Here’s a number that should stop you cold: the average behavioral health practice loses between 15 and 30 percent of its collectible revenue every year. Not to bad debt. Not to malpractice. To billing inefficiency — missed authorizations, denied claims nobody appealed, carve-out errors, coding that left money on the table session after session. The frustrating part is that most of it is preventable.
Mental health revenue cycle management (RCM) is the complete financial process that tracks a patient’s journey from appointment scheduling through final payment. It includes insurance verification, prior authorization, clinical coding, claims submission, denial management, and patient collections — all while maintaining compliance with healthcare regulations like MHPAEA and 42 CFR Part 2.
This guide covers what you actually need to know to fix it. Specifically:
- What mental health revenue cycle management includes and how it differs from general medical billing
- The 9 stages of the mental health RCM process with timing benchmarks and dollar impact at each stage
- Key performance indicators, revenue leaks, and the collection rate strategies that move practices from the industry average toward top-quartile performance
Table of Contents
What Is Mental Health Revenue Cycle Management?

Mental health revenue cycle management is the end-to-end financial lifecycle of a behavioral health practice — from the moment a patient schedules an appointment to the moment their final balance is resolved. It’s the infrastructure that turns clinical hours into actual cash flow. And in behavioral health, that infrastructure is dramatically more complex than it is in general medicine.
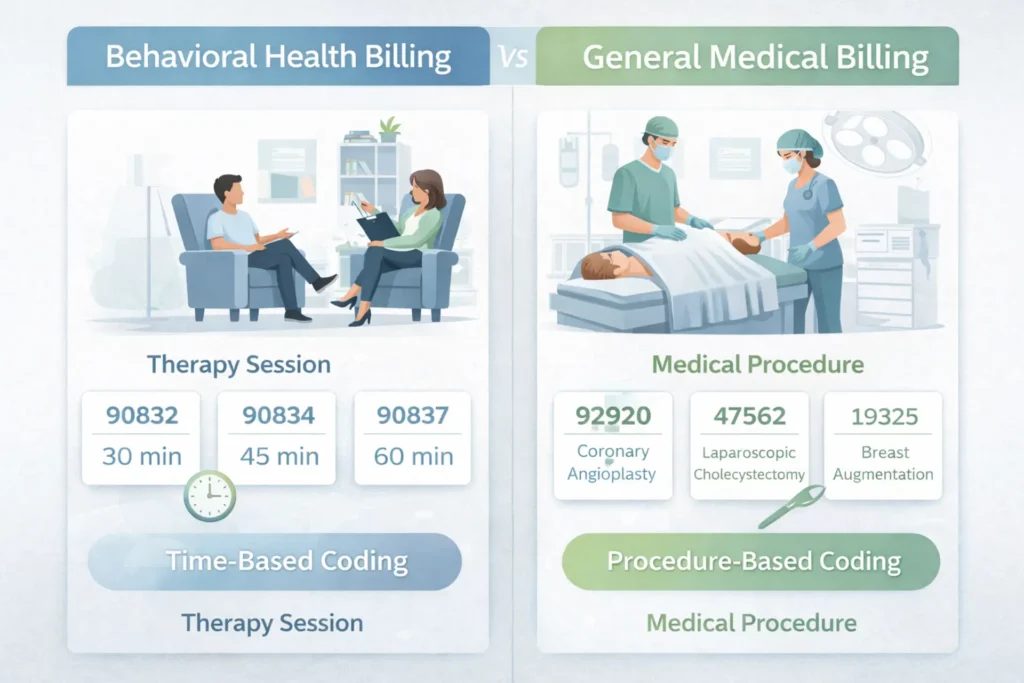
The simplest way to understand the difference: general medical billing is procedure-based and episodic. A patient comes in, something is done, a code is assigned, a claim goes out. Mental health billing is session-based, time-dependent, and ongoing. The CPT code you bill isn’t determined by what you did — it’s determined by how long you did it, documented to the minute. CPT 90832 covers 16 to 37 minutes. CPT 90834 covers 38 to 52 minutes. CPT 90837 covers 53 minutes and above. Use the wrong code because a session ran slightly shorter than documented, and you’ve either left money behind or created audit risk.
Multiply that across 25 weekly sessions, 50 weeks a year, and the revenue impact of systematic coding inaccuracy exceeds $60,000 per clinician. That’s before you account for prior authorization failures, behavioral health carve-out billing errors, and the 65 percent of denied claims that most practices never appeal.
Behavioral health revenue cycle management also operates under regulations that general medical billing doesn’t encounter. 42 CFR Part 2 creates specific consent requirements before SUD treatment claims can even be submitted. MHPAEA requires payers to apply no more restrictive limits on mental health benefits than they apply to equivalent medical benefits — and when they violate that, it creates an appeals tool most practices never use.
The types of practices that need specialized behavioral health RCM include solo outpatient therapists, group practices, Intensive Outpatient Programs (IOP), Partial Hospitalization Programs (PHP), Substance Use Disorder (SUD) treatment centers, Community Mental Health Centers (CMHCs), Certified Community Behavioral Health Clinics (CCBHCs), and residential treatment facilities. The complexity scales with the level of care — but even solo outpatient practices are affected by carve-out billing and authorization requirements that general medical billing companies are not equipped to handle.
Practices with optimized behavioral health RCM typically collect 10 to 20 percent more revenue than those using general medical billing approaches — not because they see more patients, but because they capture a higher percentage of what they’ve already earned.
| Aspect | Mental Health RCM | General Medical RCM |
|---|---|---|
| Core billing model | Time-based, recurring session model | Procedure-based, episodic care model |
| Primary coding structure | CPT 90832/90834/90837 based on exact session duration | E/M or surgical codes based on complexity |
| Authorization frequency | Per-session or weekly block (IOP/PHP) | Pre-procedure; rarely recurring |
| Payer structure | Behavioral health carve-outs common (Optum BH, Carelon, Magellan) | Integrated medical benefits |
| Regulatory overlay | 42 CFR Part 2, MHPAEA, HIPAA | HIPAA primarily |
| Documentation scrutiny | Medical necessity narrative over time; treatment response | Diagnosis and physical findings |
| Denial rate benchmark | 11–16% average nationally | 5–8% average nationally |
| Days in AR benchmark | 52 days average | 30–45 days average |
| Claim abandonment | ~65% of denied claims never appealed | Lower — higher per-claim dollar value incentivizes appeal |
| Modifier complexity | Telehealth (95, GT, FQ), interactive complexity (90785) | Anatomical modifiers (LT, RT), surgical assistants |
| Revenue leakage source | Auth expiration + carve-out errors + coding mistakes | Missing charges + downcoding E/M levels |
| Revenue leakage risk | High — 10–20% of collectible revenue | Moderate |
For practices looking to understand how behavioral health fits into the broader financial framework, our overview of the healthcare revenue cycle maps the full scope of functions from intake through collections.
The 9 Stages of Mental Health Revenue Cycle Management
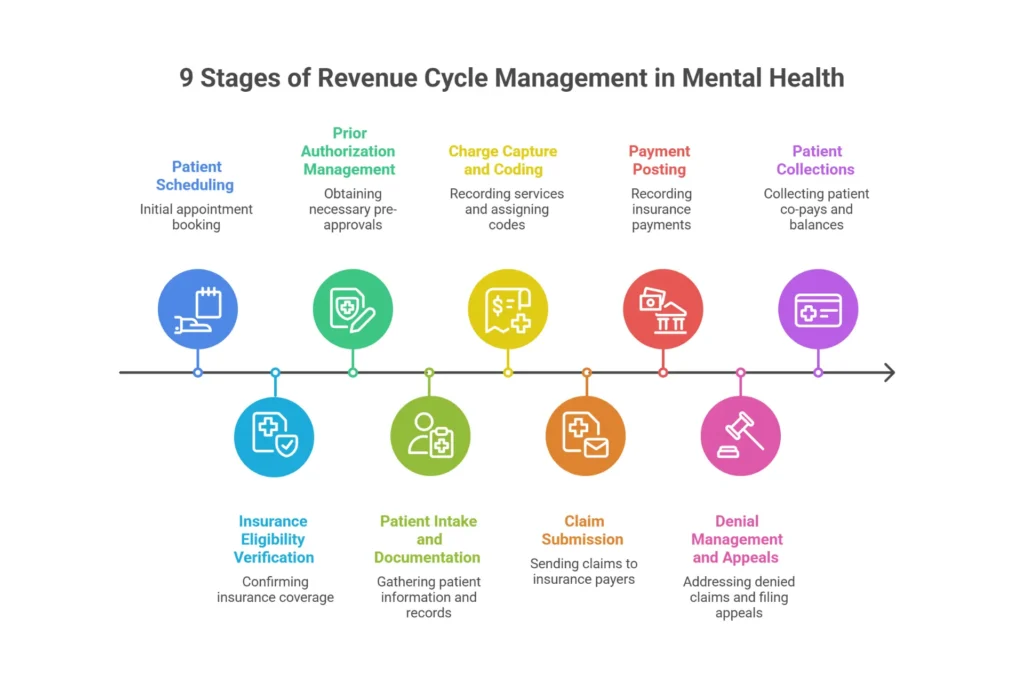
The mental health billing cycle doesn’t start when a claim is submitted. It starts before the patient ever walks through the door — and the decisions made in those early stages determine whether revenue flows cleanly or stalls at every step downstream.
Here’s where every stage fits, what it costs when it fails, and what behavioral health-specific complexity looks like at each point.
Stage 1 — Patient Scheduling (5–7 Days Pre-Visit)
This is where demographic errors and insurance data inaccuracies are born. A wrong date of birth, a transposed insurance ID, a missing secondary payer — all of it looks trivial at intake and becomes a $1,500 to $2,500 monthly claim problem. For practices with high new-patient volume, demographic accuracy at scheduling is as financially significant as any billing function downstream.
Stage 2 — Insurance Eligibility Verification (48–72 Hours Pre-Visit)
Eligibility verification in behavioral health isn’t just confirming that a patient has insurance. It requires confirming active coverage, identifying whether mental health benefits are managed by a separate behavioral health carve-out network, confirming deductible status and session limits, and flagging prior authorization requirements. Missing the carve-out identification here — billing Anthem commercial when the mental health benefits run through Carelon — creates $3,000 to $5,000 in monthly carve-out billing errors that take 30 to 60 days to surface and correct.
Stage 3 — Prior Authorization Management (72+ Hours Pre-Visit)
This is the stage with the highest financial stakes in behavioral health. Missing a prior authorization means 100 percent claim denial for the affected sessions — no partial payment, no grace period from most commercial payers. For IOP programs, authorization requires concurrent review every 7 to 10 days. Missing that window means the entire week’s revenue for that patient is gone. At $150 to $300 per session, just five to ten unapproved sessions per month represents $750 to $3,000 per clinician in permanent revenue loss. Practices with 10-plus IOP patients and no systematic authorization calendar routinely lose $15,000 to $30,000 monthly at this single stage.
Stage 4 — Patient Intake and Documentation (Within 24 Hours)
Clinical documentation doesn’t just support care — it creates or eliminates the payer’s justification for denying it. A progress note that says “patient discussed anxiety, felt better” doesn’t support medical necessity for ongoing treatment at CPT 90837. A note that documents specific symptoms, functional impairment level, treatment plan response, and clinical reasoning for continued care does. Documentation failures create $2,000 to $4,000 monthly in recoupment risk from payer audits that practices often don’t anticipate.
Stage 5 — Charge Capture and Coding (Same Day)
Time-based coding precision is where behavioral health billing diverges most sharply from every other specialty. The correct CPT code isn’t determined by the type of service — it’s determined by the documented duration. Many clinicians habitually bill 90834 to avoid the scrutiny of 90837, even when sessions clearly run 53-plus minutes with documented evidence. For a clinician seeing 25 patients per week, this fear-based downcoding costs approximately $1,175 per week or $61,000 per year per provider. Add missed interactive complexity add-on codes (90785, missed on 60 to 80 percent of eligible sessions) and the monthly coding loss for a single clinician runs $3,500 to $6,000.
Stage 6 — Claim Submission (Within 24–48 Hours)
Every day a clean, accurate claim sits unsubmitted is a day the payment clock doesn’t start. Front-end rejections from clearinghouse edits — wrong payer ID, missing authorization number, mismatched CPT and modifier — create $5,000 to $8,000 in stalled cash flow monthly. Timely filing windows compound the problem: commercial payers typically allow 90 to 180 days, carve-outs often 60 to 120 days, and Medicaid as few as 30 days in some states. Claims that sit too long in an edits queue become unrecoverable write-offs.
Stage 7 — Payment Posting (14–30 Days Post-Visit)
Payment posting is where underpayments hide. When a payer processes a 90837 claim at $112 instead of the contracted $145, that’s $33 per claim in missed revenue. At 25 weekly sessions, that’s $825 per month, $9,900 per year, from a single provider — systematically underpaying without triggering any denial alert. ERA reconciliation that audits contractual adjustments against contracted rates catches this. Manual payment posting that simply records what the payer sent does not.
Stage 8 — Denial Management and Appeals (Within 72 Hours of Remittance)
The average behavioral health practice writes off $35,000 to $50,000 in recoverable revenue annually simply because nobody has the time to appeal technical denials. Industry data from Change Healthcare consistently shows that approximately 65 percent of behavioral health denied claims are never resubmitted. On $50,000 in monthly denied claims, practices are walking away from $22,050 every month in revenue that could be recovered with proper follow-up.
The MHPAEA leverage at this stage is significant and underused. Appeals that cite parity violations — where the payer’s behavioral health criteria are more restrictive than what they apply to equivalent medical conditions — succeed at roughly 1.6 times the rate of standard medical necessity appeals. Most practices never know this tool exists. It’s standard operating procedure in specialized behavioral health billing.
Stage 9 — Patient Collections (Day of Service Through 30 Days)
Patient responsibility has become a significant portion of behavioral health revenue. High-deductible plans now account for the majority of employer-sponsored coverage, meaning patients are regularly responsible for $1,500 to $3,000 before insurance pays anything. Practices collect 80 to 90 percent of patient responsibility when it’s collected at the time of service — and only 40 to 60 percent when billed afterward. Without a card-on-file policy and automated statement workflows, $2,500 to $4,000 per month in patient balances ages into uncollectable write-offs.
| Stage | Timing Benchmark | Key Task | BH-Specific Challenge | Revenue Impact If Failed |
|---|---|---|---|---|
| 1. Patient Scheduling | 5–7 days pre-visit | Capture demographics, insurance, flag carve-out potential | Carve-out identification starts here | $1,500–$2,500/month in denials from data errors |
| 2. Eligibility Verification | 48–72 hrs pre-visit | Verify coverage, deductible, carve-out payer network | BH carve-outs require separate verification | $3,000–$5,000/month from billing wrong payer |
| 3. Prior Authorization | 72+ hrs pre-visit | Obtain initial auth; track session limits and renewals | IOP requires concurrent review every 7–10 days | $4,000–$15,000+/month from expired/missing auth |
| 4. Intake Documentation | Within 24 hrs of visit | Complete notes establishing medical necessity | Narrative-based necessity more scrutinized than in medical | $2,000–$4,000/month recoupment risk |
| 5. Charge Capture and Coding | Same day as visit | Assign correct CPT (90832/90834/90837); apply modifiers | Time-based codes require exact documentation | $3,500–$6,000/month from undercoding + missed 90785 |
| 6. Claim Submission | Within 24–48 hrs | Scrub and submit via clearinghouse | Carve-out routing errors cause systematic rejections | $5,000–$8,000/month from stalled cash flow |
| 7. Payment Posting | 14–30 days post-visit | Post ERA; reconcile contractual adjustments | Underpayments hide in contracted rate variances | $1,000–$2,000/month in undetected underpayments |
| 8. Denial Management | Within 72 hrs of remit | Categorize denial; appeal with MHPAEA leverage where applicable | 65% of denials abandoned — MHPAEA appeals succeed at 1.6× rate | 15–20% of gross revenue if denials go unworked |
| 9. Patient Collections | Day of service + 30 days | Collect copay/deductible TOS; send statements | High-deductible plans shift more revenue to patient responsibility | $2,500–$4,000/month in uncollectable balances |
Understanding how each stage connects to the full practice financial picture is covered in our guide to the revenue cycle management process — which maps how front-end functions directly determine back-end outcomes.
Key KPIs Every Mental Health Practice Should Track
If you don’t know your Net Collection Rate, your Days in AR, and your denial rate — you don’t know whether your billing is working. These aren’t administrative metrics. They’re financial vital signs. And in behavioral health, they benchmark very differently from general medicine.
The average behavioral health practice operates with a Net Collection Rate of around 91 percent and a denial rate of approximately 11.8 percent. For comparison, general medical benchmarks run at 95 to 97 percent NCR and 5 to 8 percent denial rates. That gap represents tens of thousands of dollars in annual revenue for most practices — and it’s almost entirely preventable.
Here’s how the KPIs connect to each other, which matters more than looking at them in isolation. A practice with a 15 percent denial rate will almost never see Days in AR below 50 days — because each denied claim adds 18 to 24 days to the payment cycle while it’s reworked. High DAR then reduces available cash flow, which reduces the resources available to work the denial queue, which increases the abandonment rate. The entire system degrades together. Fix the denial rate first and DAR and NCR both improve automatically.
| KPI | EliteMed Financials Threshold | Acceptable | Red Flag | BH Industry Average | Primary Lever |
|---|---|---|---|---|---|
| Net Collection Rate (NCR) | ≥96–98% | 92–95% | <90% | 91% | Reduce denials + improve patient collections |
| Days in AR (DAR) | <35 days (outpatient) | 40–50 days | >60 days | 52 days | Daily denial triage + faster claim submission |
| Denial Rate | <4% | 8–12% | >15% | 11.8% | Front-end claim scrubbing + eligibility automation |
| Clean Claim Rate (CCR) | ≥97% | 90–94% | <85% | 88% | EHR-clearinghouse integration; modifier standardization |
| Authorization Approval Rate | ≥96% (IOP/PHP) | 85–90% | <80% | 84% | Auth calendar with 80% utilization alerts |
| Patient Collection Rate | ≥90% | 75–85% | <70% | 78% | Card-on-file policy + TOS collection |
| Appeals Success Rate | >65% (with MHPAEA) | 40–50% | <30% | 42% | Parity-based appeal templates |
| 90+ Day AR Percentage | <10% | 15–18% | >25% | 21% | Weekly AR aging reviews; escalation protocol |
| Revenue Per Visit | $150–$200+ | $120–$150 | <$100 | $135 (outpatient) | Audit for undercoding; apply 90785 consistently |
Two notes on this table. First, the IOP/PHP elite DAR benchmark is 35 to 40 days — not under 30, because concurrent review authorization cycles build inherent delay into the payment timeline for intensive programs. Holding IOP billing to outpatient DAR targets sets the team up for frustration with metrics they cannot hit structurally. Second, patient responsibility now accounts for 30 to 40 percent of total behavioral health revenue in commercially insured practices. If your patient collection rate is 70 percent, your theoretical maximum NCR is around 91 percent regardless of how well everything else runs — because that 30 percent ceiling from patient abandonment prevents further improvement.
📊 Free RCM Performance Audit — Don’t know your current NCR, denial rate, or Days in AR? Our team will benchmark your practice against behavioral health industry standards and identify exactly where revenue is being lost. No charge, no commitment. Request your free audit →
Common Revenue Leaks in Mental Health Practices — And What They’re Costing You
In our work with behavioral health practices across the country, the same eight revenue leaks appear in almost every practice that is leaving money on the table. They’re not dramatic. They’re quiet, systemic, and self-reinforcing — small failures multiplied across hundreds of monthly sessions that silently erode 10 to 20 percent of revenue without ever triggering an obvious alarm.

| Revenue Leak | Monthly Impact | Root Cause | Prevention | Recovery Protocol |
|---|---|---|---|---|
| Missing prior authorizations | $8,000–$15,000 | No proactive auth tracking; assumes coverage = authorization | Auth calendar with 80% session-limit alerts; daily review | Retroactive auth request within 48 hours (~60% success) |
| Eligibility verification errors | $5,000–$10,000 | Verification only at intake; coverage lapses undetected | Automated batch VOB 24 hours before every appointment | Rebill with updated coverage; self-pay status temporarily |
| Session-length coding errors (downcoding) | $6,000–$12,000 | Fear-based billing: defaulting to 90834 instead of 90837 | Standardized start/stop documentation; monthly coding audit | Recode and resubmit if documentation supports higher code |
| Missing modifier 90785 (interactive complexity) | $1,000–$2,500 per provider | Not built into coding workflow; clinicians unaware | EHR hard stop requiring modifier selection before note sign | Corrected claim resubmission with documentation |
| IOP authorization expiration mid-treatment | $15,000–$30,000 | Manual tracking misses concurrent review windows | Daily 8 AM auth expiration report; alerts at session utilization 80% | Expedited peer-to-peer review with Medical Director |
| Carve-out billing errors | $4,000–$7,000 | Billing commercial parent instead of BH carve-out administrator | Flag carve-out payer ID in EHR at eligibility verification | Void at commercial payer; resubmit to correct carve-out |
| Timely filing denials | $3,000–$5,000 | Unsigned notes delay billing past 90-day windows | Daily unsigned note alerts; claim release same day as note sign | Appeal with clearinghouse acceptance report as proof of timely filing |
| Patient balance abandonment | $10,000–$18,000 | No card-on-file policy; paper statements sent 30+ days late | Mandatory card-on-file at intake; automated text-to-pay reminders | Payment plans; collections escalation for balances over $500 |
The carve-out billing error deserves extra attention because it’s the least visible and most systematically damaging. Optum Behavioral Health, Carelon Behavioral Health (formerly Beacon Health Options), Magellan Healthcare, and Evernorth Behavioral Health are separate payer networks managing mental health benefits independently from the commercial plans they sit behind. Being credentialed with UHC commercial does not make you credentialed with Optum BH. The claims routed incorrectly don’t even deny immediately — they pend for 30 to 45 days, then deny, at which point timely filing windows may be closing. Industry surveys estimate that 30 to 50 percent of behavioral health practices submit at least some claims to the wrong payer type annually.
The MHPAEA recovery tool is equally underused. Clinical audits of behavioral health practices consistently find that CPT 90785 (interactive complexity) is missed on 60 to 80 percent of eligible sessions — leaving $15 to $30 per session on the table. For a practice seeing families and children, that’s $1,000 to $2,500 per clinician per month in revenue earned and never billed. That’s not a denial. Nobody denied it. It just wasn’t billed.
For practices treating substance use disorder patients, MHPAEA also creates an underpayment recovery tool that almost nobody uses. If your payer reimburses SUD treatment services at rates below what they reimburse equivalent medical conditions, that may be a Non-Quantitative Treatment Limitation (NQTL) parity violation. State insurance commissioner complaints based on MHPAEA violations have successfully produced retroactive rate corrections for practices that identified the pattern and escalated it properly.
Which of These 8 Revenue Leaks Is Affecting Your Practice Right Now?
Our billing audit reviews your current denial patterns, authorization workflow, and coding accuracy against behavioral health benchmarks — and identifies exactly which of these leaks is costing you money every month. We’ve worked with practices that discovered $15,000 to $30,000 in monthly recoverable revenue they didn’t know existed.
Find My Revenue Leaks — Free →🧮 Mental Health RCM Revenue Recovery Calculator
Find out exactly how much revenue your practice is leaving uncollected — and what optimized RCM recovers
Your Revenue Recovery Analysis
Projections based on behavioral health industry benchmarks (MGMA, HFMA, Change Healthcare 2025–2026). Actual results vary by payer mix, practice type, and current workflows. For illustrative purposes only.
What Makes Behavioral Health RCM Different From General Medical Billing
Every general medical billing company says they serve mental health. Very few actually do — not because they're dishonest, but because the differences between behavioral health and general medicine run deeper than most people realize. These aren't procedural variations. They're fundamental structural differences in how care is billed, authorized, documented, and paid.
42 CFR Part 2 — The Federal Rule Nobody Warns You About
Under HIPAA, you can submit a claim for treatment services without separate patient authorization, as long as billing falls within the Treatment, Payment, and Operations exception. Under 42 CFR Part 2, that exception does not apply to substance use disorder services. Before you can submit a claim for SUD treatment to any payer, the patient must have signed a compliant Release of Information specifically authorizing that disclosure.
In general medical billing, you bill first. In SUD billing, you consent first. A practice that submits SUD claims without 42 CFR Part 2-compliant consent is committing a federal violation — not a billing error. Most general medical billing companies don't know this regulation exists. The 2024 updates to 42 CFR Part 2 clarified some consent provisions, but the core requirement remains: written, specific authorization before billing.
IOP and PHP Billing — A Different Claim Form, Different Logic
Outpatient therapy bills on the CMS-1500 professional claim form. Intensive Outpatient Programs and Partial Hospitalization Programs bill on the UB-04 institutional claim form, using revenue codes in the 0900 series. A practice that launches IOP services and continues billing them the way it bills outpatient sessions will receive systematic denials that look inexplicable until someone identifies that every claim is on the wrong form, using the wrong codes.
IOP claims use Revenue Code 0905 for psychiatric services or 0906 for substance use disorder services, paired with HCPCS code H0015 (a per diem code billed as one unit per day regardless of how many hours the patient attended, as long as the minimum threshold was met). PHP claims use Revenue Codes 0912 or 0913 depending on service intensity, with Condition Code 41 required to identify them as PHP claims. Billing H0015 with three units for a three-hour session triggers immediate denial for incorrect unit specification — and it happens constantly in practices that learned IOP billing without specific UB-04 training.
IOP authorization also operates on a weekly concurrent review cycle — documentation of continued medical necessity submitted every 7 to 10 days to justify continued enrollment at that level of care. If the patient's progress notes document stability and symptom resolution without clinical justification for continued IOP, the payer will downgrade the authorization to outpatient and deny continued IOP claims retroactively. The clinical and billing teams need to be coordinated on this. Most are not.
Carve-Out Networks and the Separate Credentialing Problem
Behavioral health carve-out networks manage mental health benefits independently from the commercial plan. Being contracted with UHC commercial does not include you in Optum Behavioral Health. Being contracted with Anthem does not include you in Carelon. The carve-out networks require separate credentialing applications, separate payer IDs for claim submission, and separate follow-up contacts for authorization and denial management.
Practices that fail to identify carve-out networks during patient eligibility verification — and then bill the commercial parent plan — see 30 to 40 percent higher denial rates in the first 90 days before the pattern becomes obvious. By then, timely filing windows may have closed on some of the affected claims.
MHPAEA — The 2024 Final Rules Changed the Landscape
The Mental Health Parity and Addiction Equity Act was significantly strengthened by 2024 Final Rules. Payers are now required to demonstrate that their Non-Quantitative Treatment Limitations — authorization requirements, medical necessity criteria, network composition standards — are not applied more stringently to behavioral health than to equivalent medical and surgical benefits.
In practice, this gives behavioral health practices specific grounds to challenge payer behavior that would have previously felt like a dead end. If a payer requires prior authorization for every therapy session but not for equivalent medical follow-up visits, that may be an NQTL parity violation. If a payer's denial rate for mental health services is materially higher than their denial rate for comparable medical services, that may be a network adequacy violation. These aren't theoretical arguments. Practices using MHPAEA arguments in denial appeals are seeing reversal rates approximately 1.6 times higher than standard appeals.
Our mental health billing services incorporate MHPAEA parity arguments as a standard component of denial management — not an escalation option for exceptional cases.
| Aspect | Behavioral Health RCM | General Medical RCM |
|---|---|---|
| Consent to bill SUD | 42 CFR Part 2 written consent required before claim submission | HIPAA TPO exception allows billing without separate release |
| Claim forms | Mix of CMS-1500 (outpatient) and UB-04 (IOP/PHP/residential) | Predominantly CMS-1500 |
| Revenue structure | Program-based bundled billing using Revenue Codes 0905/0912–0915 | Procedure-based discrete CPT billing |
| Authorization frequency | Weekly concurrent review for IOP/PHP; per-session for many codes | Pre-procedure; rarely ongoing |
| Coding basis | Time-based precision (exact start/stop documentation required) | Procedure-based; complexity scale |
| Payer network | BH carve-outs separate from commercial parent plan | Integrated medical benefits |
| Documentation scrutiny | Medical necessity requires narrative of functional impairment over time | Diagnosis and physical findings |
| Appeals leverage | MHPAEA parity arguments available; 1.6× higher success rate | Standard medical necessity arguments |
| Value-based care | CMS IBH Model (2025–2032) and CCBHC PPS shifting toward PMPM | Slower VBC adoption; predominantly fee-for-service |
| State law complexity | State confidentiality statutes add requirements beyond federal 42 CFR Part 2 | HIPAA preemption standardizes requirements nationally |
Outsourced RCM vs. In-House vs. Software — Which Is Right for Your Practice?
This question comes up every time a biller quits, a denial rate spikes past 12 percent, or AR crosses 60 days and the explanation is unclear. Let's run the actual math rather than the intuitive version.
A specialized behavioral health biller earns $46,000 to $62,000 annually. Add 25 percent for benefits, 9.5 percent for payroll taxes, $4,000 for software and tools, and $2,000 for compliance training — the fully loaded annual cost is $65,000 to $93,000. That assumes they stay. Billing staff turnover in healthcare runs 15 to 25 percent annually, and replacing a biller costs $31,000 to $60,000 in recruiting, the 3 to 6 month productivity gap while the replacement ramps up, and the cash flow freeze while claims stack.
Against that, outsourced behavioral health billing services typically cost 6 to 9 percent of collected revenue. For a practice collecting $600,000 annually, that's $36,000 to $54,000 — often less than a single in-house biller, at performance levels an in-house generalist cannot achieve without deep behavioral health specialization. The NCR gap between average in-house billing (85 to 92 percent) and specialized outsourced billing (94 to 97 percent) represents $54,000 per year on $1 million in gross billings. That gap is larger than most outsourcing fees.
For a 5-provider outpatient group billing $600,000 annually with an 82 percent in-house NCR versus a 92 percent outsourced NCR at 7 percent fee — the net ROI of outsourcing calculates to approximately 265 percent. With payback occurring in the first month of improved collections. That math isn't universal, but it's representative of what we see in mid-size outpatient practices.
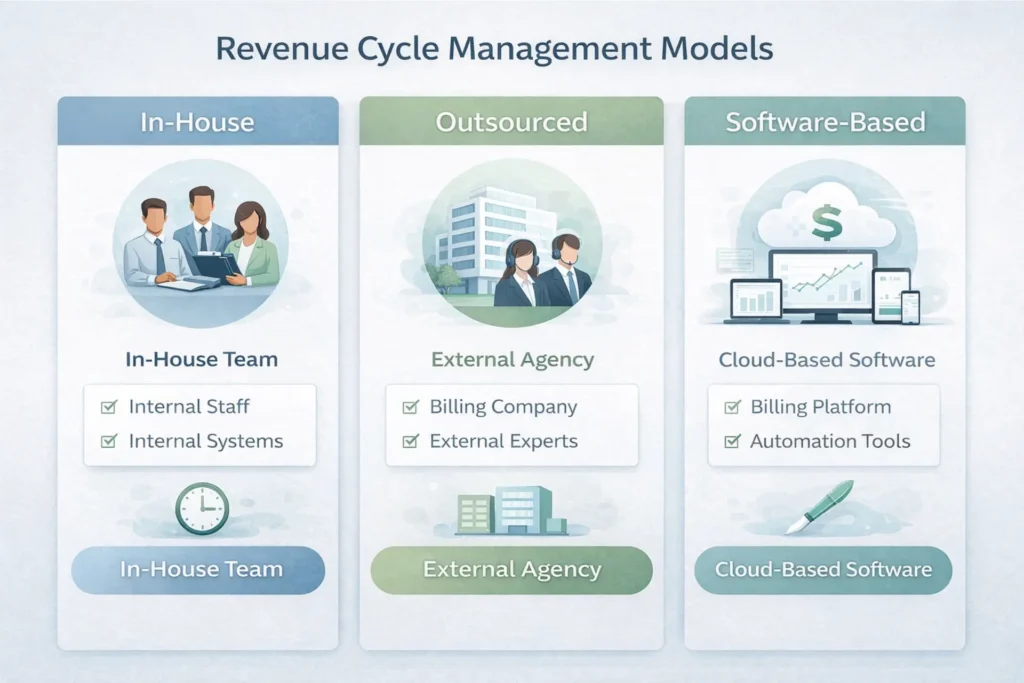
| Factor | In-House Billing | Outsourced BH RCM | Software-Only |
|---|---|---|---|
| Annual cost structure | $65,000–$93,000+ per biller (fully loaded) | 6–9% of collected revenue | $200–$500/provider/month |
| Best fit by size | $750K–$2M revenue; 4–8 clinicians | $1M+ OR any IOP/PHP/SUD program | Solo–small outpatient under $500K |
| Denial rate benchmark | 8–12% | 3–5% | Varies 5–15% depending on staff |
| Days in AR | 60–90 days | 25–35 days | 45–75 days |
| Net Collection Rate | 85–92% | 94–97% | 88–94% with trained staff |
| IOP/PHP capability | Requires UB-04 specialization | Included for BH-specialized vendors | Not adequate; CMS-1500 only |
| 42 CFR Part 2 compliance | Staff training required | Vendor manages SUD consent workflows | Platform may lack safeguards |
| Turnover risk | High — "sole knowledge" risk | None — vendor continuity | Low — platform stable |
| Scalability | Requires additional hires | Scales with collections percentage | Add provider licenses |
Software-only billing works for solo or small outpatient practices with simple payer mixes and under $500,000 to $750,000 in annual revenue. It almost universally fails for IOP and PHP programs because these require UB-04 facility billing and high-frequency concurrent reviews that logic-based automation cannot manage without human clinical coordination. The shift from CMS-1500 to UB-04 billing is often the single event that moves a practice from software-adequate to outsourcing-essential.
The full operational picture of what an end-to-end RCM function includes — and what to look for when evaluating a billing partner — is covered in our overview of complete RCM services for behavioral health practices.
How to Improve Your Mental Health Practice Collection Rate
Top-performing behavioral health practices achieve Net Collection Rates of 95 to 97 percent. The industry average is 85 to 92 percent. For a practice generating $1.5 million in annual revenue, that gap represents $45,000 to $75,000 in additional collected revenue — no new patients, no new sessions, just better execution of the billing functions already in place.
Here are the seven strategies with the clearest, most measurable impact on behavioral health collection rates.
Real-Time Eligibility Verification. Implementing automated batch eligibility checks 24 hours before every scheduled appointment — not just new patients at intake — reduces eligibility-related denials by 20 to 40 percent. At $0.25 to $0.50 per transaction, this is the highest ROI investment available in behavioral health billing. A practice avoiding $3,000 in monthly eligibility denials spends $150 on verification runs. The math requires no spreadsheet.
Time-of-Service Patient Collections. Practices collect 80 to 90 percent of copays and deductibles when collected at check-in or check-out — versus 40 to 60 percent when billed afterward. That's a 20 to 40 percentage point gap that translates to $30,000 to $90,000 in annual patient collection potential for a mid-size practice. Card-on-file policies, adopted by 82 percent of top-performing BH practices in 2026, are the infrastructure that makes this systematic rather than dependent on front-desk follow-through in individual moments.
Automated Claim Scrubbing. Pre-submission scrubbing that catches CPT and modifier combinations, authorization numbers missing on covered services, and carve-out routing errors before the claim leaves the practice improves clean claim rates by 10 to 15 percentage points. Moving from an 85 percent clean claim rate to a 95 percent clean claim rate means 10 percent fewer claims entering the denial queue — and 10 percent more claims getting paid in 14 to 21 days instead of 60 to 90.
Denial Work Queue Management. The rework cost for a single denied behavioral health claim is approximately $45 in labor and overhead. A $100 denial costs nearly half its face value just to process — which is why 65 percent of them are abandoned. The fix isn't hiring a denial specialist for every practice. It's establishing a biweekly 45-minute denial triage meeting where the billing team reviews every denied claim by payer and reason code, prioritizes by dollar value and recovery probability, and assigns follow-up before the queue ages past recovery.
MHPAEA Parity Appeals. Appeals citing MHPAEA parity violations succeed at approximately 3 times the rate of standard medical necessity appeals. Practices with documented parity appeal templates — covering session limit challenges, NQTL documentation disparities, and concurrent review criteria more restrictive than equivalent medical conditions — routinely overturn denials that standard appeals fail to recover. This is not a specialized skill. It's a template with specific language that any billing team can learn to use in 60 to 90 days with proper training.
Patient Statement and Reminder Workflows. Automated patient statement cycles — first statement within 1 to 2 weeks of balance creation, reminders every 7 to 10 days, text-to-pay links included — increase patient balance collection rates by 15 to 30 percent compared to paper statements mailed 30 days after service. 68 percent of behavioral health patients prefer mobile payment portals over paper statements. Meeting that preference isn't a technology upgrade. It's a billing fundamental in 2026.
Monthly KPI Review. Practices that conduct a formal monthly review of denial rate by payer, Days in AR by payer type, NCR trend, and 90-day AR percentage consistently identify systemic problems before they compound. A denial rate that ticks from 8 percent to 11 percent over three months signals a payer policy change or a coding pattern shift. Catching it at 11 percent is manageable. Catching it at 18 percent after six months of compounding means 4 to 6 months of rework to clear the accumulated backlog.

| Strategy | Expected NCR Improvement | Timeline to Impact | Cost Level |
|---|---|---|---|
| Real-time eligibility verification | 1–3 percentage points | 7–14 days | Low ($0.25–$0.50 per transaction) |
| Time-of-service patient collections | 3–5 percentage points | 14–30 days | Low (policy + EHR card vault) |
| Automated claim scrubbing | 2–4 percentage points | 30–60 days | Medium (software integration) |
| Denial work queue management | 2–4 percentage points | Immediate (process change) | Low (biweekly triage meetings) |
| MHPAEA parity appeals | 1–3 percentage points | 30–60 days (template development) | Low (staff training + templates) |
| Patient statement and reminder workflows | 1–2 percentage points | 14–30 days | Low (EHR automation setup) |
| Monthly KPI review | 2–5 percentage points (12-month systemic) | Ongoing | Minimal (1–2 hours monthly) |

Our denial management services incorporate all of these protocols — including MHPAEA parity appeals as standard practice — and include monthly KPI reporting so you always know where your practice stands against behavioral health benchmarks.
Don't Know Your NCR, Denial Rate, or Days in AR?
Most behavioral health practices don't — and that's exactly how 10 to 25 percent of earned revenue disappears without anyone noticing. Our team will benchmark your practice against behavioral health-specific KPIs, identify where revenue is being lost, and show you the exact gap between where you are and where you should be. No charge. No commitment.
Mental Health Revenue Codes — What Every Billing Team Needs to Know
If your practice operates any level of care beyond standard outpatient — IOP, PHP, residential, crisis services — your billing team needs to understand revenue codes. A UB-04 claim cannot process without a four-digit revenue code in Form Locator 42. Even if the CPT code is accurate and medical necessity is documented, the claim will be rejected at the clearinghouse if the revenue code field is left blank.
| Revenue Code | Description | Typical Service | Claim Form | CPT/HCPCS Pairing |
|---|---|---|---|---|
| 0900 | BH Treatments — General | Catch-all when specific code unavailable | UB-04 | Varies; use 091X when available |
| 0905 | Intensive Outpatient — Psychiatric | Psychiatric IOP (3+ hours/day) | UB-04 | H0015, S9480, CPT 90837/90853 |
| 0906 | Intensive Outpatient — Chemical Dependency | SUD IOP (3+ hours/day) | UB-04 | H0015, CPT 90837/90853 |
| 0912 | Partial Hospitalization — Less Intensive | PHP (4–6 hours/day) | UB-04 | CPT 90837/90853/90847 + Condition Code 41 |
| 0913 | Partial Hospitalization — More Intensive | PHP (6–8 hours/day, multidisciplinary) | UB-04 | CPT 90837/90853/90847 + Condition Code 41 |
| 0914 | Individual Therapy (Institutional) | One-on-one psychotherapy in facility | UB-04 | CPT 90832/90834/90837 |
| 0915 | Group Therapy (Institutional) | Group therapy in facility | UB-04 | CPT 90853 |
| 0916 | Family Therapy (Institutional) | Family sessions in facility | UB-04 | CPT 90847 |
| 1001 | Psychiatric Facility — Per Diem | Inpatient acute psychiatric | UB-04 | Bundled per diem — no separate CPT |
| 0513 | Psychiatric Clinic (Outpatient) | Freestanding outpatient psych clinic | UB-04 | CPT 90791/90837 |
| H0015 (HCPCS) | IOP per diem | Full day of IOP services (3+ hours) | UB-04 | 1 unit per day — not 1 per hour |
| H0018 (HCPCS) | Short-term residential BH | Residential treatment (non-hospital) | UB-04 | Per diem |
Three errors that happen constantly and are entirely preventable. First, H0015 is a per diem code — one unit represents the entire 3-plus-hour IOP day. Billing three units for a three-hour session triggers immediate denial. Second, Revenue Code 0905 (psychiatric IOP) and 0906 (SUD IOP) are not interchangeable. Using 0905 for SUD IOP services when the patient's primary diagnosis is substance use disorder can trigger compliance scrutiny under 42 CFR Part 2. Third, the difference between 0912 (less intensive PHP) and 0913 (more intensive PHP) is not cosmetic — CMS and most MCOs assign higher per-diem reimbursement to 0913, but documentation must support the higher clinical intensity. Billing 0913 with documentation that only supports 0912 creates recoupment risk.
For current CMS behavioral health billing guidance, the CMS Physician Fee Schedule provides authoritative rate and coding guidance. For substance use disorder treatment regulations, SAMHSA maintains current clinical and compliance resources.
How to Choose the Right Mental Health RCM Partner
Not every billing company that lists "mental health billing" on their services page actually understands behavioral health. Many are general medical billing operations that added the specialty without changing anything about their workflows, staff training, or technical infrastructure. The result for practices that hire them: average performance at industry-average prices — which means leaving $50,000 to $80,000 per year in recoverable revenue uncollected.
Here's how to identify the difference before you sign anything.
Ask what percentage of their portfolio is behavioral health. Ask for a specific number. A vendor who says "we serve many specialties including mental health" is not a behavioral health specialist. Look for 50 percent or higher in their BH client concentration — ideally above 70 percent. The carve-out routing, concurrent review management, 42 CFR Part 2 compliance, and MHPAEA appeals expertise that behavioral health practices need require daily practice. They cannot be learned adequately from a minority position in a general medical billing portfolio.
Ask them to explain their carve-out workflow. Specifically, ask how they identify whether a patient's mental health benefits are managed by Optum BH, Carelon, Magellan, or Evernorth — and how they route claims differently. A specialist will have an immediate, detailed answer. A generalist will give you a vague answer about "checking payer information." The former prevents the systematic billing errors that cost practices $4,000 to $7,000 per month. The latter lets them recur invisibly.
Ask for their current behavioral health NCR. A reputable BH billing service should show NCRs of 92 to 96 percent for their outpatient clients, with lower but still strong performance for IOP/PHP programs. Ask whether they offer contractual NCR guarantees. Top vendors include performance floors — typically 92 to 94 percent NCR — in their service agreements. If they can't tell you their current BH client average, they're not measuring it.
Ask how they handle MHPAEA in denial appeals. The answer reveals immediately whether their team is trained in behavioral health-specific billing or running standard rework appeals on BH denials. A specialized vendor will describe specific parity appeal templates and cite success rates. A generalist will look up what MHPAEA stands for after the call.
Negotiate data ownership before signing. Your patient data, claims history, and AR records belong to your practice. Any billing contract should specify that you own all data, can export it in full at any time, and face no de-conversion fees that make leaving prohibitively expensive. This is non-negotiable language, and any vendor that resists it is telling you something important about their exit economics.
Understand the transition timeline. Switching billing vendors involves a period where the outgoing vendor's claims are still processing while new claims flow to the new vendor. Expect 60 to 90 days for a clean handover and a temporary 15 to 20 percent cash flow dip in the second month as old AR dries up and new AR is still in the 14 to 21 day processing window. Ask specifically how the vendor manages the "shadow AR" — the claims submitted before the cutover date — and who is responsible for follow-up on those claims.
| Practice Type | Recommended RCM Model | Key Selection Criteria |
|---|---|---|
| Solo outpatient therapist (<$500K) | Software or entry-level outsourced | Cost efficiency; basic eligibility and claim submission |
| Small group practice (2–5 providers) | Outsourced BH-specialized (5–7% fee) | Denial management; carve-out expertise |
| Larger group practice (6–15 providers) | Full-service outsourced BH RCM (6–8%) | Account management; KPI reporting; scalability |
| IOP program (psychiatric or SUD) | Full-service with UB-04 + facility billing | Auth management; revenue code expertise; H0015 per diem |
| PHP program | Full-service with PHP authorization focus | Concurrent review; condition codes; bundled billing |
| SUD treatment center / residential | Specialized SUD billing partner | 42 CFR Part 2 compliance; HCPCS H0018/H0019/H2036 |
| CMHC / CCBHC | Enterprise BH RCM with Medicaid expertise | PPS experience; state-specific MCO billing; cost report support |
| Multi-site / multi-state | Integrated billing + credentialing | Single vendor eliminates credentialing-to-billing lag |
One integration point worth highlighting specifically: when billing and credentialing are handled by the same vendor, the credentialing effective date goes directly into the billing system without a lag. Separate vendors create a coordination gap — the credentialing firm receives an effective date and may not communicate it to the billing firm for 10 days, resulting in a week and a half of claims submitted that deny for "provider not credentialed." Our integrated credentialing services and billing operations eliminate that gap entirely — new providers start billing on their effective date, not 2 weeks later.

Stop Leaving Revenue on the Table
Your practice has already done the hard part — the clinical work is done, the sessions are documented, the hours are logged. The question is whether your billing infrastructure is collecting everything you've earned.
Free audit · No commitment · Results in 48 hours
Common Questions About Mental Health Revenue Cycle Management
What is the mental health revenue cycle?
The mental health revenue cycle is the complete financial process running from a patient's first appointment scheduling through final payment — including insurance verification, authorization, coding, claim submission, denial management, and patient collections. Behavioral health revenue cycles are more complex than general medical because of time-based CPT coding, frequent prior authorizations, behavioral health carve-out networks, and regulatory requirements like 42 CFR Part 2 for SUD services.
What are the 4 Ps of the revenue cycle?
The 4 Ps of the revenue cycle are Patient registration, Payer verification, Processing of claims, and Payment collection. In behavioral health, a fifth P is often added: Prior authorization — because it's foundational to the entire process in a way that doesn't exist in general medicine. Missed authorization is the single largest revenue leak in behavioral health, not a secondary concern.
What are the three pillars of RCM?
The three pillars of revenue cycle management are clean claim submission, denial management, and patient collections. In behavioral health, authorization management functions as an unofficial fourth pillar because everything downstream depends on it — claims cannot pay, denials cannot be avoided, and AR cannot shrink if authorization is not systematically managed from the start.
How do you improve behavioral health revenue cycle management?
The highest-impact starting points are verifying insurance eligibility before every session (not just at intake), working denied claims within 72 hours of receipt rather than letting them age, and incorporating MHPAEA parity arguments in medical necessity appeals. Approximately 63 percent of behavioral health denials are recoverable when properly appealed — practices that systematically work their denial queue add 2 to 4 percentage points to their net collection rate within 90 days.
What causes mental health claim denials?
The most common causes are missing or expired prior authorizations, behavioral health carve-out routing errors (billing commercial parent plan instead of the carve-out), incorrect CPT code selection for session length, eligibility errors from outdated or lapsed patient coverage, and timely filing violations from unsigned notes or submission delays. Together these account for approximately 80 percent of all behavioral health denials.
How long should days in AR be for a mental health practice?
Target Days in AR for outpatient behavioral health practices is 35 days or fewer, with elite practices averaging under 30 days. IOP and PHP programs run slightly higher — 35 to 40 days is the elite benchmark for intensive programs due to concurrent review authorization cycles that build inherent timing delays. Days in AR above 55 for any practice type indicates a systemic denial rate or submission timeliness problem.
What is a good collection rate for a therapy practice?
A strong Net Collection Rate for a therapy practice is 92 percent or above, with top-performing behavioral health practices reaching 95 to 97 percent. The industry average is approximately 91 percent. For a $1.5 million practice, the gap between average and top-quartile performance represents $45,000 to $75,000 in additional annual revenue — without adding a single new patient.
What makes behavioral health billing different?
Behavioral health billing differs from general medical billing primarily because of time-based CPT codes requiring exact duration documentation, weekly or per-session prior authorization requirements, behavioral health carve-out networks that require separate credentialing and billing from the commercial parent plan, 42 CFR Part 2 confidentiality requirements for SUD patients, and MHPAEA parity compliance obligations. These aren't procedural variations — they're structural differences that require specialized expertise.
Frequently Asked Questions About Mental Health Revenue Cycle Management
What is mental health revenue cycle management?
Mental health revenue cycle management (RCM) is the end-to-end financial process used by behavioral health providers to manage the lifecycle of a patient claim — from insurance verification and authorization through coding, submission, denial management, and patient collections. It differs from general medical RCM primarily because of time-based CPT coding, behavioral health carve-out networks, high-frequency prior authorization requirements, and specific regulatory compliance obligations including 42 CFR Part 2 and MHPAEA. Practices with optimized BH RCM typically collect 10 to 20 percent more revenue than those using general medical billing approaches.
What are the 9 stages of mental health revenue cycle management?
The nine stages are: (1) Patient scheduling and demographic capture, (2) Insurance eligibility verification including carve-out identification, (3) Prior authorization management, (4) Patient intake and clinical documentation, (5) Charge capture and CPT/ICD-10 coding, (6) Claim submission through clearinghouse, (7) Payment posting and ERA reconciliation, (8) Denial management and appeals, and (9) Patient collections. Authorization management at Stage 3 and denial management at Stage 8 carry the highest financial stakes — failures at these two stages account for the majority of preventable revenue loss in behavioral health practices.
What KPIs should mental health practices track for revenue cycle?
The nine core behavioral health RCM KPIs are Net Collection Rate (target 95%+), Days in AR (target under 35 for outpatient), Denial Rate (target under 5%), Clean Claim Rate (target 95%+), Authorization Approval Rate (target 90%+ for IOP/PHP), Patient Collection Rate (target 85%+), Appeals Success Rate (target 50%+), 90-day AR Percentage (target under 15%), and Revenue Per Visit (target $135+ for outpatient, $150+ with 90837 and 90785 optimization). These KPIs interact — a high denial rate directly inflates Days in AR, which caps NCR regardless of other performance factors.
What is a behavioral health carve-out and how does it affect RCM?
A behavioral health carve-out is a separate payer network that manages mental health and substance use disorder benefits independently from a commercial insurance plan. Major networks include Optum Behavioral Health (under UHC), Carelon Behavioral Health (under Anthem/BCBS in many states), Magellan Healthcare, and Evernorth (under Cigna). Billing the commercial parent plan instead of the correct carve-out results in systematic denials that typically take 30 to 60 days to surface. Proper management requires identifying carve-out status during eligibility verification and routing claims to the carve-out payer ID, not the commercial plan.
How does 42 CFR Part 2 affect mental health billing?
42 CFR Part 2 requires written patient authorization before any SUD treatment information can be disclosed to payers for billing purposes. Unlike HIPAA, which permits billing under the Treatment, Payment, and Operations exception without separate consent, 42 CFR Part 2 creates a hard stop — practices cannot generate or submit SUD claims until a compliant Release of Information is signed by the patient. Practices treating SUD patients must implement a separate consent workflow or risk federal compliance violations.
What is MHPAEA and how does it help with claim denials?
The Mental Health Parity and Addiction Equity Act requires insurers to apply no more restrictive limits to behavioral health benefits than they apply to equivalent medical and surgical benefits. The 2024 Final Rules strengthened enforcement requirements. In billing practice, MHPAEA creates grounds to appeal denials where payer authorization criteria, medical necessity standards, or session limits are more restrictive for mental health than for comparable medical conditions. Appeals citing MHPAEA parity violations succeed at approximately 1.6 times the rate of standard medical necessity appeals.
What is the difference between IOP and PHP billing?
IOP (Intensive Outpatient Program) billing uses Revenue Code 0905 for psychiatric services or 0906 for SUD services on UB-04 claims, paired with HCPCS code H0015 (one unit per full day of service). IOP requires concurrent review authorization every 7 to 10 days. PHP (Partial Hospitalization Program) uses Revenue Codes 0912 or 0913 on UB-04 claims with Condition Code 41, and provides higher-intensity bundled daily services requiring separate clinical justification for the more intensive designation. Both bill on UB-04 — not CMS-1500 — which requires facility billing expertise absent from most general medical billing operations.
How does outsourcing mental health billing improve revenue cycle performance?
Specialized outsourced behavioral health billing services typically achieve Net Collection Rates of 94 to 97 percent, compared to the 85 to 92 percent average for in-house billing. The performance gap — 5 to 12 percentage points — translates to $50,000 to $80,000 in additional collected revenue per year for a practice generating $1 million in gross billings. Against a typical outsourcing fee of 6 to 9 percent of collections ($60,000 to $90,000), the financial case varies from breakeven to net-positive depending on current in-house performance and practice complexity.
What should I look for in a mental health revenue cycle management company?
Key criteria: behavioral health portfolio concentration above 50 to 70 percent, documented experience with behavioral health carve-out billing (Optum BH, Carelon, Magellan, Evernorth), verified NCR benchmarks for their current BH clients, 42 CFR Part 2 compliance capability for SUD practices, MHPAEA parity argument use in denial appeals, contractual data ownership clauses, and defined transition protocols for in-flight claims. Request references from practices with the same levels of care as yours — outpatient references don't speak to IOP/PHP capability.
What is the average Days in AR for a behavioral health practice?
The national average Days in AR for behavioral health practices is approximately 52 days, significantly higher than the 30 to 45 day average for general medical practices. Top-performing outpatient BH practices achieve under 35 days. IOP and PHP programs should target 35 to 40 days. Days in AR above 60 indicates a systemic problem — typically a high denial rate compounding payment delays across a large percentage of monthly claims.
Can mental health RCM be improved without outsourcing?
Yes — but specific systemic changes are required. Implementing real-time eligibility verification before every appointment (not just new patients), establishing an authorization tracking calendar with 80 percent utilization alerts, conducting biweekly denial triage meetings, and adopting a card-on-file policy for patient collections will together move NCR by 5 to 10 percentage points in most practices within 90 to 180 days. The constraint is bandwidth — these improvements require 10 to 15 hours of consistent weekly administrative attention that practices with small billing teams rarely have available.
What makes behavioral health revenue cycle management harder than general medical RCM?
The core structural differences are: time-based CPT coding requiring exact minute documentation rather than procedure identification; weekly concurrent review authorization for intensive programs rather than one-time pre-procedure authorization; behavioral health carve-out networks requiring separate credentialing and claim routing from parent commercial plans; 42 CFR Part 2 consent requirements creating a pre-billing compliance obligation for SUD services; and MHPAEA parity compliance monitoring that general medical billing teams aren't trained to perform. These aren't minor variations — they require specialized infrastructure, staff training, and compliance protocols that general medical billing operations simply don't have.
Three Things That Determine Whether Your Practice Collects What It's Earned
The practices that consistently collect 94 to 97 percent of earned behavioral health revenue have three things in common that the practices collecting 82 percent do not.
They verify eligibility before every session, not just at intake. They work every denial within 72 hours, not when someone gets around to it. And they know their KPIs — NCR, Days in AR, denial rate, authorization approval rate — because you cannot manage what you cannot measure.
Everything else in this guide is operational detail that supports those three fundamentals. The 9-stage framework, the KPI benchmarks, the revenue leak analysis, the carve-out management protocols — all of it exists in service of those three disciplines, applied consistently, across every session, every claim, every month.
The gap between the industry average and top-quartile performance in behavioral health RCM is not a technology gap or a staffing gap. It's a discipline gap. Practices that execute the fundamentals consistently collect $45,000 to $75,000 more per year in revenue they've already earned. The clinical work is done. The revenue is there. The question is whether the billing system is designed to capture it.
If you want an honest assessment of where your practice stands, our team provides free revenue cycle audits for behavioral health practices — comparing your current NCR, denial rate, and Days in AR against behavioral health-specific benchmarks and identifying the specific gaps. No obligation, no pitch, just the numbers.
Our guide to improving revenue cycle management covers the operational changes that produce the fastest measurable results, and our full revenue cycle management overview maps the complete behavioral health billing landscape for practices at any stage of their RCM maturity.
Stop Leaving Revenue on the Table
Your practice has already done the hard part — the clinical work is done, the sessions are documented, the hours are logged. The question is whether your billing infrastructure is collecting everything you've earned.
Free audit · No commitment · Results in 48 hours

