
If you’ve ever stared at a CO-97 denial on a wound care claim and thought, “But I documented everything” — you already know this specialty isn’t like anything else in medical billing. Wound care denial rates average 15–30% with general RCM firms. That’s nearly triple the Medicare benchmark. One wrong depth notation, one missed dual ICD-10 on a diabetic ulcer, one compression code bundled with debridement on the same limb — and suddenly you’re reworking claims instead of seeing patients.
This FAQ hub was written to fix that. Not with vague “best practices,” but with the actual rules: specific CPT codes, MAC article numbers, modifier logic, 2026 rate updates, and documentation language that holds up under audit. Every section below answers a real question wound care providers and billing teams ask repeatedly. Take what you need.
Table of Contents
What Is Wound Care Billing?
Here’s the definition worth knowing: wound care billing is the complete administrative process of converting clinical wound treatments into standardized CPT, ICD-10, and HCPCS codes — then submitting those claims to Medicare, Medicaid, and commercial payers for reimbursement. It covers debridement, skin substitute application, negative pressure wound therapy (NPWT), compression, hyperbaric oxygen, and the evaluation and management services that happen alongside them.
But that’s the simple version. What actually makes wound care billing different from general billing is the technical architecture underneath it.
The CPT selection in wound care isn’t about the procedure name. It’s about what tissue was physically removed — subcutaneous fat (11042), muscle or fascia (11043), bone (11044) — not what was visible in the wound. Billing 11044 because “bone was probed” without documenting bone fragments excised is one of the top audit targets in OIG’s 2025 Work Plan. Documentation-to-code translation here is literal.
On top of that, diabetic foot ulcers require dual ICD-10 coding — E11.621 linked to L97.5xx (with the right laterality and depth extension). Miss the pairing, and 40% of those claims auto-deny. Add NCCI bundling rules, MAC-specific LCDs that vary by ZIP code, and the 2026 PFS Final Rule that just reclassified skin substitutes as flat-rate incident-to supplies at ~$127.14 per square centimeter — and you understand why general billing staff consistently struggle here.
Wound care billing involves two distinct functions. Coding is interpretive: assigning CPT and ICD-10 from clinical documentation following MAC LCDs like Noridian A58565 (Revision 11, effective January 1, 2026). Billing is operational: submitting via CMS-1500, applying modifiers like XS for separate anatomic sites, scrubbing NCCI edits, tracking frequency limits, and managing the denial cycle. Both functions require wound-specific expertise. A CPC who hasn’t worked wound care will miss add-on codes. A biller unfamiliar with the 12/360 frequency rule will generate auto-denials before they realize what happened.
For practices that want to understand the complete CPT landscape before going further, our wound care billing codes reference breaks down every code family with 2026 rates and MUE limits.
Can You Bill for Wound Care Services?
Yes — but the specifics matter more than the yes.
Billability in wound care depends on four things: what service was performed, how it was documented, who performed it, and where. Get all four right and you get paid. Miss one and you get a denial you’ll spend two weeks chasing.
What IS Billable (When Documented Correctly)
Selective debridement of devitalized tissue using scissors, curettes, or waterjet falls under CPT 97597 (first 20 sq cm) and 97598 (each additional 20 sq cm). These are payable in physician offices, hospital outpatient departments, and skilled nursing facilities when you can document the necrotic tissue percentage and instruments used.
Surgical debridement — the codes most practices underuse or mis-code — runs 11042 through 11047, organized by depth. Subcutaneous tissue removal bills as 11042. Muscle or fascia is 11043. Bone is 11044. Each has add-on codes (+11045, +11046, +11047) for additional surface area. These are where significant reimbursement lives for wound care specialists, and where documentation failures are most costly.
Skin substitute application (CPT 15271–15278) with Q41xx HCPCS supply codes is billable — but since January 1, 2026, skin substitutes are reimbursed at a flat ~$127.14 per sq cm rather than ASP+6%. This is a fundamental profitability shift that every wound care practice needs to account for. Product selection now directly determines your margin.
NPWT codes (97605–97608) are billable with documented pressure settings (typically 125mmHg), drainage characteristics, and wound dimensions. Compression wraps — 29580 for Unna boot, 29581 for multilayer — are separately billable, with one critical catch covered below.
E/M codes (99202–99215) on the same day as a procedure require modifier 25, but only if there’s a significant, separately identifiable reason for the visit beyond routine wound check. A new infection requiring antibiotic management qualifies. Just “wound check before dressing” does not.
What Is NOT Separately Billable
Routine dressing changes are bundled into debridement codes. CMS Article A55818 (Palmetto) is explicit about this, and most MAC articles follow the same logic. If all you’re doing is changing a dressing with no skilled debridement, you cannot bill 97597 separately.
CPT 97602 (non-selective debridement) carries Status B in physician offices — meaning it’s non-payable in POS 11. It’s payable in SNF and home health settings, but routinely billed in office, it’ll deny every time. This is one of the most common signs a practice needs specialized wound care billing support.
Services during a global surgical period require modifiers (-58 staged, -78 complication, -79 unrelated) or they’re bundled by default. And CPT 97597 billed on the same wound as 11042 on the same day has an NCCI indicator of 0 — meaning no modifier can unbundle it. Accept the bundling; don’t try to bypass it.
Provider Types Who Can Bill for Wound Care
MDs and DOs can bill all wound care codes within scope. Nurse Practitioners and PAs bill independently at 85% of the physician fee schedule rate. Physical therapists can bill 97597 and 97602 with the GP modifier under a therapy Plan of Care. Occupational therapists use the GO modifier. Podiatrists bill all wound care codes plus Q7/Q8/Q9 for routine foot care situations. Registered nurses cannot bill independently — only incident-to.
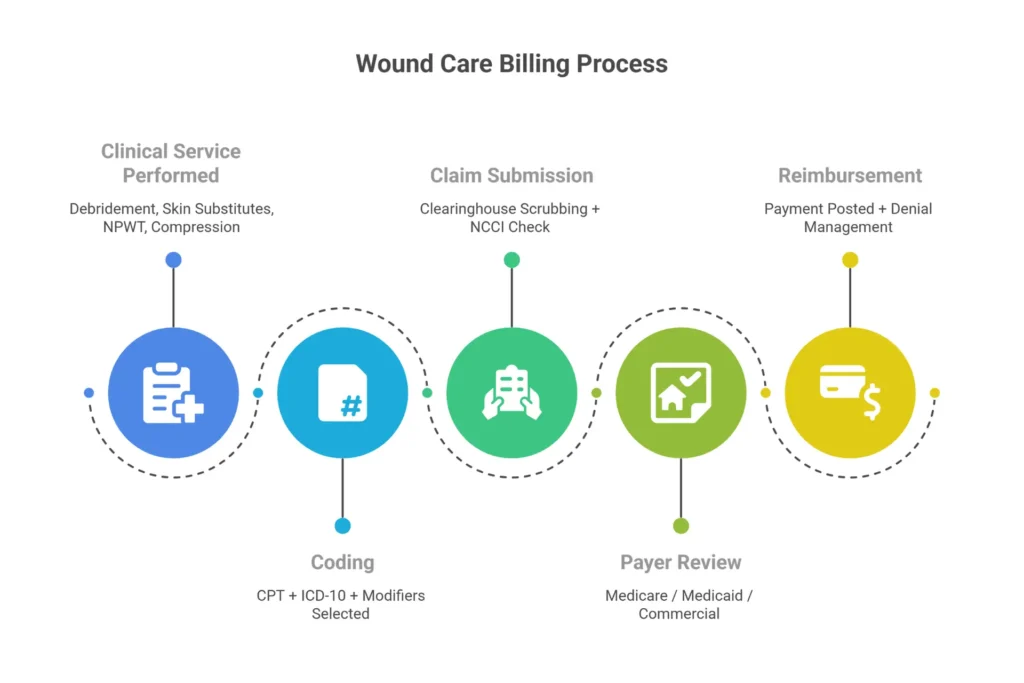
How Do You Bill for Wound Care? Step-by-Step
Most billing errors in wound care happen between the clinical encounter and the claim submission. The workflow below is the one that consistently produces clean claims.
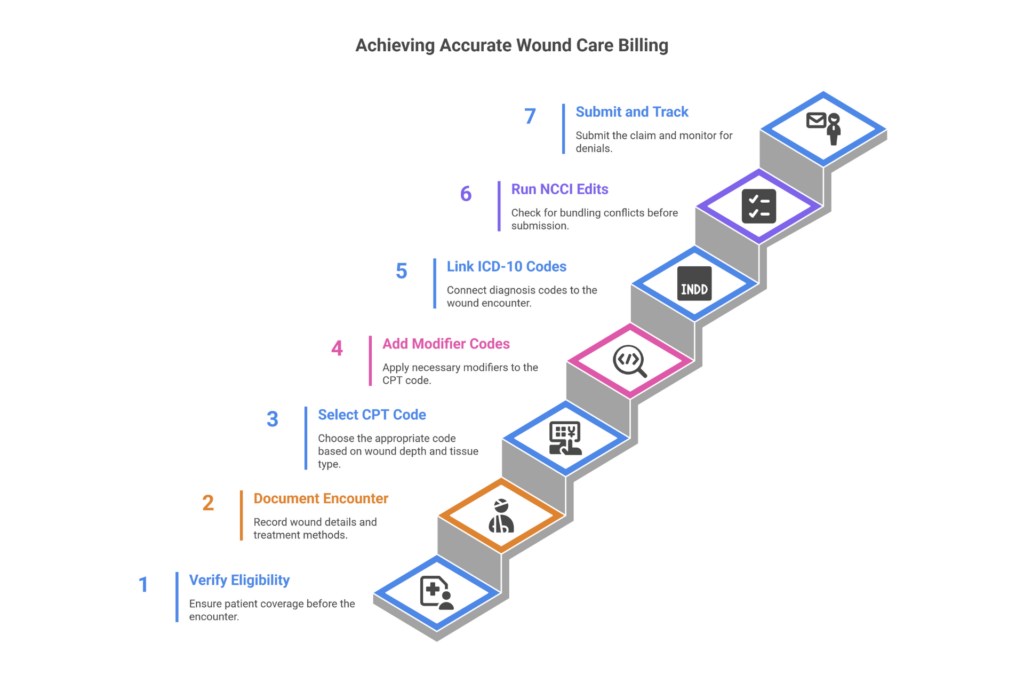
Step 1 — Document the 5 pillars before you touch a code. Every wound care note must contain: anatomic location with laterality (“right heel,” not just “foot”), measurements in cm (L×W×D), tissue composition percentages (60% slough, 30% granulation, 10% eschar), exudate type and amount, and periwound status including any tunneling by clock method. If the note doesn’t have these five elements, the coder is guessing — and guessing triggers denials.
Step 2 — Select CPT codes by the deepest tissue removed, not the wound depth. This is the rule that separates accurate wound care coding from educated guessing. If bone was exposed but only subcutaneous fat was excised, the correct code is 11042, not 11044. The clinical note must say “subcutaneous tissue debrided to bleeding margins” for 11042, or “bone fragments excised using rongeur” for 11044. “Bone visible” without removal documentation means 11042.
For multiple wounds at the same depth, sum the surface areas and bill one primary with add-ons. Three 15 cm² subcutaneous wounds equal 45 cm² total — that’s 11042 + 11045 × 2. For different-depth wounds, bill the deepest as primary and shallower wounds as separate line items with modifier XS (separate structure).
Step 3 — Assign ICD-10 with specificity. Diabetic foot ulcers need E11.621 (Type 2 DM with ulcer) plus the appropriate L97.5xx code with laterality and depth. Single-code submissions for DFUs deny at approximately 40%. Every MAC’s Group 1 covered list — Noridian A58565 has 1,173 codes — defines what ICD-10 combinations qualify for coverage. If your diagnosis isn’t on the Group 1 list, you need documented complicating circumstances or an ABN before treatment.
Step 4 — Apply modifiers correctly. XS (separate structure) is the right modifier for different anatomic sites — use it instead of 59 wherever it fits; it’s more specific and less audit-prone. Modifier 25 separates a significant E/M from a same-day procedure. RT/LT establish laterality and must match your ICD-10. GP and GO flag therapy services for PT/OT billing.
Step 5 — Scrub NCCI edits before submission. The two most commonly missed edits: 97597 + 11042 on the same wound (indicator 0 — never bypass) and compression + debridement on the same limb (Chapter 4G, indicator 1 — bypass with XS for different limbs). MUE limits apply: 11042 and 97597 each max at 4 units per day.
Step 6 — Complete CMS-1500 accurately. Box 21 contains your diagnosis pointers. Box 24E links each CPT to the correct diagnosis pointer. Box 24D holds your modifiers. The POS code matters: 11043 and 11044 are facility-only codes — they shouldn’t appear on claims from POS 11 offices.
Step 7 — Manage denials with documentation, not hope. CO-97 (bundled/necessity) accounts for roughly 40% of wound care denials. Level 1 Redetermination to the MAC must be filed within 120 days of the EOB, and your appeal packet needs the full clinical note, 30-day wound trajectory documentation, and the LCD Group 1 ICD-10 codes. Practices that send appeals with documentation win 65% of the time. Those that send appeals without documentation win 20%.
If your team is spending more time on denial rework than on clean submissions, that’s a workflow problem with a measurable cost. Our wound care billing specialists handle pre-submission claim review — catching the modifier errors and NCCI violations before they generate CO-97s.
What CPT Codes Are Used for Wound Care Billing?
The full wound care CPT landscape organizes into four families. Here’s what matters for daily billing decisions.
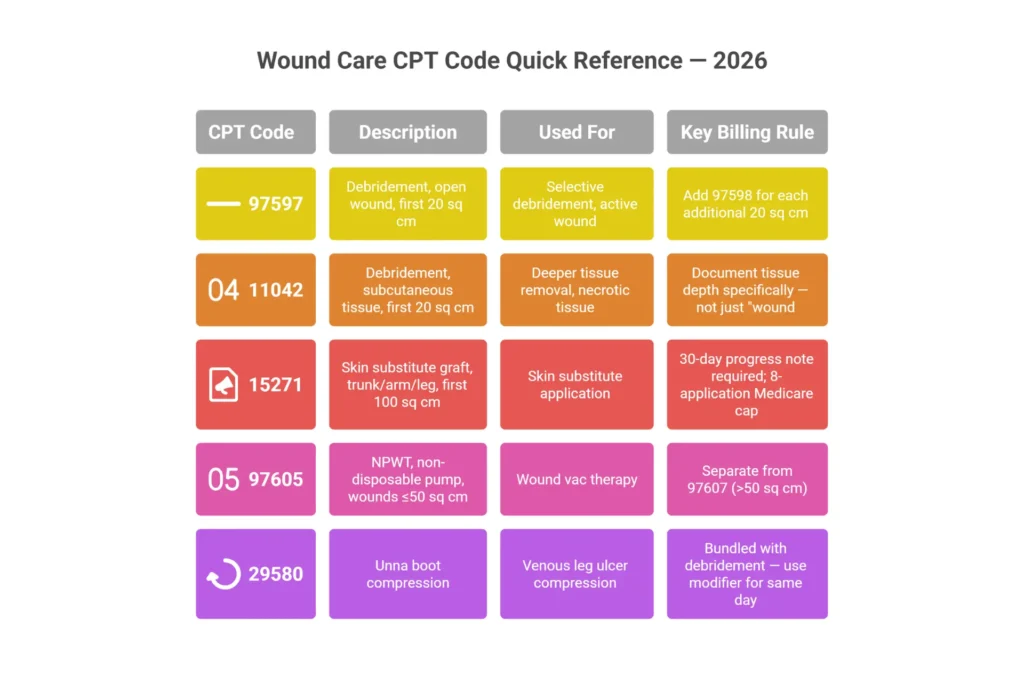
Active Wound Care Management (Non-Surgical): 97597 is selective debridement for the first 20 sq cm — document necrotic tissue percentage and instruments used. MUE is 4 units per day. Rate is approximately $85–$108 non-facility. Add-on 97598 covers each additional 20 sq cm. Status B code 97602 is non-selective — payable in SNF and home health only, non-payable in office settings.
Surgical Debridement by Depth: This is where the real complexity lives. 11042 covers subcutaneous tissue (first 20 sq cm), approximately $145–$250 non-facility. 11043 is muscle/fascia, approximately $350. 11044 is bone, approximately $450 — and must document bone removed, not just visible. Add-ons +11045, +11046, +11047 cover additional 20 sq cm increments. Important: 11043 and 11044 are facility-only codes. They cannot be billed in POS 11.
Skin Substitutes (15271–15278): The 2026 CMS rule change here is significant. All cellular and tissue-based products (CTPs) are now reimbursed at a flat rate of approximately $127.14 per sq cm as incident-to supplies, replacing the prior ASP+6% model. This means high-cost biologics that previously reimbursed at $400+ per sq cm are now at the same flat rate as economical alternatives. Product acquisition cost now directly determines profitability. The 8-application-per-12–16-week frequency limit remains.
NPWT (97605–97608): 97605 covers non-disposable equipment ≤50 sq cm. 97606 covers non-disposable >50 sq cm. 97607 and 97608 cover disposable equipment. Document pressure settings at every visit (125mmHg is standard). MUE is 1 unit per day. Compression codes 29580 (Unna boot) and 29581 (multilayer compression) are separately billable when documented with gradient pressure — but are bundled with same-limb debridement per NCCI Chapter 4G.
For a complete reference with 2026 Medicare rates and MUE limits for every code, the wound care billing codes page has the full breakdown. You can also see how coding decisions connect to compliance requirements in our wound care billing and coding services overview.
Is Wound Care Covered by Insurance?
Most wound care IS covered. The better question is whether it’s covered the way you’ve documented it, and that’s where practices consistently lose money.
Medicare Part B covers outpatient wound care at 80% after the $283 annual deductible (2026). The coverage triggers are medical necessity documentation: 30 days of failed conservative care before advanced therapies, ICD-10 codes from your MAC’s Group 1 list, and measurable healing progress (≥20% surface area reduction per 4 weeks, targeting 50% reduction by week 4). A wound that’s showing less than 1 cm of total improvement over 30 days is documented as “not improving” under LCD language — and that triggers review.
Advanced therapies have specific rules. Skin substitutes require prior authorization from most Medicare Advantage plans (about 90% of them), with a cap of 8 applications per 12–16 weeks under traditional Medicare. NPWT covers a 60-day initial period plus one 60-day extension with documentation. HBOT follows NCD 20.29 and covers up to 30 sessions initially plus 30-day extension for diabetic foot ulcers meeting Wagner grade 3 criteria.
Medicare Advantage must cover Part B-equivalent services but layers on stricter utilization management — prior auth requirements, tighter application caps (often 4 vs. Medicare’s 8), and reimbursement running 20–30% below traditional Medicare rates. MA plans deny at approximately 35% when 30-day conservative care logs are missing.
Commercial insurance (Aetna, UHC, BCBS) typically reimburses at 150% of Medicare and covers most wound care, but prior authorization requirements vary by payer. UHC requires four failed standard care attempts before skin substitute coverage. Aetna requires a 14-day NPWT trial. BCBS generally wants Wagner grade 3+ for HBOT. Know your payer mix; the PA requirements differ meaningfully.
What’s not covered: cosmetic wound care, services during a global period without appropriate modifiers, non-FDA-approved skin substitutes, and services after frequency limits are hit without a valid ABN on file.
A note on ABNs: When a service is likely to deny — frequency exceeded, non-Group 1 ICD-10, 9th skin substitute application — you must issue CMS Form CMS-R-131 before treatment. GA modifier (ABN on file), GY (statutory exclusion), GZ (no ABN, likely denial). No ABN means the provider writes off, regardless of outcome.
For providers wanting to understand the Medicare-specific requirements in depth, the Medicare wound care billing guide covers MAC-specific LCD requirements and what Noridian A58565 Revision 11 changed effective January 2026.
Is Wound Care Considered Outpatient? Does Setting Matter?
Setting matters enormously — not just for regulatory classification but for how much you actually get paid.
Yes, wound care is generally classified as outpatient when the patient isn’t admitted as an inpatient. But “outpatient” covers several different billing environments, each with its own rules.
Physician office (POS 11) is the most common setting. You bill at the non-facility rate, which bundles professional fee and overhead. Most wound care CPTs are payable here — but 11043 and 11044 are not. And CPT 97602 is Status B (non-payable). The 10-day global surgical period for 97597 and 29580 bundles routine follow-up.
Hospital outpatient (POS 22) changes the financial picture dramatically. You split-bill: professional fee on CMS-1500 and facility fee on UB-04. All CPTs are payable, including 11043 and 11044. The facility APC payment can turn a $85 code into $85 (professional) + $1,200 (APC) — a 15-fold total payment increase. HOPD isn’t the right setting for everyone, but practices seeing complex surgical cases should understand the revenue difference.
Skilled nursing facility (POS 31) has consolidated billing, which means most wound care services are bundled into the SNF per-diem RUG-IV rate. The carve-outs that can be billed separately under Part B: physician E/M codes (99307–99310) and surgical debridement (11042–11047). Routine wound care — dressing changes, standard debridement — is not separately billable in SNF Part A.
Home health (POS 12) bundles routine wound care into the 30-day HH PPS episode payment. Surgical debridement (11042–11047) can be billed separately under Part B by the ordering physician or NP. Homebound status must be documented.
Telehealth (POS 02/10): E/M codes 99202–99215 and wound photo triage code G0389 are telehealth-eligible under post-PHE permanent rules. Debridement cannot be performed or billed via telehealth — it requires hands-on in-person care. When using telehealth for wound assessment, document video wound measurement (patient-guided with ruler) and use modifiers GT or 95.
What Are the Medicare Rules for Wound Care Billing?
Medicare wound care rules live in three places: NCDs (national), LCDs (regional by MAC), and operational billing articles. Understanding which ones apply to your practice depends on your geographic jurisdiction.
Key MAC Articles by Jurisdiction:
Noridian Healthcare Solutions (JE, JF, JH — Western states) issues Article A58565, Revision 11 (effective January 1, 2026). This is the most recently updated major wound care billing article, and it matters if Noridian is your MAC. Revision 11 clarifies that 97597 and the surgical debridement codes 11042–11047 are mutually exclusive for the same wound on the same day — you can’t bill both on wound A. It also adds hyperkeratosis documentation requirements and links to LCD L38902.
Palmetto GBA (JJ, JM) governs under Article A55818, which has approximately 900 Group 1 covered ICD-10 codes and stricter documentation standards for venous leg ulcer compression.
CGS Administrators (J15) follows Article A55909, with around 950 Group 1 codes and particularly strong emphasis on 30-day conservative care failure documentation before NPWT.
Medical necessity requirements across all MACs include:
- Wound measurements (L×W×D in cm) at every visit
- Tissue type percentages
- 30 consecutive days of documented failed conservative care before advanced therapies
- Demonstrated healing trajectory: ≥20% surface area reduction per 4 weeks
- If healing has stalled: documented change in treatment plan explaining why care continues
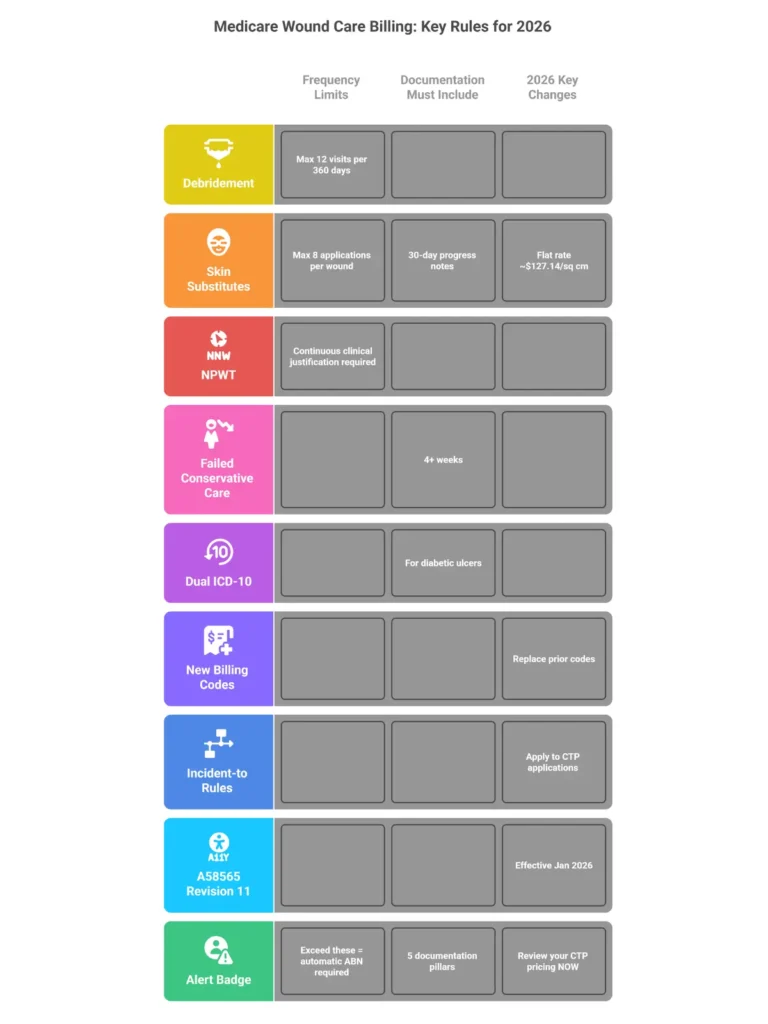
Frequency limits: The 12/360 rule caps debridement (97597–11047) at 12 sessions per 360 days. Skin substitutes max at 8 applications per 12–16 weeks. NPWT covers 60 days initial + 60-day extension with documentation. Exceeding limits without an ABN on file means the provider absorbs the denial.
The 2026 skin substitute change is the most significant reimbursement shift in wound care in years. Effective January 1, 2026, all CTPs (cellular and tissue-based products) billed via Q41xx codes are reimbursed at a single flat rate — approximately $127.14 per sq cm — across all settings. The previous ASP+6% model created wide variability ($400+ for some biologics). Under 2026 rules, the product you choose must have an acquisition cost below $127.14/sq cm to be financially viable. This is not a minor adjustment — practices with high skin substitute volume are looking at 60–90% profitability reductions if they don’t adapt their formulary.
The OIG’s 2025 Work Plan flagged wound care as a high-priority audit target after identifying $1.8 billion in potentially improper skin substitute payments. CERT data shows wound care documentation error rates around 25% — nearly three times the Medicare average of 9%. Targeted Probe and Educate (TPE) reviews are active in wound care, with MACs sampling 20–40 claims per round and a 45-day response window for ADRs.
For a full compliance breakdown by jurisdiction, including the complete MAC article comparison and ABN workflow, the Medicare wound care billing guide covers all of it.
What Documentation Is Required for Wound Care Billing?
Documentation failures are the leading cause of wound care denials — not coding errors, not modifier misuse. Documentation errors that survive to the audit stage can trigger False Claims Act liability at $11,000+ per violation. The stakes are not administrative.
The 5 Pillars of Wound Care Documentation:
- Location and laterality: “Right heel,” “left lateral malleolus” — not just “foot” or “lower extremity.” The ICD-10 laterality must match.
- Measurements (L×W×D in cm): Every visit. Surface area calculation feeds add-on code billing. Improvement tracking from these numbers is what keeps Medicare paying.
- Tissue composition: Percentages. “60% yellow slough, 30% granulation, 10% eschar” is billable language. “Wound has slough” is not. The percentage guides code selection and establishes medical necessity.
- Exudate/drainage: Type (serous, sanguineous, purulent) and amount (scant, moderate, copious). This is what differentiates a clinically deteriorating wound from a healing one.
- Edges, periwound, and tunneling: Rolled edges, periwound maceration, erythema. Tunneling documented with the clock method (“2 cm tunneling at 3 o’clock”).
Documentation that’s audit-proof vs. documentation that gets you investigated:
“Sharp debridement with sterile curette until bleeding base reached” will pass an ADR. “Curette used” will not. “Bone fragments excised using rongeur” supports 11044. “Bone visible” does not. “15% reduction in surface area and 20% reduction in slough since last visit, consistent with healing trajectory” supports continued coverage. “Wound looks better” does not.
OIG Audit Triggers to Avoid:
Template cloning — identical notes across multiple dates — accounts for approximately 25% of CERT wound care errors. Copy-paste documentation creates False Claims Act exposure. Non-specific language like “clean, dry, intact” without measurements is the most common ADR failure. And billing 11044 without explicit documentation of bone removal is a high-priority OIG target.
For Diabetic Foot Ulcers: The note must link the diabetes to the wound as a manifestation. “Type 2 DM poorly controlled (HbA1c 8.2), presenting with neuropathic right heel ulcer” — then E11.621 first in Box 21, L97.512 second. One code without the other denies at 40%.
📋 Wound Care Billing Documentation Checklist (2026)
Check off all required documentation before submitting your wound care claim. Missing any item below is the leading cause of CO-97 denials.
For the complete documentation framework — including the wound care order elements and 30-day progress documentation rules — see our wound care billing guidelines.
10 Wound Care Billing Questions — Answered Fast
Q1: What is CPT 11042 for wound care?
CPT 11042 is surgical debridement of subcutaneous tissue (fat), including epidermis and dermis, for the first 20 sq cm or less. The note must state subcutaneous fat was removed to bleeding margins — not just that the wound was cleaned. Add-on code +11045 covers each additional 20 sq cm. 2026 Medicare rate is approximately $250 non-facility. MUE is 4 units/day.
Q2: How do you bill multiple wounds in one visit?
Same-depth wounds: sum the surface areas and bill one primary code plus add-ons. Three 15 cm² subcutaneous wounds = 45 cm² total = 11042 + 11045 × 2. Different-depth wounds: bill the deepest as primary, shallower wounds as separate line items with modifier XS (separate structure). Document each wound’s location, depth, and area individually.
Q3: Are dressing changes billable separately?
Generally no. CMS Article A55818 bundles routine dressing changes into debridement codes like 97597 or E/M services. The exception is CPT 97602 in SNF and home health settings (it’s Status B — non-payable — in physician offices). HCPCS gauze codes A6222/A6223 can bill via DME for non-routine medically necessary supply needs with a Standard Written Order.
Q4: What’s the rule for billing compression with debridement?
NCCI Chapter 4G bundles compression codes 29580, 29581, and 29445 with same-limb debridement. The indicator is 1, meaning a modifier can bypass the bundle when the services occur on different limbs or different sites. Use modifier XS and document separate diagnoses and separate anatomic locations. Gradient pressure (30–50mmHg) documentation is required for the compression code to stand independently.
Q5: Can you bill 97597 and 97598 together?
Yes — 97598 is an add-on code that requires 97597 as the primary. Calculate total area, divide by 20, round up. A 60 sq cm wound with selective debridement bills as 97597 + 97598 × 2. Document cumulative surface area treated and selective removal in each segment. MUE: 97597 = 4/day, 97598 = 3/day.
Q6: Who can bill for wound care — physicians only?
No. MDs/DOs bill all wound care codes. Nurse Practitioners and Physician Assistants bill independently at 85% of the physician rate. Physical Therapists can bill 97597 and 97602 with the GP modifier under a therapy Plan of Care — but cannot bill surgical debridement codes (11042–11047). Occupational Therapists use the GO modifier. Podiatrists bill all wound codes plus Q8/Q9 for routine foot care carve-outs. RNs cannot bill independently.
Q7: How do I appeal a denied wound care claim?
Level 1 Redetermination goes to the MAC within 120 days of the EOB. Your appeal packet needs the full clinical note, 30-day wound trajectory measurements, failed conservative care documentation, and the Group 1 ICD-10 codes from your jurisdiction’s LCD. With proper documentation, the success rate is around 65%. Without it: about 20%. Level 2 Reconsideration (QIC) allows 180 days. Level 3 is an ALJ hearing — historically the highest provider success rate. For help building successful appeal packets, our denial management services are built specifically for wound care claim patterns.
Q8: What are the 5 rules of wound care billing?
(1) Measure every wound at every visit — L×W×D in cm, every time. (2) Document the exact tissue removed — fat, muscle, or bone — not just “debrided.” (3) Apply RT/LT modifiers and confirm they match the ICD-10 laterality. (4) Document 30 consecutive days of failed conservative care before billing biologics or NPWT. (5) Get a legible, authenticated signature with a date of service on the note — no signature means no payment, period.
Q9: Can telehealth be used to bill wound care?
Yes, for evaluation and management services. CPT codes 99202–99215 and G0389 (photo wound triage) are telehealth-eligible under CMS’s permanent post-PHE rules. Debridement cannot be performed or billed via telehealth — it requires physical contact. Video wound measurement is acceptable when the patient performs measurement under provider guidance with documentation. Use POS 02 or 10 with modifiers GT or 95. In 2026, G0389 is usable for ongoing wound monitoring.
Q10: What’s the difference between CPT 97606 and 97608?
97606 is NPWT for wounds greater than 50 sq cm using durable, reusable pump equipment. 97608 is an add-on code for each additional 100 sq cm of NPWT — it applies regardless of equipment type and cannot be billed without a primary NPWT code. Both require pressure settings documented at every visit. MUE for 97606 is 1 unit per day.
Should You Outsource Wound Care Billing?
Most practices that outsource wound care billing don’t do it because they gave up on in-house. They do it because they ran the math.
Here’s a real-world scenario: a practice billing $600,000 annually in wound care services with an in-house general biller. A 15% denial rate means $90,000 in denied revenue per year. With a 60% recoverable rate, that’s $54,000 walking out the door permanently — every year. Days in AR average 50+, compared to a 28-day benchmark.
Bring in a specialized wound care billing partner and the numbers shift: denial rate drops to 4%, permanent leakage drops to $1,440, and AR normalizes below 35 days. Net gain before the service fee is over $52,000. At a 6.5% service fee on collections, you’re still well ahead — and your clinical staff aren’t spending their afternoons on rework.
The gap isn’t about effort. It’s about specialization. General billing firms miss add-on codes (+11045, +97598) routinely — $150–$300 per visit in lost revenue. They don’t know the 12/360 rule triggers automatic denials if frequency isn’t tracked. They code to visible wound depth instead of excised tissue depth. They don’t maintain separate workflows for Noridian vs. Palmetto LCDs. These aren’t catastrophic failures. They’re quiet, consistent revenue leakage that compounds over time.
🩹 Wound Care Billing ROI Calculator
Enter your practice numbers below to see how much revenue a specialized wound care billing partner can recover for you annually.

Six signs your billing isn’t optimized for wound care:
- Denial rate consistently above 10%
- You’re billing 97602 in an office setting
- No add-on code revenue on large wound claims
- Days in AR above 50
- No 12/360 frequency monitoring system
- Diabetic ulcer claims missing the E11.621 + L97.5xx pairing
What a specialized wound care billing partner should actually deliver:
CWCC-certified coders on the team (verifiable via AAPC directory). MAC-specific LCD compliance checks by ZIP code. Quarterly NCCI edit scrubbing that incorporates Chapter 4G updates. Automated ABN generation before frequency limits are hit. 2026 skin substitute flat-rate tracking with Q41xx code workflows. Appeal success rates above 60% for CO-97 denials.
Before you commit to any billing service, ask them: “How do you monitor the 12/360 rule?” and “What changed in Noridian A58565 Revision 11?” If they can’t answer specifically, they’re not wound care specialists.
For a deeper look at the outsourcing decision — including a transition timeline, parallel run process, and interview questions for evaluating billing companies — see our outsource wound care billing guide.
Not sure how much revenue your current billing approach is leaving behind? Our team will review your last 90 days of claims, identify leakage points, and give you a real number — no obligation. Request a free wound care billing assessment today.
Voice Search: Quick Answers to Common Wound Care Billing Questions
What is wound care billing in simple terms? It’s the process of turning clinical wound treatments — debridement, skin substitutes, NPWT — into insurance codes and submitting claims for payment. Because wound care uses specific depth and surface area rules, accurate billing ensures your practice gets reimbursed correctly for complex procedures.
Can wound care services be billed to Medicare? Yes. Medicare Part B covers wound care when medically necessary. You need ICD-10 codes from your MAC’s Group 1 list and documentation showing 30 days of failed conservative care before advanced treatments like skin substitutes or NPWT.
What CPT code is used for wound debridement in a doctor’s office? For selective debridement of surface tissue, use CPT 97597 for the first 20 sq cm. For surgical debridement removing subcutaneous fat, use CPT 11042. Both are payable in a physician office — unlike 11043 and 11044, which are facility-only codes.
How do you document wound care for billing purposes? Record location with laterality, measurements in centimeters, tissue type percentages, drainage characteristics, and periwound status at every visit. For debridement, specify the deepest tissue removed — “subcutaneous fat to bleeding margins” for 11042, not just “wound debrided.”
What is the most common reason wound care claims get denied? Missing medical necessity documentation — specifically, failing to document the 30-day conservative care failure before advanced therapies, or documenting wound depth without explicitly stating what tissue was excised. CO-97 accounts for about 40% of wound care denials.
How do I find a wound care billing service for my practice? Look for services with CWCC-certified coders, MAC-specific LCD expertise, documented denial rates under 5%, and the ability to track frequency limits with automated ABN generation. Ask for references from wound care practices similar in size to yours, and request a sample claims audit before signing any contract.
Frequently Asked Questions About Wound Care Billing
What is wound care billing?
Wound care billing is the specialized process of translating clinical wound treatments — debridement, skin substitutes, compression, and NPWT — into standardized CPT and ICD-10 codes for insurance reimbursement. Unlike general billing, it requires precise depth documentation, compliance with MAC LCDs like Noridian A58565, and navigation of NCCI bundling rules. The 2026 PFS shifted skin substitutes to a flat-rate supply model, adding new complexity.
Can you bill for wound care dressing changes?
Generally no — CMS Article A55818 bundles routine dressing changes into debridement codes like 97597. CPT 97602 (non-selective, wet-to-moist) is payable in SNF/HHA settings but is Status B (non-payable) in physician offices. HCPCS A6222/A6223 gauze codes can apply via DME with a valid Standard Written Order for non-routine medically necessary supplies.
Is wound care billing the same as wound care coding?
No. Coding assigns the CPT (11042 for subcutaneous debridement) and ICD-10 (E11.621 + L97.512 for diabetic foot ulcer) from clinical documentation per LCD requirements. Billing handles claim submission, modifier application, NCCI scrubbing, and denial appeals. Both functions need wound-specific expertise: coders master depth rules, billers track 12/360 frequency limits and payer-specific prior auth workflows.
What insurance covers wound care services?
Medicare Part B covers debridement and NPWT at 80% post-deductible when 30-day conservative care failure is documented and ICD-10 codes appear on the LCD Group 1 list. Medicaid follows state-specific rules, often mirroring Medicare. Commercial insurers (Aetna, UHC, BCBS) cover similar services but require prior authorization for skin substitutes. Medicare Advantage adds stricter utilization review. All payers require documented medical necessity and non-healing of at least four weeks.
How long does it take to get reimbursed for wound care?
Wound care claims average 45–60 days in AR due to LCD review complexity and appeals — longer than most specialties. Practices with specialized billing partners consistently hit below 35 days through proactive NCCI scrubbing, auto-ABN workflows, and clean first-pass submissions that don’t require rework.
What is the difference between CPT 97597 and CPT 11042?
CPT 97597 is selective (non-excisional) debridement of surface tissue — epidermis and dermis — for the first 20 sq cm. CPT 11042 is surgical excision into subcutaneous fat, requiring documentation that fat was removed to bleeding margins. Use 97597 for surface-level slough removal in offices; use 11042 when subcutaneous tissue is excised. Per Noridian A58565, they cannot both be billed on the same wound the same day.
Does wound care require prior authorization?
Basic debridement (97597, 11042) typically does not. Advanced therapies — skin substitutes (15271–15278, 8-application cap), NPWT (97605–97608), and HBOT (99183, NCD 20.29) — often do. Medicare Advantage requires prior auth for 90% of these cases. Without prior authorization, expect PR-96 denials. Submit 30-day failure logs, wound metrics, and progress photos with the PA request.
What happens if a wound care claim is denied?
Technical denials (CO-16 for missing information, CO-4 for modifier issues) fix via correction and resubmission within 30 days. Clinical denials (CO-97 for medical necessity, about 40% of wound care denials) require a Level 1 Redetermination to the MAC within 120 days. Include the full clinical note, 30-day wound trajectory, and LCD Group 1 ICD-10 codes. Success rate with documentation: 65%. Without it: 20%.
Conclusion: Three Things That Will Change Your Wound Care Revenue
Wound care billing is genuinely difficult. The depth-based CPT rules, dual ICD-10 requirements, NCCI bundling edits, MAC-specific LCDs, and 2026 flat-rate skin substitute changes make it one of the most complex billing specialties in outpatient medicine. But difficult doesn’t mean unmanageable — it means the practices that invest in getting it right gain a significant financial advantage over those that don’t.
Here’s what the data actually shows: the difference between a 15% denial rate and a 4% denial rate is worth more than $50,000 per year for most wound care practices. That’s not a rounding error in the revenue cycle — that’s a meaningful number that funds staffing, equipment, and practice growth.
Three takeaways worth keeping:
First, documentation drives everything. Not the code you select — the words in the note that justify it. If the note says “bone visible,” you cannot bill 11044. If the note says “bone fragments excised using rongeur,” you can. That’s a $200 difference per claim, and it comes down to two words.
Second, the 2026 skin substitute changes are not optional knowledge. If your practice uses CTPs and you haven’t adjusted your formulary and billing workflow for the $127.14/sq cm flat rate, you may be operating at a loss on those services right now.
Third, most wound care revenue problems are not caused by insurance companies being unreasonable. They’re caused by preventable documentation gaps, missed modifiers, and billing processes designed for general medical practices rather than wound care. Fix the process, and the reimbursement follows.
If you want to know exactly where your current billing stands, our team offers a no-obligation claims assessment. We’ll review your last 90 days of claims, identify leakage points, and give you a clear picture of what’s recoverable. Beyond wound care, we also support practices with complete RCM services, medical billing, medical coding, Medicare credentialing, and full-practice financial management including digital marketing and IT services at elitemedfinancials.com.
Contact our wound care billing specialists today — and let’s find out what your revenue cycle is actually worth when it’s running the way it should.
External Resources: CMS Medicare Coverage Database for LCD and NCD lookups | AAPC CWCC Certification for verifying wound care coder credentials

