A licensed therapist sees 25 patients a week at $150 per session. That’s $3,750 every week — but only when she can actually bill insurance for those sessions. When she opens her new practice and applies to payers without a clear plan, she waits 90 to 120 days for credentialing approval while the clock keeps running. By the time her first effective date arrives, she has deferred $45,000 in revenue she will never recover. Nobody told her how long the process would take, which payers she was missing, or that submitting to the commercial plan wasn’t enough — she also needed a separate application for the behavioral health carve-out running underneath it.
This guide exists so that doesn’t happen to you. Whether you’re a solo therapist starting your first practice, a group practice adding providers, or a practice manager tracking 15 pending applications, understanding the best credentialing services for mental health — and the full process behind them — is what we cover here from start to finish.
What is mental health provider credentialing? It is the insurance verification process where a payer reviews your license, education, malpractice history, and professional background to confirm you meet their standards for in-network reimbursement. Credentialing typically takes 90 to 120 days, requires 15 to 25 documents depending on the payer, and must be completed separately for each insurance company. It is the gate between seeing patients and billing insurance — and nothing else in your revenue cycle works until it’s done.
Here is what this article covers:
- The complete 8-step credentialing process with a week-by-week 90-day timeline
- A 20-plus document checklist organized by category, including what Medicare actually requires
- Payer-by-payer guidance covering Medicare, Medicaid, commercial insurers, behavioral health carve-out networks, and TRICARE — the section no competitor publishes
Table of Contents
What Is Mental Health Provider Credentialing?
Credentialing, paneling, contracting, and enrollment get used interchangeably in therapy forums and practice management groups. They mean completely different things, and mixing them up is one of the most common reasons practice owners enter the process with the wrong expectations and wrong timelines.
Credentialing is the verification process. The payer confirms your license is real, your education is what you claim, your malpractice history is disclosed, and your references check out. Think of it as the background check every provider must pass before anything else happens.
Paneling is the result of successful credentialing. When you are paneled with a payer, you are listed in their directory as an in-network provider. Patients with that insurance can find you and use their benefits to see you.
Contracting happens after credentialing clears review. The payer sends a participating provider agreement that defines your reimbursement rates, billing rules, and obligations. You do not get paid until you sign.
Enrollment is the administrative activation — your billing information goes live in the payer’s system and claims can be submitted and paid.
Behavioral health credentialing differs from general medical credentialing in one critical way that most general guides miss: many commercial plans manage mental health benefits through separate behavioral health carve-out networks. Being credentialed with Aetna does not automatically enroll you in the Evernorth behavioral health network running underneath it. Being credentialed with UnitedHealthcare does not automatically enroll you in Optum Behavioral Health. These require separate applications, separate timelines, and separate contracts — and missing them is how providers end up with denied claims they thought would be covered.
The other meaningful difference is timeline. General medical providers average 60 to 90 days for credentialing. Behavioral health providers average 90 to 120 days for commercial payers and 120 to 180 days for carve-out networks. The system is slower, more fragmented, and more payer-specific. Understanding your healthcare revenue cycle as a behavioral health provider means accepting that credentialing is your first and most time-sensitive revenue cycle function — the one that determines whether every other billing step can proceed.
| Provider Type | License Required | Credentials Independently | Key Payer Notes |
|---|---|---|---|
| Psychiatrist (MD, DO) | Medical license + DEA | Yes | Highest reimbursement; medical board oversight; prescribing covered |
| Psychologist (PhD, PsyD) | Doctoral degree + state license | Yes | May require testing certifications for specialty payers |
| LCSW / LICSW | Master’s + full clinical license | Yes | Broad acceptance across commercial payers; independent licensure typically required |
| LPC / LCPC / LMHC | Master’s + clinical license | Yes | Medicare eligible since January 2024; state licensure variations apply |
| LMFT | Master’s + clinical license | Yes | Medicare eligible since January 2024; PECOS enrollment now required |
| PMHNP | Advanced nursing + ARNP license | Yes (supervision required in some states) | Collaborating physician agreement may be required depending on state |
| BCBA | Master’s + national certification | Yes | Limited to autism and behavioral sub-panels; certification prioritized |
| LPC-Associate / LCSW-Associate | Supervised hours + state registration | Usually not independently | May qualify under supervision for Medicaid or select commercial plans |
As of 2026, only 55 to 60 percent of behavioral health providers are in-network compared to approximately 90 percent of primary care physicians. That gap exists partly because of how difficult behavioral health credentialing is to navigate. Over 137 million Americans live in designated Mental Health Professional Shortage Areas according to HRSA 2024-2025 data. Getting credentialed is not just a revenue decision — it is how therapists become accessible to patients who need them.
Why Credentialing Is Essential — The Revenue Cost of Delays
Let’s run the honest math that most practice management guides avoid.
A therapist with a full caseload sees 25 patients per week at an average in-network reimbursement of $150 per session. That is $3,750 per week, $16,250 per month. A 90-day credentialing delay defers $45,000 in revenue. A 120-day delay pushes that to $60,000. Most commercial payers explicitly prohibit retroactive billing before the effective date — which means that revenue is not delayed, it is permanently gone.
Some Medicaid programs allow retroactive billing with a 90-day window. Blue Cross Blue Shield plans allow backdating in select states. But Aetna, Cigna, and UnitedHealthcare will not reimburse services rendered before your effective date. The revenue lost during a credentialing delay is largely unrecoverable, which makes starting early and executing the process correctly the single most important financial decision a new practice makes.
| Practice Size | Monthly Revenue per Provider | 90-Day Delay Loss | 120-Day Delay Loss | Recovery Options |
|---|---|---|---|---|
| Solo therapist (20 sessions/week) | $12,000 | $36,000 | $48,000 | Medicaid retroactive (90 days); provisional for select plans |
| Solo therapist (25 sessions/week) | $16,250 | $48,750 | $65,000 | Limited — most commercial payers deny retroactive claims |
| Small group (3 providers) | $48,750 combined | $146,250 | $195,000 | NPI Type 2 concurrent credentialing for new hires reduces compounding delays |
| Mid-size practice (8 providers) | $130,000 combined | $390,000 | $520,000 | Credentialing service with guaranteed timeline; staggered provider start dates |
Beyond the direct revenue loss, there is the directory effect. Over 78 percent of insured patients in 2025 began their provider search inside the payer’s online directory. If you are not credentialed, you do not appear. Every week you spend outside the network is a week competitors — other in-network providers in your area — are receiving the referrals that could be coming to you.
The Mental Health Parity and Addiction Equity Act, significantly strengthened by the 2024 Final Rules, changed the landscape further. Payers are now under regulatory pressure to demonstrate network adequacy for behavioral health. That means more open panels, more urgency to fill in-network slots, and more reason to credential now rather than wait. HRSA data consistently shows over 137 million Americans in shortage areas. Credentialing is how you serve those patients and get paid for it.
Our mental health billing services begin the moment your effective date is confirmed — so the transition from credentialing to active billing happens in days, not weeks.
FREE CREDENTIALING CONSULTATION
Stop Losing Revenue to Credentialing Delays — We Handle Everything
Elite Med Financials handles your credentialing AND billing together — so when your effective date arrives, your first claims go out the same day. No missed carve-out networks. No CAQH lapses. No billing gaps.
Serving mental health practices in all 50 states. Behavioral health specialists. No hidden fees.
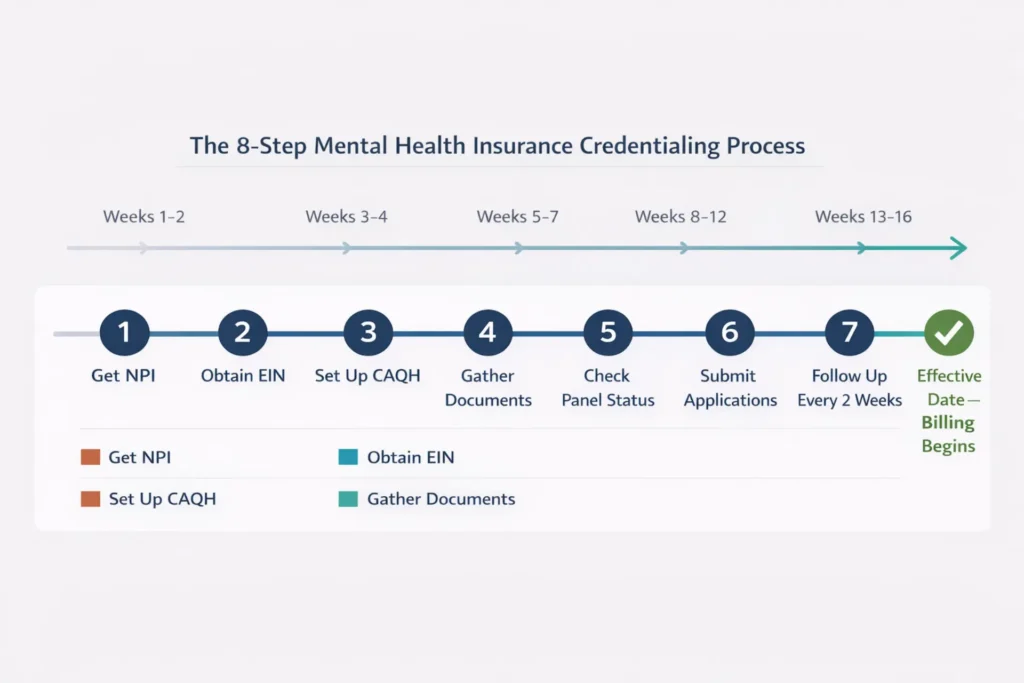
The Mental Health Credentialing Process Step by Step
How do I get credentialed with insurance as a therapist? The full process has 8 steps, runs 90 to 120 days, and begins several weeks before you submit your first application. Here is exactly what that looks like, with realistic timing at every stage.
Step 1: Obtain Your NPI
Your National Provider Identifier is your permanent identifier in the healthcare billing system. Apply for NPI Type 1 (individual) at npiregistry.cms.hhs.gov — it takes 1 to 20 days and is free. If you are billing as a group practice, you also need NPI Type 2 (organizational). Using the wrong NPI type on an application triggers claim denials post-approval and requires a correction process that adds 60 days. When you apply, select the correct taxonomy code — LPC and LMHC providers use 101YP2500X, LCSWs use 1041C0700X, LMFTs use 106H00000X, psychologists use 103TC0700X, and psychiatrists use 2084P0800X. An incorrect taxonomy code causes applications to pend for manual review and adds weeks to your timeline.
Step 2: Obtain an EIN
Your Employer Identification Number from the IRS protects your Social Security Number from appearing on superbills and claim forms. Apply at IRS.gov — it is instant and free. Always use your EIN, not your SSN, on every application and document. Using SSN on a group practice application triggers a 30 to 60 day restart when the error is caught.
Step 3: Set Up Your CAQH ProView Profile
CAQH ProView at proview.caqh.org is the centralized credentialing database that over 90 percent of commercial payers use to verify your qualifications. You upload your licenses, malpractice documentation, CV, and other credentials once, then authorize each payer to access your profile. Initial setup takes 4 to 8 hours. The critical requirement most providers miss: you must attest — confirm your data is current — every 90 days. If your attestation expires while applications are in review, payers stop pulling your data and your applications automatically pause. This single oversight accounts for the majority of credentialing delays we see, adding 30 to 60 days to timelines that were otherwise on track.
Step 4: Gather Your Documents
See the complete checklist in the next section. At minimum, have your state license, malpractice face sheet, CV, W-9, EIN confirmation, graduate transcripts or diploma, government ID, and three professional references — all in PDF format — before submitting any application. Submitting an incomplete application is worse than submitting no application, because the pender sits in a queue waiting for missing items while your timeline continues running.
Step 5: Research Payer Panels
Before spending 4 hours on an application, verify whether the panel is open. Call the payer’s provider relations line or check Availity for Aetna and BCBS, Provider Express for UHC, or CignaforHCP for Cigna. Applying to a closed panel wastes 30 to 60 days before you receive a rejection. More importantly, identify whether you need a separate behavioral health carve-out application — this is where most mental health providers lose billing access without knowing why, and it is covered in full detail in the payer section below.
Step 6: Submit Applications
Budget 2 to 6 hours per payer application. Submit through payer portals directly rather than mailing paper applications where possible. Some payers including UHC and Humana require a Letter of Interest before they will accept a formal application — call provider relations first to confirm their current intake process. Apply to 3 to 5 payers simultaneously rather than sequentially. Waiting for one payer’s approval before starting the next adds months to your overall timeline.
Step 7: Follow Up Every 10 to 14 Days
This is where most applications die. Practices that follow up biweekly reduce their credentialing timelines by 30 to 50 days. Every time you call, get a reference number, write down the representative’s name, and document what they told you. Escalate to a supervisor after 60 days with no status change. Escalate to the credentialing director after 90 days. Escalate to the state insurance commissioner after 120 days. You have more leverage than most providers realize, especially in shortage areas where MHPAEA network adequacy requirements give you grounds for a formal complaint.
Step 8: Review and Sign Your Contracts
When approval comes, you receive a participating provider agreement. Review the fee schedule before signing. While most payers have standard rates, practices in shortage areas or with specialized expertise sometimes have grounds for rate review. Request a retroactive effective date during contract signing — Medicare allows 30 days backdated to filing, and some Medicaid programs allow 90 days. Most commercial payers will not grant retroactive dates, but it costs nothing to ask at this stage and occasionally it succeeds.
Following this process is part of a well-executed revenue cycle management process — credentialing is the upstream step that determines whether every downstream billing function can work at all.
| Week | Phase | Key Actions | Milestone |
|---|---|---|---|
| 1–2 | Foundation | Apply for NPI Type 1 (and Type 2 if group); obtain EIN; create CAQH ProView profile; authorize initial payers | NPI assigned; CAQH profile active and attested |
| 3–4 | Preparation | Gather all documents; check panel status for target payers; confirm carve-out application requirements | Document file complete; target payer list confirmed as open |
| 5–7 | Submission | Submit LOIs where required; submit applications to 3–5 payers simultaneously; authorize CAQH access for each | All applications submitted; reference numbers logged for each |
| 8–12 | Follow-Up | Biweekly calls to credentialing departments; respond to RFIs within 48 hours; verify CAQH attestation still current | Applications in active review; no pended or stalled status |
| 13–16 | Contracting | Review participating provider agreements; request retroactive effective date; sign contracts | Contracts executed; effective date confirmed in writing |
| 17+ | Activation | Confirm directory listing; begin claims submission; verify first reimbursement at contracted rates | First insurance claims submitted; revenue flow begins |
Complete Document Checklist for Mental Health Credentialing
Missing or incomplete documents cause 40 to 60 percent of all credentialing delays. Most of those delays are entirely preventable with proper preparation. The checklist below covers every document category you will encounter across Medicare, Medicaid, and commercial payer applications.
Category 1: Personal Identification
Government-issued photo ID — driver’s license or passport, color scan with front and back visible. Blurry scans and cut-off edges are a surprisingly common reason for application holds. Your Social Security documentation is used initially but gets replaced by your EIN on all ongoing applications.
Category 2: Professional Licensure
Active state license with current expiration — front and back color scan. The address on your license must match the address in your CAQH profile and on every application. A single character variation causes automatic rejection in many payer systems. If you hold licenses in multiple states for telehealth, include all of them. DEA certificate is required for psychiatrists and PMHNPs only. Board certifications should be uploaded as digital scans.
Category 3: Malpractice Insurance
Your current malpractice face sheet showing carrier name, policy number, coverage dates, and limits. Minimum coverage for most major payers is $1 million per occurrence and $3 million aggregate. Some Medicaid programs accept $500,000 per occurrence and $1.5 million aggregate. If you hold a claims-made policy rather than occurrence-based, also include tail coverage documentation — its absence is a common rejection trigger that providers never expect because nobody mentioned it.
Category 4: Education and Training
Graduate diploma or transcripts in high-resolution scan from an accredited institution. Some payers accept a letter of completion for initial applications; Medicare requires official documentation. CV covering the last 5 to 10 years in month-and-year format with written explanations for any gaps exceeding 6 months. Unexplained gaps trigger manual review and add 45 to 75 days to your timeline.
Category 5: Practice and Payer Setup
NPI Type 1 printout from NPPES. NPI Type 2 if billing as a group. EIN confirmation letter from the IRS — this is the CP575 letter, or Letter 147C if your original was lost. The CP575 is the only acceptable EIN verification for Medicare enrollment; a standard welcome letter from the IRS is not sufficient. W-9 form, current tax year, signed. CAQH ProView profile with attestation current within 90 days. Bank account details for EFT payment setup.
For Medicare enrollment, you must complete PECOS enrollment at pecos.cms.hhs.gov and submit either a CMS-855I form for individual providers or a CMS-855B for group practices. PECOS is entirely separate from CAQH and takes 45 to 60 days to process on its own. Our credentialing services include complete PECOS setup and CMS-855 preparation so nothing gets missed in this process.
| Category | Document | Format Required | Payer Applicability | Common Error |
|---|---|---|---|---|
| Identity | Photo ID (driver’s license or passport) | Color scan, front and back | All payers | Blurry scan; cut-off edges |
| Tax/Entity | EIN confirmation (CP575 or Letter 147C) | Original or official copy | All payers; mandatory for Medicare | Welcome letter submitted instead of CP575 |
| Tax/Entity | W-9 form | Signed, dated PDF, current year | All payers | Old version submitted; missing signature |
| Licensure | State professional license (active) | Front and back color scan | All payers | Address mismatch; expired within 30 days |
| Licensure | DEA certificate | Digital scan, current | Psychiatrists and PMHNPs only | Expired; practice address mismatch |
| Licensure | Board certification (ABPN, ABPP, BCBA) | Digital scan, current | Specialists; some commercial plans | “Board eligible” listed as “board certified” |
| Malpractice | Insurance face sheet | PDF showing carrier, policy number, limits, and dates | All payers | Coverage below $1M/$3M minimum |
| Malpractice | Tail coverage documentation | Certificate from carrier | Claims-made policy holders only | Provider unaware it was needed; not submitted |
| Education | Graduate diploma or transcripts | High-resolution scan from accredited institution | Medicaid, Medicare; most commercial plans | Letter of completion submitted instead of degree |
| Education | CV/Resume | PDF; month/year format; gaps explained | All payers | Gaps over 6 months without written explanation |
| Education | Supervision attestation | Signed statement with supervisor details | Associate-level providers | Missing supervisor signature or contact information |
| Practice | NPI Type 1 (individual) | NPPES printout with taxonomy code visible | All payers | Wrong taxonomy code; outdated data not updated |
| Practice | NPI Type 2 (group) | NPPES printout | Group practices | Not obtained; individual NPI used for group billing |
| Practice | CAQH ProView profile | Attested within last 90 days | 90%+ of commercial payers | Attestation expired; payer data pulls stopped |
| Practice | EFT bank authorization | Digital form with banking details | All payers | Not submitted; delays first payment significantly |
| Professional | Professional references (3 to 5) | Name, title, contact information | Select payers upon request | References not notified in advance; wrong contact info |
| Medicare-Specific | PECOS enrollment | Online completion at pecos.cms.hhs.gov | Medicare billing only | Not completed; confused with NPPES registration |
| Medicare-Specific | CMS-855I or CMS-855B | Completed form submitted via PECOS | Medicare enrollment | Wrong form for practice type (I for individual, B for group) |
Mental Health Credentialing Document Checklist — 2026 Edition
Free download: 20+ documents organized by category, expiration tracking columns, and pre-submission audit checklist.
Includes: Identity | Licensure | Malpractice | Practice Setup | Medicare-Specific documents
⬇ Download Free Checklist (PDF)Or let our team handle your entire credentialing process →
How to Get Credentialed with Medicaid, Medicare, and Commercial Insurers
How do I get credentialed with insurance companies for mental health? The honest answer is that it depends entirely on which insurer you are targeting — because the process, portal, timeline, and requirements are meaningfully different for every major payer category. Here is the breakdown, including the behavioral health carve-out section that no competitor in this space publishes.
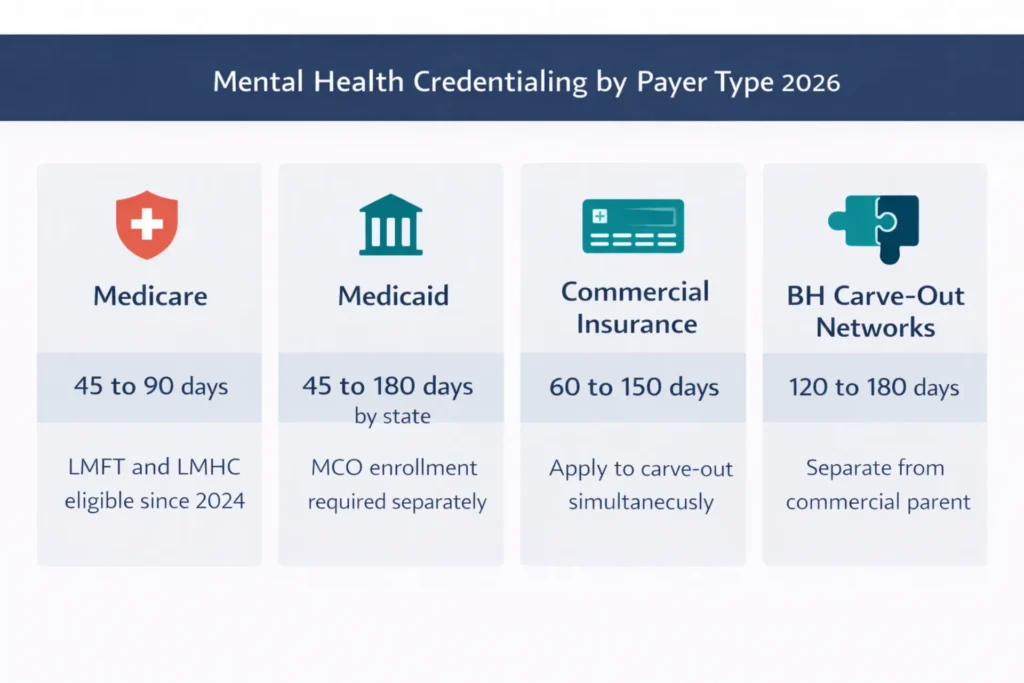
Medicare
Medicare credentialing runs through PECOS — the Provider Enrollment, Chain, and Ownership System at pecos.cms.hhs.gov. Individual providers submit a CMS-855I; groups submit a CMS-855B. The average processing time is 45 to 90 days, making Medicare one of the more predictable credentialing processes when the application is complete and accurate.
The most significant 2024 change for behavioral health: LMFTs and LMHCs became independently eligible to bill Medicare Part B as of January 1, 2024. This is a landmark expansion. Previously, these providers could only bill Medicare through supervised hospital-based or agency settings. Solo practice LMFTs and LMHCs now need to complete PECOS enrollment, and many have not yet done so. If you are an LMFT or LMHC, this is a panel you may have missed entirely — and it is one of the highest-reimbursing payers in behavioral health.
Medicare Advantage plans are separate from traditional Medicare. Enrollment in PECOS does not automatically include you in Humana Medicare Advantage, UnitedHealthcare Medicare Complete, or any other Medicare Advantage plan. Each requires its own application through the plan’s commercial credentialing portal. Medicare revalidation is required every 5 years for standard providers and every 3 years for high-risk providers including those with SUD focus. CMS does not guarantee email notification — use the Medicare Revalidation Lookup Tool annually to avoid missing a cycle that would immediately deactivate your billing privileges.
Medicaid
Medicaid is state-administered, which means the credentialing process is different in every state. Texas uses the Texas PEMS portal and typically processes in 45 to 75 days. California’s Medi-Cal runs through county Mental Health Plans and takes 90 to 180 days. New York’s OMH plans involve Health Homes structures that add layers. Ohio Medicaid routes behavioral health through Optum-managed plans with their own enrollment requirements.
For substance use disorder providers, 42 CFR Part 2 confidentiality requirements add specific compliance obligations to the credentialing application. Payers need attestation that your practice handles SUD patient records under these federal protections. Missing this attestation in carve-out network applications for SUD services is a documentation error that no general medical credentialing guide mentions — because general guides are not written for behavioral health.
In most states, you credential first with the state fee-for-service Medicaid program, then separately with each Medicaid Managed Care Organization operating in your area. A state Medicaid approval does not automatically enroll you with Centene, Molina, Anthem Medicaid, or other MCOs serving your patients. Expect 60 to 90 additional days per MCO application after state approval.
Commercial Insurance
The five major commercial payers all use CAQH but have different processes layered on top of it. Aetna runs applications through Availity with a typical 45-day need evaluation before formal credentialing begins, then 45 to 60 days of contracting — total timeline 60 to 120 days. UnitedHealthcare uses Provider Express and is typically the fastest automated commercial process at 60 to 90 days. Cigna uses CignaforHCP with timelines of 75 to 120 days. Humana requires a Letter of Interest before formal application and generally processes in 60 to 120 days. BCBS varies significantly by region — Texas and Highmark process in 60 to 90 days while New York and California BCBS plans can run 90 to 150 days with committee review phases.
Behavioral Health Carve-Out Networks — The Section Most Guides Miss
This is the part of mental health credentialing that causes more billing problems than any other single issue — and it is almost completely absent from competitor content.
A behavioral health carve-out network is a specialized insurance network that manages mental health and substance use disorder benefits separately from the main medical benefits of a commercial plan. When your patient presents an Anthem insurance card, Anthem may be paying for their medical care — but Carelon Behavioral Health is managing their mental health benefits and maintaining a completely separate provider network. You must be credentialed in both.
Major carve-out networks for mental health providers include Magellan Healthcare, Carelon Behavioral Health (formerly Beacon Health Options, formerly ValueOptions), Optum Behavioral Health (UHC’s separate behavioral health network), Evernorth Behavioral Health (Cigna and Aetna), New Directions Behavioral Health, and ComPsych for EAP credentialing.
Being credentialed with the commercial parent plan does not include you in the carve-out network. You must apply separately, wait separately, and sign separate contracts. Carve-out applications add 120 to 180 days to the timeline if not submitted simultaneously with the commercial parent. If your patient’s mental health benefits run through Carelon and you are only credentialed with Anthem commercial, every claim will deny. Our denial management team regularly identifies missed carve-out enrollment as the root cause when behavioral health practices experience systematic claim denials they cannot explain.
The fix is simple: when you apply to any commercial payer, immediately check whether they use a behavioral health carve-out and submit that application at the same time. Apply in parallel, not in sequence. This one step saves 90 to 180 days.
TRICARE
TRICARE serves active duty military, retirees, and their families. Regional contractors handle credentialing — Humana Military for TRICARE East, TriWest for TRICARE West. Mental health counselors applying for TRICARE must provide proof of NCMHCE exam passage and two years of post-master’s supervised experience. Timeline is 90 to 120 days. Both a separate TRICARE East and TRICARE West application may be needed for multi-state practices.
| Payer Type | Portal/System | Typical Timeline | Behavioral Health-Specific Requirements | 2026 Notes |
|---|---|---|---|---|
| Medicare | PECOS (pecos.cms.hhs.gov) | 45–90 days | LMFT/LMHC eligible since January 2024; CMS-855I or 855B required | Check Revalidation Lookup Tool annually |
| Medicaid — TX, FL | TX PEMS; FL Share | 45–75 days | 42 CFR Part 2 attestation for SUD; MCO enrollment is separate after state approval | Fastest state Medicaid programs |
| Medicaid — CA, NY | Medi-Cal Provider App; NY OMH | 90–180 days | County Mental Health Plan layers add significant time | Begin simultaneously with commercial applications |
| Aetna / Evernorth BH | Availity (commercial); Evernorth portal (BH carve-out) | 60–120 days each | Separate Evernorth BH application required — apply simultaneously | Panels mostly open for LCSW/LPC/LMFT |
| UHC / Optum BH | Provider Express (UHC); OptumID (BH carve-out) | 60–90 days UHC; 90–180 days Optum BH | Optum BH is entirely separate — apply at same time as UHC commercial | Applying to both simultaneously saves 90+ days |
| Cigna / Evernorth BH | CignaforHCP; Evernorth portal | 75–120 days | Evernorth BH requires separate enrollment from Cigna commercial | Shortage area panels typically open |
| BCBS Regional | State-specific portals including Availity and ProviderSync | 60–150 days | Regional BH managers vary significantly by state | Call provider relations to confirm carve-out structure in your state |
| BH Carve-Outs (Magellan, Carelon) | Carve-out-specific portals | 120–180 days | Separate from commercial parent; required for mental health billing access | Apply simultaneously with commercial parent — never sequentially |
| TRICARE | Humana Military (East); TriWest (West) | 90–120 days | NCMHCE proof required for counselors; 2-year post-master’s supervision | Military-specific documentation needed beyond standard credentialing |
Managing all of these applications simultaneously, tracking their statuses, and ensuring carve-out enrollment is not missed — particularly for practices serving multiple commercial plans — is precisely where professional credentialing services earn their fee. When credentialing is connected directly to billing, the insurance eligibility verification process also starts the moment your first effective date is confirmed — so you are not starting from scratch on the billing side while credentialing finalizes.
Common Credentialing Mistakes That Delay Revenue
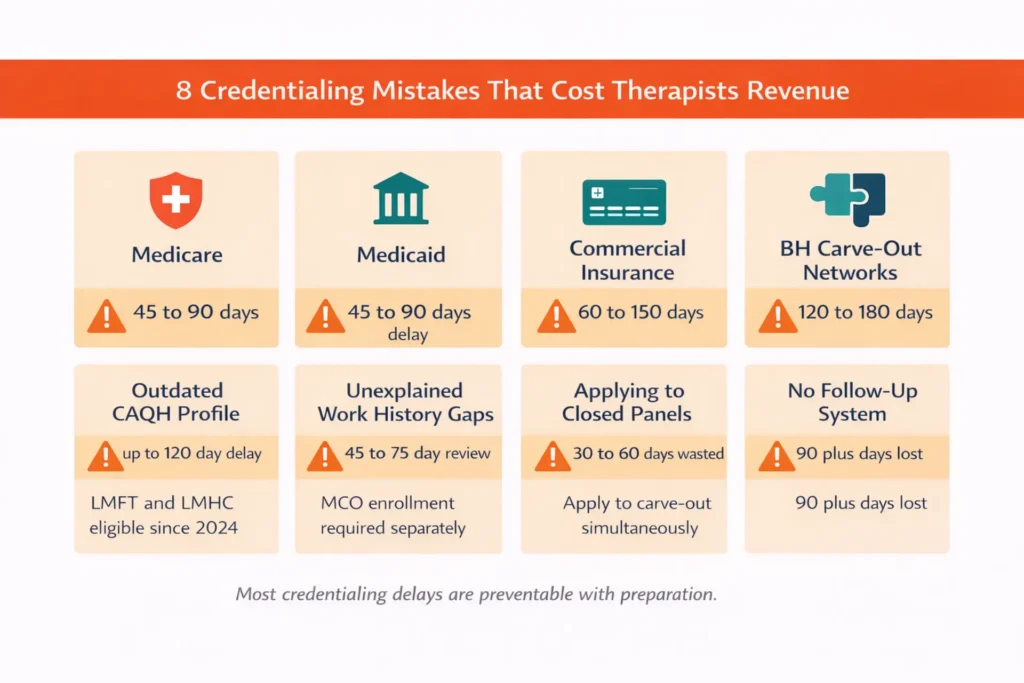
The mistake that adds 45 to 60 days to your credentialing is almost always the same thing across practices we work with. It is not a complicated application or a difficult payer. It is your CAQH attestation expiring while your applications are in review — because nobody calendared the 90-day requirement, or because the practice assumed it auto-renewed. It does not.
What we consistently see across behavioral health practices is that most credentialing delays are not caused by complex problems. They are caused by eight specific, predictable, and entirely preventable errors.
| Mistake | Root Cause | Revenue Impact | Prevention |
|---|---|---|---|
| Outdated CAQH profile | Quarterly attestation skipped; expired documents not uploaded when renewed | $18,000–$36,000 (60–120 day delay) | Calendar attestation every 90 days; upload license and malpractice renewals immediately upon receipt |
| Address mismatch across systems | License, NPI, CAQH, and applications each have slight variations in address | $13,500–$27,000 (45–90 day delay) | Standardize your exact address in NPPES and CAQH first; verify all applications match before submitting |
| SSN instead of EIN | Solo providers using personal SSN on group or business applications | $9,000–$18,000 (30–60 day restart) | Always use EIN; obtain at IRS.gov if not yet done — it takes 5 minutes |
| Wrong NPI type | Groups submitting NPI Type 1 instead of Type 2 for group billing | $18,000–$36,000 (60-day fix plus post-approval claim denials) | Register both Type 1 and Type 2; verify group applications use Type 2 |
| Missing or expired malpractice documentation | Face sheet not submitted; claims-made policy missing tail coverage | $27,000 (90-day verification halt) | Submit $1M/$3M face sheet upfront; renew 60 days pre-expiry; always include tail coverage |
| Incomplete work history | Gaps over 6 months not explained; entries listed without month-and-year format | $13,500–$22,500 (45–75 day manual review) | Cover 5 to 10 years in month/year format; write a brief explanation for every gap including parental leave and education |
| Applying to closed panels | No pre-check of panel status before submitting application | $9,000–$18,000 (30–60 days wasted before rejection) | Call provider relations or check Availity and Provider Express before any application submission |
| Insufficient follow-up | Assuming applications process automatically without regular check-ins | $27,000–$45,000 (90+ day delays for lost applications) | Biweekly calls; document date, representative name, and ticket number every time |
When a panel is closed, you have more options than most guides acknowledge. Under the 2024 MHPAEA Final Rules, payers must demonstrate adequate behavioral health network access. If you practice in a shortage area or specialize in an underserved population — eating disorders, trauma, SUD, geriatric mental health — you can file a network adequacy complaint with your state insurance commissioner. This approach has successfully opened panels for several practices we work with.
When an application is stuck past 60 days, escalate beyond the general credentialing line. Call provider relations, ask for a supervisor, and request a direct email for follow-up documentation. After 90 days, contact the credentialing director with your documented call log. After 120 days, a state insurance commissioner complaint almost always produces movement.
And when credentialing delays eventually produce claim denials — because effective dates were not coordinated with billing, or because a carve-out enrollment was missed — systematic denial management works through those recoverable claims. But the best denial is the one that never happens, which is why our credentialing work is integrated with our billing and medical coding services from day one.
How Long Does Mental Health Credentialing Take?
Mental health credentialing typically takes 90 to 120 days for commercial insurance — but that average hides enormous variation by payer, and understanding where the real delays live helps you plan around them intelligently.
Here is the realistic distribution: about 20 percent of providers complete credentialing within 60 days, typically Medicare and UHC with clean and complete applications. About 50 percent reach the 90-day mark. About 75 percent are done by 120 days. The remaining 15 to 20 percent extend to 150 or 180 days — almost always because of carve-out network applications, California Medi-Cal county layers, or applications that got lost without systematic follow-up.
| Payer | Fastest (Clean Application) | Typical | Slowest | Main Delay Factor |
|---|---|---|---|---|
| Medicare (PECOS) | 45 days | 60–75 days | 90 days | CAQH or PECOS data mismatch; 2024 expansion volume |
| Medicaid — TX, FL | 45 days | 60 days | 75 days | Fastest state programs; streamlined portals |
| Medicaid — CA, NY | 90 days | 120–150 days | 180 days | County MHP layers (CA); Health Homes structure (NY) |
| UHC via Provider Express | 60 days | 75–90 days | 120 days | Most automated commercial process available |
| Aetna via Availity | 60 days | 90–100 days | 120 days | 45-day need evaluation adds front-end time |
| BCBS (fast regions: TX, Highmark) | 60 days | 75–90 days | 120 days | Regional variation is significant |
| BCBS (slow regions: CA, NY) | 90 days | 120 days | 150 days | Manual committee review phases |
| Cigna / Evernorth commercial | 75 days | 90–100 days | 120 days | Unpredictable committee review phase |
| Optum Behavioral Health carve-out | 90 days | 120–150 days | 180 days | Separate from UHC commercial; second review layer |
| Magellan / Carelon BH carve-out | 120 days | 150 days | 180+ days | Secondary review doubles commercial timeline |
| TRICARE | 90 days | 100–120 days | 150 days | NCMHCE verification for counselors |
The revenue math at each interval is significant. At 60 days, a 25-session-per-week practice at $150 per session defers $30,000. At 90 days, $45,000. At 120 days, $60,000. At 180 days — which happens more often than people expect with carve-out applications — $90,000 in revenue that most commercial payers will not reimburse retroactively.
The fastest legitimate strategy to accelerate your timeline: complete your CAQH profile fully 4 to 6 weeks before submitting any applications. Apply to Medicare and UHC simultaneously as your first submissions. Submit commercial applications in parallel with carve-out applications on the same day, not after commercial approval. Follow up every 10 to 14 days without exception. Professional credentialing services consistently reduce timelines by 30 to 50 days through dedicated follow-up protocols, which translates to $11,250 to $18,750 in recovered revenue per provider at typical billing rates.
Can you see patients while credentialing is pending? Yes — for cash-pay or out-of-pocket clients only. For insurance billing, you cannot submit claims until you have an effective date confirmed in writing by the payer. Never tell a patient their sessions will be covered by insurance until that confirmation is in your hands.
FREE TOOL
Credentialing Revenue Loss Calculator
Enter your practice details to see exactly how much revenue a credentialing delay is costing you.
Re-Credentialing — How to Stay Continuously Compliant
Getting credentialed is the hard part the first time. Staying credentialed is the silent revenue risk that most practice owners discover only when claims start denying and nobody can immediately explain why.
Commercial payers require re-credentialing every 2 to 3 years. Aetna, Cigna, and UnitedHealthcare run 3-year cycles. BCBS and Humana range from 2 to 3 years depending on region. Medicare revalidation occurs every 5 years for standard providers and every 3 years for high-risk providers — those with SUD focus, frequent claims reviews, or prior sanctions history. NCQA and URAC accreditation standards cap re-credentialing cycles at 36 months maximum for accredited plans. Medicaid re-credentialing varies by state, with most running 3 to 5 year cycles.
| Payer Type | Re-Credentialing Cycle | Notification Method | Grace Period | Consequence of Missing Deadline |
|---|---|---|---|---|
| Medicare | Every 5 years standard; 3 years high-risk | CMS via PECOS — email not guaranteed | 90 days retroactive revalidation | PTAN deactivation; all Medicare billing stops immediately |
| Medicaid | 3–5 years by state | State portal notification varies | 30–90 days depending on state | Network termination; full re-application required |
| Aetna / Cigna / UHC | Every 3 years | CAQH-driven notices; payer reminders | None — zero-tolerance automation | Immediate network suspension; claim denials begin same day |
| BCBS / Humana | 2–3 years depending on region | Payer notice; 60–90 day window | 30 days in select regions only | Network termination; 60–120 day re-enrollment period |
| Behavioral Health Carve-Outs | 2–3 years | Carve-out portal notifications | None typically | Double suspension — commercial AND carve-out network both terminate |
The single most important re-credentialing action — and the one most consistently missed — is checking the Medicare Revalidation Lookup Tool annually. CMS does not guarantee email notification when your revalidation is due. If your PTAN deactivates because you missed a revalidation cycle, reinstatement requires a full re-enrollment and another 60 to 90 day wait. For a practice billing 25 sessions per week at $150, that is $15,000 to $22,500 in lost Medicare revenue for every month you are offline — none of which is retroactively recoverable.
Beyond scheduled cycles, several changes trigger immediate re-credentialing updates that must be completed within 15 to 30 days: license renewal, address change, name change, malpractice claims or settlements, board discipline, adding a new practice location, or changing group practice affiliation. Commercial payers use zero-tolerance automation — if CAQH data does not reflect updated information within their tolerance window, network status toggles off automatically without any manual review or warning.
For practices with three or more providers, manual tracking of re-credentialing across 50-plus expiration dates and multiple payers is genuinely unmanageable without systems. Tools worth knowing include Modio Health ($50 to $100 per month, excellent for small to mid-size practices), EddyCore ($75 to $150 per month, strong multi-payer calendar), NuCo Wallet ($20 to $40 per month, good for solo providers), and MedTrainer for compliance-heavy practices. CAQH ProView itself sends 30, 15, and 7-day attestation reminders for free — that alone is the minimum system any practice should be using.
A missed 4-month re-enrollment cycle costs a typical practice $60,000 in permanently unrecoverable revenue. Proactive re-credentialing management is not optional overhead — it is revenue protection, and it connects directly to everything else in your complete RCM services workflow.
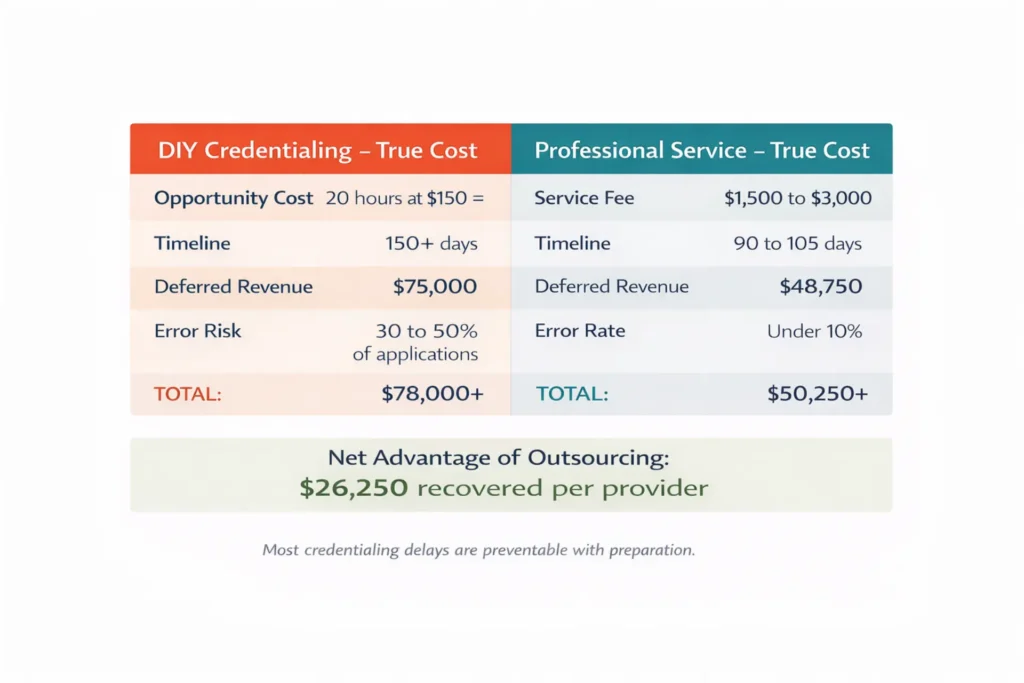
Should You Outsource Mental Health Credentialing?
Let's calculate the real cost of doing this yourself before making that decision honestly.
DIY credentialing for a 5-payer panel: the average time is 4 hours per payer application when you account for document gathering, portal navigation, Letter of Interest preparation where required, and initial follow-up calls. Five payers times 4 hours equals 20 hours. At a therapist's clinical rate of $150 per hour, that is $3,000 in opportunity cost before you count ongoing biweekly follow-up calls over 90-plus days. Add the revenue impact of a timeline that typically runs 30 to 40 days longer with DIY management than with professional follow-up — that is another $11,250 to $15,000 in deferred revenue. True DIY cost for a 5-payer first panel: $14,000 to $18,000 when you count what you are actually spending.
Professional credentialing service for a 5-payer full panel: $1,500 to $3,000 flat, including CAQH setup, all payer applications, follow-up management, and contract review. The timeline advantage — 30 to 50 days faster — recovers $11,250 to $18,750 in revenue. Net ROI: professional services pay for themselves and generate positive returns in the first month of faster billing.
| Practice Scenario | DIY Recommended? | Outsource Recommended? | Reasoning |
|---|---|---|---|
| Solo therapist, 1–3 local payers, prior credentialing experience, available time | Yes | Optional | Low volume; manageable tracking; zero direct service cost |
| Solo therapist, 4+ payers, first credentialing attempt | No | Yes | Error risk exceeds service fee; opportunity cost is significant |
| Group practice, 2–5 clinicians | No | Strongly yes | 50-plus hours of labor; ongoing re-credentialing for multiple providers |
| Multi-state telehealth practice | No | Essential | State license variations; compact applications; carve-out complexity across states |
| New practice launch, zero revenue pre-credentialing | No | Yes | Speed to revenue is critical; every deferred day is permanently lost |
| SUD specialty practice with 42 CFR Part 2 compliance | No | Yes | Carve-out compliance requirements require behavioral health expertise |
| Practice with prior credentialing problems or unexpected denials | No | Yes | Previous mistakes compound; specialist intervention prevents recurrence |
| Established solo practice, re-credentialing only, tracking system in place | Possibly | Yes if 3+ payers | Maintenance feasible solo for simple panels; group practices benefit from delegation |
Three types of credentialing services exist in 2026, and they serve different needs. Network platforms like Headway, Grow Therapy, and Alma offer free credentialing but retain 10 to 25 percent of your reimbursement — zero admin overhead, but permanently reduced income on those claims. Full-service credentialing firms charge $150 to $400 per payer or $1,500 to $3,000 for a full panel, and you retain your full contracted reimbursement rate. Integrated billing and credentialing services — which is how Elite Med Financials is structured — combine credentialing enrollment with ongoing billing management, eliminating the data hand-off delay that occurs when two separate vendors need to coordinate your effective date with your first claim submission.
When evaluating any credentialing service, ask these specific questions: Do you credential with behavioral health carve-out networks as a standard part of the service? Do you manage CAQH quarterly attestation on my behalf? Do you handle the 2024 Medicare LMFT/LMHC expansion for PECOS enrollment? Can you credential with state Medicaid and MCOs, not just commercial payers? Do you include re-credentialing management after the initial panel is established? A general medical credentialing service that cannot answer yes to all of these is not equipped for behavioral health.
When credentialing connects directly into the billing workflow — so that the moment your effective date is confirmed, clean claims are queued and correctly coded — the revenue gap shrinks to days rather than weeks. That is the integrated value of a team that handles your mental health billing services and credentialing together. Correct coding from our medical coding specialists means your first claims after credentialing approval go through clean, not back through a denial queue. Our payment posting and AR follow-up services run in parallel so nothing ages in a queue while credentialing finalizes.
FREE CREDENTIALING CONSULTATION
Stop Losing Revenue to Credentialing Delays — We Handle Everything
Elite Med Financials handles your credentialing AND billing together — so when your effective date arrives, your first claims go out the same day. No missed carve-out networks. No CAQH lapses. No billing gaps.
Serving mental health practices in all 50 states. Behavioral health specialists. No hidden fees.
Common Questions About Mental Health Credentialing
Is it hard to get credentialed with insurance as a therapist?
It is time-consuming more than technically difficult. The challenge is managing 15 to 25 documents across multiple simultaneous applications while following up every 10 to 14 days over 90 to 120 days — all while running a clinical practice. Providers who prepare documents completely before applying and follow up systematically consistently finish 30 to 45 days faster than those who approach it reactively.
Can I do my own credentialing as a therapist?
Yes, and many solo therapists with 1 to 3 simple payers do. The NPI, EIN, CAQH ProView, and payer application portals are all publicly accessible. The real cost is opportunity cost — 20 to 30 hours for a 5-payer panel at a clinical hourly rate equals $3,000 to $4,500 in forgone patient revenue. For group practices or multi-state telehealth providers, the complexity and error risk typically exceed professional service fees.
How long does mental health credentialing take in 2026?
Commercial insurance credentialing takes 90 to 120 days on average. Medicare processes faster at 45 to 90 days. Medicaid ranges from 45 days in Texas and Florida to 180 days in California and New York due to county-level structures. Behavioral health carve-out networks like Magellan and Carelon add 120 to 180 days on top of the commercial timeline when not applied to simultaneously.
What is CAQH and why do therapists need it?
CAQH ProView is a centralized credentialing database at caqh.org that over 90 percent of commercial insurance payers use to verify provider qualifications. You enter your credentials once and authorize specific payers to access your profile. The critical requirement: you must attest that your data is current every 90 days. If attestation expires while applications are in review, payer applications automatically pause, adding 30 to 60 days to your timeline.
How much does professional credentialing cost for a therapist?
Full-service credentialing for a 5-payer panel typically costs $1,500 to $3,000 from a professional firm. Per-payer rates range from $150 to $400. Ongoing re-credentialing management runs $100 to $300 per month for multi-provider practices. Network platforms like Headway offer free credentialing but retain 10 to 25 percent of your reimbursement, which significantly reduces long-term income compared to owning your contracts directly.
What are the best credentialing services for mental health providers?
The best mental health credentialing services specialize specifically in behavioral health — not general medical credentialing. They include behavioral health carve-out network enrollment as standard, manage CAQH quarterly attestation, handle Medicare PECOS enrollment including the 2024 LMFT and LMHC expansion, understand 42 CFR Part 2 requirements for SUD practices, and offer re-credentialing maintenance to protect your network status between credentialing cycles.
What documents do I need to start the credentialing process?
Core documents include: active state license, malpractice insurance face sheet showing at least $1 million per occurrence and $3 million aggregate, NPI Type 1 from NPPES, EIN confirmation letter CP575 from the IRS, completed CAQH ProView profile with current attestation, graduate diploma or transcripts, CV covering 5 to 10 years with gaps explained, three professional references, and a W-9 form. Medicare enrollment additionally requires PECOS completion and CMS-855I or 855B forms.
How do I get credentialed with insurance companies quickly?
Start preparation 6 to 8 weeks before submitting any applications. Complete your CAQH profile fully before applying. Submit to Medicare and your fastest commercial payer simultaneously as your first two applications. Apply to behavioral health carve-out networks on the same day as the commercial parent — never after. Follow up every 10 to 14 days without exception and document every call. Professional credentialing services consistently cut timelines by 30 to 50 days through systematic follow-up.
Frequently Asked Questions About Mental Health Credentialing
What is mental health provider credentialing?
Mental health provider credentialing is the process where insurance companies verify a provider's license, education, malpractice history, and professional background before enrolling them as an in-network provider. It differs from licensing (granted by the state), contracting (defines reimbursement rates), and enrollment (activates billing). The process typically takes 90 to 120 days and requires 15 to 25 documents depending on the payer. Behavioral health credentialing differs from general medical credentialing because many plans use separate carve-out networks that require independent applications beyond commercial credentialing.
How do I get credentialed with insurance as a therapist?
Getting credentialed involves 8 steps: obtain NPI Type 1 and Type 2 if billing as a group, secure an EIN from the IRS, complete your CAQH ProView profile, gather all required documents, research which panels are open, submit applications through payer portals, follow up every 10 to 14 days, and review and sign your participating provider agreement. The process takes 90 to 120 days for most commercial payers. Applying to behavioral health carve-out networks simultaneously with commercial applications saves 60 to 90 additional days compared to applying sequentially.
How long does mental health credentialing take?
Mental health credentialing takes 90 to 120 days on average for commercial insurance. Medicare processes in 45 to 90 days. Medicaid ranges from 45 days in faster states to 180 days in California and New York. Behavioral health carve-out networks add 120 to 180 days if applied to separately. Only about 20 percent of providers complete the process within 60 days. The 15 to 20 percent who extend past 180 days almost always have carve-out applications or preventable application errors at the root cause.
What documents do I need for mental health credentialing?
Required documents include: active state license, malpractice face sheet with at least $1M per occurrence and $3M aggregate coverage, NPI Type 1 number, EIN confirmation letter CP575 from the IRS, completed CAQH ProView profile, graduate diploma or transcripts, CV covering 5 to 10 years with gaps explained, three professional references, and a signed W-9 form. Medicare enrollment additionally requires PECOS completion and a CMS-855I or 855B form. Missing or incorrect documents cause 40 to 60 percent of credentialing delays.
What is CAQH ProView and how does it work?
CAQH ProView is a centralized credentialing database at proview.caqh.org used by over 90 percent of commercial payers. Providers enter credentials once, upload supporting documents, and authorize specific payers to access their profile for credentialing review. Setup takes 4 to 8 hours. Providers must attest every 90 days — if attestation lapses, payer data pulls stop automatically and applications pause, adding 30 to 60 days to credentialing timelines without any immediate notification to the provider.
What are behavioral health carve-out networks?
Behavioral health carve-out networks manage mental health and substance use disorder benefits separately from a commercial plan's main medical benefits. Examples include Magellan Healthcare, Carelon Behavioral Health (formerly Beacon/ValueOptions), Optum Behavioral Health, and Evernorth. Being credentialed with a commercial payer does not automatically enroll you in their carve-out. Missing carve-out enrollment is the leading cause of unexpected, systematic claim denials for mental health providers who otherwise believe their credentialing is complete.
How much does it cost to get credentialed with insurance?
DIY credentialing is technically free but costs 20 to 30 hours for a 5-payer panel — approximately $3,000 to $4,500 in opportunity cost at a clinical billing rate. Professional services charge $1,500 to $3,000 for a full panel setup. They typically pay for themselves by reducing timelines 30 to 50 days, recovering $11,250 to $18,750 in deferred revenue. Network platforms like Headway offer free credentialing but retain 10 to 25 percent of reimbursement, reducing long-term income compared to owning your contracts outright.
How often do mental health providers need to re-credential?
Commercial payers require re-credentialing every 2 to 3 years. Medicare requires revalidation every 5 years for standard providers and every 3 years for high-risk providers. CAQH ProView requires attestation every 90 days continuously throughout your career. Missing commercial re-credentialing deadlines triggers automatic network suspension with no grace period. Missing Medicare revalidation deactivates your PTAN immediately, stopping all Medicare billing until re-enrollment completes — typically 60 to 90 days.
What happens if you miss a re-credentialing deadline?
Missing a commercial re-credentialing deadline triggers immediate network suspension. Claims submitted after suspension are denied, and commercial payers do not allow retroactive billing for the lapse period. Re-enrollment after a lapse takes 60 to 120 days essentially repeating the full initial credentialing timeline. For a practice billing 25 sessions per week at $150, a 4-month re-enrollment period represents $60,000 in permanently unrecoverable revenue that no commercial payer will reimburse retroactively.
Should I outsource mental health credentialing or do it myself?
Outsourcing makes sense for practices with 4 or more payers, any group practice, multi-state telehealth providers, and first-time credentialing attempts. DIY works for solo therapists with 1 to 3 local payers who have prior credentialing experience and available time. The ROI calculation favors outsourcing for practices generating over $200,000 annually — the service cost ($1,500 to $3,000) is recovered in the first month of faster billing. For practices where carve-outs, Medicare, and Medicaid are all involved, specialized outsourcing is effectively essential.
What is the 2024 Medicare expansion for LMFTs and LMHCs?
As of January 1, 2024, Licensed Marriage and Family Therapists and Licensed Mental Health Counselors became independently eligible to bill Medicare Part B for outpatient services. Previously these providers could only bill Medicare through supervised hospital or agency settings. Solo practice LMFTs and LMHCs now need to complete PECOS enrollment and submit a CMS-855I form. Processing takes 45 to 90 days. This is a significant revenue opportunity that many LMFTs and LMHCs have not yet acted on, representing new access to one of behavioral health's highest-reimbursing payers.
What makes a credentialing service genuinely specialized for behavioral health?
A genuinely behavioral-health-specialized service enrolls providers in carve-out networks — Optum BH, Magellan, Carelon, Evernorth — as a standard part of the service without additional fees. It manages CAQH quarterly attestation proactively, handles Medicare PECOS enrollment including the 2024 LMFT and LMHC expansion, understands 42 CFR Part 2 compliance for SUD practices, and includes re-credentialing maintenance between cycles. General medical credentialing services routinely miss carve-out enrollment, which is the most common cause of systematic mental health billing denials.
Three Things Every Mental Health Provider Should Know Before Starting Credentialing
Credentialing is a 90 to 180 day process that determines the exact date your insurance billing can begin. Every week you delay starting is a week you add to the deferred revenue gap. Start the process 4 to 6 months before you plan to see your first insured patient — not the week you open your doors.
Behavioral health credentialing requires navigating separate carve-out networks that every general medical guide misses. If you credential with UHC but not Optum Behavioral Health, and with Cigna but not Evernorth, a significant portion of your patients will have their mental health benefits managed by networks you are not in. The claims will deny. The patients will be frustrated. This one knowledge gap causes more billing disruption in behavioral health practices than any other single issue.
Professional credentialing services pay for themselves. The math is not close: a service costing $1,500 to $3,000 that reduces your time-to-revenue by 30 to 50 days generates $11,250 to $18,750 in recovered revenue at typical billing rates. For group practices and multi-state telehealth providers, the return is even more clear.
Elite Med Financials specializes exclusively in behavioral health revenue cycle management. Our team handles credentialing and billing together — which means when your effective date arrives, your first claims go out the same day, clean, correctly coded, and connected to our ongoing AR follow-up and patient statement services. No data hand-off. No missed carve-out networks. No billing gaps while credentialing finalizes.
We serve mental health practices in all 50 states — solo therapists, group practices, telehealth providers, SUD programs, and psychiatric practices. If you want to stop losing revenue to credentialing delays and start billing with confidence from day one, reach out to our team. Learn more about how credentialing fits into your full revenue cycle at our guide to improving revenue cycle management and our overview of revenue cycle management for behavioral health practices.
PROTECT YOUR REVENUE FROM DAY ONE
Our credentialing team has helped mental health practices reduce their time-to-revenue by 30–50 days
We specialize in behavioral health credentialing — including carve-out networks, CAQH management, and the 2024 Medicare LMFT/LMHC expansion. Get a free assessment of your current credentialing status.
Schedule a Free Credentialing Assessment →