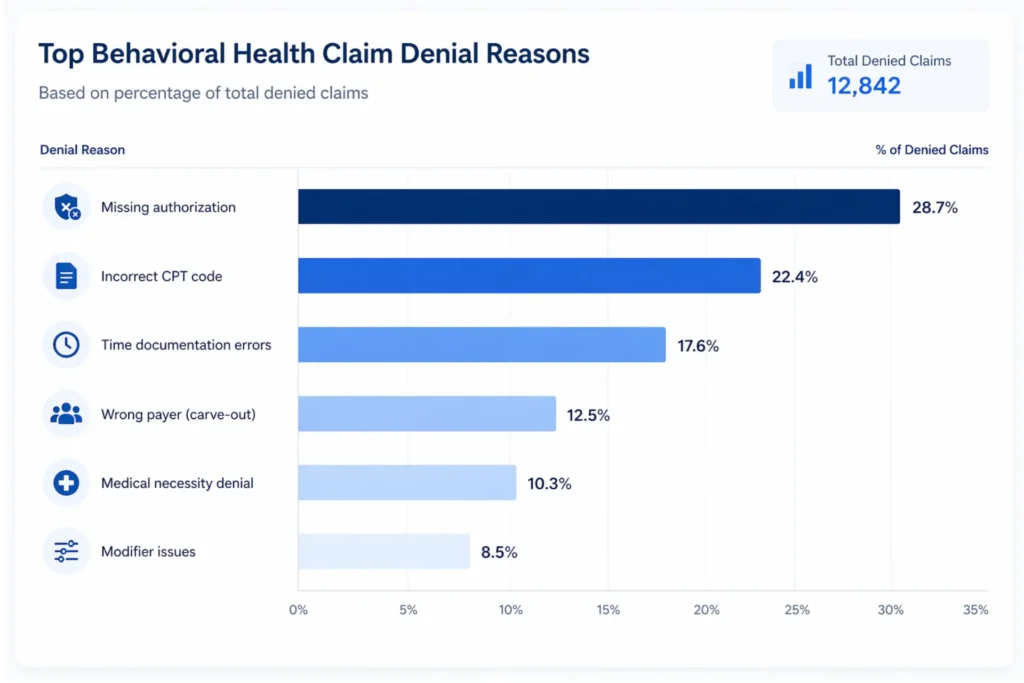
Behavioral health billing is one of the most operationally demanding specialties in healthcare revenue cycle management. Denial rates for behavioral health claims run 25–30% — nearly triple the 8–12% average in general medicine. The coding is time-based. The payers carve out mental health benefits to separate administrators. The documentation standards are stricter, more subjective, and more heavily audited than almost anything in physical medicine.
Behavioral health billing is the specialized revenue cycle management process for submitting and managing insurance claims for mental health, substance use disorder, and behavioral modification services. It relies on time-based CPT codes (90834, 90837), HCPCS Level II codes (H0015, S9480), ICD-10-CM diagnoses mapped from DSM-5 criteria, and strict medical necessity documentation — all routed through a payer ecosystem that frequently separates behavioral health benefits from medical coverage.
Whether you’re running a solo therapy practice or a multi-site treatment center with IOP, PHP, and residential programs, the billing rules in this specialty are different from every other area of medicine. This guide covers all of it — definitions, code tables, CMS compliance, incident-to billing, and the real math behind outsourcing decisions.
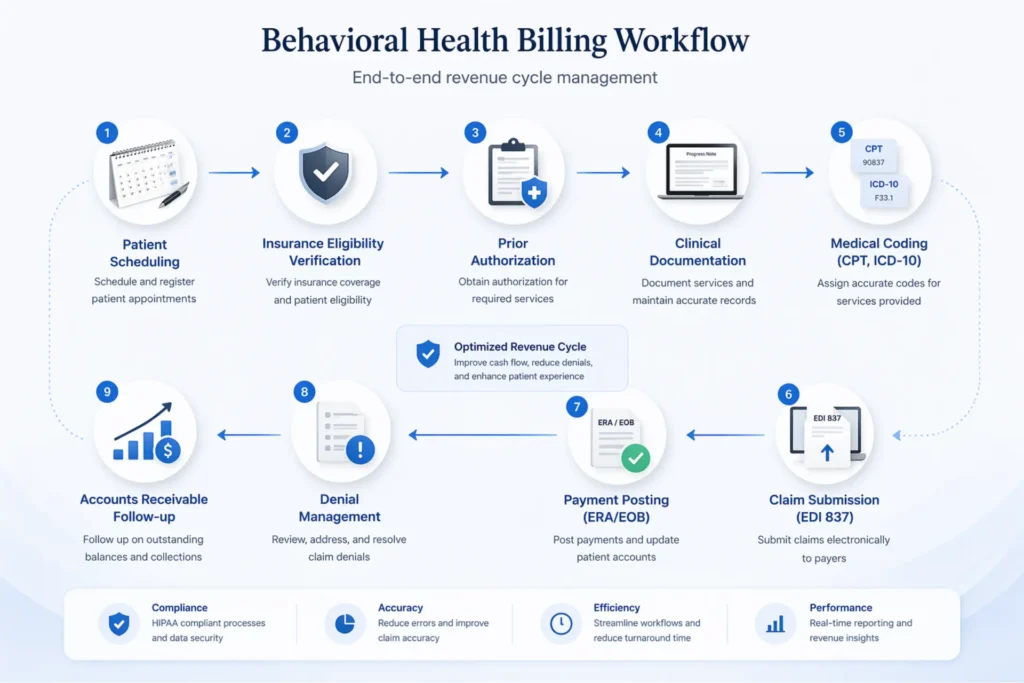
Table of Contents
What Is Behavioral Health Billing?
At its core, behavioral health billing is revenue cycle management for a specific set of clinical services: psychotherapy, psychiatric evaluation, medication management, psychological testing, crisis intervention, substance use disorder treatment, and integrated care programs like BHI and CoCM.
The term gets thrown around loosely, but the operational definition matters. Behavioral health billing covers any service that addresses mental health conditions, substance use disorders, eating disorders, developmental conditions (including ABA therapy), and behavioral modification interventions. When Optum labels their division, they call it “Behavioral Health” — not “Mental Health.” That naming isn’t arbitrary. It defines what gets billed, where claims get routed, and which compliance rules apply.
How It Differs from General Medical Billing
In general medical billing, coding is complexity-based. An E/M visit uses Medical Decision Making (MDM) to determine the code level. A surgeon removes a gallbladder, and that’s a CPT code with a fixed reimbursement regardless of how long the case took.
Behavioral health billing is time-based. A 45-minute therapy session (CPT 90834, covering 38–52 minutes of face-to-face time) pays differently from a 60-minute session (CPT 90837, covering 53+ minutes). The difference between a paid claim and a recoupment demand can come down to three minutes of documented session time.
On top of that, behavioral health uses DSM-5-TR diagnostic criteria mapped to ICD-10-CM F-codes. The payer ecosystem is fragmented — many commercial plans carve out behavioral health benefits to Managed Behavioral Health Organizations (MBHOs) like Optum, Carelon (formerly Beacon), or Magellan. Prior authorization requirements hit behavioral health at roughly five times the rate of physical medicine services. And the documentation standard isn’t objective test results — it’s clinical narrative defending why ongoing talk therapy remains medically necessary.
That’s where practices lose money. Not from coding the wrong CPT code, but from billing the wrong payer, missing an authorization, or failing to document the time that supports the code they selected.
What Services Fall Under Behavioral Health Billing
The scope is broader than most people realize:
- Individual, group, and family psychotherapy
- Psychiatric diagnostic evaluations and medication management
- Psychological and neuropsychological testing
- Crisis intervention and stabilization services
- Intensive Outpatient Programs (IOP) and Partial Hospitalization (PHP)
- Residential treatment (short-term and long-term)
- Substance use disorder treatment, including MAT (Medication-Assisted Treatment)
- Behavioral Health Integration (BHI) and Collaborative Care (CoCM)
- Applied Behavior Analysis (ABA therapy)
- Assertive Community Treatment (ACT)
The Revenue Cycle Workflow
The behavioral health revenue cycle follows the same general stages as medical billing — eligibility verification, authorization, documentation, coding, claim submission via EDI 837 transactions, payment posting from ERAs and EOBs, denial management, and patient collections — but each stage has unique failure points.
Eligibility verification in behavioral health isn’t just checking if the plan is active. You need to confirm whether mental health benefits are carved out to a separate payer and whether the specific service type requires authorization. Missing a carve-out means your claim goes to the wrong payer and comes back as a CO-109 denial. That’s not a coding issue. It’s a workflow issue.
For a deeper look at the full mental health revenue cycle, we’ve covered the end-to-end process in a separate guide.
Behavioral Health Billing vs Mental Health Billing — Is There a Difference?
Yes. And it matters more than most practices realize.
What Behavioral Health Covers
“Behavioral health” is the umbrella term. It includes everything classified as mental health services plus substance use disorder treatment (F10–F19), eating disorder services (F50.x), developmental and behavioral conditions (F80–F89, including ABA therapy for autism), and behavioral modification interventions. When payers like Optum or Carelon label their division, they use “Behavioral Health” — not “Mental Health.” That’s the industry standard.
What Mental Health Covers
“Mental health” is narrower. It typically refers to psychological conditions — depression (F32.x), anxiety disorders (F41.x), PTSD (F43.12), bipolar disorder (F31.x), schizophrenia (F20.x). The CPT codes are familiar: 90832–90837 for psychotherapy, 90791 for psychiatric evaluation, 99213–99215 for medication management.
Where They Overlap — And Where They Don’t
Both use the same psychotherapy CPT codes. Both rely on ICD-10-CM F-codes for diagnoses. Both face the same documentation requirements for medical necessity. A therapist treating generalized anxiety disorder uses the same billing workflow whether you call it “mental health billing” or “behavioral health billing.”
The divergence shows up in three places:
Coding. Substance use disorder services add HCPCS H-codes (H0001 for assessment, H0004 for individual counseling, H0015 for IOP, H0017–H0019 for residential) that don’t exist in pure mental health billing. SUD billing may also use modifier HF to indicate a substance use program.
Claim routing. A patient with depression might have claims processed by BCBS directly. That same patient’s SUD claims might route to Magellan as the behavioral health carve-out administrator. An LCSW may be paneled for “Mental Health” benefits but find themselves out-of-network for “Substance Abuse” services under the same insurance company. That’s a revenue leak most practices don’t discover until the denial arrives.
Compliance. SUD records fall under 42 CFR Part 2, which imposes stricter confidentiality requirements than standard HIPAA. You need separate written consent to disclose SUD treatment information — even for payment purposes. As of February 16, 2026, Part 2 has aligned with HIPAA to allow a single TPO (Treatment, Payment, Operations) consent, but the written consent requirement itself remains.
For foundational overviews of mental health billing codes and what mental health billing covers, we’ve published separate guides.
| Dimension | Mental Health Billing | Behavioral Health Billing |
|---|---|---|
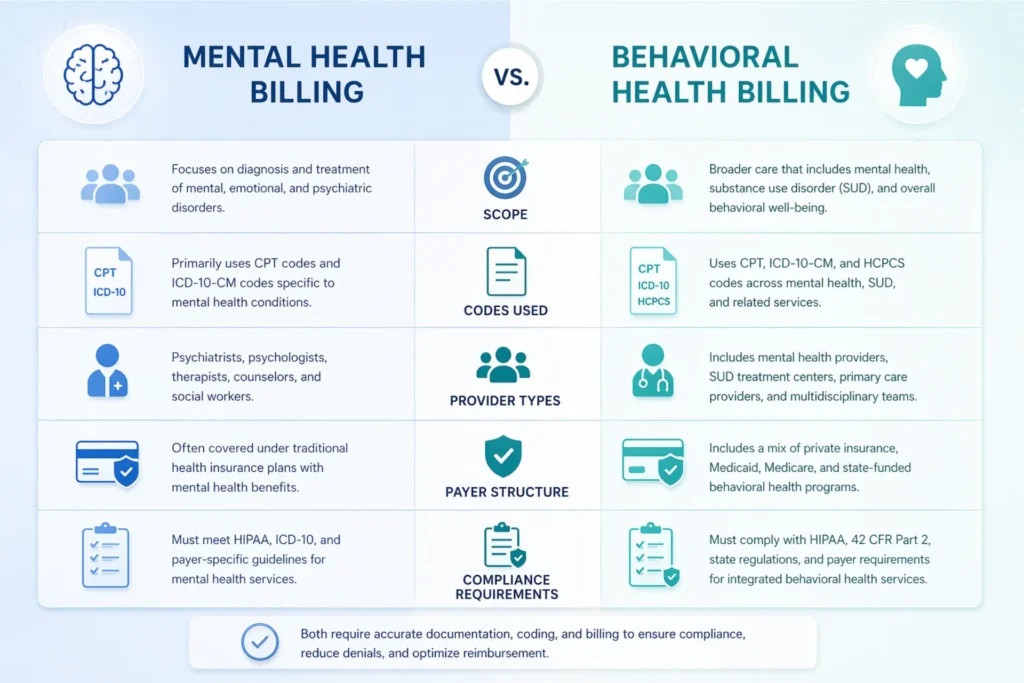
| Scope | Psychological conditions (depression, anxiety, PTSD, schizophrenia) | MH + substance use disorders + eating disorders + developmental + behavioral modification |
| Primary Codes | CPT 90832–90837, 90791, E/M 99213–99215 | All MH codes + HCPCS H-codes (H0001, H0015, H0017–H0019), S-codes (S9480) |
| Diagnostic Framework | DSM-5-TR to ICD-10 F-codes | DSM-5-TR + ASAM Criteria (Levels 1–4) for SUD placement |
| Provider Types | Psychiatrists, psychologists, LCSWs, LPCs, LMFTs | All MH providers + SUD counselors (CAADC), BCBAs, peer support specialists |
| Payer Structure | Often under primary medical carrier | Frequently carved out to MBHOs (Optum, Carelon, Magellan) |
| Key Regulation | HIPAA, MHPAEA | HIPAA + 42 CFR Part 2 (SUD confidentiality) |
| Authorization | Session-count based | Session-based + level-of-care (ASAM criteria for IOP/PHP/residential) |
CPT Codes Used in Behavioral Health Billing
This is where claims get paid or denied. If the section above is the “why,” this section is the “how.”
Psychotherapy Codes — Time Boundaries That Matter
These three codes represent the majority of behavioral health claims submitted in the United States:
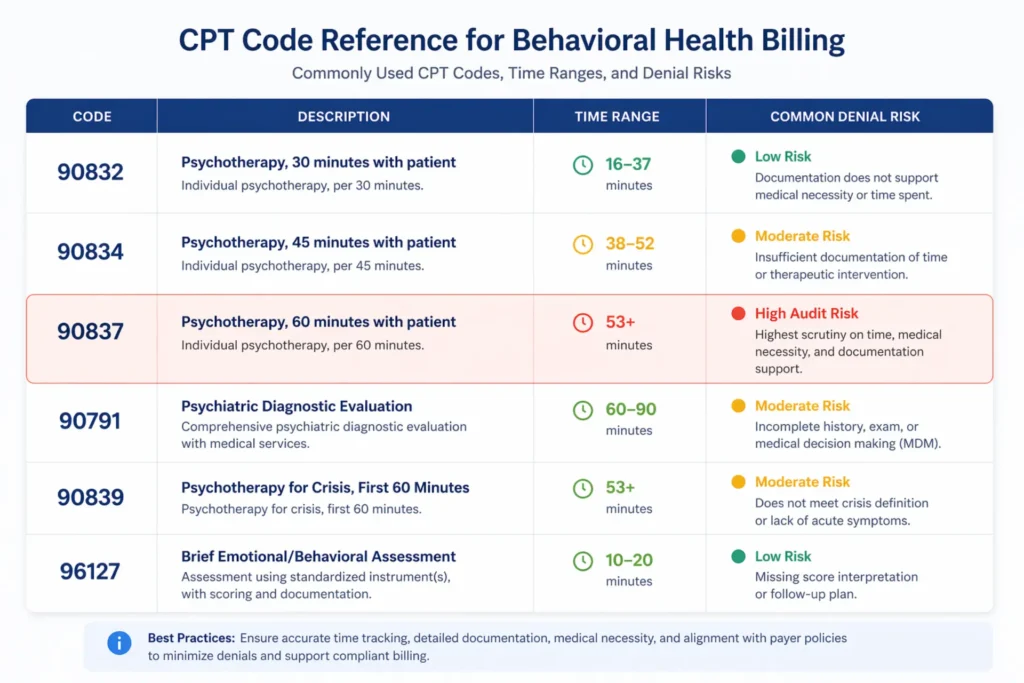
- 90832 — 30-minute psychotherapy (16–37 minutes face-to-face)
- 90834 — 45-minute psychotherapy (38–52 minutes face-to-face)
- 90837 — 60-minute psychotherapy (53+ minutes face-to-face)
The time boundaries are strict. If you document a 50-minute session, you bill 90834. If you document a 53-minute session, you bill 90837. There is no rounding. CPT 90837 is the most audited code in behavioral health — payers routinely request records for claims billed at this level and will recoup payment if the documented time falls below 53 minutes.
Document start and stop times. Not “approximately 55 minutes.” Exact clock times: “Session started at 10:02, ended at 10:57.” General duration statements are audit triggers. That claim will sit in a recoupment queue.
Psychiatric Evaluation Codes
- 90791 — Psychiatric diagnostic evaluation (without medical services)
- 90792 — Psychiatric diagnostic evaluation with medical services (prescribing capability)
These codes can be billed once per episode of illness. CMS considers an “extended break” approximately 6 months from the last visit. You cannot bill 90791 and 90834 on the same day — NCCI edits will automatically deny this combination with a CO-97 bundling denial.
Psychotherapy Add-On Codes with E/M
When a psychiatrist or NP provides both therapy and medication management in the same visit:
- 90833 — 30-minute psychotherapy add-on (16–37 min)
- 90836 — 45-minute psychotherapy add-on (38–52 min)
- 90838 — 60-minute psychotherapy add-on (53+ min)
These are never billed standalone. They pair with an E/M code (99213, 99214, 99215). Modifier -25 goes on the E/M code to indicate a significant, separately identifiable service. Missing this triggers CO-97 bundling denials immediately. And note: time spent on E/M activities is not included in the psychotherapy time used to select 90833/90836/90838.
Crisis Codes
- 90839 — Psychotherapy for crisis, first 60 minutes
- +90840 — Each additional 30 minutes (add-on)
Crisis codes cannot be billed on the same day as standard psychotherapy (90832–90838) or evaluations (90791–90792). The patient must be in documented acute distress requiring urgent intervention — not just a difficult session. Missing the crisis documentation is a guaranteed M86 denial for medical necessity.
Group and Family Therapy
- 90853 — Group psychotherapy (billed per patient per session)
- 90846 — Family therapy without the patient present
- 90847 — Family therapy with the patient present
Group therapy requires an attendance roster documenting each participant. Family therapy requires documentation of who participated and why family involvement is clinically indicated. CPT 90847 and 90837 are mutually exclusive on the same date for the same patient.
Screening and Testing
- 96127 — Brief emotional/behavioral assessment per standardized instrument (PHQ-9, GAD-7)
- 96130–96131 — Psychological testing evaluation (first hour + each additional)
- 96136–96139 — Test administration and scoring by technician or QHP
BHI and Collaborative Care Codes
- 99484 — BHI care management, ≥20 minutes/month clinical staff time
- 99492 — Initial CoCM, ≥70 minutes first month
- 99493 — Subsequent CoCM, ≥60 minutes per month
- 99494 — Additional 30 minutes CoCM
- G0323 — BHI by LCSW/psychologist (Medicare)
These integration codes are time-tracked monthly services, not per-visit codes. The billing provider must maintain a documented care plan. Less than 20 minutes of tracked clinical staff time for 99484 means no billable service that month.
HCPCS Codes for Facility-Level Behavioral Health
- H0015 — Alcohol/drug IOP services (Medicaid primary; 3+ hours/day, <24 hours)
- S9480 — IOP psychiatric (commercial payers)
- H0035 — PHP mental health (20+ hours/week structured programming)
- H0017 — Residential SUD without room/board (per diem)
- H0018 — Short-term residential (<30 days)
- H0019 — Long-term residential (>30 days)
- H2011 — Crisis intervention per 15 minutes
H-codes are primarily recognized by Medicaid. S-codes are commercial payer codes. Medicare uses G-codes (G0510/G0511) for IOP under the 2024 expansion. Billing unit definitions — per diem, per hour, per 15 minutes — vary by state Medicaid program. Know your fee schedule.
Telehealth Modifiers and Place of Service Codes
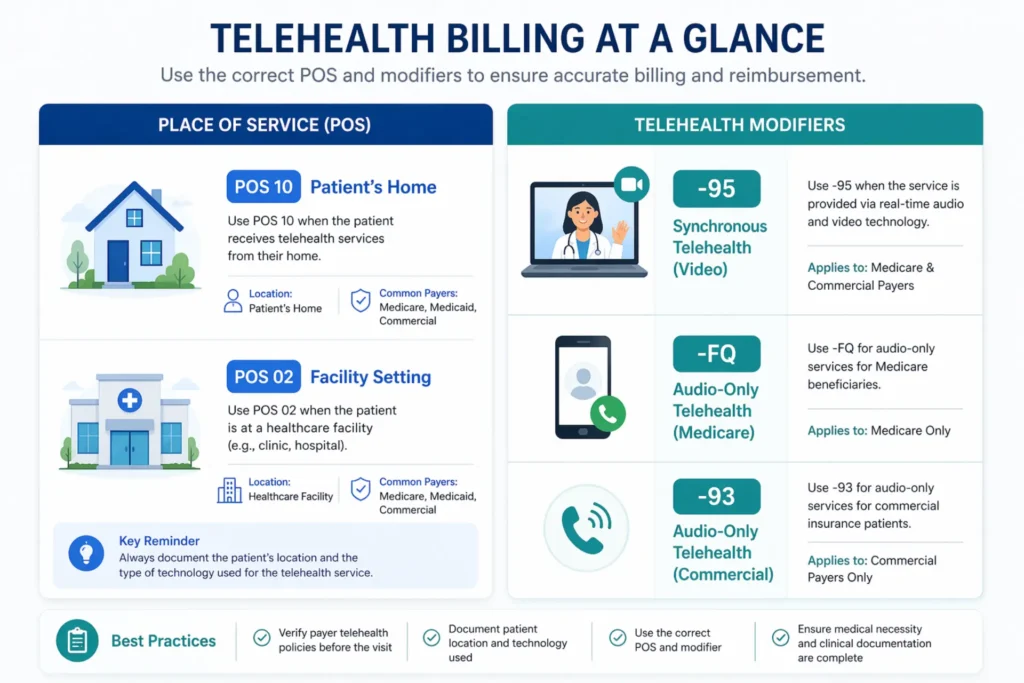
- -95 — Synchronous audio-video telehealth (most payers)
- -FQ — Audio-only mental health, Medicare permanent (2026)
- -93 — Audio-only telehealth (commercial payers)
- POS 10 — Patient at home (non-facility rate, higher reimbursement)
- POS 02 — Telehealth non-home location (facility rate, lower reimbursement)
Payer-specific modifier requirements vary significantly. Medicare wants -95 with POS 10 for video sessions and -FQ for audio-only. Some commercial payers still use -GT. UHC may require different modifier combinations than Aetna or Cigna. If the modifier and POS code don’t match the payer’s expectation, you’ll see a CO-4 denial for modifier mismatch.
For a complete breakdown of mental health CPT codes and telehealth billing rules, see our dedicated guides.
| CPT Code | Description | Time/Unit | Key Modifier/Note | Common Denial Risk |
|---|---|---|---|---|
| 90832 | 30-min psychotherapy | 16–37 min | — | <16 min documented |
| 90834 | 45-min psychotherapy | 38–52 min | — | 35 min documented (downcode to 90832) |
| 90837 | 60-min psychotherapy | 53+ min | Highest audit code | 45–50 min documented → recoupment |
| 90791 | Psychiatric evaluation | Once per 6 months | Cannot pair with 90834 same day | Repeat within 6 months (CO-97) |
| 90839 | Crisis psychotherapy | First 60 min | Cannot bill with 90832–90838 | No crisis documentation (M86) |
| 90833/36/38 | Therapy add-on + E/M | 16–37 / 38–52 / 53+ min | -25 on E/M required | Billed standalone (CO-97) |
| 96127 | Brief assessment | Per instrument | -59 if with 90791/90837 | Non-standardized tool or missing score |
| 99484 | BHI management | ≥20 min/month | Monthly care plan required | <20 min documented |
| H0015 | IOP SUD services | Per diem or per hour | Medicaid primary | No ASAM documentation |
| 90853 | Group psychotherapy | Per patient/session | Attendance roster required | >15 patients; no roster |
Is CPT 96127 a Behavioral Health Code?
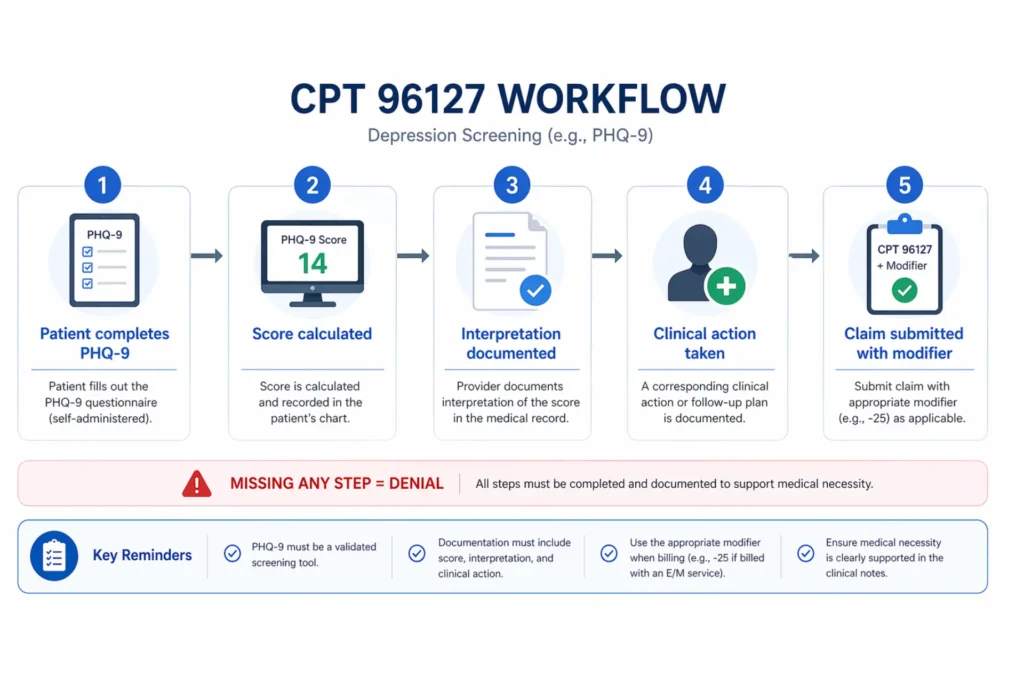
Yes. CPT 96127 — “Brief emotional/behavioral assessment (e.g., depression inventory, ADHD scale), with scoring and documentation, per standardized instrument” — is a behavioral health code. It covers validated screening tools like the PHQ-9, GAD-7, Vanderbilt ADHD Scales, AUDIT-C, DAST-10, PCL-5, Columbia Suicide Severity Rating Scale (C-SSRS), and Edinburgh Postnatal Depression Scale.
The key word is “standardized.” Self-created intake questionnaires and informal clinical interviews do not qualify. The instrument must have published validity scores. If you’re using a homegrown form, that claim will deny.
Who Can Bill 96127
Physicians (MD/DO), nurse practitioners, physician assistants, and psychologists can typically bill 96127 without issue. LCSWs, LPCs, and LMFTs often face denials because payers consider the screening assessment “inherent” to their psychotherapy codes (90834, 90837). Facebook billing forums are full of posts like “96127 is denying by most of my insurance” and “they usually consider 96127 to be bundled in 90791 or 90837.”
If your therapists administer PHQ-9 screenings, route the billing through a supervising MD or NP to capture this revenue. The clinical work is the same. The billing pathway makes the difference.
Common 96127 Denials and How to Fix Them
Bundling (CO-97). NCCI edits bundle 96127 into 90791 (psychiatric evaluation) and frequently flag it with 90837. To bill separately, you need modifier -59 or -XU on the 96127 and a distinct documentation note with: the instrument name, raw score, interpretation, and clinical action taken. Without all four elements, the override fails.
Frequency limits (CO-119). Medicare MUE caps at 2–3 units per day. Billing four PHQ-9 + GAD-7 + Vanderbilt + AUDIT-C in one visit will trigger a frequency denial on units 4+.
Non-standardized tools (N130/M86). A “feelings check-in worksheet” your practice created doesn’t qualify. Validated instruments with published norms are the only billable tools under 96127.
96127 vs G0444
Medicare uses G0444 for annual depression screening during the Annual Wellness Visit — once per 12 months, asymptomatic patients only, reimbursed at approximately $18. CPT 96127 is for symptomatic patients assessed at any visit frequency supported by medical necessity, at approximately $5 per unit. Don’t bill 96127 during a Medicare AWV when G0444 is the correct code.
At roughly $5 per unit with a cap of 2–3 units per day, 96127 looks small. But billing 2 units daily across 20 patients generates over $30,000 in annual revenue for work your clinicians are already doing. That’s not trivial.
Incident-to Billing for Behavioral Health
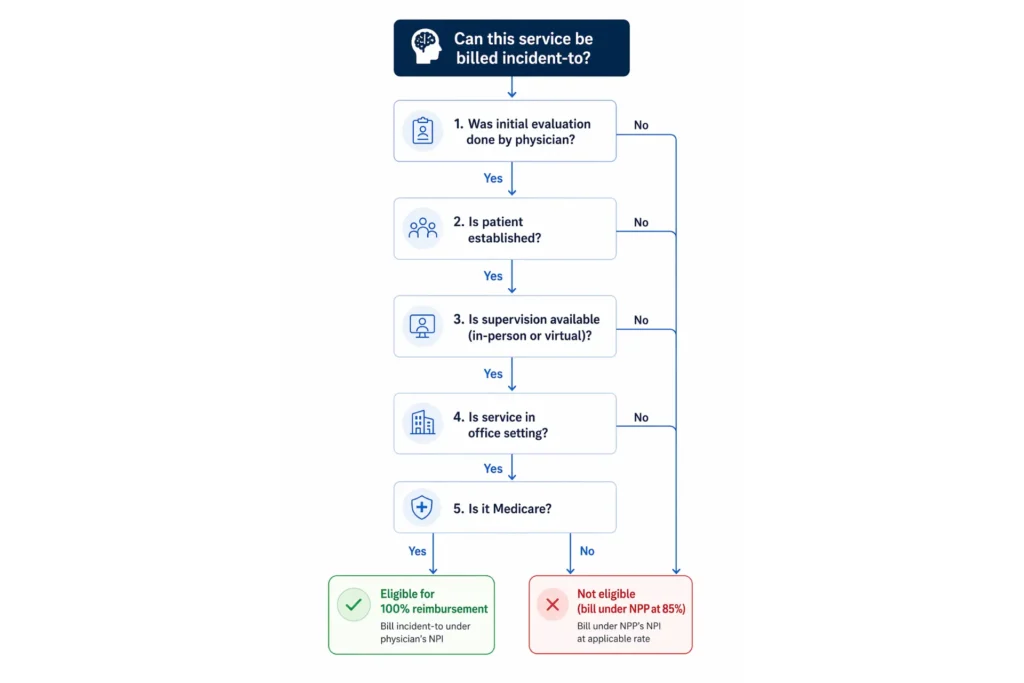
Incident-to billing is a Medicare provision that lets non-physician practitioners (NPPs) provide services under a supervising physician’s NPI, collecting 100% of the Medicare Physician Fee Schedule instead of the standard 85% NPP rate. For associate-level clinicians who can’t independently enroll in Medicare (LPC-Associates, LMFT-Associates, LMSWs), it’s often the only pathway to bill Medicare for their services at all.
The Medicare Rules
The requirements are specific and non-negotiable under 42 CFR §410.26:
- A physician (MD, DO) or qualifying NPP (NP, PA) must personally perform the initial evaluation and establish the treatment plan
- The supervising provider must be immediately available — either physically in the office suite or via real-time audio-video (virtual direct supervision became permanent in the 2026 PFS Final Rule)
- The service must follow the established treatment plan — same diagnosis, same course of care
- The service must occur in an office/clinic setting (POS 11). Not a hospital. Not a SNF. Not home health.
- The patient must be established — incident-to billing does not apply to new patients or new diagnoses
The Reimbursement Math
For CPT 90834, the difference between 100% (incident-to) and 85% (NPP independent) is roughly $18 per session. Across 20 sessions per week for an associate-level clinician, that’s $360/week or $18,720/year in additional revenue per provider.
That 15% differential funds practice overhead. For a group with three associate-level therapists, it’s over $56,000 annually.
Which NPPs Qualify
LPCs, LPC-Associates, LMFTs, LMFT-Associates, LMSWs, and pre-licensed clinicians can render services incident-to a supervising physician. LCSWs and psychologists are independently enrolled Medicare providers — they generally cannot serve as the supervising provider for incident-to purposes in most MAC jurisdictions. That’s a common misconception.
When It Does NOT Apply
- New patients or new diagnoses — the supervisor must evaluate first
- Hospital or institutional settings — use shared/split billing instead (where the substantive portion rule, >50% time or MDM, determines the billable provider)
- Most commercial payers — UHC, BCBS, Cigna, and Aetna generally don’t recognize Medicare incident-to rules. Optum’s 2026 mandate now requires both billing NPI and rendering NPI on all behavioral health claims, effectively blocking non-credentialed associates on commercial submissions.
Common Mistakes That Trigger Audits
Generic co-signatures like “I have reviewed and agree” stamped across 100+ claims are immediate audit flags. Supervisors must document substantive involvement — reviewing the treatment plan, noting clinical progress, confirming the service aligns with the established plan. A physician must see the patient every 3–6 months at minimum. Anything less looks like rubber-stamping, and auditors know the pattern.
CMS Behavioral Health Billing Guidelines
CMS guidelines form the compliance foundation for behavioral health billing. Everything commercial payers do is built on — or deviates from — the Medicare framework.
Medicare Part B Provider Types
As of January 1, 2024, LPCs and MFTs gained direct Medicare billing rights under the Consolidated Appropriations Act. They bill at 85% of the Physician Fee Schedule using their own NPI, enrolled through PECOS with CMS-855I (individual) and CMS-855R (group reassignment).
Previously enrolled provider types: psychiatrists (MD/DO), psychologists, LCSWs, NPs, PAs, and clinical nurse specialists.
Telehealth Rules for Behavioral Health (2026)
CMS has made several pandemic-era telehealth flexibilities permanent for behavioral health:
- Originating site requirement removed — patients can receive tele-mental health services from home (POS 10) or any community location (POS 02) nationwide
- Audio-only permanently reimbursed — modifier -FQ for Medicare when video technology is unavailable or declined by the patient
- In-person initiation requirement delayed until January 1, 2028 — no prior in-person visit required to start or maintain tele-mental health services throughout 2026
- Virtual direct supervision codified — real-time audio-video presence satisfies the incident-to “immediate availability” requirement under the 2026 PFS Final Rule
- Geographic restrictions permanently suspended for behavioral health services
The POS code selection affects reimbursement directly. POS 10 (patient at home) pays the non-facility rate — higher reimbursement. POS 02 (telehealth non-home) pays the facility rate — lower reimbursement. Incorrect POS selection is a common source of lost revenue that doesn’t trigger a denial but silently reduces payments.
Documentation Standards CMS Requires
CMS Article A57480 establishes the medical necessity standard for psychiatry and psychology services. For time-based psychotherapy codes, CMS requires exact start and stop times — “10:02 to 10:55,” not “approximately 53 minutes.”
Progress notes must include the diagnosis (ICD-10), presenting symptoms and severity, clinical interventions used, patient response, and progress toward measurable treatment goals. Treatment plans require updates every 3–6 months with documented measurable goals, therapy modality, frequency, and estimated duration.
The 2024 IOP Benefit Expansion
The Bipartisan Safer Communities Act added Medicare IOP coverage. IOP is billed with HCPCS G0510/G0511 on UB-04 claims using Condition Code 92 and Revenue Codes 0904–0906. The program requires 9–19 hours per week of structured programming and physician certification. This represents a significant new revenue stream for qualified facilities.
MHPAEA — Mental Health Parity
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires commercial payers to cover behavioral health benefits no more restrictively than medical/surgical benefits. The 2024 final rule mandates that payers provide comparative analyses of Non-Quantitative Treatment Limits (NQTLs) upon written request.
When a payer imposes session caps, aggressive prior authorization requirements, or restrictive network standards that wouldn’t apply to a comparable medical condition, that’s a potential parity violation. File a complaint through the CMS parity portal or escalate to your state Department of Insurance.
42 CFR Part 2 — SUD Record Confidentiality
Effective February 16, 2026, 42 CFR Part 2 final alignment with HIPAA permits a single written TPO consent for SUD records — a major simplification from the prior disclosure-by-disclosure model. Part 2 programs must now also comply with HIPAA Breach Notification requirements. The redisclosure prohibition remains, and patient consent must still be written.
Who Can Bill Medicare for Behavioral Health
Psychiatrists, psychologists, LCSWs, LPCs (2024+), MFTs (2024+), NPs, PAs, and CNSs — each enrolled through PECOS with an active NPI and Medicare provider enrollment number (PTAN). For a detailed guide on credentialing for mental health providers, we’ve covered the enrollment process separately.
Also see the AMA Behavioral Health Coding Guide for a reference across the BHI continuum.
Struggling with CMS Guidelines and Payer-Specific Rules?
EliteMed Financials handles behavioral health billing with full CMS compliance, correct modifier usage, and payer-specific rule enforcement — so your claims get paid the first time.
Behavioral Health Billing and Coding Training
One of the most common questions on AAPC forums and Reddit threads: “I’m new to behavioral health coding — where do I start?” And the honest answer depends on what you’re trying to do.
Do You Need Certification?
Coding roles — the people assigning CPT, HCPCS, and ICD-10 codes — typically require certification (CPC, CCS-P, or equivalent). Billing roles — submitting claims, posting payments, working AR — often don’t require certification, though it helps. Most hiring managers want experience first, certification second.
Programs That Matter
- AAPC CPC (Certified Professional Coder) — the most recognized coding credential; the behavioral health-specific coding course earns 10 CEUs
- AMBCI CBHB (Certified Behavioral Health Biller) — the only credential designed specifically for behavioral health billing
- AHIMA CCA/CCS — strong for health information management with coding pathways
- AAPC CPB (Certified Professional Biller) — billing-focused credential
- HFMA CRCR — revenue cycle representative certification
Costs range from $200–$1,500 for self-study courses to $2,500–$4,500 for bootcamps. CPC exam fees run about $399. The CBCS exam is around $300. Annual CEU maintenance costs $200–$500.
What Training Should Actually Cover
Generic medical coding programs spend 90% of their curriculum on surgical and E/M coding. Useful, but behavioral health requires mastery of different things:
- Time-based CPT code logic and the Midpoint Rule
- DSM-5-TR to ICD-10-CM diagnostic mapping
- HCPCS H-codes for SUD and facility services
- Telehealth modifiers (-95, -FQ, -93) and POS codes
- NCCI bundling edits for behavioral health code pairs
- 42 CFR Part 2 SUD confidentiality requirements
- Payer carve-out identification and routing
- Prior authorization management for IOP, PHP, and residential
Annual Updates You Must Track
ICD-10-CM codes update every October 1. CPT codes update every January 1. Missing these updates leads to rejected claims from day one of the new effective period. CMS Transmittal R11 (01/01/2026) narrowed CPT 90887 to physical activity and nutrition assessment — a change that caught many behavioral health billers off guard. G0017 and G0018 were added for non-facility crisis services. These aren’t optional updates.
Self-Study vs Formal Training
Free resources exist — YouTube coding channels, AAPC forums, CMS behavioral health webinars, the AMA BH coding guide PDF. They’re a decent start. But they don’t prepare you for the denial resolution logic that separates competent billers from excellent ones. If you’re serious about this field, structured training from AAPC or AMBCI with a certification exam is worth the investment. The salary premium for certified BH specialists runs 15–20% above non-certified peers, with experienced specialists earning $52,000–$72,000 and senior auditors exceeding $90,000.
The experience catch-22 is real — entry-level BH jobs want 2–3 years experience. The bridge is taking a front desk, patient access, or revenue cycle associate role at a behavioral health clinic while pursuing certification.
Skip the Learning Curve — Let Specialists Handle Your Billing
Instead of training staff on behavioral health coding, let EliteMed’s certified billing team handle it. We know every CPT code, modifier, and payer rule in this specialty — so you can focus on patient care.
Mental Health Billing Services →Behavioral Health Billing Software vs Outsourced Billing
This is the question every practice owner eventually faces: handle billing in-house using software, or hand it to a specialized company? The answer isn’t one-size-fits-all. But the math usually points in a clear direction.
In-House Software — What It Gives You
Platforms like TherapyNotes ($49–99/provider/month), SimplePractice ($29–99/month), Valant ($300–500/month for BH-specific features), AdvancedMD ($400+/month), and BehaveHealth ($200–400/provider) let your team handle scheduling, documentation, and claim submission from a single system.
The appeal is control. You see every claim in real time. You own the data. Corrections happen immediately.
The problem: software transmits claims. It doesn’t resolve denials. When a CO-97 bundling denial comes back on a 90791 + 96127 pairing, your biller needs to know whether modifier -59 was missing, whether the documentation supports separate sessions, and whether this specific payer even accepts 96127 with that primary code. That’s not a software question. It’s an expertise question.
Outsourced Billing — What a Specialized Company Does Differently
A behavioral health billing company charges 5–10% of net collections (average around 7%) or a flat fee of $3–10 per claim. For that, you get charge entry, claim scrubbing, submission, payment posting, denial management, AR follow-up, and reporting.
The value is in what the software dashboard doesn’t show you. A specialized BH billing team has resolved every denial code across hundreds of providers and multiple payers. They know that Aetna handles 90837 documentation requests differently from Cigna. They know which Medicaid programs accept H0015 per diem versus per hour. They know when a CO-50 medical necessity denial is worth a peer-to-peer review versus a written appeal.
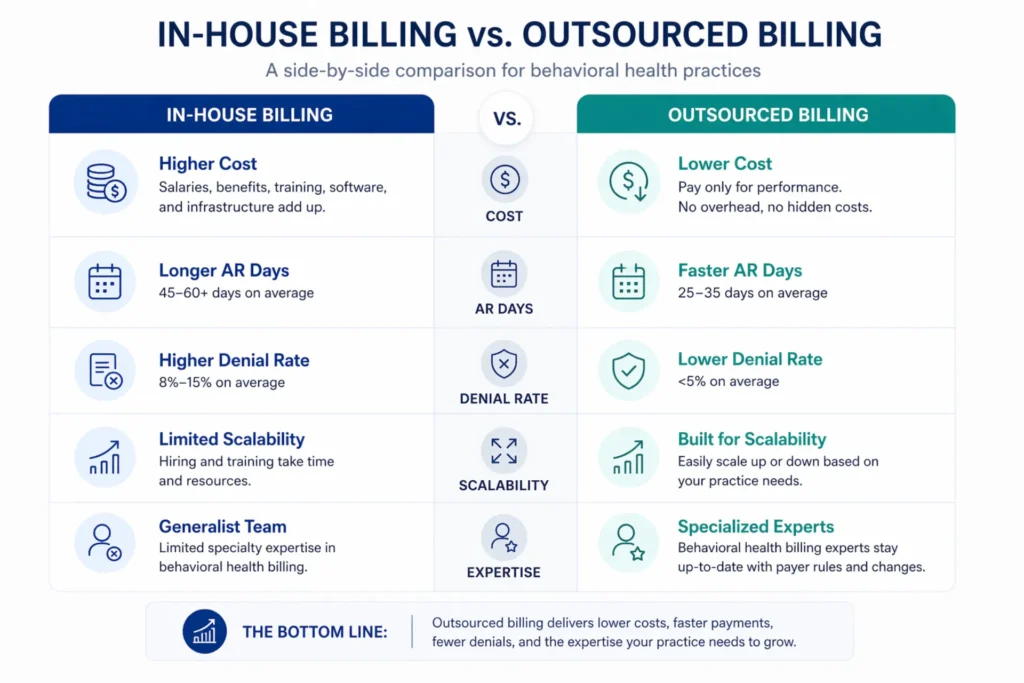
Outsourcing typically reduces AR days from 45–60 (in-house average) to 28–35 days and cuts denial rates by 30–40%.
The Real Cost Comparison
A fully loaded in-house biller costs $70,000–$100,000 per year when you add salary ($45K–$65K), benefits, software licenses, clearinghouse fees, training, and management overhead.
Outsourcing at 7% on $600,000 in annual collections costs $42,000/year.
The break-even point is roughly $700,000 in annual revenue. Below that, outsourcing is almost always cheaper. Above $1 million, the economics start favoring a dedicated in-house team — but only if you can recruit and retain a CPC-certified biller with behavioral health experience. That’s a small talent pool, and turnover kills the ROI.
Hybrid Models
The fastest-growing approach for mid-size practices: keep scheduling, eligibility, and patient-facing workflows in-house. Outsource claims submission, denial management, and aging AR to a specialized partner. This preserves front-end control while getting expert help on the back end — where the money is recovered or lost.
A Decision Framework
- Solo practice (<$300K revenue): Software is sufficient if your denial rate stays under 10%
- Small group ($300K–$1M): Hybrid or full outsourcing recommended
- Large group (>$1M): Outsource or build a dedicated in-house team with certified coders
- Denial rate >10%: Outsource immediately until the root cause is fixed
- Heavy Medicaid/carve-out payer mix: Specialized outsourcing recommended
- IOP/PHP/Residential: Full-service RCM is almost always the right call — level-of-care authorizations, daily billing, and UB-04 facility claims overwhelm most in-house teams
For detailed cost analysis, see our guide on mental health billing services cost.
| Dimension | In-House Software | Outsourced RCM | Hybrid Model |
|---|---|---|---|
| Cost | $70K–$100K/yr fully loaded | ~$42K/yr at 7% on $600K | Variable by service split |
| Control | Full real-time access | Portal-based; less day-to-day visibility | In-house retains front-end |
| Denial Expertise | Depends on staff skill | Specialized BH denial teams | Split responsibility |
| AR Days | 45–60 days | 28–35 days | Variable |
| Scalability | Fixed costs scale poorly | Variable costs align with revenue | Flexible |
| Best For | Solo (<$300K), low denial rate | Large groups, IOP/PHP/Residential | Mid-size ($300K–$1M) |
| Primary Risk | Staff turnover, expertise gaps | Vendor lock-in, transparency | Coordination complexity |
Find Out How Much Revenue You’re Leaving on the Table
EliteMed Financials provides behavioral health billing, coding, denial management, and full RCM — with denial rates under 5% and first-pass resolution above 95%.
Stop guessing. Let our team audit your current revenue cycle and show you what you’re missing.
Voice Search Q&A
What is behavioral health billing? Behavioral health billing is the process of submitting insurance claims for mental health, substance use disorder, and behavioral health services using time-based CPT codes, HCPCS codes, and ICD-10 diagnoses to collect reimbursement from payers.
What CPT codes are used for behavioral health? The most common behavioral health CPT codes are 90832 for 30-minute therapy, 90834 for 45-minute therapy, 90837 for 60-minute therapy, 90791 for psychiatric evaluation, and 90853 for group therapy. Each psychotherapy code has strict time boundaries that determine which code applies.
Is behavioral health billing the same as mental health billing? Not exactly. Mental health billing covers psychological conditions like depression and anxiety. Behavioral health billing is broader — it includes mental health plus substance use disorders, eating disorders, and behavioral modification services, with additional HCPCS codes and 42 CFR Part 2 compliance requirements for SUD records.
What is incident-to billing in behavioral health? Incident-to billing is a Medicare rule that lets therapists and counselors bill under a supervising physician’s NPI at 100% of the fee schedule rate, instead of the standard 85% rate for non-physician practitioners billing independently.
How much does outsourced behavioral health billing cost? Outsourced behavioral health billing typically costs 5 to 10 percent of net collections, with the average around 7 percent. For a practice collecting $600,000 per year, that works out to about $42,000 annually — often less than hiring a full-time in-house biller.
Is CPT 96127 a behavioral health code? Yes. CPT 96127 covers brief emotional or behavioral assessments using standardized instruments like the PHQ-9 or GAD-7. It’s billed per instrument administered, scored, and documented, with a Medicare cap of 2 to 3 units per day.
Frequently Asked Questions
What are the three types of billing in healthcare?
Professional billing covers physician services on CMS-1500 forms. Institutional billing covers facility services on UB-04 forms. Patient billing covers copays, deductibles, and coinsurance through patient statements. Behavioral health uses all three — professional for outpatient therapy, institutional for IOP and PHP, and patient billing for cost-sharing.
What is the difference between CPT 90791 and 90834?
CPT 90791 is a psychiatric diagnostic evaluation — an intake assessment done once per episode of illness (roughly every 6 months). CPT 90834 is an ongoing 45-minute psychotherapy session for 38–52 minutes of face-to-face time. They cannot be billed on the same date of service per NCCI edits.
What modifiers are used for behavioral health billing?
Common modifiers include -95 (video telehealth), -FQ (audio-only Medicare), -93 (audio-only commercial), -25 (separate E/M service same day), -59 (distinct procedural service for NCCI override), -HE (mental health program), -HF (substance use disorder program), and 90785 (interactive complexity add-on).
Who can bill CPT 99484?
Any qualified healthcare professional directing behavioral health care management services can bill 99484. Clinical staff performing the 20+ minutes of monthly care management work under the billing provider’s supervision. LCSWs and psychologists can bill G0323 for equivalent services under Medicare.
Can you bill 90834 and 96127 together?
Yes, but modifier -59 or -XU must be appended to 96127 to indicate it’s a distinct service from the therapy session. Documentation must show the screening was a separate clinical activity with its own instrument name, raw score, interpretation, and clinical action.
Is behavioral health billing harder than regular medical billing?
In most respects, yes. Time-based coding creates audit exposure that doesn’t exist in procedure-based medical billing. Payer carve-outs complicate claim routing. Prior authorization frequency is significantly higher. And documentation standards require clinical narrative defending ongoing medical necessity rather than objective test results.
How do behavioral health carve-outs affect billing?
Many commercial plans separate behavioral health benefits from medical benefits, routing them to MBHOs like Optum, Carelon, or Magellan. Claims submitted to the wrong entity — the medical carrier instead of the behavioral health administrator — produce CO-109 “plan not covered” denials.
What is the MHPAEA and how does it affect billing?
The Mental Health Parity and Addiction Equity Act requires commercial insurers to cover behavioral health benefits no more restrictively than medical and surgical benefits. This includes prior authorization frequency, session caps, and network adequacy. The 2024 final rule requires payers to provide NQTL comparative analyses upon written request.
How often should treatment plans be updated?
CMS requires treatment plan updates every 3–6 months for ongoing therapy. Plans must include the diagnosis, treatment modality, session frequency, estimated duration, and measurable goals. Missing or outdated treatment plans are a top documentation audit trigger for behavioral health claims.
What is 42 CFR Part 2 and when does it apply?
42 CFR Part 2 governs the confidentiality of substance use disorder treatment records. It requires separate written patient consent before SUD information can be disclosed — even for payment. As of February 16, 2026, Part 2 aligns with HIPAA, allowing a single TPO consent for treatment, payment, and operations while maintaining the written consent requirement.
Wrapping Up
Behavioral health billing isn’t a subset of medical billing. It’s a parallel system with its own codes, its own time rules, its own payer ecosystem, and its own compliance requirements. The practices that treat it like general medical billing are the ones running 25–30% denial rates and leaving revenue on the table.
Getting it right requires precision at every step — from verifying carve-out benefits before the first session to documenting exact start and stop times, selecting the correct telehealth modifier, and knowing when incident-to billing applies and when it creates audit exposure.
Whether you handle billing in-house or work with a specialized mental health billing partner, the fundamentals in this guide are the operational baseline. Master them, and your revenue cycle starts working the way it should.
Behavioral Health Billing, Coding, Credentialing & Full RCM
EliteMed Financials
We serve behavioral health practices nationwide with HIPAA-compliant billing, certified coding, provider credentialing, denial management, and complete revenue cycle management. Your claims. Our expertise.

