Last Updated: February 2026 | Author: Elite Med Financials Clinical Billing Team
Let me be direct with you: wound care billing is one of the most audit-prone areas in all of Medicare. It’s not because providers are doing anything wrong — it’s because the rules are genuinely complex, they change every single year, and most of what’s published online is either outdated, incomplete, or written by someone who’s never actually submitted a claim under LCD L38902.
This guide is different. What you’ll find here is built from the actual CMS coverage articles, the live LCDs, the 2024–2026 CPT descriptor changes, the ICD-10 expansions, and the NCCI edits that are actively causing denials right now. If you’re a wound care provider, coder, biller, or practice manager trying to protect your revenue in 2026, read every section.
And if you’re spending more time fighting denials than treating patients — we should talk. Elite Med Financials’ wound care billing specialists work exclusively with wound care and specialty practices, and we know exactly what the auditors are looking for.
Table of Contents
The Regulatory Framework Behind Wound Care Billing
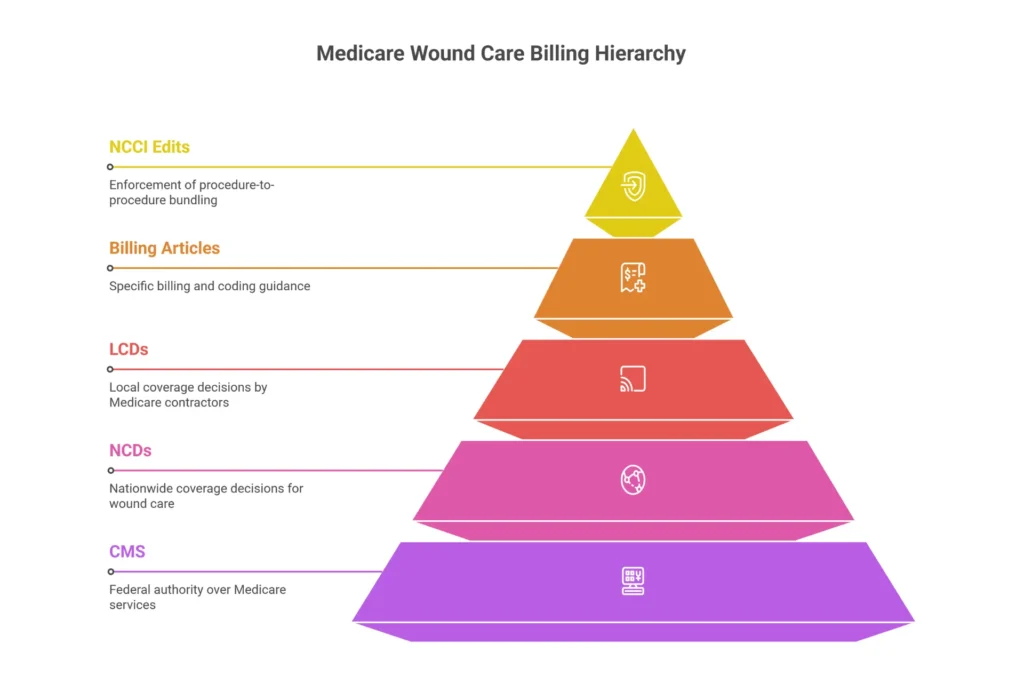
Before you touch a single CPT code, you need to understand who actually controls what Medicare pays for wound care — and why that hierarchy matters every time you submit a claim.
CMS builds wound care reimbursement in layers. At the top sit National Coverage Determinations (NCDs) — federal-level rules that apply nationwide regardless of where your practice is located. For wound care, the NCDs that matter most are NCD 270.1 (electrical stimulation and electromagnetic therapy), NCD 270.3 (blood-derived products for chronic non-healing wounds), and NCD 270.4 (decubitus ulcers). These override local rules. Always.
Below that, each Medicare Administrative Contractor (MAC) publishes Local Coverage Determinations (LCDs) — the detailed medical necessity criteria for procedures in their jurisdiction. These are the documents that list exactly which ICD-10 codes support debridement, NPWT, MIST therapy, and skin substitutes in your region. Think of NCDs as the constitution and LCDs as state law.
Then there are Billing and Coding Articles — the practical implementation guides that tell you which modifiers to use, which codes are bundled, and what documentation elements are required. The most comprehensive active article right now is A58565 (Noridian JE+JF, Revision 11, effective January 1, 2026), which covers 15+ Western and Mountain states and lists 1,173 Group 1 ICD-10 codes. Other MACs have equivalent articles: A55909 for CGS, A55818 for Palmetto and First Coast, A53001 for Novitas.
The National Correct Coding Initiative (NCCI) adds another layer — procedure-to-procedure edits that automatically deny claims where bundled codes are billed separately. And underneath it all is Section 1833(e) of the Social Security Act, which gives CMS the authority to recoup payments when documentation doesn’t support the services billed.
Here’s what most billers miss: this isn’t just theoretical hierarchy. When Noridian reviews a claim for CPT 11044, their system first checks whether the ICD-10 code is on the Group 1 list in A58565, then checks the LCD (L38902) for medical necessity criteria, then runs NCCI edits. If anything fails at any layer, the claim denies. Understanding the hierarchy lets you troubleshoot denials at the right level.
The 2026 landscape also brought a major structural shift: skin substitutes (CTPs) were reclassified from biologicals paid at ASP+6% to “incident-to supplies” under the CY 2026 Physician Fee Schedule Final Rule. The reimbursement ceiling is now a flat $127.14 per square centimeter regardless of brand. We’ll cover this in depth in the policy changes section, but know now that this changes formulary economics entirely for wound care centers.
For providers in multi-state or multi-location practices: Our RCM services include jurisdiction-specific billing protocols so your claims are compliant with the correct MAC article — not a generic template that may not match your region.
What Actually Changed in Wound Care Billing: 2024–2026 Timeline
Most articles either focus on one year or list changes without explaining their operational impact. Here’s the complete timeline with what each change actually means for your claims.
January 1, 2024 — 21 CPT Descriptor Updates
The AMA revised descriptors for 21 wound care codes to improve specificity. The affected codes include the surgical debridement series (11042–11047), active wound care codes (97597–97598), skin substitute application codes (15271–15278), and hyperkeratosis removal codes (11055–11057). The changes weren’t just cosmetic — they clarified what constitutes “selective” versus “non-selective” debridement, tightened depth-based code selection language, and eliminated ambiguity that was previously used to justify upcoding.
What it means: If your documentation language doesn’t match the updated descriptor language, your coding is vulnerable. “I removed necrotic tissue” isn’t enough. “Selective debridement of devitalized tissue from the right plantar surface using high-pressure waterjet, 12 sq cm of slough and fibrin removed” — that supports 97597.
Also effective January 2024: disposable NPWT (CPT 97607/97608) was separated from home health billing. Under Section 4137 of the Consolidated Appropriations Act, the device is now billed separately on Type of Bill 032x. If your home health agency was still bundling this, claims have been denying for over a year.
October 1, 2024 — ICD-10 Surgical Wound Expansion
T81.32XA was deleted. This was the generic code for disruption of an internal operation wound, initial encounter — and it was widely used for post-surgical dehiscence. CMS replaced it with a granular series requiring depth specificity:
- T81.320A — Disruption of deep internal surgical wound, initial encounter
- T81.321A — Disruption of superficial internal surgical wound, initial encounter
- T81.322A — Disruption of intra-abdominal surgical wound, initial encounter
- T81.329A — Disruption of unspecified internal surgical wound, initial encounter
Each code has A (initial), D (subsequent), and S (sequela) variants. If your EHR still maps to T81.32XA, your surgical wound dehiscence claims have been denying since Q4 2024. The fix requires both a system update and provider education on documenting whether dehiscence is superficial or deep.
January 1, 2025 — Strapping Code Clarification
CPT 29580 (Unna boot) received descriptor clarification distinguishing therapeutic compression from supportive strapping. This aligned with the 2022 NCCI Chapter 4, Section G update that bundled strapping with debridement on the same limb. If you’ve been billing 29580 with 11042 on the same leg without modifier XS — those claims were denied correctly.
September 25, 2025 — Noridian Article Consolidation
Noridian retired article A58567 (formerly governing JF jurisdictions — AK, AZ, ID, MT, ND, OR, SD, UT, WA, WY) and merged everything into unified article A58565, effective October 1, 2025. Revision 11 of A58565 went live January 1, 2026.
This matters for multi-state providers. If you have wound care centers in both California and Washington, you no longer need to track two separate Noridian articles. One article, one ICD-10 list, one set of rules. The consolidation also standardizes the 1,173 Group 1 ICD-10 codes and the hyperkeratosis documentation requirements across the entire Western region.
January 1, 2026 — CPT Revisions and the Skin Substitute Overhaul
Two CPT codes received revised descriptors:
CPT 29445 now reads: “Application of rigid total contact leg cast; for non-weight bearing or limited-weight bearing clinical intent” — the non-weight bearing intent must now be documented.
CPT 29581 now reads: “Application of multi-layer compression system; lower leg (below knee), including ankle and foot, requiring gradient pressure” — both elastic and inelastic components and gradient pressure are now required by the descriptor, not just good practice.
And then there’s the skin substitute change — the biggest wound care reimbursement shift in decades. The CY 2026 PFS Final Rule reclassified most CTPs from biologicals (paid at individualized ASP+6%) to “incident-to supplies” reimbursed at a flat $127.14 per sq cm regardless of brand, FDA pathway (361 HCT/P, 510(k), or PMA), or cost. The only exceptions are biologicals licensed under PHSA Section 351.
Why did CMS do this? OIG Data Brief OEI-03-23-00460 documented a 40-fold spending surge in skin substitute payments between 2019 and 2024 — from $45 million to over $1.8 billion annually. The flat rate projects $19.6 billion in savings over ten years. Expensive products that previously generated outsized revenue on ASP+6% now pay the same as cheaper alternatives.
Need help restructuring your wound care billing workflow post-2026 skin substitute reform? Our medical coding services include CTP code selection review and formulary analysis.

CPT Codes for Wound Care Billing — The Complete 2026 Reference
Active Wound Care Management: The 97xxx Series
97597 is the workhorse of outpatient wound care. It covers selective debridement of devitalized tissue (slough, fibrin, biofilm) using methods like high-pressure waterjet, sharp instruments, or mechanical scraping — first 20 sq cm or less. 97598 is the add-on for each additional 20 sq cm. Sum surface area for all wounds treated at the same session.
What people get wrong: 97597 cannot be billed with 11042–11047 on the same wound on the same day. They’re the same procedure approached from different angles — one is non-surgical, one is surgical. NCCI bundles them with no modifier bypass.
97602 (non-selective debridement) covers enzymatic agents and wet-to-moist dressings. Here’s the frustrating reality: it’s Status B — bundled. Physicians and NPPs in office settings cannot bill it separately. It may be billed by physical or occupational therapists in facility settings under a therapy plan of care, but for most office-based wound care providers, 97602 is unbillable as a standalone service.
97605–97608 cover NPWT. The split is equipment type, not wound type:
- 97605/97606: Reusable DME pump (your professional service only; the pump and supplies go to the DME MAC separately)
- 97607/97608: Disposable single-use device (all-inclusive — your service, the device, and supplies are all in the payment)
Within each pair, the split is wound size: codes ending in 5 or 7 are for ≤50 sq cm, codes ending in 6 or 8 for >50 sq cm.
97610 (MIST therapy — low-frequency ultrasound) is once per day, not billed with any debridement code on the same wound same day. Requires documentation of chronic non-healing wound status and measurable improvement with each treatment.
Surgical Debridement: The 11042–11047 Series
The rule is simple but critical: bill based on the deepest layer of tissue actually removed, not the wound depth.
- 11042: Subcutaneous tissue (fat) removed — first 20 sq cm
- 11043: Muscle and/or fascia removed — first 20 sq cm
- 11044: Bone removed — first 20 sq cm
- +11045, +11046, +11047: Add-ons for each additional 20 sq cm at the corresponding depth
For multiple wounds, sum surface areas for wounds at the same depth and report one primary code. For wounds at different depths — say, a heel wound where you debrided down to bone (11044) and a calf wound where you only reached subcutaneous tissue (11042) — report both codes with modifier XS for the separate anatomic site.
Codes 11004–11008 (necrotizing soft tissue infection debridement) and 11010–11012 (open fracture/dislocation debridement) are inpatient-only procedures and cannot be reported in office or outpatient settings. If you’re seeing these codes on outpatient claims, they’re going to deny.
For the full breakdown of every wound care CPT code including HCPCS and add-on sequencing rules, see our dedicated wound care billing codes guide.
Compression, Casting, and the NCCI Rule You Must Know
The 2022 NCCI update (Chapter 4, Section G) established that compression/strapping codes are bundled with debridement when performed on the same anatomic site on the same day:
- 29580 (Unna boot) + 11042 on the same leg = denial
- 29581 (multi-layer compression) + 97597 on the same ankle = denial
- 29445 (total contact cast) + 11042 same foot = denial
The only way to bill both is modifier XS — and only when they’re genuinely performed on different limbs with separate documentation for each site.

ICD-10 Codes That Support Medical Necessity — The “Why” Behind the Claim
Your ICD-10 code isn’t just an administrative checkbox. It’s the clinical argument for why debridement was medically necessary on this date, on this patient. An auditor reading your claim wants to see the ICD-10 code and think: “Yes, that wound required skilled intervention.” If they can’t make that connection, the claim denies.
The Dual Coding Requirement for Diabetic Ulcers
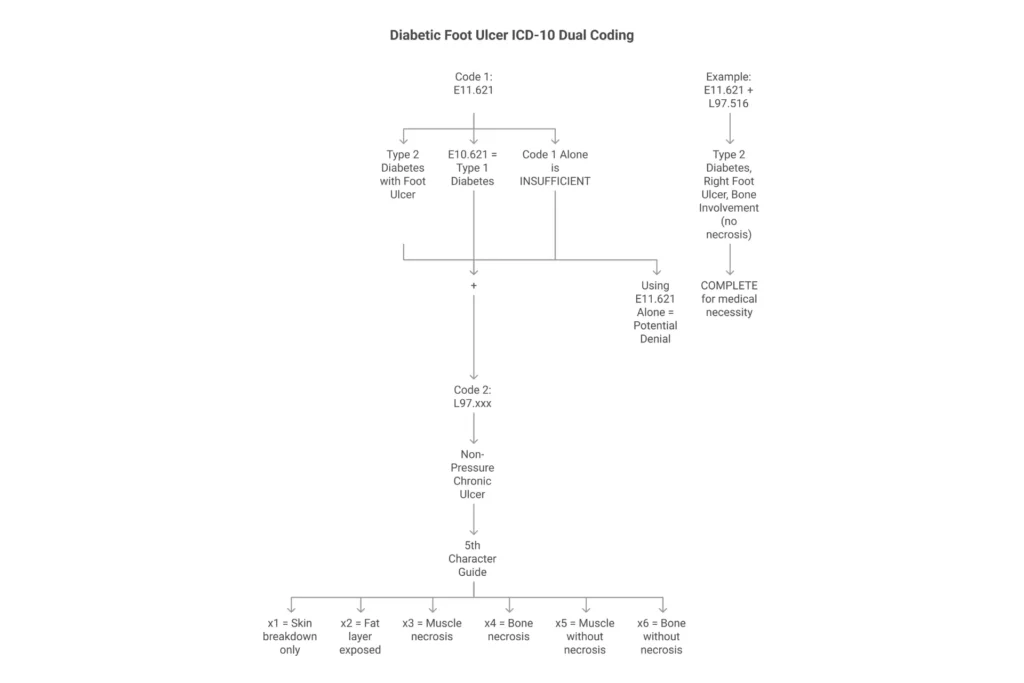
This catches providers constantly. For diabetic foot ulcers, Medicare requires two codes: the diabetes-with-ulcer code AND the site/depth-specific ulcer code.
- E11.621 (Type 2 diabetes with foot ulcer) + L97.516 (non-pressure chronic ulcer, right foot, bone involvement without necrosis) = medically necessary debridement supported
- Just E11.621 alone = insufficient specificity, potential denial
The L97 series 5th character tells the auditor exactly how deep that wound is: 1=skin breakdown only, 2=fat exposed, 3=muscle necrosis, 4=bone necrosis, 5=muscle without necrosis, 6=bone without necrosis. These depth indicators must match your CPT code selection. If you’re billing 11044 (bone debridement), your ICD-10 should show bone involvement.
The 2024 T81.32XA Replacement — What You Should Be Using Now
If you have post-surgical wound dehiscence patients and you’re still using T81.32XA — stop. That code was deleted October 1, 2024. The correct codes are:
- T81.320A: Deep internal surgical wound disruption (initial encounter)
- T81.321A: Superficial internal surgical wound disruption (initial encounter)
- T81.322A: Intra-abdominal surgical wound disruption (initial encounter)
Use A for active treatment, D for subsequent/routine follow-up visits, S for sequela (late effects). The depth specificity here isn’t just about coding compliance — it directly impacts medical necessity. Deep dehiscence justifies more aggressive debridement. Superficial dehiscence may not.
Pressure Ulcers: Stage 1 Is Non-Covered
Stage 1 pressure ulcers (L89.91x series) are not covered for debridement. Stage 1 means intact skin with non-blanchable erythema — there’s nothing to debride. Stage 2 through Stage 4 and unstageable pressure injuries qualify. When a wound is documented as Stage 1, debridement claims will deny regardless of your clinical judgment.
When NOT to Use I96 for Gangrene
I96 (Gangrene, NEC) should only be reported when gangrene isn’t already captured in another code. Do NOT report I96 alongside:
- E11.52 (Type 2 diabetes with diabetic peripheral angiopathy with gangrene) — the gangrene is already included
- I70.261/I70.262 (Atherosclerosis with gangrene) — gangrene is already included
Reporting I96 with these codes violates Excludes1 rules and triggers an automated denial.
For a complete Medicare wound care ICD-10 guide organized by wound type and LCD requirement, see our Medicare wound care billing guide.
What Medicare Actually Requires in Your Documentation
Let me tell you where most wound care audit failures originate: not from wrong CPT codes, but from documentation that doesn’t match the codes billed.
The Non-Negotiable Elements Every Visit
Per Article A58565 and Section 1833(e), every wound care visit record must contain:
- Patient name and ID on every page
- Date of service on every page
- Provider signature with credentials
- Wound location with anatomic specificity (not “lower extremity” — “right plantar 1st metatarsal head”)
- Wound measurements: length × width × depth in cm (clock method, 12:00 toward head)
- Wound bed tissue type percentages (granulation, slough, eschar, epithelialization)
- Exudate: amount (scant/moderate/copious), color, consistency
- Periwound skin condition
- Infection signs if present (erythema, warmth, purulence, odor)
- Treatment provided (method, instruments, area treated)
Matching Documentation to Your CPT Code
This is where denials happen. Here’s the specific language that must appear for each major code tier:
For CPT 97597 (selective debridement): “Selective removal of devitalized tissue [describe type: slough, fibrin, biofilm] from [location], preserving viable tissue. Method: [high-pressure waterjet/sharp/mechanical]. Total area treated: ___ sq cm.”
For CPT 11042 (subcutaneous debridement): “Sharp excision of non-viable subcutaneous tissue [fat/adipose layer] to viable tissue margins. Area: ___ sq cm.”
For CPT 11043 (muscle/fascia debridement): Must document that muscle or fascia was reached and debrided — not just “visible.”
For CPT 11044 (bone debridement): The magic words are: “Bone was exposed and tangibly debrided to healthy bleeding margins; non-viable cortical bone fragments removed.” Pathology confirmation is strongly recommended for audit defense. “Bone visible” alone does not support 11044. The bone must have been debrided.
The 30-Day Rule That Trips Up Established Patients
LCD L38902 requires measurable wound improvement — typically ≥10–20% size reduction — within 30 days of treatment. If a wound shows no progress at the 30-day mark, your documentation must explicitly address why treatment is continuing: infection, new complication, change in treatment approach, or reassessment of underlying etiology. Simply continuing the same plan without documented progress will be interpreted as services that are no longer medically necessary.
This rule catches wound care practices with high volumes of chronic patients. Monthly reassessments aren’t optional — they’re your compliance infrastructure.
Therapist Billing Under MM10176
Physical and occupational therapists billing wound care services have an additional compliance layer. Per Medicare Learning Matters MM10176:
- A physician or NPP must establish and sign a plan of care within 30 days before therapy initiation
- Progress notes are required every 10 treatment days or 30 calendar days, whichever comes first
- The plan must be recertified every 90 days
- Modifiers GP (physical therapy) and GO (occupational therapy) must appear on every therapy claim
If the plan of care isn’t in the chart, every therapy claim is vulnerable — regardless of how well the wound documentation is written.
Compliance Checklist: Modifiers, NCCI Rules, and Frequency Limits
The Modifier Hierarchy for Wound Care
One of the most common billing errors in wound care is using modifier 59 when a more specific X modifier should be applied. CMS created the X-series (XS, XE, XP, XU) precisely to provide more precise descriptions of why two procedures are distinct:
| Modifier | Use When… | Wound Care Example |
|---|---|---|
| XS | Different anatomic site/structure | Right heel debridement AND left shin debridement |
| XE | Separate encounter, same day | Morning debridement visit; afternoon assessment for new injury |
| XP | Different provider performed service | Physician debrides; PA performs subsequent procedure |
| XU | Service doesn’t overlap usual components | Specific non-overlapping circumstance |
| 59 | None of the above X-modifiers apply | Last resort — document why carefully |

For limb procedures, anatomic laterality modifiers (LT, RT) are required. For toe or finger procedures, use digit-specific modifiers (T1–T9, TA, FA, F1–F9). Noridian A58565 specifically lists these requirements — missing them is a documented denial trigger.
The NCCI Bundles You Must Know
These cannot be unbundled regardless of modifiers when performed on the same wound same day:
- 97597/97598 + 97602 (same wound)
- 97597/97598 + 11042–11047 (same wound)
- 97610 + any debridement code (same wound same day)
- 29580/29581/29445 + 11042–11047 (same limb — different limb requires XS)
- Simple wound cleaning + any debridement code
- Wound irrigation + any debridement code
Frequency Limits and When to Document Exceptions
Medicare generally limits surgical debridement to 12 sessions in a 360-day period. Within any 30-day period, 4 sessions is the threshold that triggers review. If you exceed these, your documentation must include:
- Active infection requiring aggressive management
- Documented comorbidities preventing normal healing (uncontrolled diabetes, vascular compromise, malnutrition)
- Why wound closure hasn’t been achieved
- Specific measurable progress justifying continuation
These aren’t impossible to justify — but you need to write them before the ADR arrives, not after.
The Modifier 25 Problem
To bill an E/M visit (99202–99215) on the same day as a wound procedure, modifier 25 requires a separately identifiable evaluation. That means the note must contain two distinct components: a separate medical decision-making section addressing something beyond the procedure (new infection, medication change, comorbidity management, different diagnosis), and the procedure note for the debridement.
“Evaluated wound and performed debridement” does not support modifier 25. “Evaluated new cellulitis extending 3 cm beyond wound margin, adjusted antibiotic regimen, then performed debridement” does.
ROI Denial Calculator: Is Your Wound Care Billing Costing You Revenue?
Wound Care Billing Revenue Calculator
Estimate how much revenue your practice may be losing to denials and undercoding.
MAC-Specific Wound Care Billing Requirements by Jurisdiction
Your wound care LCD isn’t the same as your colleague’s two states over. Every MAC publishes its own coverage criteria, and while the CPT codes are the same nationwide, medical necessity requirements, ICD-10 coverage lists, and documentation expectations vary. Here’s the practical breakdown:
Finding Your MAC
Go to the CMS Medicare Coverage Database. Enter your CPT code (e.g., 97597) and your state. Filter for “Active” articles and LCDs. Note the revision date — anything older than 2025 needs verification.
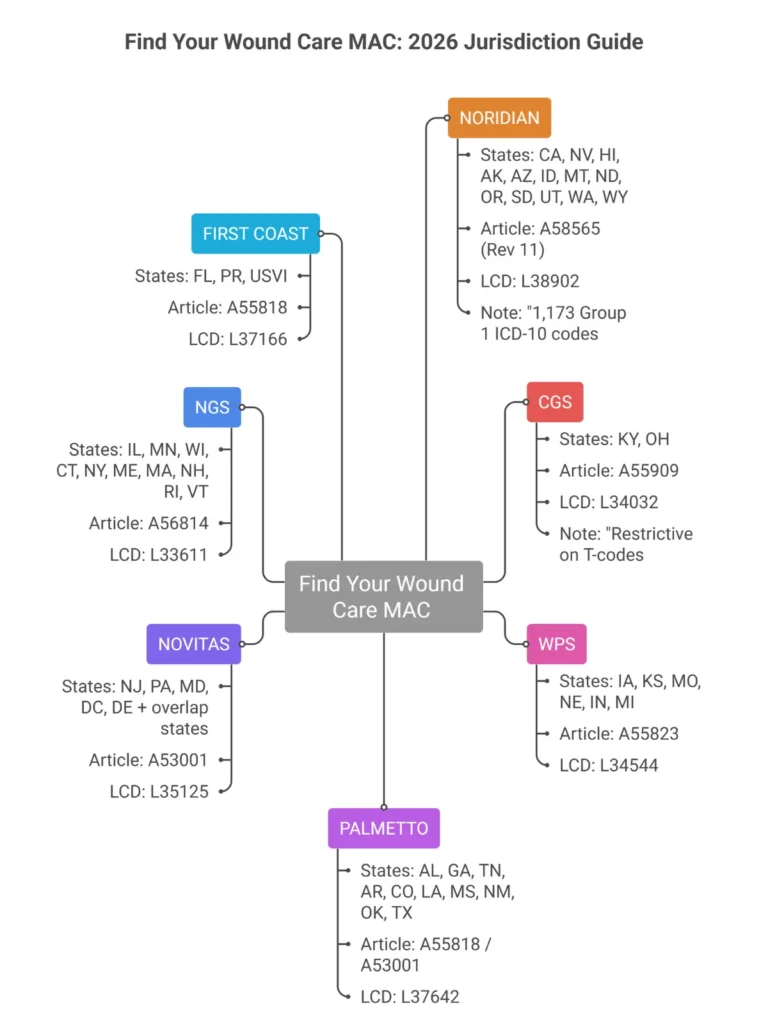
The MAC Jurisdiction Map for Wound Care
| MAC | States Covered | Active Article | LCD |
|---|---|---|---|
| Noridian | CA, NV, HI, AK, AZ, ID, MT, ND, OR, SD, UT, WA, WY | A58565 (Rev 11) | L38902 |
| CGS | KY, OH | A55909 | L34032 |
| WPS | IA, KS, MO, NE, IN, MI | A55823 | L34544 |
| Palmetto | AL, GA, TN, AR, CO, LA, MS, NM, OK, TX | A55818 / A53001 | L37642 |
| Novitas | NJ, PA, MD, DC, DE, AR, LA, TX | A53001 | L35125 |
| NGS | IL, MN, WI, CT, NY, ME, MA, NH, RI, VT | A56814 | L33611 |
| First Coast | FL, PR, USVI | A55818 | L37166 |
Key Differences That Matter Clinically
Noridian A58565 is the most specific article in the country. It provides an exhaustive list of 1,173 Group 1 ICD-10 codes and has unique hyperkeratosis documentation requirements (Groups 2 and 3 must be coded simultaneously for callus/corn removal in diabetic patients). After the September 2025 consolidation, providers across all 13 Noridian states now follow identical rules.
CGS A55909 has historically been more restrictive on surgical complication codes (T-codes). If you’re billing for post-surgical dehiscence in Kentucky or Ohio, CGS expects more detailed documentation of wound depth and prior treatment failure.
Palmetto’s approach for A55818/A53001 jurisdictions emphasizes individual medical necessity review over list-based automation. This means clinical narrative carries more weight in their adjudication process.
For providers considering outsourcing their wound care billing, jurisdictional expertise is one of the most important qualifications to ask about. Our outsource wound care billing guide covers exactly what questions to ask any billing service before signing a contract.

Recent Policy Changes and What’s Coming in 2027
The Skin Substitute “Cliff” — And Its Real-World Impact
The shift from ASP+6% to the $127.14/sq cm flat rate isn’t just a billing change — it’s a formulary decision. Products that previously reimbursed at $300–$400/sq cm under ASP+6% now reimburse at the same rate as products that cost $20/sq cm to acquire. If your wound care center built its economics around high-margin CTPs, you need to restructure now.
The three payment categories under the 2026 rule (361 HCT/Ps, 510(k) devices, PMA devices) all receive the same flat rate. The only exception is Section 351-licensed biologicals, which remain on ASP+6%. Check your formulary against the current covered product list — under 2026 LCDs, only 18 skin substitute products are explicitly listed as “covered,” while 158 are classified as “non-covered” and 154 remain at MAC discretion.
The OIG Is Watching Wound Care Closely
The 2024 OIG report documented over $100 million in improper wound care payments driven primarily by inadequate documentation. The 2025 OIG Work Plan specifically targeted skin substitute overutilization and deep debridement upcoding (billing 11044 when documentation only supports 11042). With the 2026 flat-rate reform creating new economic pressures, expect even tighter scrutiny on CTP utilization patterns.
If you’re receiving Targeted Probe and Educate (TPE) letters or Additional Documentation Requests (ADRs) for wound care, the time to audit your own documentation practices is now — not after a demand letter arrives.
What to Watch for in 2027
The proposed rule cycle for 2027 (published July 2026) is expected to include tiered APC payments for skin substitutes based on FDA pathway and clinical evidence — essentially, products with stronger outcome data may receive premium payment. A shift toward outcome-based reimbursement is likely in the mid-term. Practices that document wound closure rates, time-to-heal data, and quality-of-life outcomes will be better positioned for value-based models than those that only document procedure completion.
Also watch for Point-of-Care Imaging (POCI) mandates becoming standard for CTP reapplication authorization. Several MACs are already moving toward photo documentation requirements at specific intervals.
Understanding how revenue cycle management evolves with these regulatory shifts is why keeping your RCM strategy current matters — the billing rules that protected revenue last year may not work the same way next year.
Official CMS Resources Every Wound Care Biller Should Bookmark
Stop relying on third-party summaries for time-sensitive billing rules. These are the primary sources:
Active Billing Articles (verify revision date before relying on content):
- Article A58565 – Noridian JE/JF (Revision 11, effective 1/1/2026)
- Article A55909 – CGS
Active LCDs:
- LCD L38902 – Noridian (Wound and Ulcer Care)
National Coverage Determinations:
- NCD 270.1 — Electrical Stimulation for Wounds
- NCD 270.3 — Blood-Derived Products for Chronic Non-Healing Wounds
- NCD 270.4 — Decubitus Ulcers
- NCD 270.5 — Porcine Skin Dressings
- NCD 270.6 — Infrared Therapy Devices
- NCD 20.29 — Hyperbaric Oxygen Therapy
Subscription Services:
- CMS MLN Connects newsletter (free — subscribe at cms.gov)
- Your MAC’s email update service (Noridian, CGS, Palmetto each have separate subscription portals)
External Reference:
The American Professional Wound Care Association (APWCA) publishes clinical and coding updates that often precede or clarify CMS rule changes — worth following alongside the official CMS sources.
What CPT codes are used for wound debridement billing?
The most commonly used wound debridement CPT codes are 97597 (selective debridement, first 20 sq cm), 97598 (additional 20 sq cm), 11042 (subcutaneous surgical debridement), 11043 (muscle/fascia), and 11044 (bone debridement). Code selection is based on the deepest tissue layer removed, not wound depth.
How do you bill Medicare for wound care services?
Medicare wound care billing requires selecting the correct CPT code based on debridement depth or therapy type, pairing it with a covered ICD-10 diagnosis code from your MAC’s Group 1 list, documenting wound measurements and tissue type with each visit, and ensuring all NCCI bundling rules are followed. Claims are submitted to your Medicare Administrative Contractor based on your state’s jurisdiction.
What documentation does Medicare require for wound debridement?
Medicare requires patient identification on every page, date of service, provider signature with credentials, wound measurements (length × width × depth), tissue types with percentages, method and instruments used, tissue layers removed, and documentation that the treatment was medically necessary. For bone debridement (CPT 11044), the note must state bone was “exposed and tangibly debrided to healthy bleeding margins.”
What is the difference between CPT 97597 and 11042?
CPT 97597 is selective debridement — a non-surgical removal of devitalized surface tissue like slough and fibrin using methods such as high-pressure waterjet. CPT 11042 is surgical debridement involving sharp excision into the subcutaneous tissue layer. They cannot both be billed on the same wound on the same day due to NCCI bundling rules.
How many wound care debridements does Medicare allow per year?
Medicare generally allows up to 12 surgical debridement sessions in a 360-day period, with a threshold of 4 per 30 days. Exceeding these limits requires documented justification in the medical record, including comorbidities, infection status, and measurable clinical progress.
What changed in wound care billing for 2026?
The biggest 2026 change is the reclassification of skin substitutes (CTPs) from biologicals to “incident-to supplies” under the CMS Physician Fee Schedule Final Rule. All CTPs now reimburse at a flat rate of $127.14 per square centimeter regardless of brand, replacing the previous ASP+6% model. CPT codes 29445 and 29581 also received revised descriptors effective January 2026.
Do diabetic foot ulcers require two ICD-10 codes?
Yes. Medicare requires dual coding for diabetic foot ulcers: the diabetes-with-ulcer code (E11.621 for Type 2 diabetes with foot ulcer) plus a site and depth-specific code from the L97 series (for example, L97.516 for right foot with bone involvement without necrosis). Using only the diabetes code without the ulcer specificity code risks medical necessity denial.
Frequently Asked Questions: Wound Care Billing 2026
What are the current CMS wound care billing guidelines for 2026?
The primary sources are Article A58565 (Noridian JE/JF, Rev 11, effective January 1, 2026), Article A55909 (CGS), and A55818/A53001 (Palmetto/Novitas). These articles list covered ICD-10 codes, documentation requirements, and billing rules for debridement (11042–11047, 97597–97598), NPWT (97605–97608), MIST therapy (97610), and skin substitutes. The 2026 PFS Final Rule also restructured CTP reimbursement to a flat rate of $127.14/sq cm.
What replaced ICD-10 code T81.32XA in October 2024?
T81.32XA was deleted and expanded into depth-specific codes: T81.320A (deep internal surgical wound disruption), T81.321A (superficial), T81.322A (intraabdominal), and T81.329A (unspecified). Each has A/D/S encounter designators. Claims using T81.32XA after October 1, 2024 will deny.
Can I bill an Unna boot (29580) with debridement on the same day?
Not on the same limb. Per NCCI Chapter 4, Section G (updated 2022), CPT 29580 is bundled with surgical debridement (11042–11047) when performed on the same anatomic site on the same day. It may be separately billed with modifier XS if performed on a different limb, with documentation supporting the distinct procedure.
Does Medicare cover Stage 1 pressure ulcers for debridement?
No. Stage 1 pressure ulcers involve intact skin with no necrotic tissue present, so debridement is not medically necessary. ICD-10 codes L89.91x (Stage 1) are non-covered under all MACs. Only Stage 2 through Stage 4 and unstageable pressure injuries qualify for debridement coverage.
What is the 30-day rule in wound care billing?
LCD L38902 requires measurable wound improvement (typically ≥10–20% size reduction) within 30 days of treatment initiation. If no measurable improvement is documented within 30 days, the record must show a change in treatment approach. Continuing the same plan without progress documentation will result in denials for services deemed not medically necessary.
How do I find the correct wound care LCD for my state?
Visit the CMS Medicare Coverage Database at mcd.cms.gov. Use the Quick Search, enter your state and the CPT code (e.g., 97597), filter for “Active” documents, and identify the LCD (L-prefix) and Billing Article (A-prefix) for your MAC jurisdiction. Check the revision history to confirm you have the most current version.
What modifiers are required for wound care billing?
Modifier XS (separate structure) is used when billing debridement on multiple distinct wound sites. LT/RT modifiers are required for limb procedures. Digit-specific modifiers (T1–T9, TA, FA, F1–F9) are required for toe and finger procedures per A58565. Modifier 25 is required when billing an E/M service on the same day as a procedure. Therapy modifiers GP (PT) and GO (OT) are required for therapist-billed wound care.
What are the most common reasons wound care claims are denied?
The most frequent denial causes are: unspecified ICD-10 codes (missing laterality or depth specificity), documentation that doesn’t match CPT code billed (e.g., billing 11044 when documentation only describes fat-level debridement), NCCI bundling errors (billing 97597 and 11042 same wound), missing modifier 25 documentation for same-day E/M, exceeding frequency limits without justification, and failure to document standard care failure before advanced therapies.
Can therapists bill CPT 97597 under Medicare Part B?
Yes, physical therapists and occupational therapists can bill CPT 97597 under Medicare Part B, but only under a physician-certified plan of care (with GP or GO modifier), with proper progress note documentation every 10 treatment days or 30 calendar days, and the plan must be recertified every 90 days. CPT 97602 may also be billed by therapists in facility settings, unlike physicians in office settings where it’s Status B-bundled.
What is the 2026 skin substitute flat rate and how does it work?
Effective January 1, 2026, most skin substitute products (CTPs) are reclassified as incident-to supplies and paid at a flat rate of $127.14 per square centimeter, regardless of brand or FDA pathway (361 HCT/P, 510(k), or PMA device). Payment is tied to the application CPT codes (15271–15278). The previous ASP+6% model, which generated brand-specific variable reimbursement, is eliminated for all products except those licensed under PHSA Section 351.
Conclusion: Build Your Billing Around What CMS Actually Audits
Wound care billing in 2026 rewards exactly two things: clinical specificity in documentation and technical precision in coding. The providers getting audited aren’t necessarily doing bad wound care — they’re doing poor documentation of good care, or making coding decisions that don’t align with the regulations their MAC is enforcing.
The 2026 landscape is defined by the skin substitute flat rate, the Noridian consolidation, the T81.32XA replacement, and 21 CPT descriptor updates from 2024 that many practices still haven’t fully absorbed. Layered over that is an OIG that documented $100M+ in improper wound care payments and a 2025 Work Plan that explicitly targets deep debridement upcoding and skin substitute overutilization.
What this means practically: your billing system, your documentation templates, your coder’s knowledge base, and your compliance review schedule all need to be current as of January 2026 — not 2023 or 2024.
Three things to do this week:
- Pull your denied wound care claims from the last 90 days and identify the denial reason category. Most practices find 2–3 patterns driving 80% of their denials.
- Verify that your EHR has been updated for the T81.320–T81.329 ICD-10 series. If T81.32XA is still active in your system, you’ve had a denial source running since October 2024.
- Check your MAC’s active billing article. Confirm the revision date and compare it to what your billing team is working from.
If the answer to any of those three is unclear, that’s a signal your wound care billing deserves a professional review.
Ready to Stop Fighting Medicare Denials and Start Getting Paid?
Wound care is one of the highest-audit specialties in Medicare — and one of the most recoverable when you have a billing team that understands every layer of the regulatory framework. Elite Med Financials works with wound care practices, outpatient wound centers, and hospital-based wound programs to submit clean claims the first time, recover denied revenue, and build documentation systems that survive audits.
Our wound care billing services include:
- CPT and ICD-10 code review aligned with your MAC’s current article
- Pre-submission claim scrubbing with NCCI edit checks
- Denial management and appeal drafting
- Documentation template review against LCD requirements
- Frequency tracking and ABN management
Get a Free Wound Care Billing Assessment →
We also offer:
- Full Revenue Cycle Management (RCM) for wound care and specialty practices
- Medical Coding Services with wound care CPT specialization
- Medicare Credentialing Services to get wound care providers enrolled and billing faster
- End-to-End Practice Financial Management including enrollment, RCM, digital marketing, and IT support
Disclaimer: This guide reflects CMS published rules as of February 2026. Always verify current LCDs and billing articles in the CMS Medicare Coverage Database before submitting claims, as MAC policies and coverage criteria are subject to change.
Related Reading: How to Improve Revenue Cycle Management | Revenue Cycle Management Process | Healthcare Revenue Cycle

