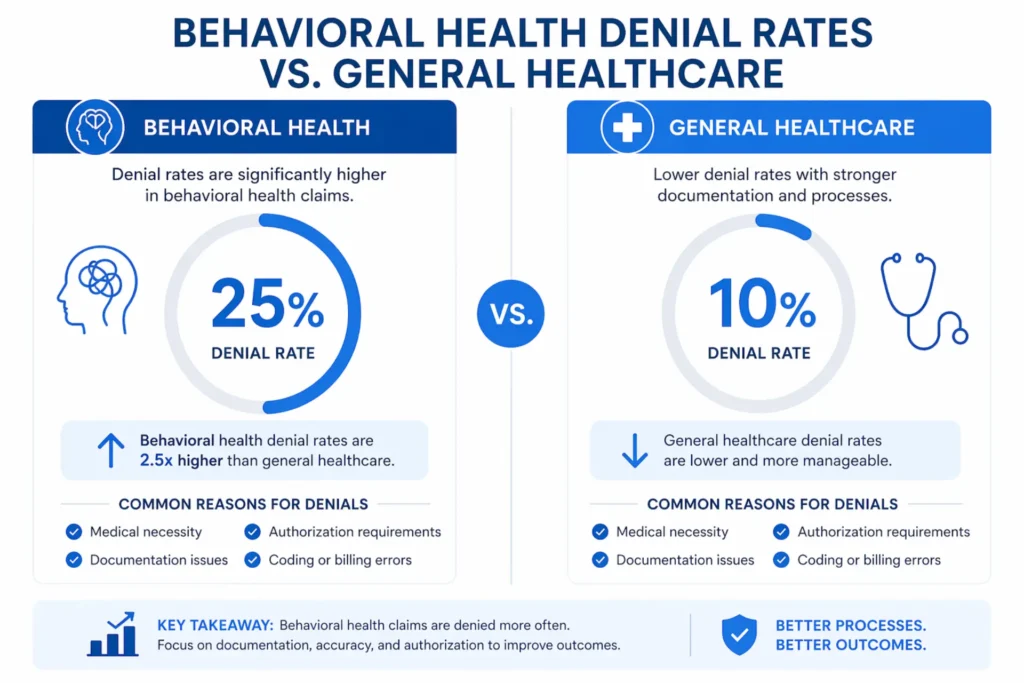
Behavioral health practices are bleeding money most owners never see. The average mental health denial rate sits between 15% and 25% — roughly triple the 8–12% you’ll find in general medicine. Every denied claim costs $25 to $62 to rework. For a practice billing $1 million a year, a 20% denial rate puts $200,000 of revenue at risk before you’ve paid a single clinician.
That’s the problem mental health billing services are supposed to solve. But most don’t. Generalist billing companies treat a denied 90837 the same way they’d treat a denied office visit — as a clerical error to fix and resubmit. In behavioral health, it’s almost never that. It’s a clinical necessity dispute. It’s a carve-out routing mistake. It’s a missing start-and-stop time that triggered an AI down-code. It’s MHPAEA parity violations buried in the fine print of a payer’s utilization management manual.
This guide is for practice owners, group directors, and billing managers who are tired of watching claims die. It covers what proper mental health billing services actually include, why behavioral health billing breaks in ways other specialties don’t, what every major denial code means, how to prevent denials at the intake desk, how to win appeals, what billing services really cost in 2026, and how to pick a partner that actually knows behavioral health instead of one that just says it does.
Table of Contents
What Mental Health Billing Services Actually Cover
Most practice owners hire a billing company thinking they’ve outsourced “billing.” They haven’t. They’ve outsourced one or two pieces of it and kept the rest on their own desk. Proper mental health billing services span the full revenue cycle — from the moment a patient calls to schedule to the day their balance hits zero.
Here’s what a full-service behavioral health billing partner actually handles.
Front-End Revenue Cycle
Insurance eligibility verification. Every patient, every session, every time — not just at intake. Behavioral health coverage shifts constantly. Plans hit session caps. Employers change mental health carve-outs from Optum to Magellan mid-year. A real billing partner runs EDI 270/271 real-time eligibility checks 72 hours before each appointment and flags anything that looks off. Missed eligibility is the single biggest preventable denial in this specialty. You can see how this should work on our insurance eligibility service page.
Prior authorization management. IOP (H0015), PHP, residential treatment (H0045), and psychological testing all require auth before the first session. Many commercial plans now require re-auth every 6 to 12 sessions for routine outpatient therapy. A billing service worth paying for tracks every auth window, alerts you at 75% utilization, and handles re-auth paperwork so your clinicians aren’t chasing it.
Patient scheduling coordination. Not the scheduling itself — that stays with your front desk — but the billing-side guardrails. No encounter should open in the EHR if there’s no active auth in Box 23. No appointment should confirm if eligibility came back inactive. This is what practices call an “auth-lock protocol,” and it stops roughly 90% of CO-197 denials before they happen.
Patient intake and documentation support. A billing partner reviews patient intake forms for subscriber/member mismatches, carve-out logos, coordination of benefits errors, and COB tripwires. They don’t do intake. They make sure intake doesn’t sink you.
Mid-Cycle Clinical and Coding
Medical coding. Behavioral health coding is a minefield. Time-based CPT codes like 90832 (16–37 min), 90834 (38–52 min), and 90837 (53+ min) get down-coded the moment a note is ambiguous on duration. Add-on codes like 90833 and 90836 need Modifier 25 when paired with E/M. Telehealth needs -95. POS 02 vs POS 10 changes based on where the patient physically sat during the session. Proper medical coding services run every note through BH-specific coding rules before a claim ever leaves the practice.
Charge entry and documentation review. This is where the “Golden Thread” either holds or snaps. Every claim should be traceable from the diagnosis (F32.9, F41.1, F43.10) to the treatment plan goal to the session note’s actual intervention. When payers’ NLP audits scan for cloned notes and missing functional impairment language, the Golden Thread is what keeps CO-50 medical necessity denials off your remittance advice. Our charge entry service builds this into every claim.
Claim scrubbing and submission. Before a claim hits the clearinghouse, it should pass through a behavioral-health-specific scrubber that checks time-to-code alignment, modifier logic, POS consistency, NCCI edits, and payer-specific quirks. A clean claim rate below 95% means the scrubber isn’t doing its job. Good claim submission services push first-pass rates to 96–99%.
Back-End Collections
Payment posting. ERAs need to post cleanly, adjustments need to reconcile against contracts, and underpayments need to get flagged — not written off. Without accurate payment posting, you can’t measure net collection rate, and without that, you can’t spot a payer quietly underpaying you by 7%.
Denial management. This is the work most billing services quietly skip. Decoding CARC/RARC codes, building appeal packets with PHQ-9 trends and ASAM documentation, drafting MHPAEA parity language, scheduling peer-to-peers, and escalating to external review — that’s a dedicated function, not a side job. Our denial management services exist because general billers don’t do this well.
AR follow-up. Claims don’t pay themselves. A real billing partner works aging buckets at 30, 45, 60, and 90 days, calls payers with rep IDs and reference numbers logged, and won’t let a claim die quietly. This is what proper AR follow-up looks like.
Patient statements and collections. Clear, compliant, HIPAA-safe patient statements that actually get paid, with proper Good Faith Estimate handling under the No Surprises Act.
Credentialing and payer enrollment. You can have the best billing in the world and still get CO-252 denials if your CAQH profile is out of sync or a provider’s re-cred date expired. Behavioral health credentialing is its own discipline — taxonomy codes, panel closures, Medicaid enrollments, the works.
A mental health billing service that doesn’t touch all of these pieces isn’t a billing service. It’s a claim submitter.
Why Behavioral Health Billing Is So Complex
If you’ve ever asked a generalist biller “why is mental health so hard?” and gotten a shrug, this section is for you. Behavioral health isn’t harder because the codes are weirder. It’s harder because the entire claims adjudication system was built around objective medical specialties — and mental health is the one specialty payers can get away with scrutinizing.
The Subjectivity Problem
A broken ankle has an X-ray. A heart attack has a troponin level. A torn ACL has an MRI. There’s a picture, a number, a measurable thing the payer can point at.
Depression has a patient saying they feel sad. Anxiety has panic attacks the payer didn’t witness. PTSD has trauma the payer will never see. The clinical reality is documented in narrative — a progress note. And narrative is subjective. Subjectivity is the opening payers exploit.
That’s why effective documentation in behavioral health sounds more like physical therapy than psychiatry. Instead of “patient feels better,” you need “PHQ-9 decreased from 18 to 10; patient returned to part-time work after three months of absence.” That’s functional impairment. That’s what survives an audit.
The Parity Shell Game
The Mental Health Parity and Addiction Equity Act (MHPAEA) is supposed to make this stop. It requires group health plans to treat mental health on equal terms with medical and surgical benefits. In practice, payers have gotten creative.
Non-Quantitative Treatment Limitations (NQTLs) are the workaround. Instead of saying “we only cover 20 therapy sessions” (which would be an obvious parity violation), plans write medical necessity criteria that quietly cap care at around the same number. Instead of requiring prior auth on every physical therapy session (they don’t), they require it for every 8th psychotherapy session. The American Psychiatric Association’s 2024 parity report found behavioral health services require prior authorization 5.4 times more often than comparable medical services.
Knowing how to cite MHPAEA in an appeal isn’t a legal hobby. It’s a revenue recovery skill.
Time-Based CPT Code Chaos
Psychotherapy is billed by time. Not “a session” — time.
| CPT Code | Session Length | Billable When |
|---|---|---|
| 90832 | 30 minutes | 16 to 37 minutes of therapy |
| 90834 | 45 minutes | 38 to 52 minutes of therapy |
| 90837 | 60 minutes | 53+ minutes of therapy |
| 90791 | Intake | Diagnostic evaluation |
| 90853 | Group | Group therapy session |
A 49-minute session is a 90834. A 53-minute session is a 90837. A clinician who writes “session lasted about an hour” in their note has given the payer a free down-code from 90837 ($135) to 90834 ($100) — a loss of $35 per claim, multiplied across every client that week.
UnitedHealthcare’s Optum division is especially aggressive here. Their proprietary AI — internally referred to as nHale — flags clinicians whose 90837 frequency sits outside a bell curve and down-codes automatically. The only defense is documented start-and-stop times in every single note.
If you want a deeper walkthrough, our breakdown of mental health CPT codes and the full behavioral health billing codes reference cover every scenario.
The Carve-Out Maze
Here’s a situation that costs small practices thousands every year. A patient hands the front desk a Blue Cross Blue Shield card. Staff runs eligibility, sees “active,” and bills BCBS. Six weeks later a CO-29 timely filing denial comes back. Why? Because their employer carved mental health out to Magellan, and the 90-day filing window at Magellan closed before anyone noticed the card had a small carve-out logo on the back.
Common carve-outs behavioral health practices run into:
- Optum managing mental health benefits for UnitedHealthcare
- Magellan Health managing behavioral health for many BCBS plans and state Medicaid
- Evernorth handling Cigna’s behavioral network
- Beacon Health Options for various commercial and Medicaid plans
Front desk staff should be trained to look for carve-out logos on the back of every insurance card, not just the front.
Telehealth Modifier Minefield
Since the pandemic, telehealth in behavioral health has permanent Medicare coverage but a labyrinth of modifier rules across payers:
- Modifier 95 — synchronous audio-video (most commercial)
- Modifier GT — legacy Medicare modifier, still required by some plans
- Modifier 93 — audio-only (commercial and Medicare for specific BH services)
- Modifier FQ — audio-only for FQHCs
- POS 02 — telehealth not in patient’s home
- POS 10 — telehealth in patient’s home
One missing or incorrect modifier can flip a paid claim into a CO-97 bundled denial. Our guide to telehealth mental health billing walks through every payer’s rules.

Common Billing Mistakes That Quietly Kill Revenue
These are the mistakes I see every week when auditing behavioral health practices. None of them feel catastrophic in the moment. Together, they take 15–20% of your net revenue.
Billing 90837 without documenting start and stop times. Payers now down-code automatically. If the note reads “45-minute session” but you billed 90837, the system corrects it to 90834 and you eat the $35 delta — every session, every week, every year.
Missing Modifier 25 on E/M plus psychotherapy. A psychiatrist billing 99214 plus 90833 (add-on psychotherapy) without -25 on the E/M gets a CO-97 bundled denial. The fix takes 10 seconds. The rework takes 45 days.
Skipping real-time eligibility at the appointment. Eligibility you verified three months ago is not eligibility today. Deductibles reset. Carve-outs change. Patients switch jobs. Check every time, 72 hours out if possible.
Using Z-codes as the primary diagnosis. Z63.0 (relationship distress) and Z71.9 (counseling, unspecified) are almost never covered as primary. Pair them with an F-code — F32.9 for MDD, F41.1 for GAD, F43.10 for PTSD — and the claim pays.
Treating rejections and denials as the same thing. A clearinghouse rejection (missing ID, bad DOB) is a fixable data error — just correct and resubmit. A payer denial (CO-50, CO-197) is a formal appeal situation. Resubmitting a denied claim gets it bounced back as CO-18 Duplicate and wastes an appeal window.
Letting credentialing lapse. Re-credentialing cycles run every 12 to 24 months. One missed CAQH attestation and every claim from that period can come back CO-252. The best credentialing services for mental health track attestation dates automatically.
Not checking HIPAA-compliant handling at every stage. Sending clinical documentation over unencrypted email for an appeal is a breach waiting to happen. Proper HIPAA compliance in mental health billing is non-negotiable.
Tired of Watching Preventable Denials Eat Your Revenue?
EliteMed Financials handles pre-submission claim scrubbing, 72-hour real-time eligibility verification, and payer-specific rule enforcement for behavioral health practices — so denials don’t happen in the first place. Our first-pass clean claim rate for mental health averages 97%+.
Why Mental Health Claims Get Denied More Than Any Other Specialty
Here’s the data side. Behavioral health doesn’t just feel harder than general medicine. The numbers prove it.
Denial Rate by Specialty (2026 Benchmarks)
| Specialty | Average Denial Rate | Primary Drivers |
|---|---|---|
| General Medicine (Primary Care) | 8–12% | Eligibility, minor coding edits |
| Physical Therapy | 12–14% | Visit limits, progress documentation |
| Psychiatry (E/M + Med Management) | 12–18% | Prior auth timing |
| Outpatient Psychotherapy | 16–21% | Medical necessity, session caps |
| Substance Use Disorder | 14–20% | ASAM criteria disputes |
| IOP / PHP Programs | 28–36% | NQTLs, retro denials |
| Residential Treatment | 25–35% | Prior auth complexity |
| Psychological Testing | 40%+ | Prior auth not obtained |
Behavioral health claims face initial denial rates 50% to 85% higher than comparable medical claims. And the reason isn’t clinical. It’s structural.
The AI Audit Layer
Payers have deployed machine learning to claim review over the past two years. Optum’s internal system flags providers whose 90837 frequency sits above the network average. Aetna’s utilization management algorithms scan progress notes for cloned text week over week. Anthem’s documentation review triggers on missing functional impairment language.
The result: a claim that would have paid in 2021 can now trigger a CO-50 medical necessity denial in 2026 based purely on how the note is phrased.
The Overturn Paradox
Here’s the quiet truth about behavioral health denials: when practices actually appeal, they win most of the time. Health Affairs’ 2025 research on mental health claim appeals found overturn rates between 57% and 82% at the external review level. The American Psychiatric Association’s parity tracking shows 81.7% of denials reaching an Independent Review Organization (IRO) get reversed.
So why do practices lose money? Because they don’t appeal. The average behavioral health practice formally appeals only 40–50% of its denials. The other half ages out of the filing window and becomes a permanent write-off.
The Cost of a Single Denial
Before a denied claim ever gets paid, the practice has already spent money on it:
- $62.40 average administrative cost to rework an appealed behavioral health claim (2026)
- $25 to $35 rework cost for simpler denials (coding fixes, resubmissions)
- $115 average reimbursement per outpatient therapy claim
Do the math. A $115 reimbursement with a $62 rework cost means 54% of revenue vanishes the moment a claim bounces — and that’s before you count the cash flow delay.
For context on why these systemic pressures exist, CMS published updates on behavioral health billing policies that practices should stay current with, and the American Psychiatric Association maintains parity enforcement resources worth reviewing.
Denial Rate Benchmarks: What’s Normal vs What’s a Red Flag
A practice owner asked me last month: “Is a 17% denial rate bad?” The honest answer is “it’s average for behavioral health, which means you’re leaving money on the table.” Here’s how to read your numbers.
The “Vital Seven” Behavioral Health Billing KPIs
| KPI | What It Measures | BH Target | Red Flag |
|---|---|---|---|
| First Pass Resolution Rate | Claims paid on first submission | 90–95% | <85% |
| Clean Claim Rate | Claims accepted without edits | >95% | <90% |
| Denial Rate | Denied $ ÷ Total billed $ | <10% | >20% |
| Days in AR | Avg. days to collection | <50 days | >60 days |
| Net Collection Rate | Payments ÷ (Charges − Write-offs) | >96% | <92% |
| Denial Recovery Rate | Recovered ÷ Total denied | >50% | <35% |
| Cost to Collect | Billing cost per $100 collected | <$10 | >$12 |
A denial rate under 10% is best-in-class for behavioral health. Between 10–15% is average. Over 20% is a red flag — it usually means front-end processes are broken, not that your clinicians are coding poorly.
The “Five Red Flags” Checklist
If any three of these describe your practice right now, something’s wrong with your billing operation:
- You can’t pull a real-time denial rate report
- Days in AR are over 60
- You don’t know your top five CARC codes by volume
- You’ve written off more than 3% of billed charges in the last quarter
- Your biller can’t name a single appeal they filed this month
This isn’t about blame. It’s about visibility. Most practices don’t track these because no one taught them to.
The 10 Most Common Mental Health Denial Codes (and How to Fix Each)
Roughly 80% of behavioral health denials come from these 10 CARC codes. Master the fixes for these, and you’ve solved most of your revenue leak.
1. CO-50 — Not Medically Necessary
What triggers it: The payer’s AI (or human reviewer) decided the session wasn’t needed. Usually means missing PHQ-9/GAD-7 scores, no quantified progress, or cloned notes.
Fix: Don’t resubmit — appeal. Build an appeal packet with score trends (PHQ-9 went from 18 to 10), functional impairment language (“patient returned to work after 3-month absence”), and a cite of APA clinical practice guidelines.
2. CO-197 — Prior Authorization Missing or Expired
What triggers it: Claim submitted without auth, or auth expired before the session date.
Fix: Check payer portal for existing auth. If none, request retroactive auth (most commercial plans allow 60–90 days). If denied, escalate to peer-to-peer review.
3. CO-16 — Claim Lacks Information
What triggers it: Wrong CPT-to-time match (90837 for a 48-minute session), missing modifier, incorrect subscriber info.
Fix: Run a data correction review. Send corrected claim (CLM05-3 code 7), not a resubmission.
4. CO-27 — Expired Coverage
What triggers it: Patient’s coverage ended before the date of service, or benefit limit hit.
Fix: Re-verify eligibility. If patient had retroactive Medicaid coverage, appeal with proof. If benefit truly exhausted, transition to self-pay with a Good Faith Estimate.
5. CO-29 — Timely Filing Expired
What triggers it: Claim submitted past the payer’s window. Common when claims were sent to the wrong payer (carve-out issue).
Fix: Pull the clearinghouse 277 Acceptance Report as proof of original submission. Appeal citing equitable tolling if the payer’s own actions caused the delay.
6. CO-18 — Duplicate Claim
What triggers it: Same claim submitted twice. Usually happens when staff resubmits a denied or pending claim instead of checking status.
Fix: Use a 276/277 claim status inquiry to check status before any resubmission. If denial, formal appeal — not resubmit.
7. CO-97 — Service Bundled or Included in Another Payment
What triggers it: Missing Modifier 25 on an E/M billed same day as psychotherapy. Or missing Modifier 59/XE for distinct service.
Fix: Append the correct modifier. Resubmit as corrected claim.
8. CO-252 — NPI Invalid or Not Credentialed
What triggers it: Provider not yet credentialed with payer, CAQH profile lapsed, taxonomy code mismatch, billing under wrong NPI.
Fix: Verify CAQH profile is current. Confirm provider’s effective date with payer. If credentialing lapsed, expedite re-credentialing before resubmitting.
9. CO-167 — Diagnosis Not Covered
What triggers it: Claim billed with a Z-code (Z63.0, Z71.9) as primary, or a non-covered DSM-5 diagnosis.
Fix: Re-review diagnosis pairing. Pair Z-codes with primary F-codes. Adjust per payer’s covered diagnosis list.
10. CO-4 — Modifier Missing or Inconsistent
What triggers it: Procedure requires a modifier the claim didn’t have. Common with telehealth (missing -95).
Fix: Append correct modifier (-95 for commercial telehealth, -93 for audio-only, etc.). Corrected claim resubmission.
How to Prevent Denials Before a Claim Is Even Submitted
Prevention is roughly 5 times cheaper than appeals. Every dollar you spend on front-end verification saves five dollars on back-end rework. Here’s the prevention stack that actually works.
The 72-Hour Gatekeeper Protocol

Run real-time eligibility verification 72 hours before every appointment. Check:
- Active coverage
- Behavioral health carve-out status
- Remaining session limits
- Deductible met / unmet
- Prior auth requirements
- Copay amount
That 72-hour window gives your team time to call the patient, fix issues, or reschedule if coverage lapsed. Availity, Change Healthcare’s VerifyNow, TherapyNotes’ integrated RTE, and SimplePractice all support EDI 270/271 transactions natively.
Auth-Lock Scheduling
Configure your EHR so no encounter can open without a valid auth number in Box 23 (when auth is required). This single rule eliminates about 90% of CO-197 denials. For IOP and PHP programs, set a 75% utilization trigger — when 75% of authorized sessions are used, the system flags the patient for re-auth.
The Golden Thread Documentation Standard
Every session note should connect, in writing, to:
- The intake assessment and DSM-5 diagnosis
- The specific treatment plan goal
- The intervention delivered this session
- A measurable outcome (symptom reduction, functional improvement)
This is the standard payers’ AI audits scan for. A note that reads “patient feels better” flunks. A note that reads “PHQ-9 today: 12, down from 18 at intake; patient sleeping 6 hours consistently, up from 2–3” passes.
Pre-Submission Claim Scrubbing
Every claim should pass through a behavioral-health-specific scrubber before it leaves the clearinghouse. The scrubber should check:
- CPT-to-time alignment (90837 requires 53+ min documented)
- Modifier logic (-95 for telehealth, -25 for E/M + therapy)
- POS consistency (02 vs 10 vs 11)
- ICD-10 validity and CPT-ICD pair rules
- NCCI edits
- Payer-specific rules (Optum, Aetna, BCBS all differ)
A properly configured scrubber pushes first-pass clean claim rates from 82% (industry average for DIY) to 96%+ (specialist billing).
Front-Desk Training on Carve-Outs
Teach your front desk team to physically flip every insurance card over and look for behavioral health carve-out logos. Optum, Magellan, Evernorth, Beacon — those logos mean you bill the carve-out, not the medical plan. Missing this is the #1 cause of CO-29 timely filing denials in behavioral health.
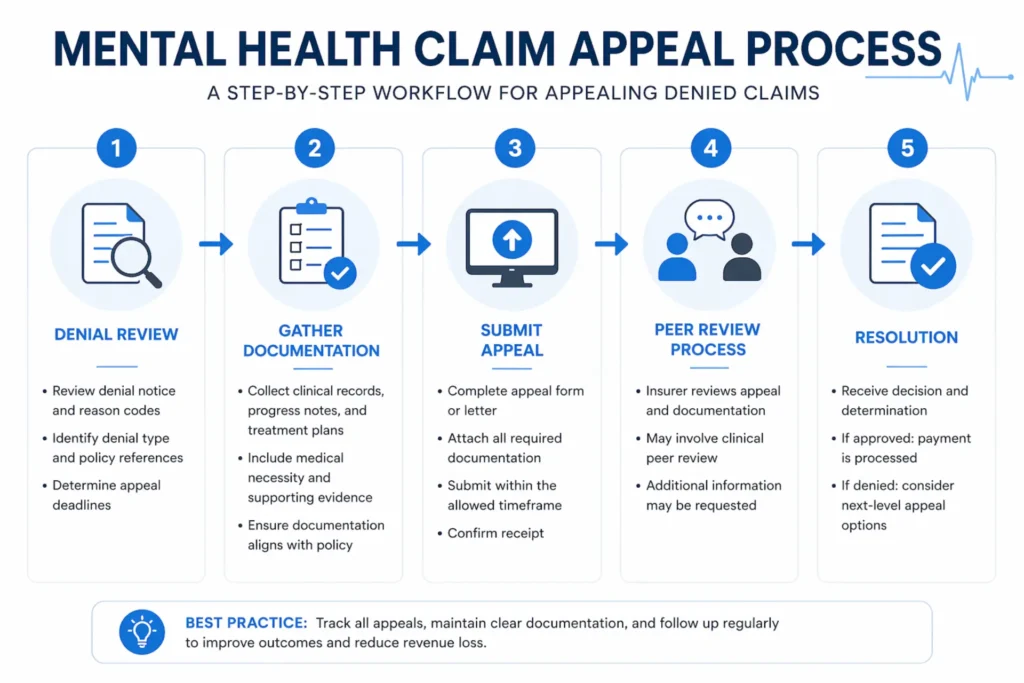
Step-by-Step Guide to Appealing a Denied Mental Health Claim
When prevention fails, appeals recover the revenue. The process isn’t complicated — but it’s disciplined, and most practices skip steps. Here’s the sequence.
Step 1: Decode the Denial
Pull the EOB or ERA and identify:
- CARC code (e.g., CO-50) — the reason
- RARC code (e.g., N115) — the remark, often the specific gap
- Group code — CO (contractual, appealable), PR (patient responsibility), OA (other), PI (payer info)
If it’s a PR group code, the patient owes. If it’s CO, you appeal.
Step 2: Confirm Denial vs Rejection
A rejection happened before adjudication — fix and resubmit as a corrected claim. A denial happened after adjudication — formal appeal. Confusing these is the #1 mistake.
Step 3: Assemble the Clinical Evidence Packet
Include:
- Original claim and EOB
- Intake assessment with DSM-5 diagnosis
- Treatment plan with measurable goals
- All progress notes from dates in dispute
- Quantified assessment scores (PHQ-9, GAD-7, BDI, CAPS, HAM-D, GAF)
- Functional impairment documentation
Bundle as a single indexed PDF under 10 pages. Label attachments as Exhibit A, B, C.
Step 4: Draft the Appeal Letter
A winning appeal letter has five elements:
- Claim identifiers — claim #, date of service, patient ID
- Factual clinical summary — quantified, not narrative (“PHQ-9 decreased from 18 to 10”)
- Regulatory citation — MHPAEA 42 USC §300gg-5, APA guidelines, ASAM criteria
- Attachments index
- Specific requested action — “Reverse denial and reprocess for $XXX”
Use bold headers, bullet points, and a data correction table when relevant. Reviewers scan for three minutes before deciding. Walls of text get denied.
Step 5: Submit via the Right Channel
Most payers now require portal submission (Availity, OptumProviderExpress, Aetna provider portal). When portals aren’t an option, send via certified mail with return receipt or fax with confirmation sheet. Log the submission date, acknowledgement number, and representative ID on every contact.
Step 6: Follow Up on a Schedule
- Day 7 — confirm receipt
- Day 14 — status inquiry
- Day 30 — request supervisor review if no movement
- Day 45 — escalate to peer-to-peer or external review
Escalation: Peer-to-Peer Review
If the first appeal loses, request a peer-to-peer review. Under MHPAEA, you have the right to a like-specialty peer — a psychiatrist for psych claims, not a general medical reviewer. Behavioral health peer-to-peers hit 40–60% success rates. Prepare a 3–5 bullet clinical summary before the call.
Escalation: External Review (IRO)
After exhausting internal appeals, escalate to an Independent Review Organization. External review for behavioral health overturns 62% of denials on average, and the decision is binding on the payer. The window to file is typically 180 days from the final internal denial.
Don’t Write Appeal Letters. Get Paid Instead.
Our behavioral health denial management team handles every step — CARC code analysis, clinical packet assembly, MHPAEA-cited appeal drafting, peer-to-peer scheduling, and external review escalation. Overturn rates run 55–70% on appealed claims. You focus on patients. We recover the revenue.
Denial Management Services →Appeal Timeline by Payer (2026)
Missing an appeal deadline is irretrievable. The claim is permanently lost. Here’s the window for each major payer.
| Payer | Initial Appeal Filing Window | Processing Time | Expedited Option |
|---|---|---|---|
| Medicare (Level 1 Redetermination) | 120 days from RA date | 60 days | Yes — urgent |
| Medicare (Level 2 QIC) | 180 days from L1 decision | 60 days | Yes |
| UnitedHealthcare / Optum | 65 days from EOB | 30 days | 72 hours |
| Aetna | 180 days from EOB | 30 days | 72 hours |
| Cigna / Evernorth | 180 days from EOB | 30 days | 72 hours |
| Anthem / BCBS | 180 days from EOB | 30–60 days | 72 hours |
| Humana (Commercial) | 180 days from EOB | 30 days | 72 hours |
| Humana (Medicare Advantage) | 65 days from EOB | 30 days | 72 hours |
| ERISA Plans | 60 days from denial | 60 days | Yes |
| Medicaid (varies by state) | 30–90 days | 90–120 days | State-specific |
Expedited appeals apply when a delay would jeopardize a patient’s life, health, or functional capacity — suicide risk, active detox, inpatient holds. These require a physician signature and must be resolved in 72 hours. Expedited success rates run 40–60%, far above the standard 25%.
In-House vs Outsourced Mental Health Billing: The Real Comparison
This is the question every practice owner eventually asks. The honest answer isn’t “outsource always” or “in-house always.” It’s a math problem tied to your revenue, payer mix, and operational maturity.
The Cost Reality
In-house biller, fully loaded:
- Base salary: $55,000 – $75,000
- Benefits + taxes (30% loading): $16,500 – $22,500
- Software, clearinghouse, EHR modules: $10,000 – $25,000
- Training, CEUs, conferences: $5,000
- Manager time allocation (20%): ~$15,000
- Turnover cost (25% annual attrition): $25,000 amortized
Fully loaded cost per in-house biller: $75,000 to $110,000 annually.
Outsourced billing:
- Percentage of collections: 4% – 8% (behavioral health average ~6%)
- On $1M collections: $40,000 – $80,000
- On $2M collections: $80,000 – $160,000
The Performance Reality
| Metric | In-House Average | Specialized BH Billing Company |
|---|---|---|
| Denial Rate | 12–18% | 2–5% |
| Clean Claim Rate | 82–88% | 96–99% |
| Days in AR | 50–65 days | 28–35 days |
| Appeal Success | 20–35% | 45–70% |
| Cost to Collect | ~14.7% | ~5.4% |
For a $3 million practice, the cost-to-collect gap alone represents about $279,000 a year. That’s not a billing decision. That’s the difference between scaling and stalling.
The Break-Even Threshold
- Under $500K annual revenue: In-house often wins on raw cost, if you have a seasoned biller
- $500K – $1M: Outsourcing usually wins once you factor denial recovery
- $1M – $5M: Outsourcing almost always wins
- $5M+: Depends on whether you can build an in-house specialty team at scale
The break-even for most behavioral health practices is around $600,000 in annual revenue. Above that, specialized outsourcing typically delivers 15–25% higher net collections after fees.
When to Stay In-House
- Under 5 clinicians, Medicare-primary payer mix
- A tenured, CPC-certified biller with low turnover
- $10M+ revenue with a dedicated 3+ person billing team
- Highly specialized workflow (e.g., neuro-feedback, forensic psych)
When to Outsource
- Denial rate above 10%
- Days in AR above 45
- Adding 2+ providers per quarter (credentialing volatility)
- Biller turnover in the last year
- Net collection rate below 95%
- No real-time denial reporting
Our full breakdown of outsourcing mental health billing covers the decision framework in more depth.
The Hybrid Model
Some practices run a middle path: keep eligibility and charge entry in-house (front desk already does it), outsource denial management and AR follow-up. This works for 10+ clinician groups with stable staff. It fails when accountability blurs and denials fall into the gap between the two teams.
How Much Do Mental Health Billing Services Cost in 2026?
Pricing in this industry has three common structures. Understanding them prevents overpayment.
Percentage of Collections (Most Common)
- Range: 4% – 8%
- Behavioral health average: 6%
- Best for: Most practices; aligns biller incentives with your revenue
At 6% on $1M collected, you’re paying $60,000 a year. That covers end-to-end RCM, denial management, AR follow-up, reporting, and usually credentialing support.
Per-Claim Pricing
- Range: $4 – $10 per claim
- Best for: High-volume practices with predictable claim count
At $6 per claim with 500 claims/month, you’re paying $36,000/year. This can undercut percentage models for simpler payer mixes, but it removes the biller’s incentive to chase difficult claims.
Flat Monthly Fee
- Range: $1,500 – $5,000/month
- Best for: Small solo practitioners with predictable volume
Rarely the best financial fit for multi-provider groups.
What Should Be Included
A fair 6% contract should cover:
- Eligibility verification (unlimited)
- Charge entry and coding review
- Claim submission and scrubbing
- Payment posting
- Denial management (including appeals)
- AR follow-up (all aging buckets)
- Patient statements
- Monthly KPI reporting
- Credentialing updates (often included)
Watch out for contracts that charge extra for appeals, carve out denial management, or bill separately for credentialing. Those are structured to look cheap up front and cost more in practice. Our deep-dive on mental health billing service costs breaks down every pricing model.
How to Choose the Right Mental Health Billing Partner
Most billing sales pitches sound identical. Here’s how to separate real behavioral health specialists from generalists with a mental health landing page.
The Seven Questions That Expose Generalists
Ask these in the first sales call. Watch the answers.
1. What’s your average denial rate on behavioral health claims? A real specialist will say 3–5% and back it up. A generalist will say “we don’t track by specialty.”
2. How do you handle 90837 down-codes? A specialist talks about start-and-stop time documentation, NLP note review, and payer-specific billing intensity flags. A generalist doesn’t know what you’re asking.
3. Do you cite MHPAEA in appeals? A specialist says yes and can name the statute (42 USC §300gg-5) and explain NQTL comparative analysis. A generalist stalls.
4. How do you identify behavioral health carve-outs at intake? Specialists describe back-of-card logo checks, eligibility verification for carve-out routing, and clearinghouse carve-out detection. Generalists say “our system checks coverage.”
5. What’s your first-pass clean claim rate specifically for behavioral health? Answer should be 95%+. If they quote a blended overall rate, they don’t track BH separately.
6. Can I see a sample monthly KPI report? If they can’t show you a denial-by-CARC breakdown, a payer-by-payer denial trend, and days-in-AR by bucket, they’re not measuring what matters.
7. Do you handle peer-to-peer review scheduling? A real specialist coordinates peer-to-peers with the clinician and follows up. A generalist hands you a denial letter and says “call the payer.”
Credentialing and Onboarding Should Be Seamless
Good billing partners take 30 to 60 days to onboard you — payer enrollment, EHR integration, workflow training, historical claim cleanup. A partner who says “we can start billing Monday” hasn’t set up any of this and will cost you in month two. Our guide on how to choose a mental health billing service walks through the vendor evaluation process step by step.
What Real Specialization Looks Like
- Clinical staff include licensed behavioral health professionals, not just generalist coders
- ASAM criteria training for SUD billing
- DSM-5 literacy (not just ICD-10)
- Parity law and MHPAEA education for appeals teams
- Payer-specific playbooks for Optum, Magellan, Aetna, Cigna, BCBS
- Real-time dashboards, not monthly PDFs
If you’re running a small group practice specifically, our dedicated resource on mental health billing for small group practices covers what to look for at your scale.
The Non-Negotiables
- HIPAA compliance baked into every workflow, every vendor integration
- Monthly reporting with real metrics, not fluff
- Transparent pricing with no hidden charge categories
- Contract exit terms that don’t trap you for years
- Dedicated account management — you should have a person, not a ticket queue
Mental Health Billing That Actually Captures Your Revenue
EliteMed Financials runs end-to-end behavioral health billing with built-in denial prevention, a dedicated appeals team, real-time KPI dashboards, and monthly reporting you can actually read. No guesswork. No generic billing playbooks. Just specialists who understand why 90837 denials happen and how to stop them.
Common Q&A
Q: What do mental health billing services actually include? A full service covers eligibility verification, prior authorization tracking, medical coding, claim scrubbing, claim submission, payment posting, denial management, appeals, AR follow-up, patient statements, and credentialing support. Anything less is a claim submitter, not a billing partner.
Q: Why do mental health claims get denied so much? Behavioral health claims face denial rates around 15–25%, compared to 8–12% in general medicine. The reasons are subjective medical necessity, prior authorization requirements 5.4 times higher than medical services, time-based CPT coding errors, carve-out routing mistakes, and telehealth modifier confusion.
Q: How much should I pay for mental health billing services? Most behavioral health practices pay 4–8% of collections, averaging around 6%. On $1 million in collections, that’s $60,000 per year for end-to-end revenue cycle management, denial handling, and reporting.
Q: Is it worth outsourcing mental health billing? For practices over $600,000 in annual revenue, outsourcing to a behavioral health specialist almost always delivers better net collections than in-house billing. Specialists hit 2–5% denial rates versus 12–18% in-house, with 55–70% appeal success versus 20–35%.
Q: What’s a good denial rate for a mental health practice? Under 10% is best-in-class. Between 10–15% is average. Above 20% is a red flag signaling systemic problems with front-end verification, coding accuracy, or prior authorization tracking.
Q: How do I appeal a denied mental health claim? Decode the CARC code on the EOB, confirm it’s a denial (not a rejection), assemble a clinical evidence packet with PHQ-9/GAD-7 scores and treatment plan documentation, draft an appeal letter citing MHPAEA if applicable, submit through the payer’s portal with confirmation, and follow up on a scheduled cadence. If the first appeal loses, escalate to peer-to-peer review and then to external review with an Independent Review Organization.
Frequently Asked Questions
What’s the difference between mental health billing and general medical billing?
Mental health billing uses time-based CPT codes (90832/90834/90837) that require exact session duration documentation, handles subjective medical necessity that payers scrutinize more aggressively, navigates behavioral health carve-outs that general billing doesn’t encounter, and applies MHPAEA parity law in appeals. General medical billing rarely deals with any of these.
How long does it take to see results after switching billing services?
Most practices see first-pass clean claim rate improvements within the first billing cycle (2–4 weeks). Denial rate reductions typically show up by month 2–3. Full revenue cycle optimization — including Days in AR reduction from 60+ days down to under 40 — usually takes 90 days.
Do billing services handle credentialing?
Good behavioral health billing partners include credentialing support in their service. This covers CAQH profile maintenance, payer enrollment, re-credentialing tracking, and taxonomy code updates. Credentialing gaps cause CO-252 denials, so it should never be handled separately from billing.
Can billing services help with telehealth claim issues?
Yes. A specialist handles the complete telehealth modifier matrix — Modifier 95 for synchronous commercial, GT for legacy Medicare, 93 for audio-only, FQ for FQHCs — plus POS 02 versus POS 10 based on patient location. Telehealth denials are usually payer-specific, so the billing partner’s payer rule library matters.
What happens to claims in progress when I switch billing services?
A proper transition plan includes historical claim cleanup — working the existing AR aging buckets, filing remaining appeals, and closing out open denials — before switching to the new workflow. Expect a 30–60 day transition window where both teams coordinate.
How do I know if my current billing is costing me money?
The five-red-flag checklist: you can’t pull a real-time denial rate, Days in AR exceed 60, you don’t know your top five CARC codes by volume, you’ve written off more than 3% in the last quarter, and your biller can’t name an appeal they filed this month. Any three of these mean you’re losing revenue you could recover.
Is behavioral health billing subject to different HIPAA rules?
Substance use disorder (SUD) records carry extra protection under 42 CFR Part 2, with stricter consent requirements than standard HIPAA. Any billing partner handling SUD claims must understand Part 2 compliance, not just baseline HIPAA.
What reports should I expect every month from a billing service?
At minimum: first-pass clean claim rate, denial rate trended over 90 days, denial volume by CARC code, Days in AR by aging bucket, net collection rate, appeal volume and success rate, and a payer performance breakdown. If your current reports are missing any of these, you’re flying blind.
The Bottom Line
Behavioral health billing is its own specialty. The codes are different. The denial patterns are different. The regulatory framework — MHPAEA, parity enforcement, 42 CFR Part 2 — is different. The payer behavior is different, with AI-driven audits that target mental health more aggressively than any other category of care.
A practice that treats billing like an administrative afterthought will lose 15–25% of its revenue to preventable denials. A practice that invests in proper behavioral health billing services — whether in-house with a certified, trained team or outsourced to a specialist — captures that revenue and grows faster than the competition.
The decision isn’t “should I pay for billing services?” You’re already paying, whether through denied claims, unappealed write-offs, inflated cost-to-collect, or lost clinician time. The real decision is whether you want that cost working for you or against you.
If denial rates over 10%, Days in AR past 50, or write-offs above 3% sound familiar, the problem isn’t your clinicians or your patients. It’s the operation around them. Fix that, and the revenue follows.
Full-Service Behavioral Health Billing, Coding, Credentialing & Denial Management
EliteMed Financials works with mental health practices nationwide — solo clinicians, group practices, IOP/PHP programs, and residential programs. HIPAA-compliant workflows, certified coders, dedicated denial management, and transparent reporting. Compliance baked into every workflow.