Telehealth mental health billing is one of the most overlooked revenue drivers in behavioral health practices — and here’s a number that should bother you: the average behavioral health practice has a net collection rate somewhere between 78 and 84 percent. That sounds acceptable until you work out what the remaining 16 to 22 percent actually represents.
For a group practice using telehealth mental health billing, generating $800,000 per year, a net collection rate of 80 percent means $160,000 in earned revenue that never lands. Not because the clinical work wasn’t done. Not because the insurance wouldn’t cover it. Because the billing — the part that turns therapy hours into operating cash — is leaking in places no one is watching closely enough.

Mental health billing services are the specialized infrastructure that closes that gap. They’re not the same as general medical billing. Not even close. Behavioral health has its own CPT codes, its own authorization logic, its own carve-out networks, its own parity compliance landscape, and its own denial patterns. Treating it like routine medical billing is exactly how most practices end up at 80 percent when 95 percent is achievable.
This guide covers everything you need to understand about mental health billing services — what they include, where the revenue leaks are, what the coding actually looks like, and how to evaluate whether your current billing setup is performing or quietly costing you money every month.
Here’s what we’ll cover:
- What mental health billing services include from intake through collections
- Why behavioral health billing fails — the five systemic breakdowns that drain most practices
- The CPT codes, authorization workflows, and denial management tactics that determine your collection rate
- MHPAEA — the parity law most practices never use in their favor
- The KPIs that tell you in 10 minutes whether your billing is working or broken
- How to compare in-house versus outsourced billing honestly, without the sales pitch
Table of Contents
What Telehealth Mental Health Billing Services Actually Include

The phrase “telehealth mental health billing services” gets used loosely, especially in behavioral health telehealth billing environments. Some vendors mean they’ll submit your claims. Some mean they’ll handle your entire revenue cycle from the moment a patient schedules to the moment their final balance is collected. The gap between those two things is enormous — both in complexity and in what it’s worth to your practice.
A real, full-service mental health billing operation covers nine functional stages. Understanding each one matters because revenue can break down at any of them, and most practices don’t know which stages they’re missing until they audit.
Stage 1: Patient scheduling and intake. This is where revenue risk begins, not where people think it does. The intake call establishes the insurance information that determines whether any future billing will work. Collecting incorrect or incomplete insurance data at intake creates downstream failures that are expensive to correct — and often aren’t caught until a claim denies 30 days later. Proper patient scheduling services capture the right information the first time.
Stage 2: Insurance eligibility verification. This step should happen before every single appointment — not just at intake, not just annually. Benefits change. Plans lapse. Deductibles reset in January. A patient whose insurance verified clean at the start of the year may have a completely different benefit structure by March. Professional eligibility verification services catch these changes before the session happens, not after it gets billed and denied.
Stage 3: Prior authorization management. This is arguably the highest-leverage stage in behavioral health billing. Commercial payers require prior authorization for ongoing outpatient therapy and concurrent authorization for intensive levels of care. Miss a concurrent review window for an IOP patient and you lose that week’s revenue — typically $2,000 to $4,000 per patient. The authorization management process must be proactive, tracked by expiration date, and owned by someone who understands behavioral health authorization criteria.
Stage 4: Patient documentation. The clinical note isn’t just a clinical document — it’s the financial record. If the note doesn’t support the code billed, the claim is vulnerable to denial on audit. Patient documentation services ensure records meet payer requirements for the specific codes submitted.
Stage 5: Charge entry and coding. For behavioral health, charge entry requires selecting the correct CPT code based on session type and time, attaching the appropriate diagnosis codes, applying telehealth modifiers if applicable, and ensuring everything is entered accurately in the practice management system before submission. Errors at this stage multiply downstream.
Stage 6: Claim submission. A clean claim goes out correctly formatted, within the payer’s timely filing window, to the right payer entity — which in behavioral health often means a managed behavioral health organization (MBHO) rather than the commercial carrier. This distinction matters. Submitting to the wrong entity is a systemic error that generates denials with misleading reason codes. Professional claim submission services manage this routing correctly.
Stage 7: Payment posting. When payers remit, the payment posting process must accurately record what was paid, what was adjusted, and what balance — if any — transfers to the patient. Errors here create phantom balances, missed underpayments, and incorrect patient statements.
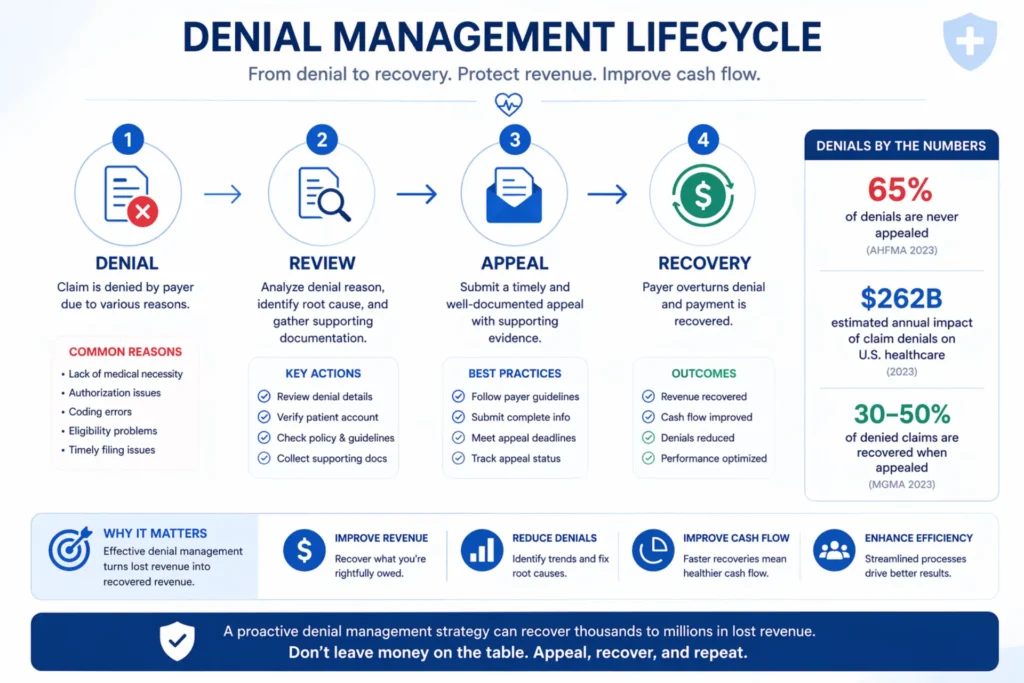
Stage 8: Denial management and AR follow-up. This is where most practices hemorrhage revenue silently. The denial rate for behavioral health claims averages 18 to 22 percent at first submission. Of those denials, an estimated 65 percent are never appealed — they’re just written off. But most behavioral health denials are recoverable. A structured denial management program, combined with aggressive AR follow-up, is where professional billing services prove their value most clearly.
Stage 9: Patient collections and statements. The patient balance — copays, deductibles, coinsurance — is the final piece of the revenue cycle. Patient statement services that communicate clearly, bill promptly, and offer flexible payment options collect more and create less friction than ad-hoc collection processes.
The difference between a practice running all nine stages correctly and one running three or four of them is a 15 to 20 percentage point gap in net collection rate. That gap, for most practices, is tens of thousands of dollars per year.
Not Sure Which of the 9 Stages Is Leaking Your Revenue?
Most practices don’t know their net collection rate, their denial rate, or which stage of the revenue cycle is costing them the most. Our team will benchmark your billing against behavioral health-specific performance standards, identify exactly where revenue is being lost, and show you a clear picture of what better looks like. No charge. No commitment.
Why Behavioral Health Billing Fails — and It’s Not What You Think
When practices have billing problems, the instinct is to look at the billing. Wrong claim format. Wrong codes. Slow submission. Those issues exist, but they’re rarely the primary driver of revenue loss. The bigger problems in behavioral health billing are structural — they’re built into how the practice operates before a single claim goes out.
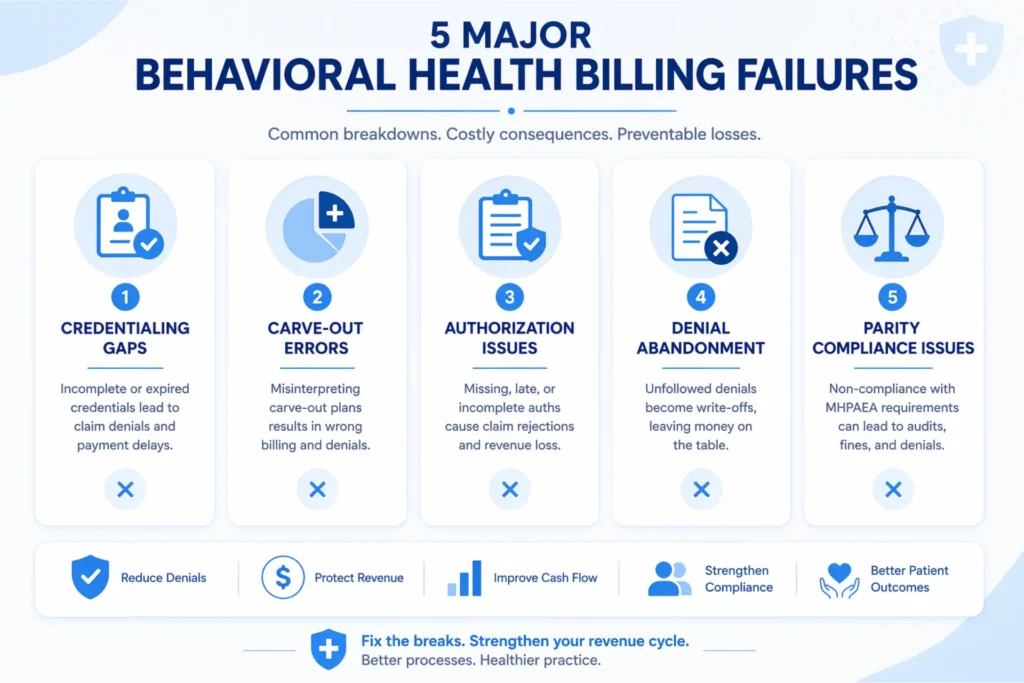
Here are the five breakdowns that drain the most revenue from behavioral health practices.
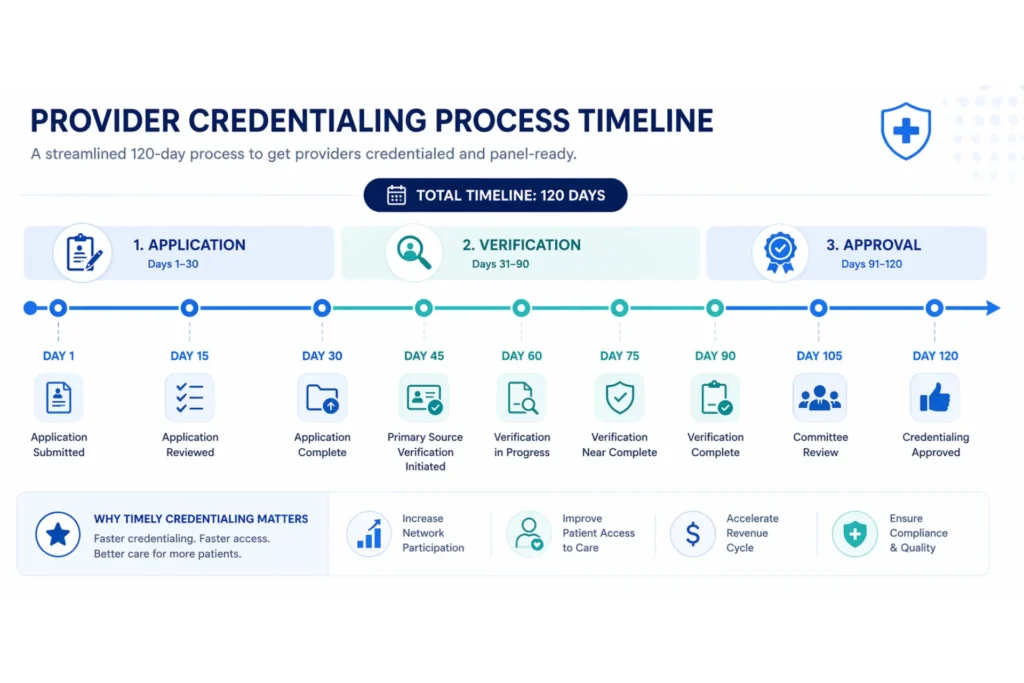
Breakdown 1: Credentialing gaps. A provider who isn’t credentialed with a payer can’t bill that payer for services rendered. That seems obvious. What’s less obvious is the number of practices that have providers seeing patients for 60, 90, or 120 days while their credentialing applications are pending — and submitting claims as if the credentialing is complete. Those claims will ultimately deny or be recoverable only with significant administrative effort. Some will exceed their timely filing window entirely and be unrecoverable. The average commercial credentialing timeline is 90 to 120 days. That timeline needs to be initiated before a provider sees their first patient, not after. Credentialing services that understand behavioral health payer requirements — including the carve-out networks — are a prerequisite for billing, not an afterthought.
Breakdown 2: Carve-out billing errors. Behavioral health carve-out networks are the single most misunderstood billing complexity in this specialty. Many large commercial plans — Anthem, Cigna, UnitedHealthcare — carve out their behavioral health benefits to separate managed behavioral health organizations. Magellan. Beacon (now Carelon Behavioral Health). Optum Behavioral Health. ValueOptions. The commercial plan handles medical. The carve-out handles mental health. If you submit a behavioral health claim to the commercial plan because that’s what’s on the insurance card, it denies. Not because the patient isn’t covered — they are. But because you sent it to the wrong entity. A billing team that doesn’t know to check for carve-outs at eligibility verification will generate months of systematic denials before anyone figures out what’s happening.
Breakdown 3: Authorization gaps and concurrent review failure. Prior authorization is required by most commercial payers for outpatient therapy and is mandatory for intensive services. The authorization process in behavioral health isn’t one-and-done — it requires ongoing management. For IOP programs, concurrent review authorizations typically cover 7 to 10 days of treatment and must be renewed before expiration, often while simultaneously submitting clinical justification documentation for the next period. A practice that doesn’t have a structured authorization tracking system will regularly discover — after billing — that services rendered weren’t authorized, and the window to appeal or request retroactive authorization has closed.
Breakdown 4: Denial abandonment. This is the quietest and most expensive billing problem in behavioral health. The denial comes in. Someone looks at it. It looks complicated. The timely filing window is months away. There’s no one in the office whose job is specifically to work denials. So it sits, ages, and eventually gets written off. In a practice billing $600,000 per year with a 20 percent denial rate, that’s $120,000 in denied claims at first submission. If 65 percent of those denials are never appealed — consistent with behavioral health billing research — that’s $78,000 in recoverable revenue abandoned annually. Denial management isn’t optional. It’s the difference between an 80 percent collection rate and a 94 percent collection rate.
Breakdown 5: MHPAEA compliance failures by payers — and silence from providers. The Mental Health Parity and Addiction Equity Act requires commercial payers to cover mental health and substance use disorder services under the same terms as medical and surgical benefits. In practice, many payers violate this requirement through non-quantitative treatment limitations — stricter prior authorization criteria, lower reimbursement rates, narrower networks, and more aggressive utilization management for behavioral health than for comparable medical services. Most practices don’t know this is happening. And most don’t know that MHPAEA provides a legal basis for appeals that, when filed correctly, have a significantly higher success rate than standard clinical appeals. A billing partner that understands MHPAEA enforcement turns otherwise-unwinnable denials into recoverable revenue.
Mental Health CPT Codes — The Foundation of Every Clean Claim
Telehealth mental health billing starts with CPT codes, especially when using mental health telehealth CPT codes for remote sessions, and if you’re not selecting them with precision, you’re either leaving money behind or creating audit exposure. The behavioral health CPT code set is not complicated — but it’s unforgiving on time documentation, and it has nuances that general medical billers consistently get wrong.
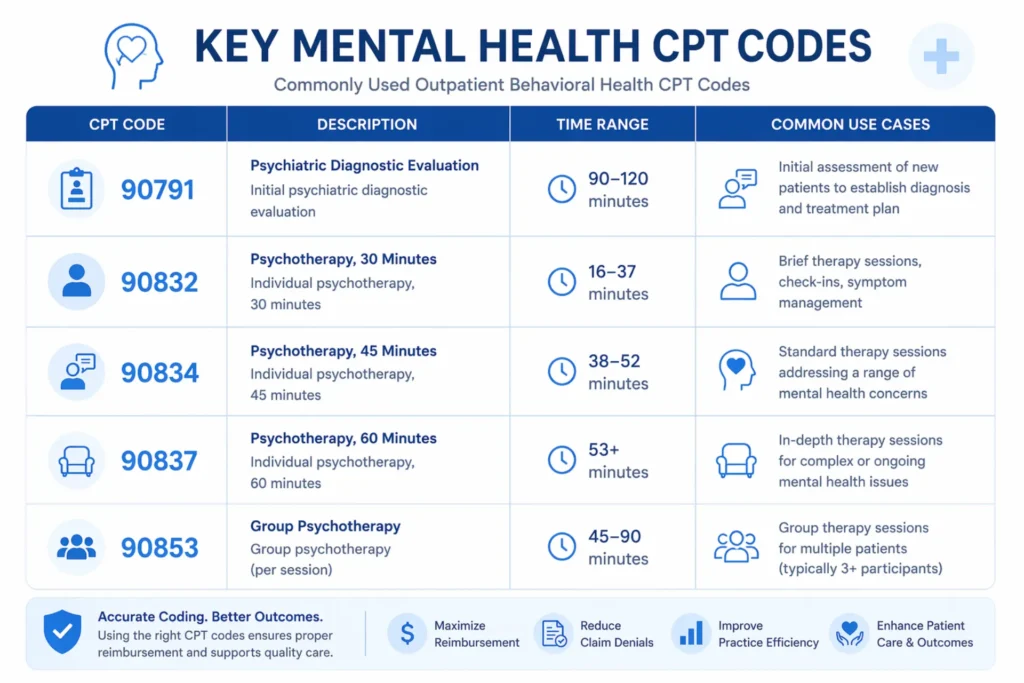
Here’s the core code set that drives the majority of outpatient behavioral health billing:
CPT 90791 — Psychiatric Diagnostic Evaluation. This is the intake assessment — the first clinical encounter where a comprehensive psychiatric evaluation is performed without medical services. It’s untimed, which means it’s not subject to the time-based billing rules that govern the psychotherapy codes. Bill it once for the diagnostic evaluation. It covers the biopsychosocial assessment, mental status, review of diagnostic tests, and treatment recommendations. Commonly billed for new patients. Not appropriate for routine follow-up sessions. Medicare and most commercial payers cover it at rates ranging from $145 to $250 depending on geographic location and payer contract.
CPT 90792 — Psychiatric Diagnostic Evaluation with Medical Services. Same evaluation framework as 90791, but includes a physical exam component, prescription medication coordination, and ordering of diagnostic tests. This code is for prescribers — physicians, nurse practitioners, and physician assistants — not for therapists or counselors. Using 90792 when 90791 is appropriate (or when the provider type doesn’t qualify) creates compliance risk. The distinction matters.
CPT 90832 — Individual Psychotherapy, 30 minutes. Covers sessions in the 16 to 37-minute range. This is where time documentation starts to matter critically. The note must support the time billed. A session documented as “approximately 30 minutes” is not the same as a note that records a start time and end time establishing 22 minutes of face-to-face clinical contact. If your clinical notes don’t have timestamps, you have an audit vulnerability every time you bill 90832. Medicare pays approximately $68 to $85 for this code.
CPT 90834 — Individual Psychotherapy, 45 minutes. Sessions from 38 to 52 minutes. The billing sweet spot for most outpatient therapy sessions. Time documentation applies here with equal rigor. Many providers schedule 45-minute sessions but run long or short — the documentation must match the time range, not the scheduled duration. Medicare reimbursement is approximately $98 to $120.
CPT 90837 — Individual Psychotherapy, 60 minutes. Sessions of 53 minutes or more. This is the highest-value standalone psychotherapy code in routine outpatient billing. Medicare pays approximately $140 to $175 for 90837, depending on location and practice setting (non-facility vs. facility rate). When billing telehealth, the time documentation rules are identical — the platform session start/end time should be in the note. If a patient consistently gets 50-minute sessions and you’re billing 90837, you have both an underdocumentation problem and a upcoding risk.
CPT 90847 — Family Psychotherapy with Patient Present. This code covers family sessions where the identified patient participates. It’s distinct from 90846 (family therapy without the patient present — less commonly covered by commercial payers). 90847 is not time-restricted in the same way as individual psychotherapy codes, though it requires documentation of the family members present and the therapeutic content addressed.
CPT 90853 — Group Psychotherapy. Per-patient billing for group sessions. A group of 8 patients generates 8 claims for a single session. Group billing requires documentation of each participant, the therapeutic modality, and the clinical content. Some payers have group size limits — billing 90853 for a group of 12 when the payer limits reimbursement to groups of 8 creates both a compliance issue and a likely audit trigger.
CPT 90849 — Multiple Family Group Psychotherapy. This code was permanently added to the Medicare telehealth services list in CY 2026, making it billable via telehealth permanently. It covers group sessions attended by multiple patients and their family members simultaneously — common in IOP and PHP settings for family therapy components.
The add-on codes: 90785, 90833, 90836, 90838. Interactive complexity (90785) is an add-on that can be appended to evaluation and psychotherapy codes when specific clinical complexity factors are present — a legally authorized guardian, communication assistance, evidence of a physical or sexual abuse relationship, or restraint or seclusion. It pays $20 to $30 per session when correctly applied and documented. The psychotherapy add-on codes (90833 for 30 minutes, 90836 for 45 minutes, 90838 for 60 minutes) are appended when a prescriber conducts an evaluation and management visit AND provides psychotherapy during the same encounter. These codes are only for medical providers — physicians, NPs, PAs — not for therapists or counselors.
Crisis codes: 90839 and 90840. CPT 90839 covers psychotherapy for crisis situations — the first 60 minutes (actually the 37 to 74-minute range). 90840 is the add-on for each additional 30 minutes of crisis intervention. These are higher-reimbursing codes, but they require specific documentation elements that clinical staff often don’t know: urgent assessment and history, mental status exam, mental health disposition, and implementation of psychotherapeutic interventions. If your staff doesn’t document all those elements, an audit will reduce the claim to a lower-level service.
For practices operating at outpatient, IOP, or PHP levels of care, professional medical coding services that understand behavioral health specificity — time thresholds, add-on code eligibility, facility vs. non-facility rate differences — are not a luxury. They’re a financial necessity.
More detail on behavioral health CPT codes and their documentation requirements: mental health CPT codes guide and mental health billing codes reference.
Is Your Coding Costing You Money on Every Session You Bill?
Undercoding, overcoding, missing add-on codes, incorrect modifier usage, time documentation gaps — these are the quiet revenue leaks that show up in your net collection rate but are nearly impossible to see without a dedicated coding audit. Our behavioral health coding specialists review your current coding patterns against payer benchmarks and identify exactly where you’re losing money per claim.
Audit My Coding — Free →Insurance Credentialing for Mental Health Providers — The Revenue Problem Nobody Discusses
If billing is the engine of a mental health practice’s revenue cycle, credentialing is the ignition. Without it, nothing moves.
Credentialing is the process by which a payer verifies a provider’s qualifications — education, licensure, training, malpractice history, hospital affiliations — and formally enrolls them in the payer’s network. Until that process is complete and the provider has an active contract, claims submitted under their NPI will deny for non-covered services regardless of clinical quality, documentation accuracy, or coding precision.
The timeline problem is what kills practices. Commercial credentialing takes 90 to 120 days. Medicare and Medicaid credentialing can take 60 to 90 days with a functioning enrollment process. A new hire or a practice expansion means 3 to 4 months of revenue either delayed or permanently lost, depending on how the practice handles billing during the pending period.
There are specific approaches that protect revenue during credentialing gaps — billing under a supervising provider during a provisional period, for instance, when state regulations and payer contracts permit it. But these approaches must be managed carefully; incorrect application creates compliance risk that’s worse than the revenue problem it’s solving. Professional credentialing support navigates these situations correctly.
The other credentialing issue specific to behavioral health is carve-out network credentialing. A provider who is credentialed with Anthem BCBS commercial is not automatically credentialed with the Magellan or Beacon network that manages Anthem’s behavioral health benefits. These are separate credentialing processes with separate applications, separate timelines, and separate contract terms. A practice that doesn’t know this will credential providers with the medical plan and then wonder why behavioral health claims deny — because their providers aren’t in the right network.
For practices hiring multiple providers, expanding to new payers, or operating in the group practice model where multiple clinicians share a billing infrastructure, credentialing management is a continuous operational function, not a one-time task. It requires tracking re-credentialing deadlines, managing CAQH profiles, monitoring provider roster changes with payers, and handling any credentialing disputes or re-verification requests that come through. The detail required to get all of this right for mental health credentialing is why most practices that try to manage it in-house eventually lose track of something expensive.
Prior Authorization in Mental Health — The Process That Breaks More Revenue Cycles Than Anything Else
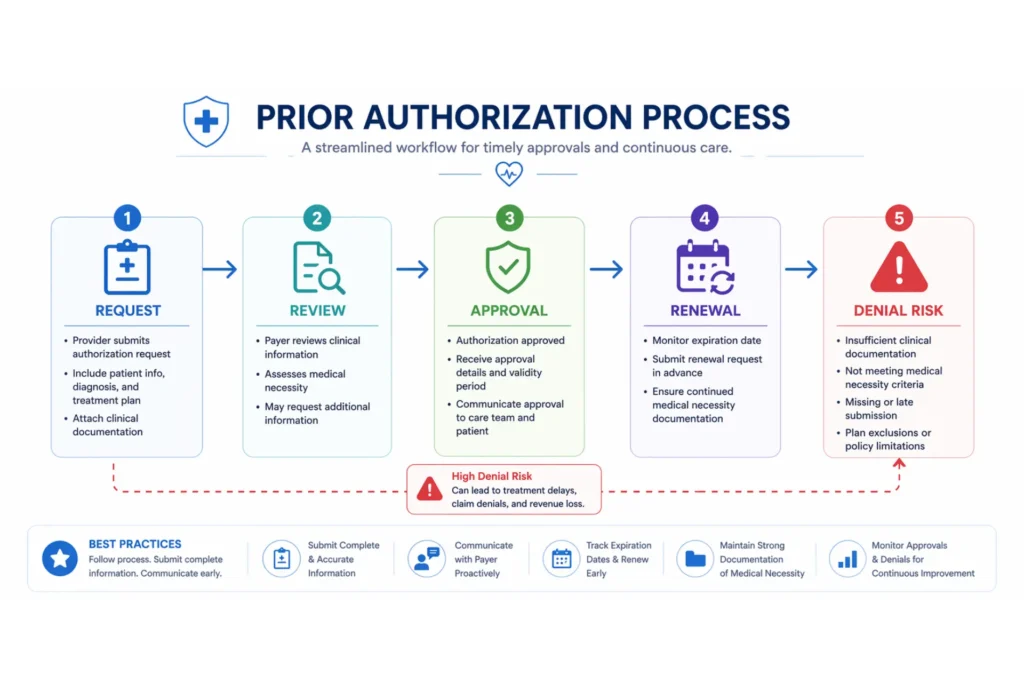
Prior authorization is the formal process of getting payer approval before providing services. In most specialties, it’s manageable. In behavioral health, it’s a near-constant operational burden — and when it breaks, the financial consequences are immediate.
Here’s what makes prior authorization in mental health different from other specialties:
Outpatient therapy authorization. Most commercial payers require prior authorization for outpatient individual therapy, family therapy, and group therapy. Some require authorization from session one. Others allow a limited number of sessions (typically 3 to 8) before authorization is required. The practice must know each payer’s specific authorization trigger and initiate the process proactively — not reactively when a claim denies.
Concurrent authorization for IOP and PHP. For intensive levels of care, authorization isn’t obtained once at admission — it’s renewed continuously throughout the episode of treatment. IOP typically requires concurrent review every 7 days. PHP may require review every 3 to 5 days. Each renewal requires clinical justification documentation demonstrating that the patient continues to meet the medical necessity criteria for that level of care, based on the behavioral health criteria the payer uses (most commonly MCG or InterQual criteria, or the American Association of Addiction Medicine criteria for SUD programs).
Missing a concurrent review window — or submitting for authorization after the authorized period has already ended — results in a retroactive denial that is difficult to overturn. The payer’s position is that services were rendered without active authorization. The practice’s position is that the patient was clinically appropriate and the authorization lapse was administrative. Most payers will reject the appeal on procedural grounds regardless of clinical appropriateness. The only protection is a system that tracks every authorization expiration date and triggers renewal submissions with sufficient lead time.
Single case agreements. When a patient’s treating provider is out of network with their behavioral health payer, single case agreements (SCAs) allow for reimbursement at a negotiated rate for a specific episode of treatment. SCAs are more common than most practices realize — they’re often the answer when a new patient presents with out-of-network behavioral health coverage but limited in-network options. Negotiating SCAs effectively requires knowing the payer’s typical out-of-network rate methodology and making the case for a rate that reflects the provider’s clinical value. This is a specialized skill that general medical billing vendors rarely have.
The authorization management function also intersects with MHPAEA compliance. If a payer applies prior authorization requirements to behavioral health services that are more stringent than their requirements for comparable medical services, that’s a potential parity violation. Building documentation of authorization denial patterns is part of a well-run behavioral health billing operation — not just for appeals, but for potential regulatory complaints if patterns of discriminatory utilization management are identified. More on this in the MHPAEA section below.
For more detail on navigating the full revenue cycle in this context: mental health revenue cycle management and the RCM process guide.
Denial Management in Behavioral Health — Why 65% of Winnable Appeals Never Get Filed
Denial management is the most measurably impactful function in a mental health billing operation, and it’s the one that most practices handle worst.
Here’s the landscape: the average first-pass denial rate for behavioral health claims is 18 to 22 percent. At a practice billing $600,000 annually, that’s $108,000 to $132,000 in denied claims at first submission every year. Research on behavioral health billing shows that approximately 65 percent of those denials are never appealed — they’re reviewed once, judged too complex, and written off. But the reality is that 60 to 80 percent of behavioral health denials are recoverable with the right appeal process.
The math on denial abandonment is sobering. A practice with $120,000 in annual denials, writing off 65 percent, is leaving $78,000 in recoverable revenue on the table every year. That number compounds — it’s $78,000 in year one, $78,000 in year two, and so on, because the systemic issues driving the denials never get identified and fixed if no one is working the appeal queue.
The most common denial types in behavioral health — and the right response to each:
Not medically necessary (CO-50, CO-57). These are the denials that require clinical appeals. The payer’s medical reviewer determined that the documentation doesn’t support the level of care or frequency of service. The winning appeal includes the clinical notes, a peer-to-peer review request when appropriate, and — critically — a MHPAEA argument if the payer is applying medical necessity criteria to behavioral health that it doesn’t apply to comparable medical services.
No authorization on file (CO-15, CO-29). These denials require an administrative response demonstrating that authorization was obtained or that the service falls within a coverage policy that doesn’t require authorization. When authorization genuinely wasn’t obtained, these denials require either a retroactive authorization request or a detailed appeal demonstrating clinical necessity and payer-side procedural issues.
Timely filing (CO-29). Claims submitted outside the payer’s filing window. This is mostly preventable — a well-run billing operation rarely has timely filing denials. When they do occur, the appeal requires documentation of the original submission date and proof that the denial wasn’t received until the filing window had passed. Keep your clearinghouse submission records. They’re your only evidence in a timely filing dispute.
Invalid or missing modifier (CO-4, CO-5). For telehealth billing, wrong place of service codes, missing telehealth modifiers, or incorrect modifier usage. These are straightforward corrected claims — the billing error is fixed and the claim resubmitted.
Coverage terminated (CO-27). Patient wasn’t covered on the date of service. Preventable with proactive eligibility verification. When it does happen, some situations allow retroactive billing to a secondary payer or self-pay conversion with adequate notice to the patient.
Exceeded benefit limits (CO-96). The patient’s plan has a session limit that’s been reached. Before writing these off, check MHPAEA. If the plan covers comparable medical services without a session limit but applies a session limit to behavioral health, that’s a parity violation that can be challenged on appeal.
Structured denial management for behavioral health isn’t just about working the individual denials — it’s about building the data to identify patterns. If 30 percent of denials from a specific payer are “not medically necessary” denials for a specific level of care, that’s either a documentation problem or a payer problem. The analysis tells you which. Fixing the documentation problem requires staff training. Fixing the payer problem requires MHPAEA appeals, peer-to-peer reviews, and sometimes regulatory escalation.
For practices that are not currently running an active denial management program, the first 90 days of working an aged AR typically uncovers three to five times the initial investment in recoverable revenue. We’ve seen practices with $40,000 to $60,000 in recoverable denials sitting in their AR aging reports, untouched, because no one had the time or expertise to work them.
See how improving your revenue cycle management connects directly to denial recovery and long-term collection rate improvement.
MHPAEA — The Parity Law Most Mental Health Practices Never Use
The Mental Health Parity and Addiction Equity Act is one of the most important billing tools in behavioral health, and most practices don’t know it exists as an operational tool — they think of it as a policy concept, not something they can invoke in an appeal.
Here’s the core of it: MHPAEA requires commercial insurance plans that cover mental health and substance use disorder services to provide those benefits at parity with medical and surgical benefits. The law applies to both quantitative limits (like visit limits or day limits) and non-quantitative limits (like prior authorization criteria, reimbursement rate structures, and network adequacy standards).
The non-quantitative treatment limitation (NQTL) provisions are where most parity violations occur — and where most practices have the strongest billing arguments they’re not making.
Consider these scenarios:
A payer requires prior authorization for every behavioral health outpatient therapy session above 10 per year but does not require prior authorization for comparable medical services like ongoing physical therapy or chronic disease management. That’s a potential NQTL parity violation.
A payer applies a session limit of 30 behavioral health visits per year but has no comparable limit on medical visits for ongoing conditions. That’s a quantitative treatment limitation parity violation.
A payer’s behavioral health reimbursement rates are structurally lower than rates for comparable medical services — measured by conversion factor or relative value unit methodology. The 2024 MHPAEA Final Rule strengthened the requirements for comparative analysis of these rates.
When any of these patterns appear in a denial or a payment rate dispute, a MHPAEA-grounded appeal — one that specifically invokes the parity analysis, requests the payer’s comparative analysis documentation, and frames the denial as a potential federal law violation — has a substantially higher success rate than a standard clinical appeal. Payers know the regulatory exposure and respond differently when the MHPAEA framework is invoked correctly.
Building this into your denial management workflow requires a billing partner who understands MHPAEA at an operational level. Most general medical billing vendors don’t. Most in-house billing coordinators don’t. This is one of the areas where specialized behavioral health billing expertise generates measurable financial returns that are difficult to replicate with generalist billing infrastructure.
Related resource: why practices choose to outsource mental health billing and how to choose a mental health billing service.
The KPIs That Tell You Whether Your Mental Health Billing Is Working

You can’t manage what you don’t measure. Most behavioral health practices don’t measure their billing performance with any specificity — they look at deposits in the bank account and make qualitative judgments about whether things are “going well.” That approach makes it nearly impossible to identify where money is being lost or where to focus improvement efforts.
Here are the KPIs that matter in behavioral health billing, what they measure, and what the benchmarks look like:
Net Collection Rate (NCR). The most important number in your revenue cycle. It measures total collections as a percentage of net collectible charges — that is, charges after contractual adjustments. An NCR of 95 percent or higher is excellent. 90 to 94 percent is acceptable. Below 90 percent means money is leaking somewhere and needs to be found. Most practices that don’t have dedicated billing oversight operate in the 78 to 85 percent range. The gap between 80 and 95 percent, for a $500,000 practice, is $75,000 per year.
First-Pass Acceptance Rate (FPAR). The percentage of claims that are accepted and processed by the payer on the first submission without requiring correction or resubmission. A FPAR of 95 percent or higher indicates a clean billing operation. Below 90 percent indicates systemic issues — coding errors, incorrect payer routing, missing modifiers, eligibility problems — that need to be identified and fixed at the source. The FPAR is where you find root causes; the NCR is where you see the financial damage.
Days in AR. The average number of days it takes for a submitted claim to reach payment or final disposition. The behavioral health benchmark is 30 to 40 days. When Days in AR climbs above 50, it typically indicates a backlog in follow-up, slow authorization processes, or systemic denial management problems. Above 60 days is a warning sign. Above 90 days means there are almost certainly large amounts of aging receivables that are at risk of becoming unrecoverable.
Denial Rate by Payer and Denial Type. This is the diagnostic tool that reveals where your billing is breaking. A 5 percent denial rate from one commercial payer and a 28 percent denial rate from another tells you something specific — the second payer has a pattern problem, whether that’s authorization criteria, eligibility issues, network confusion, or coding disagreements. Denial rate by type (clinical vs. administrative vs. eligibility) tells you whether you’re dealing with a documentation problem, a billing operation problem, or a coverage problem.
AR Aging Distribution. What percentage of your total accounts receivable is in each aging bucket — 0 to 30 days, 31 to 60 days, 61 to 90 days, over 90 days. A healthy AR aging distribution should have 80 percent or more of total AR in the 0 to 60-day bucket. When claims age beyond 90 days without being worked, recovery rates drop significantly. Claims beyond 120 days are often unrecoverable due to payer timely filing restrictions on appeals.
Revenue per Provider and per Session. Tracking average collected revenue per session, by provider and by payer, identifies both coding opportunities (a provider consistently billing 90834 when sessions typically run 53+ minutes) and contract value questions (a payer paying 60 percent of what others pay for the same codes).
If you don’t currently have visibility into these numbers, the first step isn’t changing your billing vendor — it’s a billing audit that establishes your baseline. You can’t make evidence-based decisions about billing performance without the data. For a more detailed breakdown of the revenue cycle metrics that matter: healthcare revenue cycle and revenue cycle management overview.
🧮 Mental Health Billing Revenue Calculator
See how much revenue your current billing performance may be costing you annually.
📊 Your Billing Performance Snapshot
* Estimates assume 48 billing weeks per year and a 95% benchmark net collection rate. Actual results depend on payer mix, authorization management, denial recovery, and billing workflow quality.
Get a Free Billing Audit to Recover This Revenue →In-House vs. Outsourced Mental Health Billing — The Honest Comparison
This is the conversation most billing articles handle with a predetermined conclusion. We’re going to try to be honest about it, because the right answer genuinely depends on your practice’s size, your service mix, and your current operational capacity.
Here’s what the real comparison looks like:
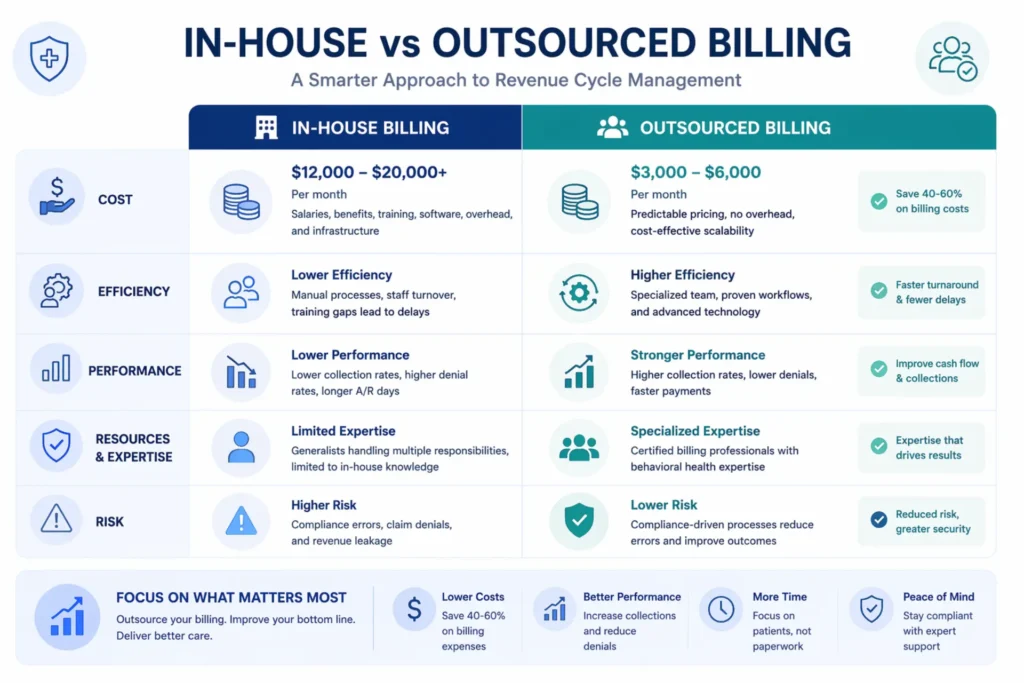
In-house billing costs more than most practices calculate. The common error is comparing only the salary cost of an in-house biller to the percentage fee of an outsourced service. That comparison ignores: payroll taxes (7.65 percent of salary), benefits (insurance, PTO, retirement contributions — typically 25 to 35 percent of salary), EHR and practice management software subscriptions that the biller uses, training and continuing education to keep billing knowledge current, coverage during vacations and illness (mental health billing cannot pause for 2 weeks because someone is on leave), and the management overhead of supervising a billing employee. When you add all of that up for a full-time biller at $48,000 to $55,000 salary, the true cost is typically $70,000 to $80,000 per year. And that assumes competent performance, which isn’t guaranteed.
Outsourced billing typically costs 6 to 10 percent of collections. For a practice collecting $400,000 per year, that’s $24,000 to $40,000 annually — less than a full-time biller’s fully loaded cost. But the percentage model means the billing service has a financial incentive to maximize collections, which aligns with the practice’s interest. The comparison isn’t just cost — it’s cost-adjusted-for-performance. A billing service collecting 94 percent net at 8 percent of collections is worth significantly more than an in-house biller collecting 82 percent with no performance pressure.
Where in-house billing works well: Large organizations (20+ providers) with dedicated billing departments, specialized expertise, and management infrastructure. High-volume practices with simple, uniform service mixes that benefit from standardized workflows. Organizations with existing investment in billing infrastructure, revenue cycle leadership, and billing compliance programs.
Where outsourced billing works better: Solo and group practices below 10 providers. Practices with complex service mixes (IOP/PHP/outpatient combined). Practices entering new payers or expanding to telehealth where specialized expertise matters. Any practice that can’t sustain dedicated billing oversight — where billing is done by a clinical administrator whose primary job isn’t billing. Practices that have chronic AR aging problems or high denial rates and need structural improvement, not just continuation of the current approach.
The hybrid model. Some practices have a front-office person handling intake, scheduling, and eligibility verification, while outsourcing coding, claim submission, denial management, and AR follow-up. This works well when the front-office function genuinely adds value at the patient touchpoint, and the administrative complexity of coding and appeals is managed by specialists. The key is defining responsibilities clearly so nothing falls in the gap between the two.
For a more detailed analysis of this decision: the case for outsourcing mental health billing and what mental health billing services cost.
How to Choose a Mental Health Billing Service — Eight Questions to Ask Before You Sign
Not all mental health billing services are the same. Some are general medical billing vendors with a few behavioral health clients. Some are behavioral health specialists who understand every nuance of the codes, authorizations, carve-outs, and parity landscape. The difference between those two categories is measurable in your monthly collection rate.
Here are the eight questions that will reveal which category you’re dealing with:
1. What percentage of your clients are behavioral health practices? If the answer is less than 50 percent, you’re looking at a general medical biller with some behavioral health exposure. That’s not the same as a specialist. Behavioral health billing requires sustained focus on a set of payer relationships, authorization patterns, and coding rules that are different from every other specialty. Part-time expertise produces part-time results.
2. How do you handle carve-out billing? The right answer involves a specific description of how the vendor identifies carve-out plans at eligibility verification, which managed behavioral health organizations they’re experienced with (Magellan, Beacon/Carelon, Optum Behavioral Health, ValueOptions/Carelon), and what their process is for submitting to the correct entity. If the person you’re talking to doesn’t know what a carve-out is, end the conversation.
3. What is your average net collection rate for behavioral health clients? Ask for a specific number, not a range. Ask for it broken down by service type if you offer both outpatient and IOP/PHP. A vendor that can’t answer this question with specificity either isn’t tracking it or isn’t proud of the answer. Acceptable net collection rate for behavioral health with good billing management is 93 to 96 percent. Below 90 percent is a problem.
4. How do you manage prior authorization and concurrent review? The answer should describe a specific tracking system — not a spreadsheet, not “we handle it manually,” but an actual authorization management workflow with expiration tracking and proactive renewal triggers. For IOP and PHP programs, ask specifically how they manage concurrent review timelines and what their process is when authorization is at risk of lapsing.
5. What is your denial appeal process? The answer should describe how denied claims are categorized by denial type, what the escalation path looks like for clinical denials (including peer-to-peer reviews), and whether they use MHPAEA arguments in behavioral health appeals. If MHPAEA isn’t part of their appeal toolkit, they’re leaving winnable cases on the table.
6. What billing software and clearinghouse do you use? The answer tells you something about their infrastructure investment and their ability to integrate with your existing practice management system. Ask about their compatibility with your EHR before discussing anything else.
7. What does your reporting look like? You should receive regular reports showing NCR, FPAR, Days in AR, denial rates by payer and type, and AR aging distribution. If a billing service can’t produce these reports — or if they’re only willing to share “deposit activity” — they don’t have the data infrastructure to manage your billing effectively or the transparency to demonstrate performance.
8. What are your contract terms and what happens to my AR if I leave? This is the question most practices forget to ask before they sign. Some billing vendors retain control of your AR data, charge transition fees, or continue billing your claims during an extended notice period that creates cash flow complications. Know the exit terms before you’re in the contract.
For more guidance on evaluating billing vendors: how to choose a mental health billing service and the complete beginner’s guide to mental health billing.
Mental Health Billing for Specific Practice Types — What Changes by Setting
The core billing principles apply across all behavioral health settings, but the execution details vary significantly by practice type. Here’s what changes for the most common settings:
Solo outpatient therapist. The primary billing challenges are insurance credentialing (which payers to credential with and when), carve-out identification at eligibility verification, and denial management for the inevitable authorization and medical necessity denials. The volume is manageable — typically 15 to 30 sessions per week — but the administrative burden of managing it well alongside clinical work is real. Most solo therapists either underperform on billing because they’re managing it themselves or overpay for underdifferentiated billing services that don’t understand behavioral health specifics. The economic case for specialized outsourced billing at a percentage of collections is strong for solo providers.
Group practice (5–20 therapists). Multiple provider credentialing management becomes a significant operational function. Different providers may be credentialed with different payer panels, creating complex routing requirements for eligibility verification and claim submission. Telehealth billing across state lines adds licensure and payer enrollment complexity. Performance tracking by provider — which clinicians are getting clean claims versus generating denial patterns — becomes important for both billing optimization and provider management. An integrated RCM services approach that manages credentialing, billing, and reporting for the full provider panel is the standard infrastructure for group practices at this scale.
IOP and PHP programs. The most complex billing environment in behavioral health. Revenue codes, UB-04 billing, concurrent authorization management, medical necessity documentation for level-of-care criteria, utilization management interactions, and mixed-payer environments where some patients have commercial coverage, some have Medicaid managed care, and some have Medicare or dual eligibility. The average IOP program operating without specialized behavioral health billing loses 20 to 30 percent of collectible revenue to authorization gaps, incorrect revenue codes, and abandoned clinical denials. This is also the setting where MHPAEA parity arguments have the highest dollar value — a wrongly denied high-deductible commercial authorization for a week of IOP is $4,000 to $6,000 per patient.
Telehealth-only or hybrid practices. The telehealth mental health billing 2026 landscape for behavioral health has changed significantly, especially in behavioral health telehealth billing workflows — Medicare extended through December 31, 2027, audio-only permitted for any reason through 2027, the in-person requirement waived through January 2028 — creates specific billing requirements. Place of service codes (POS 10 for patient at home, paying the higher non-facility rate), telehealth modifiers behavioral health such as modifier 95 for audio-video and modifier 93 for audio-only, and documentation of patient location in clinical notes are all telehealth-specific billing requirements. A billing team that understands the post-Consolidated Appropriations Act 2026 landscape captures the full non-facility rate differential. One that doesn’t may be billing POS 02 (facility rate, lower) when POS 10 (non-facility rate, higher) is appropriate.
Telehealth mental health billing has become a permanent part of behavioral healthcare delivery in 2026. Practices that optimize behavioral health telehealth billing, use the correct mental health telehealth CPT codes, and apply proper telehealth modifiers behavioral health are consistently outperforming those using outdated billing workflows.

You’ve Already Done the Hard Work.
Let’s Make Sure You Get Paid for It.
You’ve built the practice. You’ve seen the patients. You’ve written the notes. The question is whether your billing infrastructure is collecting everything your clinical work has earned — or quietly leaving 15 to 25 percent on the table every single month.
Free audit · No commitment · Results in 48 hours
Frequently Asked Questions About Mental Health Billing Services
What do mental health billing services typically cost?
Mental health billing services typically charge between 6 and 10 percent of collections, though some vendors use flat monthly fees for lower-volume practices. The percentage model aligns the billing service’s financial incentive with yours — they collect more only when you collect more. At 8 percent of a $400,000 practice, that’s $32,000 per year, which compares favorably to the fully loaded cost of an in-house biller ($70,000 to $80,000 per year including taxes, benefits, and overhead). More detail: mental health billing services cost guide.
What is the difference between mental health billing and general medical billing?
Mental health billing uses time-based CPT codes that require documented session duration for accurate coding, while general medical billing is primarily procedure-based. Behavioral health has its own managed care carve-out network structure (Magellan, Beacon/Carelon, Optum Behavioral Health), which general medical billers frequently don’t understand. Prior authorization in mental health requires concurrent review management for intensive services — a cycle that doesn’t exist in most medical specialties. Denial management in behavioral health includes MHPAEA parity arguments that are irrelevant in medical billing. The specialties require different training, different payer relationship knowledge, and different workflows.
How do I know if my current billing is performing well?
Measure your net collection rate (NCR), first-pass acceptance rate (FPAR), and Days in AR. An NCR above 93 percent, FPAR above 95 percent, and Days in AR below 40 days indicate a performing billing operation. If your NCR is below 90 percent, your denial rate is above 15 percent, or you have significant AR aging beyond 90 days, your billing has revenue leaks that need to be identified and corrected. A billing audit can establish your baseline and identify exactly where money is being lost.
What is a carve-out in behavioral health billing, and why does it matter?
A behavioral health carve-out is an arrangement where a commercial insurance plan contracts with a separate managed behavioral health organization (MBHO) to administer mental health and substance use disorder benefits. Common MBHOs include Magellan, Beacon Health Options (now Carelon Behavioral Health), Optum Behavioral Health, and ValueOptions. When you bill a behavioral health claim for a carve-out patient, the claim must go to the MBHO — not to the commercial carrier. Submitting to the commercial carrier generates a denial that looks like a benefits issue but is actually a routing issue. Identifying carve-outs at eligibility verification and routing claims correctly is a core behavioral health billing skill.
How long does insurance credentialing take for mental health providers?
Commercial insurance credentialing typically takes 90 to 120 days. Medicare and Medicaid credentialing can take 60 to 90 days with a complete, accurately submitted application. Behavioral health carve-out credentialing (with Magellan, Beacon, Optum Behavioral Health) is a separate process from commercial plan credentialing and has its own timeline. Providers should begin credentialing applications at least 90 days before their first patient date, and billing infrastructure should be designed to handle the provisional period appropriately.
Can I use the same billing service for telehealth and in-person sessions?
Yes — but make sure your billing service understands the telehealth-specific billing requirements: place of service code selection (POS 10 for patient at home pays the higher non-facility rate; POS 02 for patient not at home pays the facility rate), modifier selection (modifier 95 for audio-video, modifier 93 for audio-only when patient can’t use or declines video), and documentation requirements (patient location must be in the clinical note). The Consolidated Appropriations Act, 2026 extended Medicare telehealth through December 31, 2027, making telehealth billing a long-term operational function rather than a temporary pandemic accommodation.
What is MHPAEA, and how does it affect billing?
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires commercial insurance plans to cover mental health and substance use disorder services at parity with medical and surgical benefits. In billing, this matters most in denial management — when a payer denies a behavioral health service based on criteria it doesn’t apply to comparable medical services, that’s a potential parity violation that can be used as a basis for appeal. MHPAEA-grounded appeals, particularly for prior authorization denials and session limit denials, have higher success rates than standard clinical appeals because they invoke a federal legal requirement, not just clinical preference.
What happens if a prior authorization expires before I submit for renewal?
If services are rendered after an authorization expires and before a new authorization is obtained, the claims for those services will typically deny for “no authorization on file.” Recovery options depend on the payer and how quickly the lapse is discovered — some payers permit retroactive authorization requests within a limited window (typically 24 to 72 hours for urgent clinical circumstances). Most do not. The best protection is a prospective authorization tracking system that flags renewals at least 5 to 7 days before expiration and prioritizes renewal submissions for high-census IOP and PHP programs where authorization gaps carry the highest dollar risk.
How does denial management work in behavioral health billing?
Denial management involves identifying, categorizing, and appealing denied claims. In behavioral health, the process starts with denial intake — sorting denials by type (medical necessity, authorization, eligibility, coding, timely filing). Clinical denials are escalated for peer-to-peer review requests and MHPAEA analysis when applicable. Administrative denials are corrected and resubmitted. Denials are tracked by payer and denial type to identify patterns that indicate systemic issues — a documentation training problem, a payer-specific coverage dispute, or a billing workflow error. A structured denial management program should recover 60 to 80 percent of first-pass denied claims.
Is outsourcing mental health billing HIPAA-compliant?
Yes, provided the billing vendor executes a properly structured Business Associate Agreement (BAA) with your practice before accessing any protected health information. The BAA documents the vendor’s obligations for handling PHI under HIPAA — safeguards, breach notification, permitted uses, and patient rights. A reputable mental health billing service will have a standard BAA and will execute it before any data sharing occurs. This is a basic compliance requirement; if a vendor doesn’t proactively provide a BAA, consider it a disqualifying omission.
What mental health billing services does Elite Med Financials provide?
Elite Med Financials provides comprehensive mental health billing services including insurance credentialing, eligibility verification, prior authorization management, medical coding, claim submission, payment posting, denial management, and AR follow-up. We specialize in behavioral health — outpatient practices, IOP programs, PHP facilities, SUD treatment centers, and community mental health organizations. We operate in all 50 states, handle behavioral health carve-out billing, and use MHPAEA arguments in denial management when applicable. Our services are available at mental health billing services.
What should I ask a mental health billing vendor before signing a contract?
The eight most important questions: (1) What percentage of your clients are behavioral health practices? (2) How do you handle carve-out billing? (3) What is your average net collection rate for behavioral health clients? (4) How do you manage prior authorization and concurrent review? (5) What is your denial appeal process, including MHPAEA? (6) What billing software and clearinghouse do you use? (7) What regular reporting do you provide, and what metrics does it include? (8) What are your contract terms and what happens to my AR if I switch providers? Detailed guidance at: how to choose a mental health billing service.
Questions and Answers
What are mental health billing services?
Mental health billing services are specialized billing operations that manage the entire revenue cycle for behavioral health practices — from verifying insurance eligibility before the first session to collecting the final patient balance after the last. They handle CPT coding for therapy sessions, prior authorization management, claim submission to commercial insurers and their managed behavioral health carve-outs, denial management, and AR follow-up. Unlike general medical billing, they understand the time-based coding rules, authorization cycles, carve-out network structures, and parity law requirements that are unique to behavioral health.
How much do mental health billing services cost?
Mental health billing services typically cost between 6 and 10 percent of collections, with most behavioral health specialists charging 7 to 8 percent. For a practice collecting $400,000 per year, that’s $28,000 to $32,000 annually. That compares favorably to the fully loaded cost of an in-house biller, which typically runs $70,000 to $80,000 per year once you include salary, taxes, benefits, and software. The percentage model also aligns the billing service’s incentive with the practice’s — they collect more when you collect more.
What CPT codes are used for mental health billing?
The core mental health CPT codes are 90791 for psychiatric diagnostic evaluations, 90832 for 30-minute psychotherapy, 90834 for 45-minute psychotherapy, 90837 for 60-minute psychotherapy, 90847 for family therapy with the patient present, 90853 for group therapy, and 90849 for multiple-family group psychotherapy. Add-on codes include 90785 for interactive complexity and the prescriber-only codes 90833, 90836, and 90838. The psychotherapy codes are time-based — the session duration must be documented in the clinical note to support the code billed.
What is a behavioral health carve-out?
A behavioral health carve-out is an arrangement where a commercial insurance plan delegates its mental health and substance use disorder benefit management to a separate company called a managed behavioral health organization. Common ones include Magellan, Beacon Health Options (now Carelon Behavioral Health), Optum Behavioral Health, and ValueOptions. When patients have carve-out plans, mental health claims must go to the carve-out organization, not to the commercial carrier. Billing to the wrong entity causes denials that look like coverage issues but are actually routing errors.
How long does mental health credentialing take?
Mental health credentialing with commercial payers typically takes 90 to 120 days. Medicare enrollment generally takes 60 to 90 days with a complete application. Credentialing with behavioral health carve-out networks — Magellan, Beacon, Optum Behavioral Health — is a separate process with its own timeline. Providers should begin credentialing at least 90 days before seeing their first insured patient, and practices should have a billing plan for the credentialing period to manage claims appropriately during the waiting period.
Can telehealth mental health billing be used for therapy sessions?
Yes — mental health telehealth billing uses the same CPT codes as in-person sessions, paired with the appropriate telehealth modifier and place of service code. For audio-video sessions, use modifier 95. For audio-only sessions when the patient can’t use or declines video, use modifier 93. Use place of service code 10 when the patient is at home — this pays the higher non-facility rate for most mental health codes — and POS 02 when the patient is at another location. Medicare coverage for behavioral health telehealth is extended through December 31, 2027.
What is the average net collection rate for mental health practices?
The average net collection rate for behavioral health practices falls between 78 and 84 percent, based on industry data from behavioral health billing surveys. Practices with dedicated, specialized mental health billing services typically achieve net collection rates of 93 to 96 percent. The difference between 80 and 95 percent, for a practice collecting $500,000 per year, is $75,000 in additional annual revenue — without seeing a single additional patient.
What is MHPAEA and why does it matter for mental health billing?
The Mental Health Parity and Addiction Equity Act requires commercial insurance plans to cover mental health and substance use disorder services under the same terms as medical and surgical benefits. In billing, it provides a legal basis for appealing denials when a payer applies stricter authorization criteria, lower reimbursement rates, or tighter treatment limits to behavioral health services than it applies to comparable medical services. A well-executed MHPAEA appeal has a higher success rate than a standard clinical appeal, making it a practical billing tool — not just a policy concept.

Conclusion
Telehealth mental health billing is not general medical billing — especially in behavioral health, where complexity is significantly higher with different codes. It has its own complexity — carve-out networks, time-based coding rules, concurrent authorization management, MHPAEA parity enforcement, and denial patterns that require behavioral health expertise to address effectively. The practices that treat it accordingly — with specialized billing infrastructure, active denial management, credentialing oversight, and real performance tracking — collect what they earn. The ones that treat it as a generic administrative function leave 15 to 25 percent of earned revenue uncollected, year after year, without knowing exactly why.
Three things to take from this guide:
First, measure your baseline. If you don’t know your net collection rate, your first-pass acceptance rate, and your Days in AR, you can’t manage your billing performance. Pull those numbers. Compare them to the benchmarks in this guide. The gap tells you what your billing is worth fixing.
Second, identify your highest-cost leaks. Most practices have two or three systemic issues driving most of their revenue loss. Carve-out routing errors, authorization management gaps, and denial abandonment are the most common. Fixing those three problems closes the majority of the collection gap for most practices.
Third, match your billing infrastructure to your specialty. If you’re using a general medical biller or managing billing internally with a clinical coordinator whose primary job isn’t billing, you’re operating with the wrong infrastructure for the complexity of behavioral health. The cost of specialized billing support is almost always less than the revenue it recovers.
Elite Med Financials specializes in mental health billing across all service settings and all 50 states — outpatient, IOP, PHP, SUD, CMHC, solo through group. We handle credentialing, billing, denial management, and AR follow-up with behavioral health expertise that general vendors don’t have. If you want to know exactly how much your current billing is leaving on the table, we’ll run a free audit against behavioral health benchmarks — no charge, no obligation.
You’ve Already Done the Hard Work.
Let’s Make Sure You Get Paid for It.
You’ve built the practice. You’ve seen the patients. You’ve written the notes. The question is whether your billing infrastructure is collecting everything your clinical work has earned — or quietly leaving 15 to 25 percent on the table every single month.
Free audit · No commitment · Results in 48 hours