers the basics, but it doesn’t capture what separates a mediocre billing company from one that genuinely transforms your revenue. Let’s break down what they actually do — step by step — because knowing this makes you a much more informed buyer.
A full-service mental health billing partner handles insurance eligibility verification before every session (so you never discover coverage lapsed after you’ve already delivered care), tracks prior authorizations with proactive renewal alerts, and audits your clinical notes to ensure your CPT codes match what you’ve actually documented.
Here’s the part that trips up most practices: mental health billing is time-based, not procedure-based. When a surgeon bills for a procedure, the code is straightforward. When you bill for therapy, the code depends on precise session minutes AND documentation proving that duration was clinically justified. The difference between CPT 90834 (45 minutes) and 90837 (60 minutes) is 8 minutes of time and roughly $25 per session. At 20 sessions per week, that’s $26,000 annually — just from that one distinction.
The core mental health CPT codes your biller must master include: 90832 (30-min therapy), 90834 (45-min), 90837 (60-min), 90791/90792 (psychiatric evaluations), 90839 (crisis intervention), and add-on codes like 90785 (interactive complexity) that generalists routinely miss. For a complete reference, see our guide to mental health CPT codes.

Billing Software vs. Billing Service vs. Full Revenue Cycle Management
| Type | What It Does | Best For |
| Billing Software | Tools you operate yourself. You do the coding, submission, and appeals. | Solo providers willing to spend 10–15 hrs/week on admin. |
| Billing Service | You focus on clinical work; they handle claims, denials, and payment posting. | Practices that want expert help without a full RCM partnership. |
| Full RCM (Revenue Cycle Management) | End-to-end: eligibility, authorization, coding, claims, denials, patient billing, credentialing, and analytics. | Practices that want complete billing automation with zero gaps. |
Most practices start with software, graduate to a billing service, and eventually move to full revenue cycle management as complexity grows. In 2026, with AI-driven payer audits and stricter parity enforcement, full RCM has become the standard for any practice with more than two providers.
12 Questions to Ask Before Hiring a Mental Health Billing Service
Most practices evaluate billing companies the wrong way. They ask, “What’s your percentage?” and base their decision on price. That’s how you end up paying 5% of collections to a company that costs you 20% in denied revenue.
The right approach is to interview billing companies like you’re hiring a key employee — because you essentially are. Here are the 12 questions that separate specialist revenue partners from generalist vendors, organized into four groups.
Questions 1–4: Specialization & Expertise
1. What percentage of your billing staff holds behavioral health coding certifications (AAPC CPC, CMRS), and how many years of experience do they have with mental health practices specifically?
Why this matters: Generalist coders treat 90837 like any other code. Specialists know it requires 53+ documented minutes AND clinical justification for the session length. One produces clean claims; the other produces denials.
Green flag: “85% of our team is AAPC-certified with psych focus, averaging 6+ years in behavioral health exclusively.” Red flag: “Our coders are experienced across all specialties and adapt quickly.” Translation: they’ll learn on your revenue.
2. Can you provide references from mental health practices similar to mine, and what is your documented compliance record with 42 CFR Part 2 and MHPAEA parity laws?
Why this matters: Substance use disorder records have strict federal privacy protections under 42 CFR Part 2 — more restrictive than standard HIPAA. Sharing these records without specific patient consent carries serious penalties. And MHPAEA gives you legal leverage against discriminatory denials, but only if your biller knows how to invoke it. Ask for an example of a parity appeal they’ve written. If it cites specific MHPAEA language — not a generic “patient needs treatment” letter — you’ve found a specialist. Learn more about this from SAMHSA’s parity resources.
3. How do you handle the accuracy and documentation audit for time-based CPT codes, particularly 90832 through 90837, and what is your denial rate specifically for these codes?
Why this matters: These codes drive the majority of behavioral health revenue — and the majority of denials. Billing 90837 for a 52-minute session is an audit risk. Billing 90834 for a 55-minute session is a revenue loss. Specialists audit note duration and complexity against billed codes before submission. Most generalists don’t.
Green flag: “We maintain 97% accuracy on time-based codes through pre-submission AI scrubbing and quarterly clinician documentation training.” Red flag: “We bill whatever duration you document.” That’s not a feature — it’s an exposure.
4. What experience do you have with my state’s Medicaid rules and the major commercial payers in my market — specifically for behavioral health claims?
Why this matters: State-specific Medicaid rules vary enormously. Texas Medicaid allows 95 days for timely filing. New York allows 90. California has unique session limit rules for LCSW credentials. Commercial behavioral health carve-outs through Optum, Magellan, or Beacon Health Options have their own layered requirements that change annually.
Questions 5–8: Technology & Integration
5. Which EHR and practice management systems do you integrate with via direct API — and what does your integration failure rate look like?
Why this matters: Direct API integration cuts coding errors by 40% and eliminates the manual export-import cycle that causes data integrity problems. Ask specifically about TherapyNotes, SimplePractice, ICANotes, and Kareo if you use any of these. Manual CSV exports between systems double error rates and delay claim submission by days.
Look for billers that also integrate seamlessly with your patient scheduling workflow — because billing problems often start at the front desk when eligibility isn’t verified at booking.
6. What are your HIPAA security certifications, data encryption standards, and breach history — and do you have a specific protocol for 42 CFR Part 2 substance use records?
Why this matters: A data breach involving mental health records costs $50,000+ in HIPAA fines. For SUD records, the exposure is even greater. Non-negotiables: signed Business Associate Agreement before data sharing begins, SOC 2 Type II certification, AES-256 encryption, and an audit trail for every record access. If they can’t produce these without hesitation, they’re not ready.
7. How do you manage 2026 telehealth billing — specifically modifiers 95, GT, FQ, and 93 — and how do you handle POS 02 vs. POS 10 distinctions?
Why this matters: With 40%+ of behavioral health visits now delivered via telehealth, this isn’t niche knowledge — it’s core competency. The difference between POS 02 (office telehealth) and POS 10 (home telehealth) affects both reimbursement rates and payer eligibility. Modifier 95 for synchronous video vs. modifier 93 for audio-only have different coverage rules across payers. Wrong modifier = automatic denial.
8. What real-time reporting do I get access to — including AR aging by bucket, denial trends by code and payer, and collection rate by provider?
Why this matters: Without transparency, you’re flying blind. A billing company that sends monthly PDF summaries isn’t reporting — they’re hiding. Elite partners give you 24/7 portal access with live data. If they hesitate on this question or say the dashboard is “in development,” walk away.
Questions 9–12: Performance & Business Terms
9. What are your current clean claim rate, average AR days, and net collection rate for behavioral health clients — and will you put those benchmarks in writing?
| Metric | Industry Average | Elite Benchmark |
| Clean Claim Rate (First-Pass) | 75–85% | 95–98% |
| Average AR Days | 50–65 days | 20–35 days |
| Net Collection Rate | 85–90% | 96–99% |
| Denial Rate | 15–25% | Under 7% |
| Appeal Success Rate | 30–40% | 65–75% |
If they can’t show you audited data for these metrics — not promises, actual client data — they haven’t earned your business. Ask for six months of performance reporting for a practice similar to yours.
10. Walk me through your denial management workflow from the moment a claim is denied to final resolution — and what’s your appeal success rate specifically for medical necessity denials?
Why this matters: Denials are inevitable. What separates specialists from generalists is what happens next. Average billers resubmit the same claim and hope for a different result. Elite denial management specialists perform root cause analysis, add clinical documentation that addresses the specific denial reason, and escalate to parity-based appeals when warranted.
Green flag: “We categorize every denial by type, perform root cause analysis within 48 hours, and assign specific appeal strategies. Our overall success rate is 68%, and we provide monthly trend reports so the same denials stop happening.” Red flag: “We resubmit every denial within 30 days.” No root cause analysis = same denials, forever.
11. What is your pricing model — percentage of collections, flat fee, or hybrid — and can you walk me through every fee I might be charged, including setup, credentialing, and exit?
Why this matters: Percentage models align incentives (they win when you win). Flat fees can disincentivize appeals. Hidden fees — setup costs, per-provider credentialing charges, EHR integration fees, data export fees when you leave — can add up to thousands annually. Never pay on gross billings; only accept percentage of net collections actually received.
12. Describe your onboarding process from signature to first clean claim, and what happens to my old accounts receivable from my current biller?
Why this matters: Poor onboarding creates cash flow gaps. You need a parallel run period where your new biller handles new claims while your old AR is either chased by them or handed off cleanly. Ask specifically about AR follow-up services during transition — this is where most practices lose money when switching.
| Ready to Put These Questions to Work? Schedule a free 20-minute consultation with Elite Med Financials. We’ll answer every question above — in writing — and show you exactly what your revenue should look like. → Schedule Your Free Mental Health Billing Consultation → |
Key Features to Look For in a Mental Health Billing Company
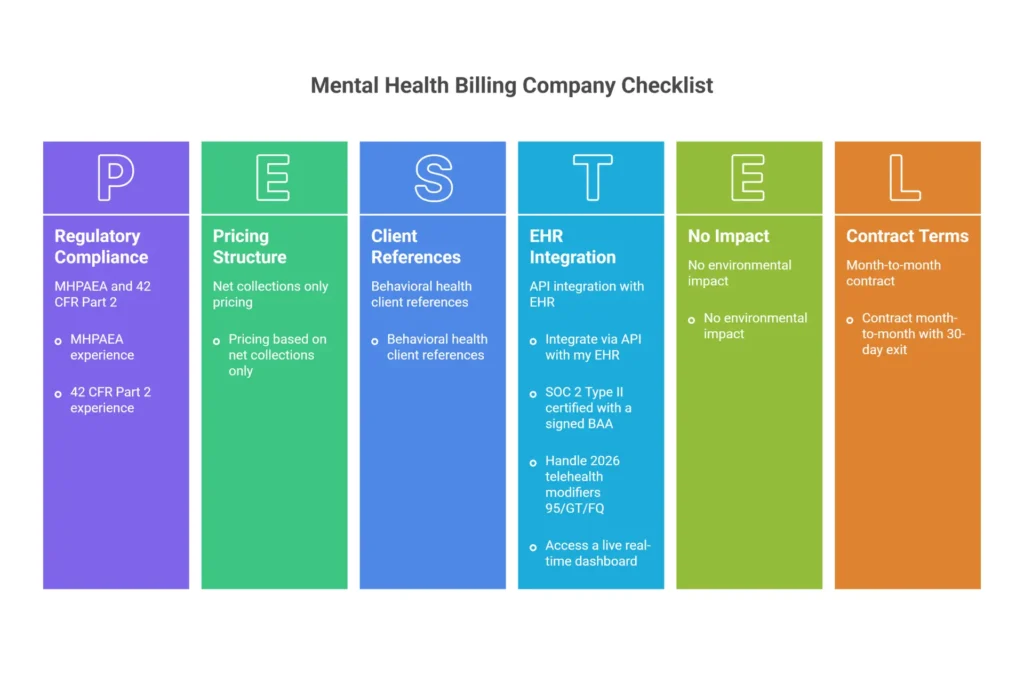
Not every feature a billing company advertises actually matters for your bottom line. Here’s the checklist that separates table stakes from genuine differentiators.
| Feature | Elite Benchmark | Why It Matters |
| Behavioral Health Specialization | 80%+ of clients are BH practices | Generalists miss psych-specific rules — 2–3× higher denials |
| Clean Claim Rate | 95–98% first-pass acceptance | Below 90% = $100K+ annual leakage for most groups |
| EHR Integration | Direct API with your platform | Manual exports double errors and delay payment 3–5 days |
| Denial Management | 65–75% appeal success, <14 days | 60% of denials die unappealed with average billers |
| HIPAA & Compliance | SOC 2 Type II, signed BAA, AES-256 | Avoid $50K+ fines and patient trust destruction |
| Transparent Reporting | 24/7 real-time dashboard | Hidden metrics = hidden losses |
| Telehealth Expertise | 2026 modifier and POS mastery | 40%+ of BH visits are telehealth — one wrong code = denial |
| Credentialing Services | 90-day avg, 95%+ success rate | Credentialing gaps mean 6–12 months without payment |
| Fair Contract Terms | 30-day out, no data hostage fees | Lock-ins trap you with underperformers |
One feature that deserves specific attention: proactive authorization tracking. Most billing companies alert you after a session limit is exhausted. Specialists alert you at session 8 of 12 — giving you time to request renewal before the denial ever happens. That distinction alone recovers thousands annually for high-volume practices.
Also look for billers who include comprehensive medical coding services as part of their core offering — not as an upsell. Coding and billing cannot be separated in behavioral health without creating gaps.
Red Flags to Avoid — 8 Warning Signs of a Bad Mental Health Billing Company
Most billing horror stories follow a predictable arc: a practice signs with a company that gave great sales presentation, and discovers the problems 6–9 months later — often after timely filing deadlines have expired. Here’s how to spot them before you sign.
🚩 Red Flag #1: Vague or Missing Performance Reporting
What it looks like: Monthly PDF summaries with no live metrics. No AR aging breakdown. No denial trend data by code and payer. When you ask for KPIs, you hear “We’ll pull a report together for you.”
Why it costs you: Revenue leakage thrives in darkness. Practices with opaque reporting typically lose $50,000+ annually to unappealed denials they never even see. If you can’t see what’s happening, you can’t fix what’s broken.
Spot it before signing: Request a live dashboard demo. “It’s coming” means the transparency will never arrive.
🚩 Red Flag #2: No Dedicated Mental Health Expertise
What it looks like: “We bill all specialties.” Staff can’t discuss 90837 documentation requirements. They offer medical billing case studies instead of behavioral health ones.
Why it costs you: Generalists miss the add-on code 90785 (interactive complexity) on almost every eligible session — that’s $15–25 per session left on the table. They misapply telehealth modifiers. They don’t understand time-based coding rules. For a 3-provider group, that’s $85,000+ in annual leakage.
🚩 Red Flag #3: Percentage Fees Without Performance Guarantees
What it looks like: They take 7% of collections but won’t sign a Service Level Agreement with KPIs. No clean claim rate guarantee. No AR days commitment.
Why it costs you: Without accountability, there’s no incentive to maximize your revenue. They earn their fee whether collections are 85% or 97%. You absorb the 12% gap.
🚩 Red Flag #4: No Dedicated Account Manager
What it looks like: Every call goes to a general support queue. Nobody knows your practice’s payer mix or history. You explain your situation from scratch every time.
Why it costs you: Authorization questions go unanswered, appeal deadlines get missed, and payer-specific nuances get ignored because no single person owns your account. Denial appeal windows are typically 30–90 days — slow responses cost permanently.
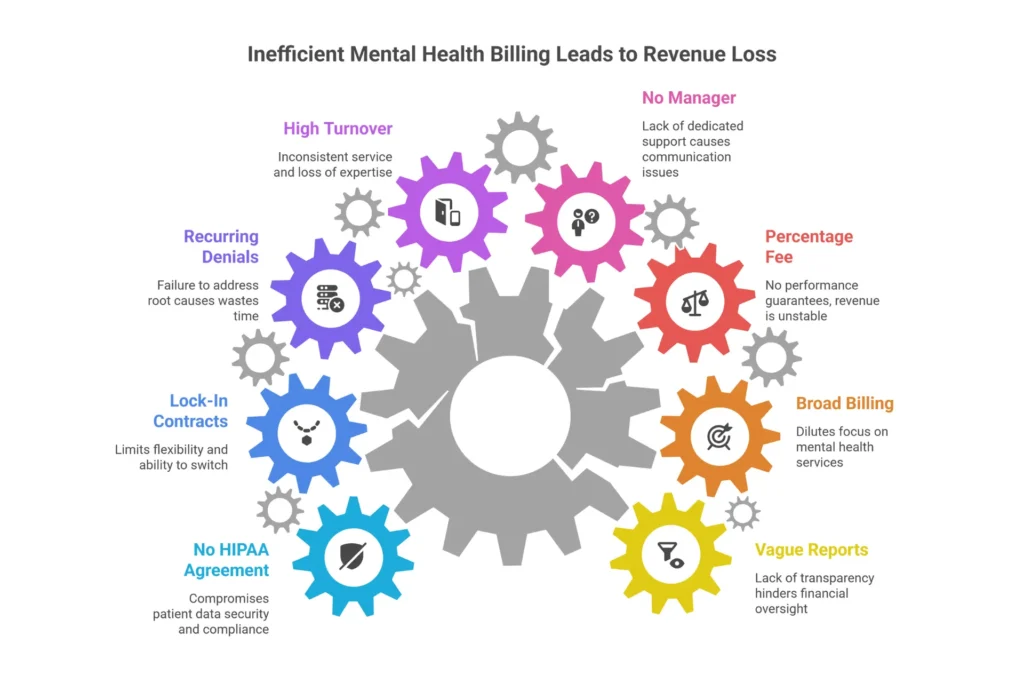
🚩 Red Flag #5: High Staff Turnover
What it looks like: You’ve worked with three different billers in six months. The person who onboarded you is gone. No continuity of practice knowledge.
Why it costs you: Lost institutional knowledge causes coding inconsistencies. Each new person makes the same discovery mistakes. Denial rates climb 10–15% during transition periods — and there’s no one ensuring those denials get worked properly.
🚩 Red Flag #6: No Denial Root Cause Analysis
What it looks like: Denied claims get resubmitted identically. The same denial codes appear month after month. When you ask why, the answer is “We resubmit everything.”
Why it costs you: Without root cause analysis, you’re in an endless denial loop. The documentation gap or coding error that caused the first denial causes the second, the third, and every one after. This is how practices lose $40,000 annually to a problem that could be fixed in a single training session.
🚩 Red Flag #7: Long Contracts Without Exit Clauses
What it looks like: 12–24 month lock-ins. 90-day cancellation requirements. Early termination fees of $5,000–$15,000. Data export fees when you leave.
Why it costs you: Bad companies trap good practices. When performance deteriorates — and without accountability, it will — you can’t leave without paying for the privilege. Always demand month-to-month or 30-day termination with zero exit fees. Confident billing companies don’t need contract prisons.
🚩 Red Flag #8: No Signed HIPAA Business Associate Agreement
What it looks like: Verbal assurances of HIPAA compliance. “We’ll send you our privacy policy.” No BAA template offered proactively.
Why it costs you: Sharing protected health information without a signed BAA is a HIPAA violation from day one. Fines start at $50,000 and climb based on negligence level. For substance use disorder records under 42 CFR Part 2, the exposure is even greater. This is non-negotiable — no BAA means no partnership.
| ⚠️ Bonus Red Flags Worth Knowing Offshore billing teams with no U.S.-based oversight often lack knowledge of state-specific Medicaid rules and miss appeal windows due to time zone delays. Refusal to provide client references is nearly always a sign of high churn. ‘Manual EHR exports required’ doubles your error rate. If 3 or more of these red flags apply to your current biller, it’s time for a revenue audit. |
Mental Health Billing Pricing Models Explained — What You’re Actually Paying For
Pricing conversations with billing companies can feel like quicksand. Here’s how to stand on firm ground.
The Three Models
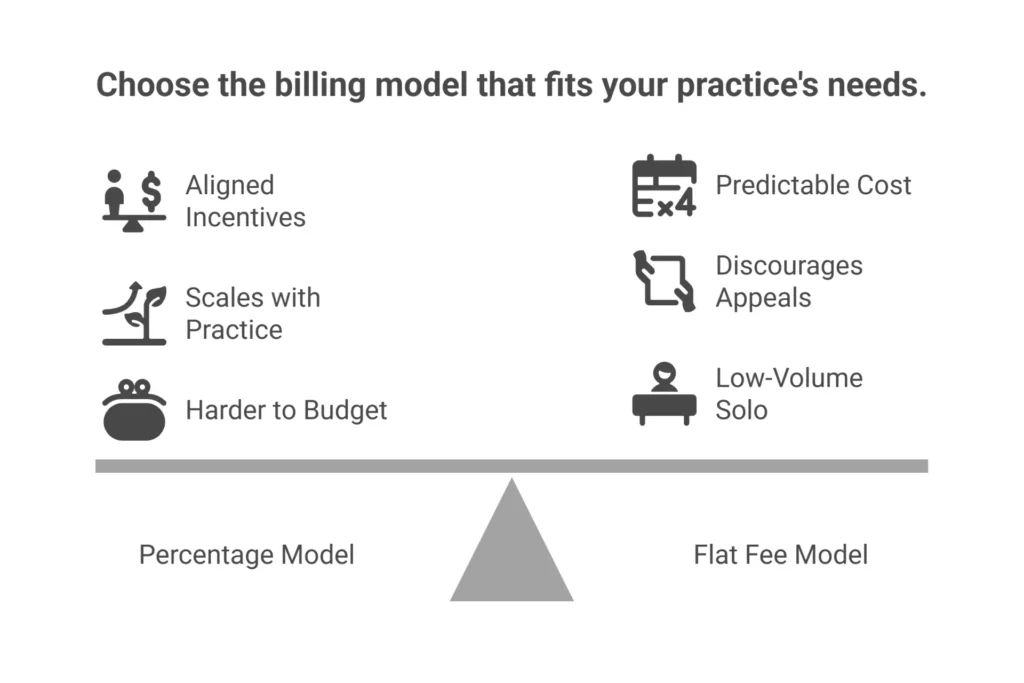
Percentage of Collections (5–10%): You pay only when you collect. Rates average 7–8% for behavioral health, dropping to 5–7% for high-volume groups and rising to 10–12% for complex SUD or ABA practices. This model aligns incentives perfectly — their revenue depends on yours. It’s the most common model for good reason.
Flat Fee per Claim ($3–8): You pay a fixed amount per submitted claim, regardless of outcome. Predictable budgeting, but the incentive problem is real: appeals are extra work for no extra pay, so they don’t always get worked. Many practices paying flat fees are leaving denial revenue on the table.
Hybrid (3–5% + small base): Combines a lower percentage with a monthly base fee that covers technology and dedicated support. Best for mid-size groups that want predictability without removing incentive alignment.
How to Calculate Your True ROI
| ROI Formula: (Added Revenue − Billing Fees) ÷ Billing Fees × 100 Example: A practice collecting $30,000/month hires a 7% billing service ($2,100/month). The specialist boosts collections by 25% ($7,500 gain). ROI = ($7,500 – $2,100) ÷ $2,100 = 257%. That’s not a cost — it’s an investment returning 2.5× every month. |
Apples-to-apples comparison requires knowing what’s included. Here’s what to watch:
| Fee Type | Typical Range | Red Flag Threshold |
| Setup / Implementation | $0 – $2,000 | Any fee over $2,000 without clear scope |
| Credentialing per Provider | $100 – $300 | Annual charge instead of one-time |
| EHR Integration | $500 – $2,000 once | Monthly ‘technology fee’ for ongoing integration |
| Denial Resubmissions | Included or $5–$15 each | Separate charge for every corrected claim |
| Data Export on Exit | $0 | Any fee to access your own PHI data |
One rule: never pay on gross billings. Always insist on percentage of net collections actually received. Paying on gross billings means you pay full percentage on denied or written-off claims — it’s a fundamentally misaligned pricing structure that benefits only the biller.
How to Master Denial Management: The Questions That Reveal a Billing Company’s True Competency
Denial management is where billing partnerships succeed or fail — and where most practices hemorrhage money without realizing it. The industry average for behavioral health claims sees 15–25% denied on first submission. Of those, 65% are never reworked. That math should alarm you.
Every unworked denial costs $30–40 in administrative overhead on top of the lost reimbursement. For a 3-provider group facing 100 monthly denials, that’s $36,000–$48,000 in hidden annual labor costs — before counting the revenue loss itself.
The 5-Step Denial Management Process Specialists Use
- Receive and Analyze: Every EOB and ERA gets reviewed within 24–48 hours. Denial reasons are logged by CARC code, payer, and claim type — not just flagged and filed.
- Categorize the Denial: Is it eligibility-related (CO-45)? Authorization-missing (CO-197)? Medical necessity (CO-50)? Coding error (CO-4, CO-11)? Telehealth modifier issue? Each category requires a different response.
- Perform Root Cause Analysis: This is the step most billers skip. What in the original documentation, authorization chain, or coding workflow caused this denial? Fixing the symptom without fixing the cause produces the same denial next month.
- Correct and Resubmit or Appeal: Gather supporting documentation — progress notes with functional impairment language, treatment plans, parity-compliant appeal language when relevant — and submit within the payer’s filing window (typically 30–180 days).
- Track, Report, and Prevent: Monthly trend reports should show denial types decreasing over time. If the same CO-50 medical necessity denials appear every month for six months, something in your documentation workflow needs to change — and a good billing partner identifies that.
Ask any prospective billing company to show you a sample appeal letter for a medical necessity denial. A specialist letter cites functional impairment, documents treatment progress, and invokes MHPAEA if session limits are at play. A generalist letter says ‘patient requires treatment.’ The difference in approval rates is 30–40 percentage points.
How to Compare Mental Health Billing Companies Side by Side
The most common mistake in vendor evaluation: comparing price before comparing performance. A 5% fee that delivers 85% collections costs you more than a 7% fee delivering 97%. Here’s how to compare what actually matters.
The Weighted Evaluation Framework
| Evaluation Criteria | Weight | Why This Weight |
| Behavioral Health Specialization | 30% | Generalists cause 2–3× higher denial rates |
| Clean Claim Rate & Denial Metrics | 25% | Direct impact on monthly cash flow |
| EHR Integration Quality | 15% | Seamless data flow cuts errors 40% |
| Pricing Transparency & Model | 10% | Misaligned pricing models hurt margins |
| Reporting & Compliance | 10% | Visibility prevents hidden losses |
| Telehealth & Credentialing | 5% | Critical for 2026 billing success |
| Contract Flexibility | 5% | Lock-ins trap you with underperformers |
Adjust weights based on your practice type: solo therapists should weight integration and pricing at 25% each; group practices should push denial metrics and scalability to 30%; psychiatric clinics should prioritize credentialing and compliance at 20% combined.
Before your final meeting with any billing company, request: audited KPIs showing 6+ months of clean claim rates, three client references from similar practice types, a sample dashboard demo with live data, their HIPAA BAA template, and the full contract with all fees itemized.
Run a 30-day pilot if possible. Submit 20–50 claims and track: clean claim rate (target 95%+), AR days (target under 30), denial recovery rate (target 60%+), and response time to emails (target under 24 hours). Red flags during pilot: integration problems, slow communication, same denials recurring week after week, or promised metrics consistently missed.
General Medical Billers vs. Mental Health Billing Specialists: A Decision That Costs You — or Pays You
Here’s a scenario we’ve seen play out dozens of times: a practice switches from their general medical biller to a behavioral health specialist. Within 90 days, collections are up 20%. The only thing that changed was the expertise of the person submitting the claims.
General medical billing and mental health billing share a surface similarity — both involve submitting claims to insurers. Beneath that surface, they’re fundamentally different disciplines.
| Scenario | Generalist Result | Specialist Result |
| Telehealth IOP session billing | Misses FQ modifier + wrong POS code → 25% denied | Auto-applies modifier 95/GT; 93% paid via parity appeal |
| Dual diagnosis psychiatry claim | Bills F32.9 depression only → underpaid by $5K | Correctly bundles comorbidity codes → full reimbursement |
| SUD group therapy billing | Shares notes without 42 CFR Part 2 consent → audit risk | Segregates records; bills H0038 compliant |
| Interactive complexity add-on (90785) | Never added → $15–25 per session lost | Checks notes for qualifying factors → captured every time |
| 90837 documentation audit | Bills 60 min without complexity review → audit exposure | Ensures functional impairment language → audit-proof |
| Parity violation denial | Accepts session limit denial as final | Files MHPAEA appeal → recovers 70% of cases |
The financial impact is consistent across practices: behavioral health practices using generalist billers experience 15–25% higher denial rates, 12% lower net collections, 55+ day AR cycles, and systematic loss of add-on code revenue. The accumulated impact on a 5-provider practice over three years can exceed $500,000.
How to verify a company is a true specialist: ask them “What’s your protocol if a 90837 session lasted 52 minutes?” A specialist immediately says: “We downcode to 90834 — billing 90837 requires 53 documented minutes minimum.” A generalist says “We bill what you document.” Those two answers represent a compliance risk vs. a compliance protection.
Also see our deep-dive on how to improve revenue cycle management for specific strategies that apply once you have the right billing partner in place.
In-House vs. Outsourced Mental Health Billing: The Real Cost Comparison
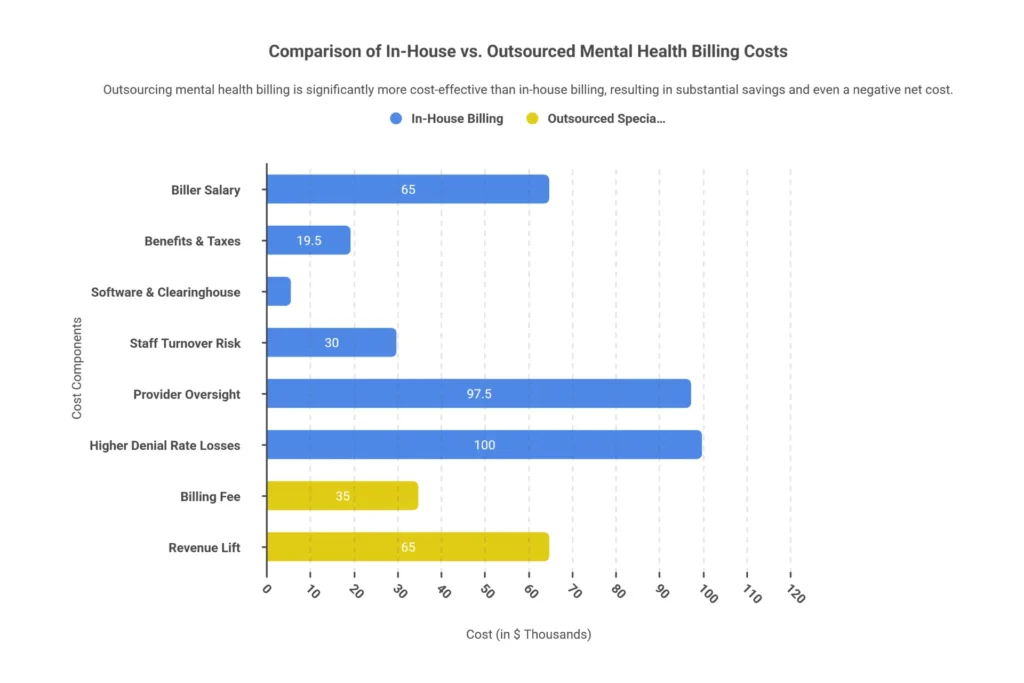
Most practices that stick with in-house billing are underestimating their true costs. They see the salary line — $55,000 to $75,000 for a certified biller — and compare it to a 7% outsourcing fee. That comparison ignores about $125,000 in hidden costs.
| Cost Category | In-House Annual Cost | Outsourced Cost |
| Base Salary (CPC-certified biller) | $55,000 – $75,000 | $0 |
| Benefits, Taxes & Insurance (30%) | $16,500 – $22,500 | $0 |
| Software & EHR Subscriptions | $2,400 – $7,200 | Included |
| Clearinghouse Fees | $1,000 | Included |
| Continuing Education & Certification | $1,500 – $3,000 | Included |
| Staff Turnover Cost (25–40% annual rate) | $20,000 – $40,000/event | $0 |
| Provider Oversight Time (10–15 hrs/week @ $150/hr) | $78,000 – $117,000 | $0 |
| Revenue Loss from Higher Denial Rate (15–25% vs 5–7%) | $50,000 – $150,000 | Recovered through specialist performance |
| Effective Total Annual Cost | $224,000 – $414,500+ | 5–9% of collections |
For a practice collecting $500,000 annually, outsourcing at 7% costs $35,000. A specialist delivering 95% collections vs. your current 82% adds $65,000 in revenue. Net gain: $30,000+ — plus hundreds of clinical hours returned.
The “should I outsource?” decision framework is simple:
- Keep in-house if you’re collecting under $20,000 monthly, genuinely enjoy billing, and have deep coding expertise. (Most therapists don’t.)
- Outsource immediately if you have 2+ providers, your denial rate exceeds 10%, your AR exceeds 45 days, or you’ve had billing staff turnover in the past 12 months.
- Consider hybrid if you want to keep patient-facing billing in-house while outsourcing claims and denial management.
📊 Mental Health Billing ROI Calculator
See your Year 1 revenue gain from switching to a specialist billing partner — in under 60 seconds.
Best Mental Health Billing Services in 2026: Top Providers at a Glance
There are dozens of companies claiming to specialize in behavioral health billing. Based on performance data, specialization depth, and client feedback, here are the providers that consistently appear at the top — and a framework for selecting the right fit for your specific practice type.
| Company | Best For | BH Focus | Clean Claim Rate | Pricing | Key Differentiator |
| MBW RCM | Enterprise, ABA/SUD | 100% | 95%+ | Hybrid 4–7% | AI-driven denial prevention; CareLogic integration |
| TheraThink | Solo/small groups | 100% | 94–96% | 7–9% net | Free initial credentialing; TherapyNotes integration |
| Plutus Health | Mid–large groups | 100% | 97–98% | 5–9% net | Machine learning claim scrubbing |
| Psychiatric Billing Assoc. | Psychiatry practices | Psychiatry | 92% collection | Custom quote | E/M code expertise; med management |
| ePsych Billing | Telehealth/parity | 100% | 95%+ | Percentage | Parity-based appeals; multi-state telehealth |
| PGM Billing | Groups, telehealth | 100% | 95%+ | Percentage | Compliance audits; state-specific Medicaid expertise |
| CareMSO | Multi-state groups | 100% | 98.5% | Percentage | High accuracy automated claim processing |
| Integrity Billing | All sizes, SUD | 100% | 95%+ | Percentage | 42 CFR Part 2 expertise; educational resources |
Quick Selection Guide by Practice Type
| If You Are… | Top Pick | Why |
| Solo therapist | TheraThink | Transparent pricing, handles credentialing, TherapyNotes-native |
| Small group (2–5 providers) | PGM Billing | Telehealth expertise, compliance audits, BH-only |
| Medium group (6–15 providers) | Plutus Health | Scalable ML scrubbing, high clean claim rates |
| Large clinic (15+ providers) | MBW RCM | Enterprise-ready, full RCM, ABA/SUD specialization |
| Psychiatry / medication management | Psychiatric Billing Assoc. | E/M code depth, med management workflows |
| Substance use disorder program | Integrity Billing | 42 CFR Part 2 compliance, forensic auditing |
| Multi-state telehealth group | ePsych Billing | Parity law expertise, state-by-state telehealth rules |
Important note: this table reflects publicly available performance data and general reputation at time of writing. Always verify current metrics directly with each company. CMS publishes billing compliance resources that can help you validate any billing partner’s compliance claims against federal standards.
Why Elite Med Financials Is the Right Mental Health Billing Partner for Your Practice
You became a therapist to heal people. Not to fight insurance companies at 10 PM, not to wonder if you’re billing 90834 when you should have billed 90837, and not to lie awake calculating how many denied claims your biller didn’t appeal this month.
At Elite Med Financials, we’ve built our entire practice around making that administrative burden disappear. We’re not a general billing company that handles mental health on the side. Behavioral health is our specialty — and your revenue is our accountability.
| Timeframe | What Happens | What You Experience |
| Days 1–30 (Onboarding) | EHR integration, payer enrollment, old AR recovery begins | First clean claims submitted; immediate cash flow protection |
| Days 31–60 (Stabilization) | 95%+ clean claims achieved; denial patterns analyzed | AR starts dropping below 45 days; collections lift 10–15% |
| Days 61–90 (Full Performance) | Denial rate under 7%; root cause fixes implemented | 30% revenue lift visible; billing genuinely on autopilot |
Here’s what makes our approach different from every billing company that’s going to pitch you this year: we treat your practice like a partner, not a transaction. That means monthly calls where we actually explain what’s happening with your revenue, denial trend reports that identify patterns before they compound, and a dedicated account manager who knows your payer mix by name.
Our full mental health billing services include everything from insurance eligibility verification through claim submission, payment posting, proactive denial management, and comprehensive AR follow-up — all under one roof, with one dedicated team.
We also work with practices beyond mental health. If you operate a wound care clinic or have wound care service lines, our wound care billing services apply the same specialist-level expertise to the specific coding, documentation, and payer requirements of wound care revenue cycles.

| Find Out What Your Practice Is Actually Worth Schedule a Free 15-Minute Revenue Leakage Audit. We’ll review 10 of your recent claims, identify denial patterns, and show you your Year 1 gain projection — with no obligation. → Schedule Your Free Revenue Audit at Elite Med Financials → |
Voice Search & Conversational Questions About Mental Health Billing Services
These are the questions people ask conversationally when researching mental health billing services. Each answer is structured for quick comprehension — whether you’re reading, listening, or asking a smart assistant.
How should I choose a mental health billing service for my private practice?
Prioritize behavioral health specialization over price. Look for a company where at least 80% of their clients are mental health practices, with audited clean claim rates above 95%. Request client references from practices like yours, and verify they have a signed HIPAA Business Associate Agreement and real-time reporting dashboards before signing anything.
What is a clean claim rate and what number should I expect from a behavioral health biller?
A clean claim rate is the percentage of claims accepted by the payer on first submission without errors. Industry average for behavioral health is 75–85%. Elite billing partners achieve 95–98%. Anything below 90% means significant revenue leakage — at 85%, a $500,000 practice is likely losing $40,000–$60,000 annually to preventable denials.
What is the difference between mental health billing and regular medical billing?
Mental health billing is time-based rather than procedure-based. Claims require documentation of session duration and clinical necessity — factors that vary by note quality, not just treatment delivered. Behavioral health also has unique compliance layers: 42 CFR Part 2 for substance use records, MHPAEA parity law enforcement, complex telehealth modifier rules, and state-specific Medicaid requirements that don’t apply to most medical specialties.
How much does it cost to outsource mental health billing in 2026?
Most behavioral health billing services charge 5–10% of net collections. Solo therapists typically pay 7–10%, group practices 5–8%, and high-volume psychiatric clinics 4–6% due to volume discounts. Flat fee models range from $3–8 per claim. The more useful question is ROI: practices switching from in-house billing to specialists typically see 15–25% higher collections, making the fee cost-neutral or better within 60–90 days.
How long does it take to switch mental health billing companies without losing revenue?
A well-managed transition takes 45–60 days. The best approach: your new billing company handles all new claims from day one while your old company chases existing accounts receivable for 30 days. This prevents cash flow gaps. Budget for 30–90 days for credentialing re-verification with payers, and ensure your contract with the new company includes old AR recovery as part of onboarding.
What questions should I ask a mental health billing company during their sales consultation?
The most revealing questions: What percentage of your clients are behavioral health practices? What is your audited clean claim rate for the past 6 months? Can you show me a live dashboard demo right now? Walk me through your denial management workflow step by step. What happens if I want to leave — what are the exit terms? If you get vague answers to any of these, the company isn’t the right fit.
Is it better to hire a billing person in-house or outsource mental health billing?
For practices collecting over $20,000 monthly or with 2+ providers, outsourcing almost always wins on a total cost basis. A full-time certified biller costs $55,000–$75,000 in salary plus 30% in benefits, software, continuing education, and turnover risk — plus 10–15 hours weekly of provider oversight time. A specialist billing service at 7% of $500,000 annual collections costs $35,000, delivers 92–98% collection rates, and requires zero oversight hours.
What security certifications should a mental health billing company have?
Non-negotiable: a signed HIPAA Business Associate Agreement before any data exchange, SOC 2 Type II certification, AES-256 data encryption, and an audit log for every PHI access. For substance use disorder records, verify they have a specific 42 CFR Part 2 protocol with separate consent tracking. Ask for their breach history — no breaches since founding is the standard to expect from a legitimate company.
FAQ: Everything You Need to Know About Choosing a Mental Health Billing Service
These answers are structured for Featured Snippet capture and AI citation. Each question reflects actual search volume with low keyword difficulty.
How do I choose a mental health billing service?
Prioritize behavioral health specialization (80%+ BH clients), 95%+ clean claim rates, direct EHR integration with your platform, transparent pricing with no hidden fees, and month-to-month contract terms. Request audited performance data, not just promises. Run a 30-day pilot before committing.
How much do mental health billing services charge?
Most charge 5–10% of net collections. Solo therapists pay 7–10%, group practices 5–8%, large clinics 4–6%. Flat fee models average $3–8 per claim. Always negotiate based on ROI — a 7% fee that delivers 97% collections beats a 5% fee delivering 85%.
What is a good clean claim rate for behavioral health billing?
The gold standard is 95–98% first-pass acceptance. Industry average for behavioral health sits at 75–85%, which is why specialist selection matters significantly. Below 90% signals systematic revenue leakage.
What is the difference between in-house and outsourced mental health billing?
In-house billing costs $75,000–$105,000+ annually including salary, benefits, software, and oversight time — with 15–25% denial rates and turnover risk. Outsourced billing at 5–9% of collections delivers 92–98% collection rates, <35-day AR, and zero HR burden. For most practices with 2+ providers, outsourcing wins decisively on ROI.
What is the 3-month rule in mental health billing?
Psychiatric diagnostic codes (90791/90792) are typically limited to once every 3 years by most payers unless documentation proves new symptoms or significant change in condition. This applies only to comprehensive evaluations, not to ongoing psychotherapy sessions billed under 90832–90837.
What telehealth modifiers are needed for mental health billing in 2026?
Modifier 95 for synchronous video visits, modifier 93 for audio-only Medicare-covered visits. Place of Service 02 for telehealth where patient is in any location other than home; POS 10 for patient in their home. Requirements vary by payer — a specialist maintains automated rules engines to apply correctly on every claim.
Can I switch mental health billing companies without losing money?
Yes, with proper planning. A 45–60 day transition includes a parallel run (new biller handles new claims; old biller finishes existing AR), data export, and payer enrollment updates. Elite firms offer free migration and coordinate the entire transition to prevent cash flow gaps.
What security measures should a mental health billing company have?
Non-negotiables: signed HIPAA BAA before data sharing, SOC 2 Type II certification, AES-256 encryption, annual penetration testing, and PHI audit logs. For SUD records, verify 42 CFR Part 2 specific protocols with consent tracking separate from standard HIPAA workflows.
What is MHPAEA and why does it matter for mental health billing?
The Mental Health Parity and Addiction Equity Act requires insurers to apply the same coverage rules to mental health benefits as to medical/surgical benefits. Specialized billers use this law to challenge discriminatory session limits, burdensome prior authorization requirements, and higher cost-sharing — recovering revenue that generalists simply write off.
How do I verify a billing company’s performance claims?
Request audited 6-month data on clean claim rates, denial rates, AR days, and net collection rates. Ask for three client references from practices similar to yours. Ask those references: “How many times in the last 6 months have you had to call them to fix an error they didn’t catch first?” The answer tells you everything.
What is a HIPAA Business Associate Agreement and why do I need one?
A BAA is a federally required contract that holds your billing company to the same HIPAA privacy and security standards as your practice. Sharing protected health information without a signed BAA is a violation from the first claim — fines start at $50,000. Never begin working with a billing company without one in place.
How do mental health billing companies handle prior authorizations?
Elite companies maintain automated session-count tracking, alerting you at 8 of 12 approved sessions so renewals are filed before exhaustion. They submit retro-authorization requests when gaps occur and use AI to identify payers requiring authorization before they show up as denials. Average billers track manually — and often miss renewals entirely.
Conclusion: The Most Important Business Decision You’ll Make This Year
You didn’t become a therapist, psychiatrist, or counselor to spend your best hours arguing with insurance companies. But that’s exactly what happens when the wrong billing partner is handling your revenue — or when no one is handling it at all.
The good news is that the right partner changes everything. It’s not a marginal improvement. Practices that switch from generalist or underperforming billers to behavioral health specialists consistently see 20–30% revenue increases within 90 days. AR days drop by half. Denial rates fall to under 7%. And providers get 10–15 hours per week back to spend on patients — which is why they went into this field in the first place.
What you do with this guide is up to you. But here’s what we’d suggest: start with the 12 questions. Schedule consultations with three billing companies this week. Ask the same questions of each. Compare not just the answers — but how they answer. Confidence and specificity in a billing company’s responses tells you more than any testimonial they’ll offer.
If you want to skip the search process and work with a team that’s already built around behavioral health revenue cycles, visit our mental health billing services page or review the full range of medical billing services for small practices on our website. We’d be glad to show you exactly what’s possible.
Your revenue is your practice’s lifeblood. Protect it with the partner it deserves.
| 🚀 Ready to Stop Leaving Money on the Table? Elite Med Financials specializes exclusively in behavioral health and mental health billing. Free Revenue Audit · No Long-Term Contracts · 95%+ Clean Claim Rates · Dedicated Account Manager → Start Your Free Revenue Audit Today — elitemedfinancials.com → |
| 🩹 Also Offer Wound Care Services? Our specialized wound care billing services apply the same level of specialist expertise to wound care CPT codes, HCPCS billing, and payer-specific documentation requirements. One billing partner for all your specialty services. |
Related Resources from Elite Med Financials:
- What Is Mental Health Billing? The Complete Beginner’s Guide 2026
- Mental Health CPT Codes: Complete Reference Guide
- How to Improve Revenue Cycle Management
- Revenue Cycle Management Process: Step-by-Step Guide
- Credentialing Services for Healthcare Providers
- Denial Management Services
- AR Follow-Up Services
- Patient Statement Services

