Wound care graft Medicare coverage under Part B is confirmed — but only when medical necessity is fully documented and your claim satisfies Local Coverage Determination (LCD) L33831 criteria. Coverage applies to cellular and tissue-based products (CTPs) used for diabetic foot ulcers, venous leg ulcers, and pressure injuries that have not responded to at least four weeks of standard conservative treatment.
That one paragraph answers the question thousands of providers, practice managers, and patients type into search engines every month. But if you’ve ever submitted a graft claim and watched it get denied — or worse, flagged during a RAC audit three years later — you already know the answer is nowhere near that simple.
Medicare’s wound care graft coverage framework is one of the most policy-dense, product-specific, and audit-sensitive billing areas in all of healthcare. The 2026 CMS final rule reshaped how skin substitute products are categorized, priced, and reimbursed. LCD policies vary by MAC jurisdiction. Product Q-codes change. Documentation that was sufficient in 2023 can fail medical necessity review in 2026.
This guide covers everything: how Medicare covers wound grafts by setting, what the LCDs actually require, which products are on the covered list, what the 2026 fee schedule looks like, and how to appeal when coverage is wrongfully denied. Whether you’re a wound care specialist, a revenue cycle manager, or a practice owner trying to understand why your reimbursement dropped, this is the most complete reference you’ll find in 2026.
What Are Wound Care Grafts? The Types Medicare Actually Recognizes
Before diving into coverage rules, it’s worth being clear about what Medicare considers a “wound graft” versus what it doesn’t — because that distinction determines which billing pathway applies and which LCD governs your claim.
CMS classifies wound graft products primarily as cellular and tissue-based products (CTPs), sometimes called skin substitutes. These are bioengineered or biologically derived materials applied to a wound to facilitate healing. Medicare distinguishes them from simple wound dressings (covered separately under the surgical dressing LCD) and from traditional autografts, which are procedures involving a patient’s own skin (billed under different CPT codes and covered under different rules).

The four major CTP categories Medicare recognizes:
- Cellular-based products — contain living cells (fibroblasts, keratinocytes, or both) and function as bioactive scaffolds. Products like Apligraf (Organogenesis) and Dermagraft (Organogenesis) fall here.
- Acellular dermal matrices (ADMs) — processed tissue that provides a scaffold without living cells, such as Oasis Wound Matrix (Smith & Nephew).
- Amniotic membrane products — derived from the placenta’s amniotic layer; include EpiFix and AmnioFix (both by MIMEDX), as well as multiple Q-coded products. For a deep dive on amniotic membrane billing specifically, see our guide on amniotic membrane graft billing, CPT codes, and Q-codes.
- Omega-3 fish skin grafts — an emerging class; Kerecis Omega3 Wound from Kerecis uses Atlantic cod skin and has earned Medicare coverage under specific criteria.
Additionally, products from manufacturers including Integra LifeSciences, LifeNet Health, MTF Biologics, and Stryker carry HCPCS Q-codes recognized within the CTP framework, each with product-specific coverage criteria.
What Medicare does not cover under this framework: standard hydrocolloid dressings, foam dressings, hydrogels, or compression bandaging — those are surgical dressings billed separately. Negative pressure wound therapy (wound VAC) has its own LCD. And cosmetic skin procedures are explicitly excluded.
Understanding which product type you’re dealing with before submitting a claim is not optional. The wrong billing pathway is one of the most common sources of preventable denials in wound care practices.
Does Medicare Cover Wound Grafts? Part A, Part B, and Medicare Advantage — Explained
The short answer is yes. The longer answer is: it depends on where the graft is applied, which part of Medicare the patient has, and whether your documentation meets the threshold that each MAC enforces.
Here’s how coverage breaks down by setting:
Table 1: Medicare Coverage for Wound Care Grafts by Setting
| Care Setting | Medicare Part | Coverage Status | Key Requirements | Important Notes |
|---|---|---|---|---|
| Physician Office | Part B | Covered | LCD medical necessity, valid Q-code, conservative care failure | Most common billing setting; physician bills global fee |
| Hospital Outpatient (HOPD) | Part B (OPPS) | Covered | Same LCD criteria; facility bills via APC | Product packaged under OPPS in some cases; separate billing rules apply |
| Ambulatory Surgical Center (ASC) | Part B | Covered | ASC-approved procedure; prior auth varies by plan | Check ASC covered procedures list annually |
| Skilled Nursing Facility (SNF) | Part A (consolidated billing) | Limited | Bundled into SNF PPS during qualifying stay | Separate Part B billing available post-qualifying stay in some scenarios |
| Home Health | Part A or Part B | Limited | Under home health benefit; grafts typically not separately billable during active HH episode | Exceptions exist; document carefully |
| Inpatient Hospital | Part A | Covered under DRG | Part of inpatient stay reimbursement | Not separately billable; document for DRG optimization |
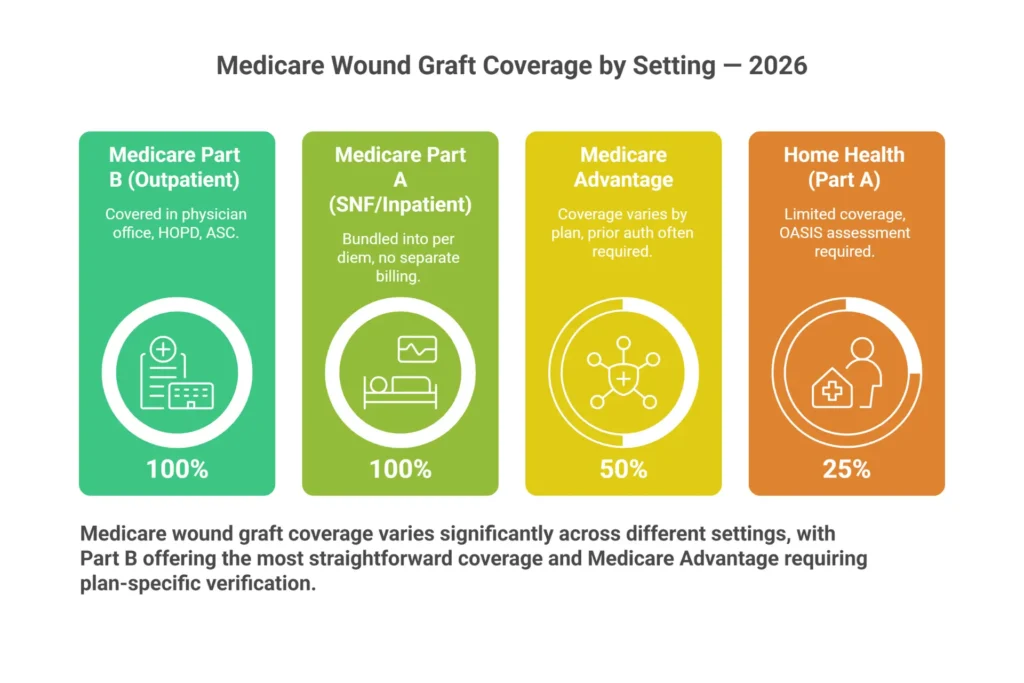
Medicare Advantage (Part C) deserves special attention here. MA plans are required by law to cover everything Original Medicare covers — but they’re permitted to impose prior authorization requirements, use different formularies for CTPs, and require network-based referrals. In our experience working with wound care practices across multiple MAC jurisdictions, Medicare Advantage wound graft denials are disproportionately high compared to traditional Medicare. The reason is almost always prior authorization that wasn’t obtained, or a product that’s on Medicare’s covered list but excluded from that specific MA plan’s approved product formulary.
If you’re billing Medicare Advantage plans for wound grafts, the verification step before the first graft application is not just recommended — it’s financially essential. Our wound care RCM specialists handle MA plan verification as a standard part of the pre-claim workflow because the cost of a missed prior auth is never worth the shortcut.
Medicare Part B is where the vast majority of wound care graft billing happens — specifically through the Physician Fee Schedule (PFS) for office-based procedures and the Outpatient Prospective Payment System (OPPS) for hospital-based outpatient wound care centers.
Medicare Wound Graft
Coverage Eligibility Checker
Answer 6 quick questions to see if your patient’s wound graft treatment is likely covered under Medicare — and what documentation you’ll need.
LCD Policies That Govern Wound Care Graft Medicare Coverage in 2026
If you’re billing wound care grafts to Medicare and you haven’t read the applicable LCD cover to cover, you’re operating blind. These policies are not suggestions — they are the rulebook that Medicare Administrative Contractors use to approve or deny your claims.
The primary LCD governing cellular and tissue-based products nationally is L33831 (Cellular and Tissue-Based Products for Chronic Wounds), though the specific LCD number varies by MAC jurisdiction. Complementary policies include the related Article A59518, which provides billing and coding guidance, and L35041 in some jurisdictions. Always verify the active LCD with your specific MAC.
The six MACs and their jurisdiction coverage:
- Novitas Solutions — JH (PA, NJ, MD, DE, DC) and JL (AR, CO, LA, MS, NM, OK, TX)
- CGS Administrators — J15 (KY, OH) and JM (AL, GA, TN)
- WPS Government Health Administrators — J5 (IA, KS, MO, NE) and J8 (IN, MI)
- Palmetto GBA — JM/J11 (NC, SC, VA, WV) and JJ (CA)
- First Coast Service Options — JN (FL, PR, VI)
- National Government Services (NGS) — J6 (IL, MN, WI) and JK (CT, ME, MA, NH, NY, RI, VT)
Each MAC publishes its own version of the CTP LCD, and while the criteria are substantially similar, there are meaningful differences in how they define “adequate conservative treatment,” what documentation they require for wound measurements, and how they handle products added to the covered list mid-year.
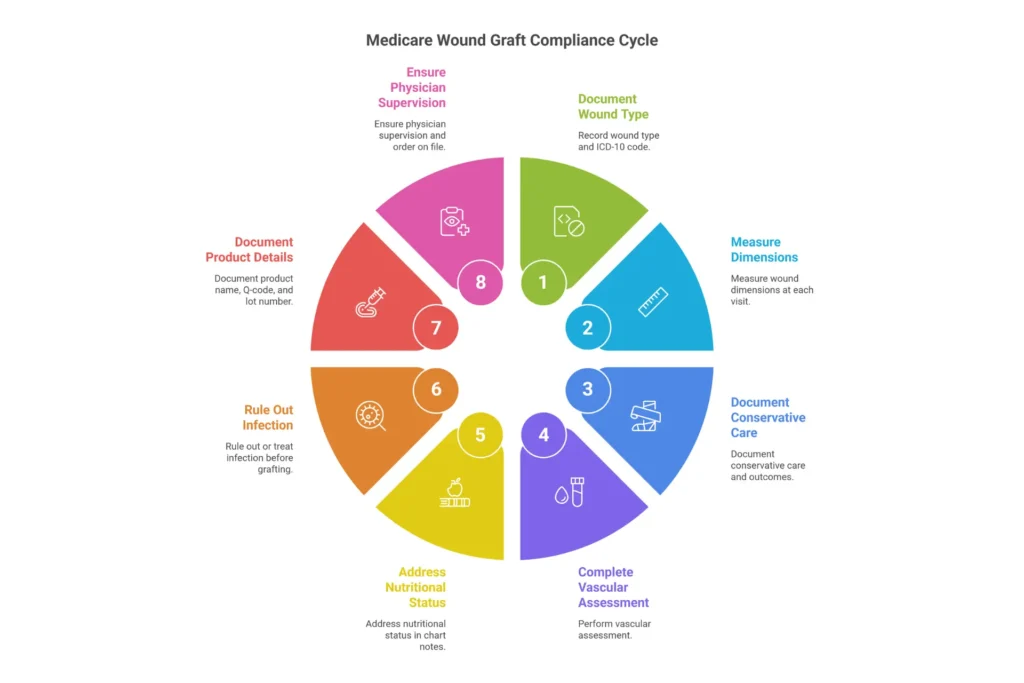
What LCD L33831 generally requires for coverage:
The foundational requirement is that the patient has a chronic wound — typically a diabetic foot ulcer (ICD-10: E11.621 or similar), a venous leg ulcer (I83.009), or a pressure injury (L89.xxx staging codes) — that has been treated with appropriate standard of care for at least four consecutive weeks without achieving 50% closure.
The LCD also requires:
- Adequate vascular supply confirmed (ABI ≥ 0.5 or toe pressure ≥ 30 mmHg for diabetic foot wounds)
- Wound infection controlled or absent at time of application
- Off-loading compliance documented for DFUs
- Compression therapy compliance for VLUs
- Nutritional status addressed
- Comorbidities managed (glycemic control documented for diabetics)
What changed in 2026: CMS’s final rule for skin substitutes restructured how products are categorized for payment. Under the 2026 policy, products are now classified into two payment categories under the OPPS: a high-cost category and a low-cost category, replacing the previous “pass-through” and “packaged” structure for many products. This has significant reimbursement implications depending on which products you’re using. Our Medicare wound care billing guide covers the 2026 final rule changes in more detail.
Critical billing note: LCD coverage does not guarantee reimbursement. A covered product applied to a covered wound type in a covered setting can still be denied if the documentation in the medical record doesn’t support the criteria above. This is where most practices bleed revenue.
Which Wound Graft Products Does Medicare Cover? The 2026 Product Guide
This is the section every wound care provider needs bookmarked, because the covered product list changes, Q-codes get reassigned, and products move between coverage categories.
Table 2: Medicare-Covered Wound Graft Products — Key 2026 Examples
| Product Name | Manufacturer | Product Type | Common Q-Code | Coverage Status | Primary Indication |
|---|---|---|---|---|---|
| EpiFix | MIMEDX | Dehydrated amniotic membrane | Q4131 | Covered | DFU, VLU, surgical wounds |
| AmnioFix | MIMEDX | Amniotic membrane (injectable/topical) | Q4186 | Covered | DFU, VLU |
| Grafix | Organogenesis | Cryopreserved placental membrane | Q4155 | Covered | DFU, VLU |
| Apligraf | Organogenesis | Bilayered cellular matrix | Q4101 | Covered | DFU, VLU |
| Dermagraft | Organogenesis | Dermal substitute | Q4106 | Covered | DFU |
| Oasis Wound Matrix | Smith & Nephew | Acellular ECM (porcine intestine) | Q4102 | Covered | DFU, VLU, partial thickness wounds |
| Kerecis Omega3 Wound | Kerecis | Fish skin (acellular) | Q4212 | Covered (verify) | DFU, VLU, burns |
| PuraPly Antimicrobial | Organogenesis | Collagen matrix + polyhexamethylene biguanide | Q4183 | Covered | Infected/at-risk DFU |
| Affinity | LifeNet Health | Amniotic allograft | Q4196 | Covered | DFU, VLU |
| TheraSkin | Stryker | Cryopreserved human skin allograft | Q4105 | Covered | DFU, VLU |
| AmnioBand | MTF Biologics | Amniotic membrane allograft | Q4130 | Covered | DFU, VLU |

Important caveats on this table: Q-codes are assigned annually by CMS. Some products share Q-codes within a category. Products listed as “covered” are subject to the medical necessity criteria above — coverage is not automatic. Always verify current Q-code assignments against the most recent CMS HCPCS update and confirm the product is on your MAC’s covered list before the first application.
Products not on the covered list cannot be billed to Medicare directly and require an Advance Beneficiary Notice (ABN) if the patient will be expected to pay out of pocket.
For a comprehensive overview of our verified graft program and which products we support, visit the EliteMedFinancials Wound Care Graft Products page.
Medical Necessity Documentation Requirements — What Survives an Audit
Here’s the uncomfortable truth about wound care graft billing: most of the practices that get hammered in OIG or RAC audits didn’t commit fraud. They simply had documentation gaps that made defensible claims indefensible on paper.
The documentation requirements for CTP claims are specific, and they need to be present in the medical record at the time of service — not reconstructed retroactively when you get a demand letter.
Table 3: Pre-Claim Documentation Checklist for Wound Care Grafts
| Documentation Element | What to Include | Common Failure Point |
|---|---|---|
| Wound type and etiology | ICD-10 code with specific wound location; confirm chronic wound criteria | Using unspecified codes (e.g., L89.90) instead of staged codes |
| Conservative treatment history | 4+ weeks of standard care with dates, wound measurements, products used | Vague entries like “wound care ongoing” without specifics |
| Wound measurement | Length × width × depth at each visit; photodocumentation recommended | Missing depth measurement; no before-after photos |
| Vascular assessment | ABI result with date; toe pressure for DFU if ABI borderline | Missing or outdated vascular studies (>12 months old) |
| Infection status | Clinical exam findings; culture results if applicable | No documentation that wound was infection-free prior to graft |
| Off-loading compliance (DFU) | Type of off-loading device, patient compliance note | Documented recommendation without documented compliance |
| Compression therapy (VLU) | Type, frequency, patient compliance | Same compliance documentation failure as DFU |
| Glycemic control (DFU) | Recent HbA1c; note on glycemic management | HbA1c >12% with no documentation of management plan |
| Product applied | Exact product name, lot number, Q-code, size applied | Generic descriptions without product-specific identifiers |
| Medical necessity rationale | Narrative explaining why standard care failed and CTP is appropriate | Boilerplate language that doesn’t reflect the specific patient |
| Physician attestation | Treating physician signature and credentials | Mid-level provider signing without supervising physician documentation per MAC rules |
The 4-week conservative care requirement is the single most frequently cited deficiency in post-payment reviews. “Conservative care” means documented wound care — debridement, appropriate dressings, off-loading, compression — not just the passage of time. If your records say “patient treated conservatively” without specific entries showing what was done, on which dates, and how the wound responded, you do not have documentation that will survive a Medicare review.
Need a deeper walkthrough of documentation standards? Our wound care billing guidelines page and our wound care billing and coding services team can audit your current documentation workflow.
Medicare Reimbursement Rates for Wound Grafts — 2026 Fee Schedule
One of the most common questions wound care practices ask us is: “How much does Medicare actually pay for wound grafts?”
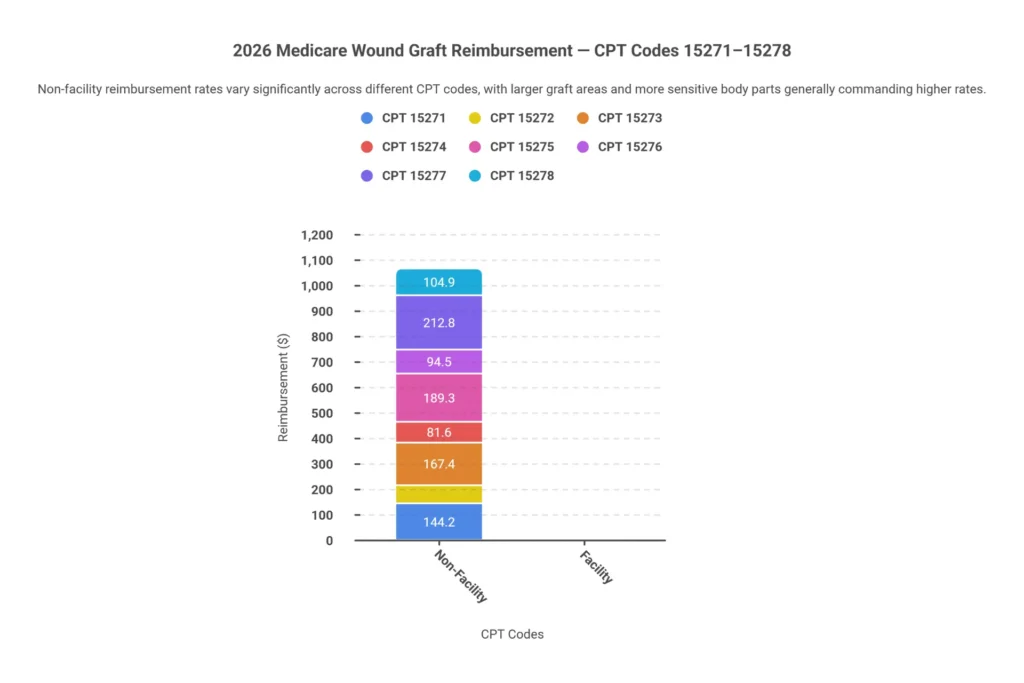
The answer has two parts: the application fee (CPT codes 15271–15278) and the product fee (Q-codes). Under the Physician Fee Schedule, Medicare reimburses the application procedure separately from the graft material itself. Under OPPS for hospital outpatient settings, the reimbursement structure differs — products may be bundled or separately billable depending on their payment category under the 2026 final rule.
CPT Code Range for Wound Graft Application:
- 15271 — Application of skin substitute graft, trunk/arms/legs; first 25 sq cm or less
- 15272 — Each additional 25 sq cm (add-on to 15271)
- 15273 — Application, trunk/arms/legs; first 25 sq cm or less (repeat application)
- 15274 — Each additional 25 sq cm (add-on to 15273)
- 15275 — Application, face/scalp/eyelids/mouth/neck/ears/orbits/genitalia/hands/feet/digits; first 25 sq cm or less
- 15276 — Each additional 25 sq cm (add-on to 15275)
- 15277 — Application, face/scalp/etc; first 25 sq cm or less (repeat application)
- 15278 — Each additional 25 sq cm (add-on to 15277)
Table 4: 2026 Medicare Reimbursement Rates — Wound Graft Application CPT Codes
| CPT Code | Description | Non-Facility Rate (approx.) | Facility Rate (approx.) | Global Period |
|---|---|---|---|---|
| 15271 | First application, trunk/arms/legs, ≤25 sq cm | $175–$210 | $95–$120 | 10 days |
| 15272 | Add-on per 25 sq cm | $55–$75 | $30–$45 | N/A (add-on) |
| 15273 | Repeat application, trunk/arms/legs, ≤25 sq cm | $155–$190 | $85–$110 | 10 days |
| 15274 | Repeat add-on per 25 sq cm | $50–$70 | $28–$42 | N/A (add-on) |
| 15275 | First application, face/hands/feet, ≤25 sq cm | $195–$235 | $110–$140 | 10 days |
| 15276 | Add-on per 25 sq cm, face/hands/feet | $60–$80 | $35–$50 | N/A (add-on) |
| 15277 | Repeat application, face/hands/feet, ≤25 sq cm | $170–$210 | $100–$130 | 10 days |
| 15278 | Repeat add-on per 25 sq cm | $55–$75 | $30–$45 | N/A (add-on) |
Rates reflect approximate 2026 Medicare PFS national averages. Actual payment varies by geographic locality adjustment. Verify current rates in the CMS Physician Fee Schedule Look-Up Tool.
Product reimbursement (Q-codes) is billed separately and varies significantly by product. High-cost products like Grafix or Apligraf can carry Q-code reimbursement ranging from several hundred to several thousand dollars per application, depending on the size applied and the payment category. This is where the 2026 CMS final rule matters most — products previously benefiting from pass-through payment status have transitioned to the new categorization structure, which in some cases reduced reimbursement.
For complete wound care billing codes including CPT, HCPCS, and ICD-10, our wound care billing codes guide is the most comprehensive reference we’ve published.
On modifiers: Getting modifiers right prevents a significant percentage of wound care graft denials. Key modifiers include:
- Modifier 59 (or the preferred XS, XP, XE, XU variants) — identifies distinct procedural services
- Modifier 76 — repeat procedure by same physician
- Modifier 77 — repeat procedure by different physician
Modifier 59 and its X-modifier variants are particularly important when billing debridement on the same day as graft application. Our medical coding services team reviews modifier application as part of every wound care coding audit we perform.
How a Clean IVR Process Eliminates Coverage Surprises Before They Happen
You can have the best wound care documentation in your state, the most medically appropriate product selection, and perfectly coded claims — and still watch reimbursement grind to a halt if you skip the insurance verification step.
The Insurance Verification and Real-time (IVR) eligibility check is not glamorous work. But in wound care graft billing, it is arguably the highest-value 15 minutes in your revenue cycle.
Here’s what a proper pre-graft IVR process should verify:
Coverage verification fundamentals:
- Confirm the patient has active Medicare Part B (not just Part A)
- Identify whether the patient has a Medicare Advantage plan and which one
- For MA plans: call the plan directly to verify wound care graft coverage, prior authorization requirements, and approved product list
- Check deductible status — a patient who hasn’t met their annual Part B deductible will owe the deductible before coinsurance kicks in
- Verify secondary insurance (Medigap, employer supplemental) to understand patient responsibility
Graft-specific verification steps:
- Confirm the specific product Q-code is covered under the patient’s plan
- Verify prior authorization is not required, or obtain it before scheduling
- Check how many prior applications are on record (some LCDs and MA plans cap the number of graft applications per wound episode)
- Confirm the billing provider is credentialed with Medicare and the MA plan
That last point trips up more practices than you’d think. A provider who isn’t properly enrolled with Medicare — or whose enrollment information is outdated — will have every claim rejected at the front end regardless of clinical quality. Our Medicare credentialing services team handles provider enrollment and re-validation to make sure you never lose revenue to an enrollment issue.
What happens when IVR reveals a problem: If verification shows a coverage issue — prior auth required, product not covered, patient in a benefit period that restricts graft billing — you have options. Issue an ABN if there’s a reasonable expectation Medicare will deny coverage and the patient may want to proceed privately. Document the ABN conversation. Get the patient’s signature. This protects both the practice and the patient.
The IVR process, done right, converts from a cost center into a revenue protection tool. Practices that skip it are essentially performing $1,000–$5,000 procedures on credit — hoping reimbursement follows. It often doesn’t.
What Happens When Graft Coverage Lapses — Understanding the 6-Year Audit Exposure Window
Here’s a scenario that plays out in wound care practices more than most providers realize: a product loses its Medicare coverage status, or a patient’s coverage changes mid-treatment, and claims continue to be submitted as if nothing changed. This isn’t always intentional. Product coverage status updates aren’t sent in certified mail. LCD revisions go into effect on specific dates. A provider focused on clinical care can miss a policy change that has billing implications.
The problem is that Medicare can look back up to 6 years when conducting post-payment reviews. Under the False Claims Act, the look-back window for fraud and overpayment can extend even longer. RAC (Recovery Audit Contractor) audits, ZPIC (Zone Program Integrity Contractor) reviews, and OIG investigations all operate within this window.
What does this mean practically?
A claim submitted correctly under coverage rules that were in effect in 2022 may be reviewed — and potentially recouped — in 2026 if a MAC conducts a complex review and determines the documentation was insufficient by current standards. This is technically called a “non-affirmation” — the auditor can’t confirm the claim met medical necessity requirements at the time of service based on what’s in the record.
Protecting your practice for the long game:
- Maintain complete wound care records for a minimum of 7 years (10 years in some states)
- Document every conservative treatment entry as if an auditor will read it
- Keep a running log of the coverage status of every product you use, with dates
- Conduct internal billing audits at least annually — our wound care billing audit services can identify exposure before CMS does
- Know your MAC’s probe and educate protocols; if you receive an Additional Documentation Request (ADR), respond completely and on time
When an overpayment demand arrives, providers have the right to self-disclose, repay voluntarily, or appeal. The appeal pathway runs through the MAC, then to the Qualified Independent Contractor (QIC), then to an OMHA Administrative Law Judge (ALJ), then to the Medicare Appeals Council, then to the Departmental Appeals Board (DAB), and finally to Federal District Court if necessary. Most meritorious appeals that survive to the ALJ level are resolved favorably — but getting there requires rock-solid documentation.
Our denial management and AR recovery services actively manage open audit responses and overpayment appeals for wound care clients.
Common Reasons Medicare Denies Wound Graft Claims — And How to Appeal
Denial management in wound care graft billing is a specialty within a specialty. The claim submission process involves more variables than almost any other outpatient service: product identity, application site, wound type, prior application history, documentation completeness, modifier accuracy, and MAC-specific coverage criteria. Each variable is a potential denial point.
Table 5: Top Wound Graft Denial Codes — Quick Reference
| CARC Code | RARC Code | Denial Reason | Most Common Cause | Fix |
|---|---|---|---|---|
| CO-50 | N362 | Not medically necessary | Documentation doesn’t support LCD criteria | Submit complete medical records with conservative care history on appeal |
| CO-97 | N401 | Benefit included in global period | Graft billed within global period of prior procedure | Use modifier 79 (unrelated procedure) if clinically distinct; or rebill correctly |
| CO-96 | N425 | Non-covered charge | Product Q-code not on covered list or covered at zero | Verify product coverage status; issue ABN if applicable |
| PR-B7 | — | Patient ineligible for benefit | MA plan prior auth not obtained; benefit period restriction | Obtain PA before next application; bill patient with ABN if Medicare won’t cover |
| CO-4 | — | Incorrect modifier | Modifier 59/XS/XP/XE/XU applied incorrectly | Review modifier guidance; rebill with correct modifier |
The appeals process for wound graft denials:
Level 1 — MAC Redetermination: Submit within 120 days of the initial denial notice. Include all medical records, the LCD you believe the claim satisfies, a letter of medical necessity from the treating physician, and a point-by-point rebuttal of the denial rationale. Many well-documented claims are recovered here.
Level 2 — QIC Reconsideration: If Level 1 fails, you have 180 days to file with the Qualified Independent Contractor. This is a fresh review by an entity independent of the MAC. Include everything from Level 1 plus any additional clinical evidence.
Level 3 — OMHA ALJ Hearing: Only available if the amount in controversy exceeds the annual threshold (check current CMS threshold). ALJ decisions take time — often 12–24 months in the current queue — but overturn rates for well-documented cases are meaningful.
Level 4 — Medicare Appeals Council: Reviews ALJ decisions. Less commonly reached but important for systemic issues.
Level 5 — Federal District Court: For cases above the jurisdictional minimum. Rare for single claims.
The most important thing to understand about the appeals process is that it works — if your documentation is solid. Most practices leave significant money on the table by not appealing the denials they can win. At EliteMedFinancials, our wound care billing specialists track open appeals, manage deadlines, and prepare the appeal packages that recover revenue providers thought was lost.
For help managing wound care billing denials and AR, our team offers a free billing audit to identify your current denial patterns and recovery opportunities.

Special Considerations: Medicare Advantage Plans, Prior Authorization, and the 2026 Landscape
Medicare Advantage deserves its own section because the coverage experience is so materially different from Original Medicare, and the number of Medicare patients enrolled in MA plans now exceeds 50% of all Medicare beneficiaries.
Under the Consolidated Appropriations Act of 2021 and subsequent CMS rulemaking, MA plans were given greater flexibility in implementing prior authorization for wound care services — and they’ve used it. As of 2026, virtually every major MA plan (UnitedHealthcare, Humana, Aetna, Cigna, Blue Cross, Centene/WellCare) requires prior authorization for CTP/wound graft applications.
What this means operationally:
- Your PA request must include the same documentation a Medicare LCD would require — wound measurements, conservative care history, vascular studies, product selection rationale
- PA approval is product-specific; approval for EpiFix does not automatically transfer to Grafix if you substitute
- PA has a validity period; if the approved application window passes and you haven’t applied the graft, you need a new PA
- Denial of PA is not the end — you can file an expedited appeal within the MA plan’s own process, or request a peer-to-peer review with the MA plan’s medical director
The practical implication for wound care practices: your pre-service workflow for MA patients needs to be as robust as your post-service billing workflow. A five-minute PA check before scheduling can prevent a $3,000 claim from sitting unresolved in AR for six months.
Also relevant for 2026: CMS finalized new rules requiring MA plans to process PA requests more quickly and to align PA criteria more closely with Original Medicare coverage policies. Practices experiencing systematic MA denials for wound grafts that Medicare would cover should document these denials and escalate — CMS’s complaint processes for MA plans are underutilized but available.
Voice Search: Medicare Wound Care Graft Questions — Answered Directly
The following questions reflect how patients, caregivers, and providers actually ask about Medicare wound graft coverage.
How much does Medicare pay for a skin graft?
Medicare reimburses wound graft application through CPT codes 15271–15278, with payment ranging from approximately $85 to $235 for the application procedure depending on the body location and facility setting. The graft product itself is billed separately through HCPCS Q-codes and can add hundreds to thousands of dollars in reimbursement depending on the product, size, and payment category. The patient is responsible for the standard 20% Part B coinsurance after the annual deductible is met.
What is the skin substitute fee schedule for 2026?
CMS updated the skin substitute payment methodology in its 2026 final rule, establishing two payment categories under the Outpatient Prospective Payment System: a high-cost category and a low-cost category. Products assigned to each category are updated annually on the CMS website. Under the Physician Fee Schedule, application codes 15271–15278 are valued at approximately $85–$235 nationally. Q-code product payments are published in the annual PFS and OPPS rules.
What is the final rule for skin substitutes in 2026?
CMS’s 2026 final rule reclassified skin substitute products (cellular and tissue-based products) from the previous pass-through and packaged payment structure under OPPS into two consolidated payment categories. The rule also tightened LCD alignment requirements and clarified that products must appear on the CMS-published covered product list to be separately billable. Practices that were billing transitional pass-through products need to verify whether those products have been assigned to the new high-cost or low-cost categories.
Does Medicare cover wound care at home?
Medicare Part A covers wound care provided by a Medicare-certified home health agency, including skilled nursing visits for wound treatment, as part of the home health benefit — provided the patient meets homebound criteria and has a physician order. The home health agency bills under a 30-day payment period system. Wound graft products are generally not separately billable under the home health episode; they are considered included in the bundled payment. Some products may be covered separately under specific limited circumstances — verify with the HHA’s billing team.
What are the most common reasons Medicare denies wound graft claims?
The most frequent denial reasons are insufficient medical necessity documentation (particularly missing conservative care history), using a product that is not on the covered list, billing outside the applicable LCD’s diagnostic criteria, and failure to obtain prior authorization for Medicare Advantage patients. Modifier errors and global period conflicts are also common. Most denials are appealable and, when documentation is complete, recoverable.
How do wound care graft coverage rules differ between Medicare and Medicare Advantage?
Original Medicare follows LCD criteria published by the applicable MAC for the provider’s state. Medicare Advantage plans must cover the same wound graft services that Medicare covers but can impose prior authorization requirements, use a restricted product formulary, and require network referrals that Original Medicare does not. This means a patient with an MA plan may face more barriers to coverage even though the underlying Medicare benefit is the same.
Frequently Asked Questions: Medicare Wound Care Graft Coverage
Does Medicare cover wound grafts for diabetic foot ulcers?
Yes. Diabetic foot ulcers are one of the primary covered indications under LCD L33831. Medicare will cover wound graft application for a DFU coded E11.621 (or the applicable E11.6×1 code based on laterality and complication) when the wound has been treated with conservative care including adequate off-loading and local wound care for at least four weeks without achieving adequate healing. Vascular sufficiency and glycemic management must be documented.
How many wound graft applications will Medicare cover?
Medicare does not set a hard limit on the number of applications per wound, but it does require that each application be medically necessary. The LCD requires documented wound response — typically evidence that the wound is progressing toward healing — to justify continued applications. Some MACs look at the pattern of applications per wound and may request records if the number appears unusually high. A wound that is worsening despite multiple CTP applications should prompt documentation explaining the clinical rationale for continued treatment.
What is an ABN and when do I need one for wound grafts?
An Advance Beneficiary Notice of Noncoverage (ABN) is a written notice given to a Medicare beneficiary before furnishing a service that you expect Medicare may deny. You must issue an ABN when there is a genuine question whether Medicare will cover the specific graft for this patient — for example, if the conservative care period is borderline, the product is on a covered list but the indication is outside typical parameters, or you know the patient’s MA plan has a restrictive formulary. A valid ABN shifts financial liability to the patient for that service. You cannot issue an ABN for services that are categorically excluded from Medicare (Medicare never covers them regardless of circumstances).
Can I bill Medicare for wound graft application and debridement on the same day?
Yes, but modifier usage is critical. Debridement performed at the same visit as graft application should be coded with the appropriate modifier to identify it as a distinct service (Modifier 59 or preferred X-modifiers: XS, XP, XE, or XU). Without the correct modifier, Medicare will bundle the debridement into the graft application fee and pay only the graft code. However, documentation must support that the debridement was clinically distinct from the graft preparation and medically necessary in its own right.
What ICD-10 codes are used for wound graft claims?
The most commonly used ICD-10 codes for wound graft claims include: E11.621 (Type 2 diabetes with foot ulcer), E11.622 (Type 2 diabetes with other skin ulcer), I83.009 (Varicose veins with ulcer, unspecified), L89.xxx staging codes for pressure injuries, and L97.xxx codes for non-pressure chronic skin ulcers. Using unspecified codes when specific codes are available is a common audit flag — code to the highest level of specificity documented in the record.
How do RAC audits target wound care graft claims?
Recovery Audit Contractors use automated algorithms to flag claims that show patterns associated with overpayment risk. In wound care, common RAC triggers include: high volume of graft applications per provider or per patient, repeat applications on the same wound without documented healing progress, billing the same product Q-code multiple times without appropriate time between applications, and claims where the procedure code doesn’t match the documented wound type. RAC audits can result in complex medical reviews requesting up to 80% of a sample of claims. Maintain complete, defensible records for every graft claim going back six years.
Do I need Medicare credentialing to bill wound care grafts?
Yes. To bill Medicare for any service including wound graft applications, the treating provider must be enrolled in Medicare as a participating or non-participating provider and must have a valid NPI linked to their Medicare enrollment. The practice location (billing address) must also be enrolled. Changes in practice location, group affiliation, or ownership require updated enrollment. Lapses in enrollment result in claim rejections at the front end, not just denials — and retroactive enrollment is not available in most cases. Our Medicare credentialing team manages the enrollment process from initial application through approval and handles re-validations on schedule.
Table 6: Medicare Wound Care Graft Coverage — Quick Reference Summary
| Category | Key Details |
|---|---|
| Governing policy | LCD L33831 (or jurisdiction equivalent); Article A59518 |
| Primary covered indications | DFU, VLU, pressure injuries (non-healing, post 4-week conservative care) |
| Application CPT codes | 15271, 15272, 15273, 15274, 15275, 15276, 15277, 15278 |
| Product billing | HCPCS Q-codes (product-specific; verify annually) |
| Covered settings | Physician office, HOPD, ASC; limited in SNF/home health |
| Patient cost-sharing | 20% coinsurance + Part B deductible |
| Prior authorization | Required for Medicare Advantage; generally not required for Original Medicare |
| Appeal levels | MAC → QIC → ALJ (OMHA) → Medicare Appeals Council → DAB → Federal Court |
| Audit look-back | 6 years (False Claims Act: up to 10 years) |
| 2026 key change | CMS final rule: CTP products reclassified into high-cost/low-cost payment categories |
Conclusion: Getting Medicare Wound Care Graft Coverage Right in 2026
Medicare does cover wound care grafts — but “covered” is not the same as “reimbursed.” The gap between those two words is where wound care practices lose tens of thousands of dollars every year.
The practices that consistently get paid for wound graft services share a common set of habits: they document conservative care in detail, they verify coverage before applying the graft, they code to the highest specificity, they use the right modifiers, they check Q-code assignments annually, and they appeal the denials they should win. None of these habits require more clinical sophistication. They require billing infrastructure that’s built for the complexity of wound care.
If you’re not getting paid what you should be for wound care graft services — or if you’re worried about audit exposure from past claims — the best first step is a billing audit. Not a general billing audit, but a wound care–specific review that looks at documentation completeness, coding accuracy, denial patterns, and AR aging on wound care claims.
That’s exactly what EliteMedFinancials does.
🔵 Ready to Maximize Your Wound Care Graft Reimbursement?
Check Your Wound Care Coverage — Free Eligibility Verification
Our wound care billing specialists verify Medicare and Medicare Advantage coverage before your first graft application — so you know exactly what will be reimbursed before you pick up the product.
🟢 Interested in Our Verified Wound Care Graft Program?
Explore Wound Care Graft Products
We work with practices to pair the right covered graft product with complete billing support — so the clinical and revenue cycle sides of graft treatment work together seamlessly.
🔴 Dealing With Denied or Underpaid Wound Care Claims?
Schedule a Free Wound Care Billing Audit
We’ll review your current wound care billing, identify where revenue is leaking, and give you a clear action plan — at no cost and no obligation.
EliteMedFinancials provides end-to-end revenue cycle management, medical billing, medical coding, credentialing, and wound care–specific billing services for practices across the United States. Our team understands wound care billing from the clinical documentation side to the final payment posting — and we’re ready to help your practice get paid for every graft you apply.
External References:
- CMS Local Coverage Determinations Database — Official source for L33831 and related LCD policies
- CMS 2026 Hospital Outpatient Prospective Payment System Final Rule — 2026 skin substitute payment category changes
Related reading:
- Wound Care Billing Codes: Complete CPT, HCPCS, and ICD-10 Reference
- Medicare Wound Care Billing Guide
- How to Outsource Wound Care Billing — A Practical Guide
- Outpatient Wound Care Billing
- Amniotic Membrane Graft Billing: CPT Codes and Q-Codes
- Wound Care Billing FAQ
- Revenue Cycle Management for Healthcare Providers