Every mental health practice owner I talk to says the same thing: “We’re HIPAA compliant.” Then I ask one question — “Can you show me your last risk assessment?” — and the room goes quiet.
Here’s the reality. HIPAA violations don’t just trigger fines. A single OCR investigation costs $15,000 to $100,000 in legal fees before any penalty lands. The actual civil penalties run up to $2,190,000 per violation category.
And for mental health practices? The stakes climb even higher. Mental health PHI carries what compliance attorneys call a “stigma multiplier.” A data breach involving depression diagnoses or substance use disorder records doesn’t just violate privacy — it can destroy a patient’s career, custody arrangement, insurance standing, and social relationships.
If your practice bills mental health services — or if you outsource that billing to a third-party company — HIPAA compliance in mental health billing is the single most important operational risk you manage. Not coding accuracy. Not claim volume. Compliance.
This guide breaks down every regulatory layer your billing operation must address in 2026.

Quick Definition: HIPAA compliance in mental health billing refers to the set of federal regulations governing how protected health information (PHI) is used, stored, transmitted, and disclosed during the billing lifecycle. It includes the HIPAA Privacy Rule, Security Rule, and Breach Notification Rule, plus the 42 CFR Part 2 overlay for substance use disorder records.
Table of Contents
Why HIPAA Compliance in Mental Health Billing Is Non-Negotiable
Let me put numbers to this so there’s no ambiguity.
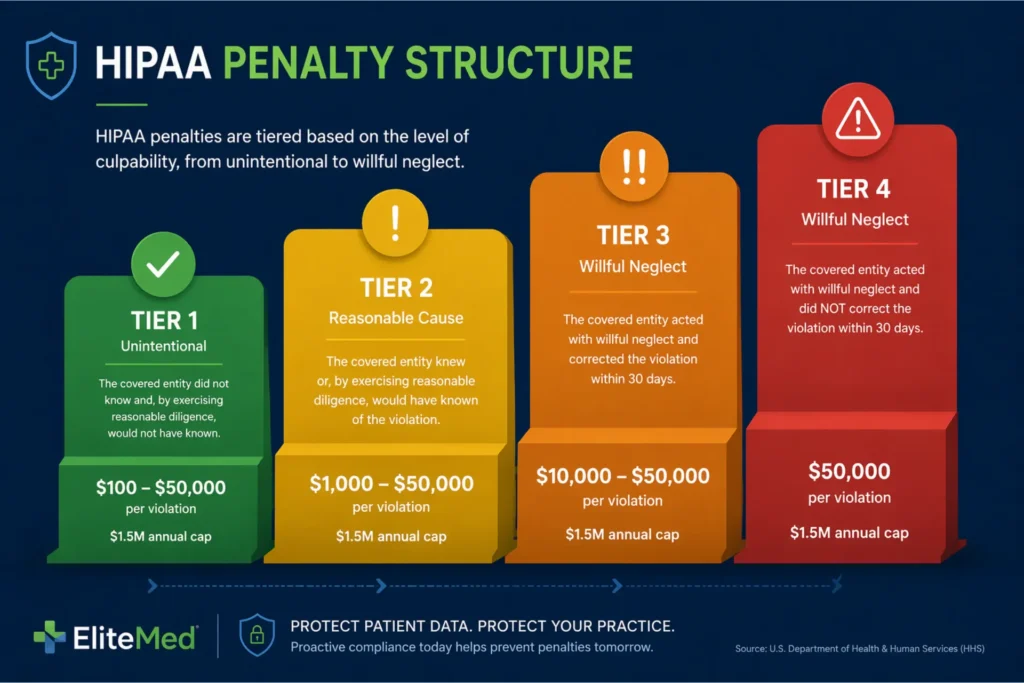
The Four-Tier Civil Penalty Structure (2026)
The Office for Civil Rights (OCR) enforces HIPAA penalties under a four-tier civil structure defined in 45 CFR §160.404. These figures adjust annually for inflation. Here’s where we are in 2026:
- Tier 1 — No Knowledge: $141 to $36,500 per violation. Annual cap: $36,500.
- Tier 2 — Reasonable Cause: $1,424 to $73,011 per violation. Annual cap: $146,000.
- Tier 3 — Willful Neglect, Corrected: $14,602 to $73,011 per violation. Annual cap: $2,190,000.
- Tier 4 — Willful Neglect, Not Corrected: $73,011 to $2,190,000 per violation. Annual cap: $2,190,000.
That $2,190,000 cap is per category of violation. A single ransomware incident can trigger multiple categories — one for Security Rule failures, another for Breach Notification delays. The exposure compounds fast.
Criminal Penalties Most Practices Don’t Realize Exist
Criminal penalties under 42 U.S.C. §1320d-6 escalate quickly:
- Unknowing violations: up to 1 year imprisonment
- Obtaining PHI under false pretenses: up to 5 years
- Intentional misuse for personal gain or malicious harm: up to 10 years
This isn’t theoretical. Billing employees have been prosecuted for selling SUD diagnosis data. Staff members have faced criminal charges for accessing celebrity client records.
Why Mental Health PHI Is Different
When a cardiology practice suffers a breach, patients face identity theft risk. When a mental health practice suffers a breach, patients face employment discrimination, custody challenges, insurance denials, and social stigma.
ICD-10 codes in the F10-F99 range — covering substance use disorders, schizophrenia, mood disorders, anxiety, and trauma — are among the most sensitive data points in all of healthcare. This stigma multiplier is why OCR treats mental health breaches with heightened scrutiny.
The 42 CFR Part 2 Layer
If your practice treats patients with substance use disorders (SUD), you’re not just bound by HIPAA. 42 CFR Part 2 imposes stricter consent requirements on SUD records.
Under the 2024 Final Rule that aligned Part 2 with HIPAA, a patient can now provide a single “General Designation Consent” for treatment, payment, and operations (TPO). But your billing company still needs a Qualified Service Organization Agreement (QSOA) — not just a BAA — to handle those SUD claims.
Many practices don’t know this. That gap is where Tier 3 and 4 penalties live.
Your Billing Company Is Directly Liable Too
Since the Omnibus Rule of 2013, business associates — including billing companies, clearinghouses, and offshore coders — face the same penalty structure as covered entities. Your billing vendor’s HIPAA failure is your HIPAA failure.
If you’re still building your understanding of how mental health billing works, start with the complete beginner’s guide to mental health billing before diving deeper here.
The Three HIPAA Rules Applied to Mental Health Billing
HIPAA isn’t one rule. It’s three distinct frameworks that govern different aspects of your billing operation.
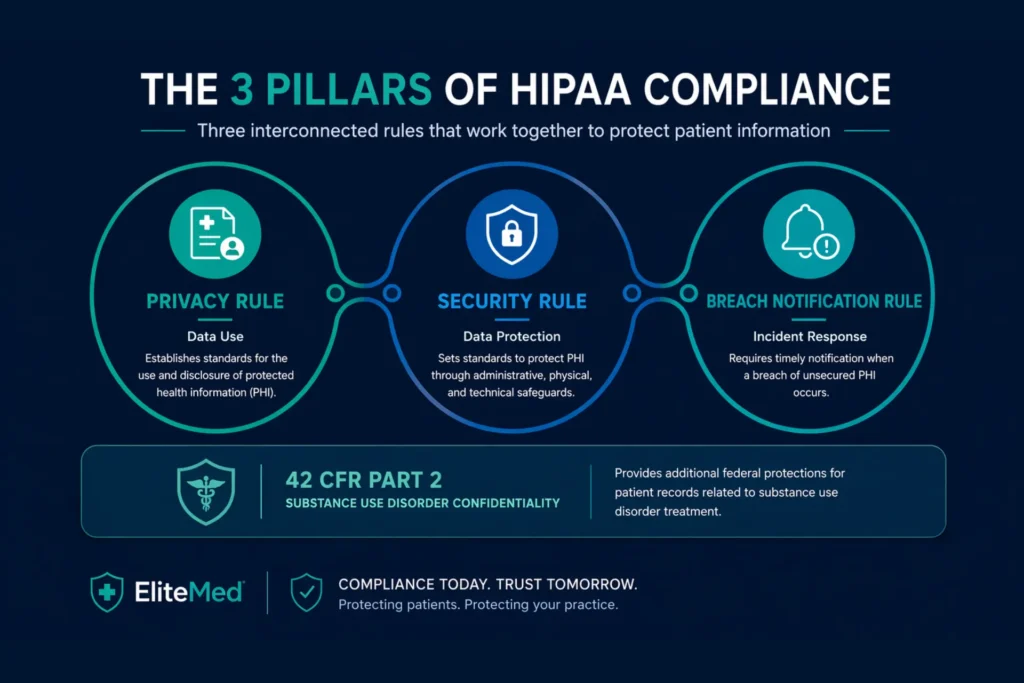
The Privacy Rule: Who Sees What
The Privacy Rule controls what data gets used and who sees it. Under 45 CFR §164.502(b), the “minimum necessary” standard requires that billing staff access only the PHI needed for their specific task.
A biller submitting claims needs:
- Patient name and date of birth
- Member ID and insurance details
- CPT codes and ICD-10 diagnosis codes
- Dates of service and charge amounts
They don’t need access to the full clinical chart. They absolutely don’t need access to psychotherapy notes.
Psychotherapy Notes vs. Progress Notes
This distinction matters. Under 45 CFR §164.501, psychotherapy notes — the therapist’s personal process notes — receive special protection. They require specific patient authorization for any use, including payment.
Progress notes used for billing purposes are a separate category. If your billing company can open psychotherapy notes in your EHR, that’s a minimum necessary violation waiting to happen.
The Security Rule: How Data Is Protected
The Security Rule controls how electronic PHI (ePHI) is protected. It mandates three categories of safeguards:
Administrative Safeguards (9 standards) — including risk analysis, workforce security, security awareness training, and contingency planning. The annual risk analysis under §164.308(a)(1) is the single most important HIPAA document your practice maintains.
Physical Safeguards (4 standards) — covering facility access controls, workstation use and security, and device and media controls. If your billing staff work remotely — and most do in 2026 — their home office setup falls under these requirements.
Technical Safeguards (5 standards) — including access control, audit controls, integrity controls, authentication, and transmission security. These carry the heaviest compliance burden for billing because claims data moves through multiple systems.
Required vs. Addressable: Don’t Get Fooled
A critical concept: the Security Rule distinguishes between “required” and “addressable” implementation specifications.
Addressable doesn’t mean optional. It means you must implement the specification or document why an equivalent alternative is reasonable.
For mental health billing data — given the stigma multiplier — encryption (AES-256 at rest, TLS 1.2+ in transit) and multi-factor authentication are the documented “reasonable and appropriate” controls. Skipping them without a documented alternative is willful neglect.
The Breach Notification Rule: The 60-Day Clock
Under 45 CFR §§164.400–414, if unsecured PHI is breached, you must notify affected individuals within 60 days of discovery.
Breaches affecting 500 or more individuals also require notification to HHS OCR and prominent media outlets in the affected state. Smaller breaches must be reported to HHS annually.
The 60-day clock starts on “Day 0” — the date anyone in your organization (or your billing company) first learns of the breach. Not the date you confirm it. Not the date you investigate it. The date you become aware of it.
A billing vendor who discovers a breach on March 1 and doesn’t tell you until April 15 has consumed 45 of your 60 days.
The 4-Factor Breach Risk Assessment
Before the clock starts, the 4-factor breach risk assessment under §164.402(b) determines whether the incident qualifies as a breach:
- The nature and extent of the PHI involved
- Who accessed or received the unauthorized disclosure
- Whether the PHI was actually acquired or viewed
- What mitigation was taken to reduce risk
For mental health billing data, Factor 1 almost always registers as high-risk because F-codes reveal psychiatric diagnoses.
How 42 CFR Part 2 Layers On Top
For SUD billing, all three HIPAA rules apply plus Part 2’s stricter consent and disclosure requirements.
Your billing company needs both a BAA and a QSOA. The 2024 Final Rule allows a General Designation Consent for TPO, but every claim containing SUD data (F10-F19 codes) must include a “Notice to Accompany Disclosure” embedded in the claim notes segment.
A standard BAA alone is legally insufficient for SUD billing.
For a deeper look at the revenue cycle stages where these rules intersect, see the guide on mental health revenue cycle management.
Business Associate Agreements: Your Primary Legal Shield
A one-page BAA from a billing company isn’t streamlined. It’s legally deficient.
Under 45 CFR §164.504(e), a compliant Business Associate Agreement must contain 12 specific provisions. These aren’t suggestions. They’re statutory requirements. If any are missing, the BAA fails to provide “satisfactory assurances” under §164.502(e)(2) — and sharing PHI under that agreement becomes an impermissible disclosure.
The 12 Required BAA Provisions
Every BAA for a mental health billing company must include:
- Permitted uses and disclosures — limiting PHI use to claims submission, payment posting, and denial management
- Prohibition on non-permitted uses — the billing company cannot sell patient lists or use PHI outside the contract
- Minimum necessary standard — billing access limited to only the data needed for the billing task
- Patient rights preservation — support for accounting of disclosures and other patient rights
- Breach reporting — best practice: within 5 business days of discovery
- HHS audit access — vendor must turn over records during OCR investigations
- Subcontractor compliance — signed BAAs required with every downstream vendor
- PHI return or destruction — certificate of destruction required upon contract end
- Covered entity authorization — support for legally required disclosures
- Prohibition on further re-disclosure — no sharing with investors, affiliates, or other clients
- Breach notification timelines — aligned with §164.410
- Agent/subcontractor flow-down — downstream vendors bound by identical restrictions
The Subcontractor Chain Problem
Mental health billing often involves multiple handoffs:
Practice → Billing Company → Clearinghouse → Offshore Coder
Under §164.504(e)(2)(ii)(D), every link in that chain needs a BAA. If your billing company’s offshore coding partner doesn’t have a signed BAA and suffers a breach, both the billing company and your practice are liable.
BAA vs. QSOA for SUD Billing
If your practice bills any SUD codes (F10-F19), a standard BAA is not enough. 42 CFR Part 2 §2.12(c) requires a separate Qualified Service Organization Agreement (QSOA).
The QSOA prevents the billing company from re-disclosing SUD data in a lawsuit or to a downstream vendor without the patient’s consent.
The most efficient approach: a dual-purpose BAA/QSOA agreement that incorporates both HIPAA and Part 2 language.
8 Red Flags in a BAA
Walk away — or at minimum renegotiate — if you see any of these:
- The agreement is less than 2 pages (can’t physically contain 12 required elements)
- No breach notification timeline specified
- Missing subcontractor language
- No data destruction clause
- Template predates 2013 (pre-Omnibus)
- No QSOA language for SUD billing
- The vendor refuses to negotiate any terms
- The person signing lacks authority

The HHS Model BAA Template is the safe-harbor standard. Any billing vendor whose BAA deviates significantly from it without clear justification should trigger a deeper review.
Understanding what you’re paying for matters too. Review the breakdown of mental health billing services costs to see how compliance infrastructure factors into pricing.
Is Your Billing Company’s BAA Missing Critical Provisions?
EliteMed Financials maintains fully Omnibus-compliant BAAs with 5-business-day breach notification, subcontractor chain documentation, and QSOA integration for SUD practices.
Review Our Mental Health Billing Services →How to Evaluate Your Billing Company’s HIPAA Compliance
A billing company claiming “HIPAA compliance” without evidence is like a restaurant claiming health department approval without a posted inspection score. The claim is meaningless without verification.
The “HIPAA Certified” Myth
There is no official “HIPAA certification.” OCR has stated this explicitly. What exists is third-party validation through recognized security frameworks — and those frameworks differ significantly in rigor.
SOC 2 Type II: The Minimum Market Standard
A SOC 2 Type II report demonstrates that a vendor’s security controls operated effectively over a 6-to-12-month period, audited against five Trust Service Criteria:
- Security
- Availability
- Processing Integrity
- Confidentiality
- Privacy
Look for an unqualified opinion (clean report). A qualified opinion means the auditor found material control failures — a serious red flag. If the report is older than 6 months, request a Bridge Letter confirming continued compliance.
HITRUST CSF: The Gold Standard
HITRUST CSF certification — available at r2, i1, and e1 levels — maps directly to HIPAA requirements and is considered the gold standard for healthcare data protection.
A billing company offering only a self-attested “HIPAA compliance letter” with no third-party validation should not handle your patients’ mental health data.
10 Questions to Ask Before Signing
Question 1: Can you share your current BAA template? Acceptable: post-2013 Omnibus-compliant agreement with 5-business-day breach notification. Red flag: refusal to share, or template shorter than 2 pages.
Question 2: Who are your designated HIPAA Privacy Officer and Security Officer? Acceptable: named individuals with contact information. Red flag: “We don’t have one” or “IT handles that.”
Question 3: When was your last risk assessment — can we see a summary? Acceptable: annual assessment with findings and remediation plans. Red flag: “We’ve never done one.”
Question 4: What encryption standards do you use? Acceptable: AES-256 at rest, TLS 1.2+ in transit. Red flag: “We don’t encrypt” or “email is plaintext.”
Question 5: How do you handle offshore staff access to PHI? Acceptable: role-based access, MFA, downstream BAAs, training documentation. Red flag: “Offshore teams have open access.”
Question 6: What’s your written breach notification timeline to us? Acceptable: 5 business days. Red flag: “We’ll notify you promptly” with no defined clock.
Question 7: Have you had any reported HIPAA breaches in the last 3 years? Verify independently by searching the HHS Breach Portal at breachportal.hhs.gov. Multiple entries signal systemic governance failures.
Question 8: What’s your access control model? Acceptable: Role-Based Access Control (RBAC) with unique user IDs and MFA. Red flag: “We use one shared login for the billing team.”
Question 9: Do you hold SOC 2 Type II or HITRUST certification? Acceptable: current third-party validation on file. Red flag: only a self-attested compliance letter.
Question 10: How do you destroy PHI when our contract terminates? Acceptable: documented process with signed certificate of destruction within 30 days. Red flag: “We keep historical data” with no retention schedule.
7 Documents to Request
Before signing any BAA, demand:
- Current BAA template
- Written HIPAA policies and procedures manual
- Annual risk assessment summary
- Workforce training records
- Incident response plan
- Third-party security assessment (penetration test summary)
- Subcontractor list with downstream BAA evidence
Refusal to provide any of these is a termination-level red flag.
Switching Billing Companies: The Transition Protocol
When switching vendors, demand a certificate of destruction from the outgoing vendor. Manage the 60-day tail period for AR follow-up while immediately cutting off access to new patient data.
For a full framework on selecting the right partner, see the guide on how to choose a mental health billing service.
8 Common HIPAA Violations in Mental Health Billing
These eight violations account for the majority of HIPAA enforcement actions related to billing. Every one of them is preventable.
Violation 1: No BAA or Expired BAA
This is the single most common — and most easily avoidable — violation.
A practice sharing PHI with a billing company, clearinghouse, or cloud vendor without a signed BAA violates 45 CFR §164.502(e)(2).
Here’s the math that should concern you: 100 patients × 365 days without a BAA = 36,500 distinct violations. At the Tier 4 floor of $73,011 per violation, exposure reaches the $2,190,000 annual cap almost immediately.
Fix: Maintain a BAA register with start dates, expiration dates, and 30-day renewal reminders.
Violation 2: Minimum Necessary Failure
Billing staff with full EHR access who can read psychotherapy notes, unrelated clinical history, or other patients’ records violate §164.502(b).
This happens constantly when practices give billing companies “global admin” EHR credentials instead of role-restricted accounts.
Fix: Configure role-based access control (RBAC) so billers see only the financial and demographic tabs — name, member ID, CPT/ICD-10 codes, dates of service, and charge amounts.
Violation 3: Unsecured PHI Transmission
Sending claims, EOBs, or patient statements via unencrypted email or standard FTP violates §164.312(e)(2).
An email containing a patient’s F41.1 generalized anxiety disorder code sent over basic Gmail is a breach waiting to happen.
Fix: Mandate SFTP or HTTPS portals for all claims data. Use HIPAA-compliant email platforms with signed BAAs for any billing correspondence containing PHI.
Violation 4: Inadequate Workforce Training
HIPAA requires documented annual training under §164.530(b). A verbal “don’t share patient info” at orientation doesn’t count.
OCR looks for sign-in sheets, training content documentation, quiz scores, and completion certificates.
Fix: Annual documented training covering minimum necessary, phishing awareness, password hygiene, MFA usage, incident reporting, and 42 CFR Part 2 rules for SUD practices. Budget $50–$200 per person per year for platforms like MedTrainer or HSC Health.
Violation 5: Improper PHI Disposal
Printed EOBs and patient ledgers in an unlocked trash can. Decommissioned hard drives donated or sold without wiping. Both violate §164.530(c) and §164.310(d).
Fix: Cross-cut shredding for paper. NIST 800-88-compliant data destruction for electronic media. Document every disposal with a log entry.
Violation 6: Unauthorized Access (Snooping)
A billing employee opens a celebrity client’s chart out of curiosity. A staff member checks their ex-spouse’s records.
These violate §164.502(a) and can trigger criminal penalties under 42 U.S.C. §1320d-6 if motivated by personal gain.
Fix: Enable audit logs on all sensitive record access and review them quarterly. Enforce your sanctions policy consistently.
Violation 7: Missed 60-Day Breach Notification Deadline
Your billing vendor discovers a ransomware attack on Day 1. They spend three weeks investigating internally before telling you on Day 22. You then take another 45 days to notify patients. You’ve just missed the 60-day federal deadline under §164.404.
Fix: Require 5-business-day vendor breach notification in your BAA. Maintain pre-drafted notification letter templates. Create a breach response playbook with a Day 30–45 risk assessment trigger.
Violation 8: 42 CFR Part 2 SUD Disclosure Without Consent
A billing company submits a claim with an F11.20 (opioid use disorder) diagnosis code to an employer-sponsored health plan without a valid General Designation Consent.
The employer’s HR department sees the code on the EOB. The patient loses their job.
Under the 2024 Final Rule, this violation now carries civil penalties enforced by OCR with the same $2,190,000 annual cap.
Fix: Flag all SUD claims for Part 2 review before submission. Obtain General Designation Consent. Require a QSOA with every billing vendor handling SUD data.
The Change Healthcare Lesson
In February 2024, the ALPHV/BlackCat ransomware group attacked Change Healthcare — the largest healthcare clearinghouse in the United States, processing roughly 40% of all US claims.
The breach exposed over 100 million records. UnitedHealth Group paid a $22 million ransom. The system outage lasted six weeks.
During those six weeks, practices couldn’t submit claims, post payments, or verify eligibility. OCR opened an investigation.
The entry point? A Citrix remote access portal without multi-factor authentication.

For mental health practices, this breach proved three things:
- Single-clearinghouse dependency is an existential risk
- MFA is non-negotiable
- Your billing company’s security failures become your revenue disruption
Worried About Compliance Gaps in Your Billing Workflow?
EliteMed Financials operates with role-based access controls, encrypted data transmission, documented workforce training, and multi-clearinghouse redundancy to protect your revenue and your patients.
Talk to Our Mental Health Billing Team →Secure Data Transmission in Mental Health Billing
The Change Healthcare breach wasn’t caused by a sophisticated zero-day exploit. It was caused by a missing MFA configuration on a remote access portal.
The most devastating healthcare breach in US history started with a basic security control that someone didn’t enable.
In 2026, secure data transmission is the technical baseline for mental health billing compliance — not an advanced security feature.
Encryption Standards You Must Meet
Under 45 CFR §164.312(e)(2)(ii), transmission security is technically an “addressable” specification. But for mental health billing data, the documented reasonable and appropriate controls are:
- AES-256 encryption at rest
- TLS 1.2 or TLS 1.3 in transit
Failing to implement these without a documented equivalent alternative is treated as willful neglect by OCR.
Every device that touches billing data — laptops, desktops, tablets — must have full-disk encryption enabled (BitLocker for Windows, FileVault for Mac). Every connection to a clearinghouse, payer portal, or EHR must use TLS-encrypted channels.
Email: The Weakest Link in Billing
More HIPAA violations originate from email than any other transmission method.
An email platform is only HIPAA-compliant for billing if it meets three requirements:
- Signed BAA from the email provider
- End-to-end encryption (AES-256 plus TLS)
- Audit logging of who sent what, when, and who opened it
HIPAA-compliant email platforms: Paubox (seamless encrypted delivery), Virtru (client-side encryption plugin), Google Workspace with a HIPAA BAA, Microsoft 365 with a HIPAA BAA.
NOT compliant — do not use for PHI: Basic Gmail free accounts, Yahoo Mail, WhatsApp, standard SMS, consumer Dropbox, Facebook Messenger.
Using any of these for billing communications containing PHI is a Tier 2-3 violation.
Secure File Transfer Methods
Claims files, reports, and patient data must move through secure channels.
Acceptable: SFTP (SSH File Transfer Protocol), HTTPS portal uploads, VPN-tunneled connections.
Not acceptable: Standard FTP (transmits data in plaintext), consumer cloud share links.
Ban FTP entirely from your billing operation.
Clearinghouse Diversification After Change Healthcare
No practice should route more than 60-70% of claims through a single clearinghouse.
Maintain credentials with at least two clearinghouses — Waystar, Availity, Trizetto, or a regional alternative. Demand SOC 2 Type II reports from each.
This is now a contractual requirement for practices that take revenue continuity seriously.
Multi-Factor Authentication: The Non-Negotiable
Under §164.312(d), every billing portal must require multi-factor authentication.
TOTP-based authenticators (Google Authenticator, Authy) are the 2026 standard. SMS-based MFA is weaker due to SIM-swapping vulnerabilities.
Every billing user must have a unique user ID — shared logins are a Security Rule violation. Automatic session timeout should be set to 15 minutes.
And when a billing staff member leaves? Access must be revoked within one hour of termination. Not end of day. Not end of week. One hour.
Audit Logs: The 6-Year Retention Rule
Under §164.312(b), every system touching ePHI must log who accessed what, when, and from where.
These logs must be retained for at least 6 years and reviewed quarterly by your designated Security Officer.
Flag unusual patterns: mass data exports, off-hours access, access from unfamiliar IP addresses.
ERA Files Are PHI
Electronic Remittance Advice (835 files) contain patient names, diagnosis codes, service dates, and payment amounts.
They must be stored in encrypted databases with access restricted to payment posting staff only. Unencrypted email delivery of ERA files is a violation.
For practices managing their own payment posting and claim submission, these secure transmission requirements apply at every stage.
For authoritative reference on enforcement actions and Security Rule requirements, visit the HHS OCR Compliance and Enforcement page and the full text of 45 CFR Part 164.
The Complete HIPAA Compliance Checklist for Mental Health Billing
HIPAA compliance is governed by one principle that overrides everything else: “If it isn’t documented, it didn’t happen.”
OCR doesn’t accept verbal assurances. During an investigation, they request documents. If the document doesn’t exist, the compliance activity didn’t exist. Every record must be retained for 6 years.
The good news: OCR evaluates practices on a “reasonable good faith” standard. A practice demonstrating five elements is positioned for Tier 1-2 findings rather than Tier 3-4 penalties.
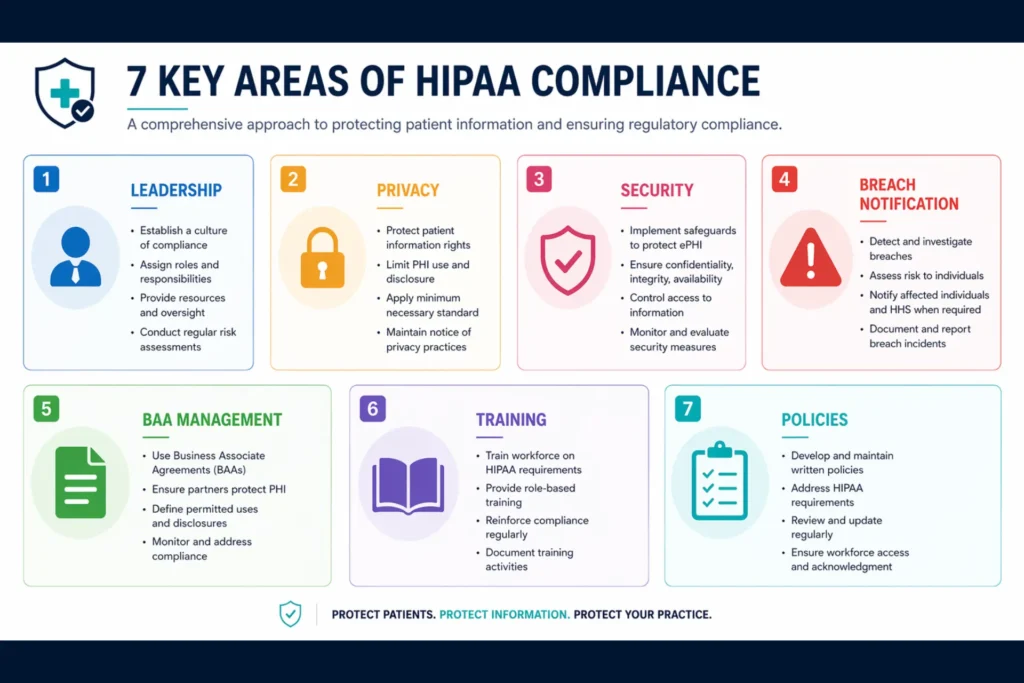
Category 1: Leadership and Governance
- Designate a HIPAA Privacy Officer in writing
- Designate a HIPAA Security Officer in writing (§164.308(a)(2))
- In small practices, the practice manager often fills both roles
- Publish officer names and contact information
- Document all appointments and review annually
Category 2: Privacy Rule Compliance
- Provide a current Notice of Privacy Practices (NPP) to every patient
- Apply the minimum necessary standard to all billing disclosures
- Document role-based access justification for each billing position
- Maintain an accounting of disclosures system capable of 60-day response
- Separate psychotherapy notes from billing-accessible records
Category 3: Security Rule Compliance
- Conduct an annual Security Risk Assessment using the free HHS SRA Tool at healthit.gov
- Document the 3-part output: assessment, risk management plan, implementation evidence
- Implement unique user IDs, RBAC, auto-logoff, AES-256 encryption, audit logging
- Maintain a contingency and backup plan
- Implement immediate access revocation on staff termination
The annual SRA is the most important document in your entire compliance program. A missing SRA is an automatic Tier 3-4 escalation trigger.
Category 4: Breach Notification Readiness
- Maintain a written incident response plan
- Document 4-factor risk assessments for every security incident
- Keep pre-drafted notification letter templates ready
- File annual small-breach HHS report for incidents under 500 individuals
Category 5: BAA and Vendor Management
- Maintain a BAA inventory listing every vendor that touches PHI
- Verify all BAAs are Omnibus-compliant with 12 required elements
- Ensure 5-business-day breach notification language is present
- Confirm QSOAs are in place for SUD practices
- Search the HHS Breach Portal annually for each vendor
- Demand SOC 2 Type II reports or HITRUST certifications
- Review vendor security annually
Category 6: Workforce Training
Train all staff annually on:
- HIPAA fundamentals and minimum necessary
- PHI handling in billing workflows
- Email and transmission security
- Phishing awareness and password hygiene
- MFA usage and incident reporting
- 42 CFR Part 2 rules (if applicable)
Train new hires before they access PHI. Document everything. Budget $50–$200 per person per year.
Category 7: Policies and Procedures
Adopt the seven minimum required policies:
- Privacy Policy
- Security Policy
- BAA Management Policy
- Breach Response Policy
- Social Media Policy
- Workforce Sanctions Policy
- Device/Media Disposal Policy
Review and update all policies annually — January is the standard reset month. Distribute to all staff with signed acknowledgment forms.
Realistic Implementation Timeline
Moving from compliance zero to compliance ready takes 6 to 12 months for a small practice.
Start here: the BAA inventory. It’s the highest-priority, highest-ROI action.
Then: schedule the HHS SRA Tool session. Build policies and training from there.
For external validation: budget $3,000–$7,500 for a third-party HIPAA audit every 2-3 years.
HIPAA Compliance Checklist for Mental Health Billing (2026)
Track your practice’s compliance across all 7 required categories. Check off completed items to see your progress.
All 35 items completed — your compliance framework is in place.
Ready to Work With a Billing Partner That Treats Compliance as Infrastructure?
EliteMed Financials maintains documented risk assessments, role-based access controls, encrypted data transmission, and full BAA/QSOA documentation — so your compliance posture is bulletproof from Day 1.
Voice Search Q&A: HIPAA Compliance in Mental Health Billing
What is HIPAA compliance in mental health billing?
HIPAA compliance in mental health billing means following federal rules that protect patient health information during the entire billing process. It covers how data is used, stored, transmitted, and disclosed — from the moment a claim is created through payment posting and patient statements. Mental health billing has extra requirements because diagnoses like depression, anxiety, and substance use disorders carry heightened sensitivity.
What are the HIPAA penalties for mental health billing violations?
HIPAA civil penalties for mental health billing violations range from $141 per violation for unknowing errors up to $2,190,000 per violation category per year for willful neglect that isn’t corrected. Criminal penalties can reach 10 years imprisonment for intentional misuse of patient data. The penalty tier depends on whether the practice knew about the violation and whether they tried to fix it.
Does my billing company need a BAA for mental health billing?
Yes. Under federal law, any company that handles protected health information for billing purposes must have a signed Business Associate Agreement before receiving any patient data. Operating without a BAA is one of the most common HIPAA violations and can trigger penalties up to the annual cap of $2,190,000.
What is 42 CFR Part 2 and how does it affect mental health billing?
42 CFR Part 2 is a federal regulation that provides extra privacy protections for substance use disorder patient records. It requires stricter consent before SUD diagnosis codes can be shared with insurers or billing companies. If your practice treats patients for alcohol or opioid use disorders, your billing company needs a Qualified Service Organization Agreement in addition to the standard BAA.
How do I know if my billing company is HIPAA compliant?
Verify compliance by requesting a signed BAA with all 12 required provisions, a current SOC 2 Type II report with an unqualified opinion, annual risk assessment documentation, workforce training records, and an incident response plan. Search the HHS Breach Portal for their name. Ask who their designated HIPAA Security Officer is. If they can’t answer these questions, they shouldn’t be handling your patient data.
Frequently Asked Questions
What happens if a mental health billing company violates HIPAA?
The billing company faces its own penalties — since 2013, business associates are directly liable under HIPAA. Penalties follow the same four-tier structure as covered entities, reaching up to $2,190,000 per violation category annually. The practice that hired them may also face penalties for failing to conduct adequate vendor due diligence or for operating without a proper BAA. An OCR investigation typically spans 6 to 18 months of data analysis, with legal defense costs ranging from $15,000 to $100,000 before any settlement.
Is there a difference between HIPAA and 42 CFR Part 2 for billing?
Yes. HIPAA governs all protected health information and allows data sharing for treatment, payment, and operations under the TPO framework without additional patient consent for each transaction. 42 CFR Part 2 adds stricter requirements specifically for substance use disorder records — requiring explicit patient consent before SUD diagnosis codes can be shared with payers or billing companies. A practice treating SUD patients needs both a BAA and a QSOA with their billing vendor.
Can a patient sue a therapist for billing-related HIPAA violations?
HIPAA itself doesn’t create a private right of action — patients can’t sue directly under HIPAA. However, patients can file complaints with HHS OCR that trigger investigations, and they can pursue state-law claims for negligence, breach of confidentiality, or violations of stricter state privacy laws. In states like California (CMIA), Illinois (MHDDCA), or New York (Mental Hygiene Law §33.13), patients have additional legal avenues beyond federal HIPAA protections.
What is the minimum necessary standard in mental health billing?
The minimum necessary standard under 45 CFR §164.502(b) requires that billing staff access only the protected health information needed for their specific task. A biller submitting claims needs patient demographics, insurance details, CPT codes, and ICD-10 diagnosis codes. They do not need access to full clinical charts, psychotherapy notes, or unrelated medical history. Practices must configure their EHR systems with role-based access controls that restrict billing staff to financial and demographic data only.
How often should a mental health practice conduct a HIPAA risk assessment?
At minimum, annually. The Security Risk Assessment under 45 CFR §164.308(a)(1) is the foundational HIPAA compliance document — OCR requests it first in every investigation. The HHS SRA Tool at healthit.gov provides a free, structured framework. Practices should also conduct risk assessments after any significant change: new billing vendor, new EHR system, office relocation, transition to remote billing staff, or after any security incident.
Is emailing patient billing statements a HIPAA violation?
Not automatically — but it is if the email isn’t properly secured. A HIPAA-compliant email for billing requires three things: a signed BAA from the email provider, end-to-end encryption (AES-256 plus TLS), and audit logging. Platforms like Paubox, Virtru, Google Workspace with a BAA, and Microsoft 365 with a BAA meet these standards. Basic Gmail, Yahoo, WhatsApp, and SMS do not. Sending an unencrypted email containing a patient’s diagnosis code is a transmission security violation under §164.312(e).
What should I do if my billing company has a data breach?
Your billing company should notify you within 5 business days of discovering the breach — verify this timeline is in your BAA. Once notified, conduct a 4-factor breach risk assessment under §164.402(b) to determine severity. If the breach qualifies, you must notify affected patients within 60 days of the breach discovery date. For breaches affecting 500 or more individuals, you must also notify HHS OCR and prominent media in the affected state. Document every step. Engage healthcare counsel immediately. Begin planning for denial management and AR follow-up disruptions if the breach affects your clearinghouse connectivity.
Does HIPAA apply to offshore billing companies?
Yes. HIPAA applies to any entity that handles PHI on behalf of a US covered entity, regardless of geographic location. Offshore billing companies must sign a BAA, comply with all Security Rule safeguards, and maintain the same access controls as domestic vendors. The practical challenge is that OCR’s enforcement leverage diminishes offshore, making contractual protections — downstream BAAs, indemnification clauses, clean desk policies, and right-to-audit provisions — even more critical. Practices should demand documentation of offshore security controls and conduct annual vendor reviews.
Building a Compliance-First Billing Operation
HIPAA compliance in mental health billing isn’t a checkbox you tick once a year. It’s an operational system that runs continuously — assessing risk, documenting controls, training staff, reviewing vendors, and adapting to new threats.
What Compliance-First Practices Have in Common
The practices that avoid OCR penalties and protect their patients share five characteristics:
- They conduct annual risk assessments using the HHS SRA Tool
- They maintain current BAAs with every PHI vendor
- They train staff annually with documented proof
- They monitor access logs and flag anomalies
- They treat their billing company’s security posture as an extension of their own
The Real Cost Comparison
The cost of building this system is measured in hours of administrative time and modest subscription fees.
The cost of not building it is measured in six-figure legal fees, years of Corrective Action Plan oversight, and the irreversible harm to patients whose most sensitive diagnoses become public.
Start This Week
Pull your BAA inventory. Schedule your SRA. And if your billing company can’t answer the ten questions in this guide, it’s time to find one that can.
HIPAA-Compliant Mental Health Billing, Coding & Full RCM
EliteMed Financials provides mental health billing, medical coding, credentialing, and full revenue cycle management for behavioral health practices nationwide — with compliance built into every workflow.