Psychiatric billing is not therapy billing. It operates in a different lane — one that combines prescribing authority, E/M coding, medication management, psychotherapy add-ons, procedural billing for ECT and TMS, and inpatient facility claims under a single provider type. That makes it one of the most complex billing specialties in healthcare.
Psychiatric billing services cover the full revenue cycle for psychiatrists, psychiatric nurse practitioners (PMHNPs), and physician assistants working in mental health. This includes diagnostic evaluations using CPT 90792, E/M visits coded under 99213–99215, pharmacological management via 90863, psychotherapy add-on codes like +90833 and +90836, and procedures such as electroconvulsive therapy (90870) and transcranial magnetic stimulation (90867–90869) — all routed through payer systems that frequently carve out behavioral health to separate administrators like Optum, Carelon, or Magellan.
Psychiatric billing is a specialized form of medical billing for diagnosing and managing mental health disorders. Unlike therapy-only billing, it includes E/M codes, medication management, 90792 evaluations, and procedures like ECT or TMS, while also supporting psychotherapy add-on codes and payer-specific medical or behavioral health routing.
Revenue cycle data shows behavioral health denial rates can reach 15–25%, with psychiatric E/M and medication-management denials commonly reported around 12–18%. For a practice collecting $1 million annually, a 20% denial rate puts roughly $200,000 at risk every year.
This guide covers all of it — codes, PMHNP billing rules, claim submission workflows, software options, inpatient billing, and the real math behind outsourcing decisions.

Table of Contents
What Is Psychiatric Billing? How It Differs from General Mental Health Billing
Psychiatric billing is a hybrid discipline. It combines medical billing, behavioral health coding, and mental health revenue cycle management into a single workflow that most therapy-only billing systems can’t handle.
Core Definition
At its foundation, psychiatric billing covers claim submission and reimbursement for services provided by prescribing mental health providers — psychiatrists (MD/DO), psychiatric nurse practitioners (PMHNP-BC), and physician assistants with psychiatric specialization. These providers can bill E/M codes, medication management, diagnostic evaluations with medical services, and somatic procedures. That’s a fundamentally different coding universe than what an LCSW or LPC operates in.
How It Differs from Therapy-Only Billing
The distinction isn’t just terminology. It’s operational.
Therapy-only billing relies primarily on psychotherapy CPT codes — 90832, 90834, 90837 for individual sessions, plus 90846/90847 for family therapy and 90853 for group. The diagnostic evaluation code is 90791 (without medical services). The claim goes to the behavioral health benefit, and that’s it.
Psychiatric billing adds an entire second layer. A psychiatrist evaluating a new patient uses CPT 90792 — psychiatric diagnostic evaluation with medical services — because they’re assessing medication options, reviewing lab values, and making prescribing decisions. Follow-up visits are billed under E/M codes (99213, 99214, 99215) based on medical decision making. When therapy is provided in the same visit, add-on codes (+90833, +90836, +90838) are layered on top with modifier -25 on the E/M code.
That dual-coding triage — deciding whether a visit is E/M only, therapy only, or a combination — is where most billing errors happen. And it’s where most denial management work starts.
Services Covered Under Psychiatric Billing
The scope goes well beyond talk therapy:
- Psychiatric diagnostic evaluations (90791, 90792)
- E/M visits for medication management (99213–99215)
- Pharmacological management (90863)
- Psychotherapy — standalone and add-on codes
- Electroconvulsive therapy (ECT — 90870)
- Transcranial magnetic stimulation (TMS — 90867, 90868, 90869)
- Inpatient psychiatric professional services
- Group therapy (90853) and family therapy (90846, 90847)
- Behavioral Health Integration (G0323) and Collaborative Care (99492)
- Psychological testing coordination
The Psychiatric Revenue Cycle
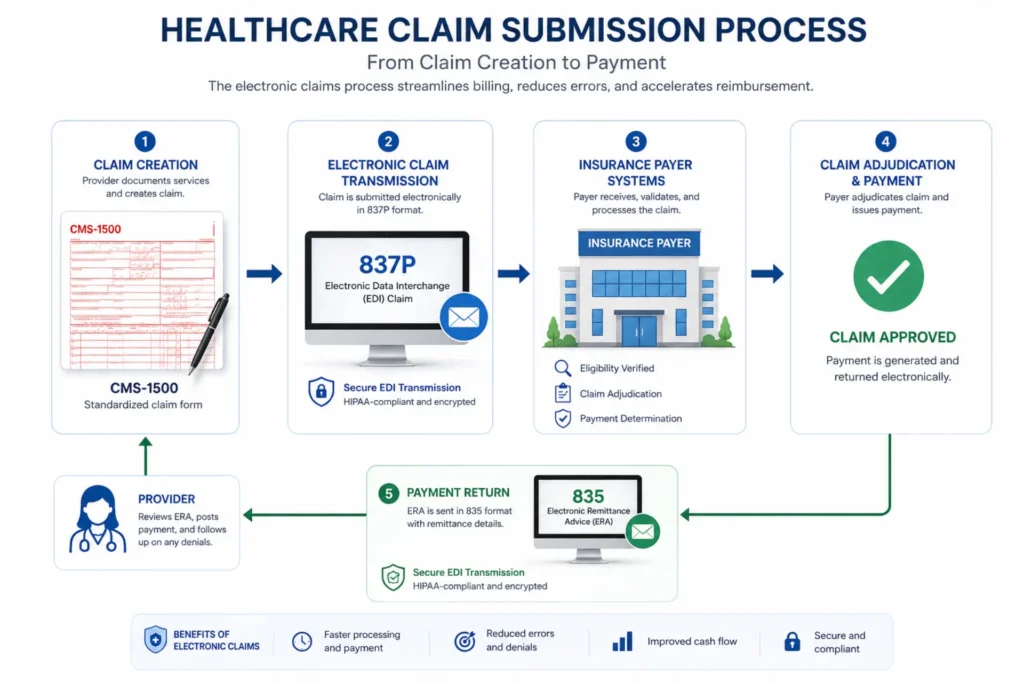
The psychiatric revenue cycle follows the same general stages as medical billing — eligibility verification using EDI 270/271 transactions, prior authorization, clinical documentation, coding and charge entry, claim submission via ANSI 837P, payment posting from ERA 835 remittances, and AR follow-up.
But the failure points are different. Before the first claim goes out, you need to know whether behavioral health benefits are carved out to a third-party MBHO. If Optum manages the psychiatric benefit but you submit to BCBS, that claim comes back as CO-109 — wrong payer. That’s not a coding error. It’s a workflow error that happens before coding even starts.
For a foundational overview of what mental health billing covers and the broader behavioral health billing framework, we’ve published separate guides.
| Feature | Psychiatric Billing | Therapy-Only Billing |
|---|---|---|
| Core Service | Medical management + therapy | Talk therapy and counseling |
| Primary Clinicians | Psychiatrists, PMHNPs, PAs | LCSWs, LPCs, LMFTs, psychologists |
| Key CPT Codes | 90792, 99202–99215, 90863, ECT/TMS | 90791, 90832–90838, 90846–90853 |
| Medication Management | Included through E/M or 90863 | Not allowed |
| Diagnostic Evaluation | 90792 with medical services | 90791 without medical services |
| Combination Billing | E/M + psychotherapy add-on + modifier -25 | Psychotherapy + crisis or interactive complexity |
| Procedures | ECT (90870), TMS (90867–90869) | Generally not applicable |
| Claim Routing | May split between medical and BH carve-out | Usually behavioral health benefit only |
| Top Denial Driver | Medical necessity of E/M level + medication management NCCI conflicts | Session limits, ongoing therapy necessity |
Psychiatric Billing Codes — Complete 2026 Reference
This is where claims live or die. Every code has a time rule, a documentation requirement, and at least one denial trigger that catches practices off guard.
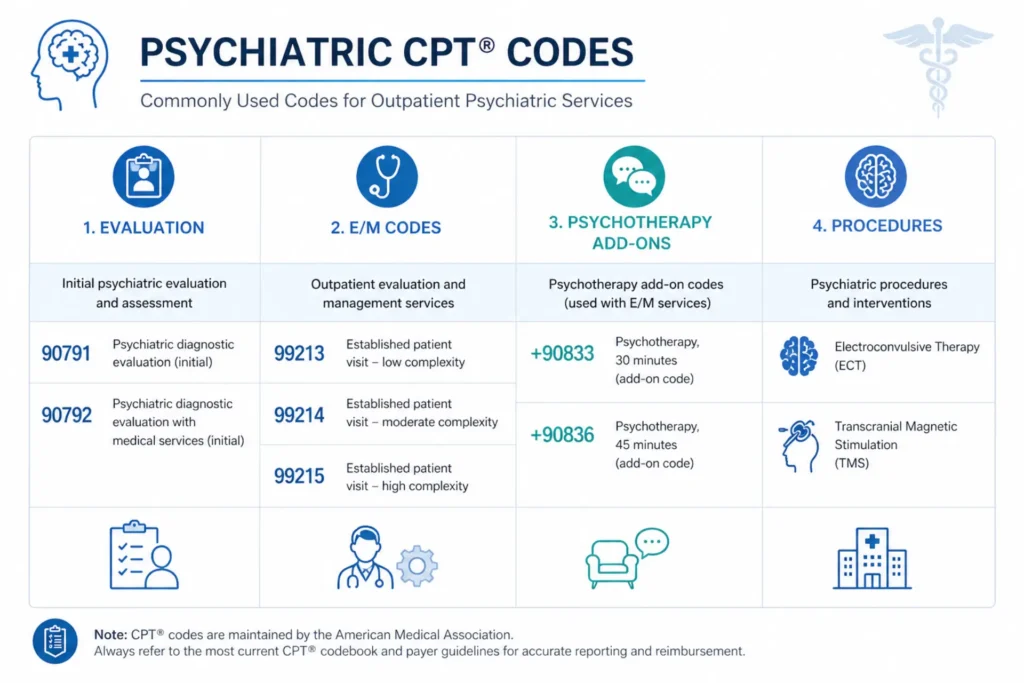
Psychiatric Evaluation Codes: 90791 vs 90792
CPT 90791 is a psychiatric diagnostic evaluation without medical services. Any qualified mental health provider can bill it — psychiatrists, psychologists, LCSWs, PMHNPs.
CPT 90792 is a psychiatric diagnostic evaluation with medical services. Only prescribers can bill this code. It requires a medical component — medication assessment, lab review, physical health considerations alongside the psychiatric evaluation. A PMHNP in a full practice authority state can bill 90792. An LCSW cannot.
Both codes are limited to one per client, per provider or group (same billing NPI), per calendar year under most payer policies. CMS Article A57480 considers an extended break approximately 6 months from the last visit. You cannot bill 90791 or 90792 on the same day as psychotherapy codes without specific payer approval.
E/M Codes for Psychiatry (99202–99215)
Follow-up psychiatric visits — medication checks, treatment adjustments, symptom monitoring — are billed using standard E/M codes. Code selection is based on medical decision making (MDM), not time, when psychotherapy add-ons are also billed.
- 99213 — low MDM (stable medication, routine follow-up)
- 99214 — moderate MDM (medication change, new symptom evaluation)
- 99215 — high MDM (complex polypharmacy, safety concerns, SI/HI risk)
Medication Management (90863)
CPT 90863 — pharmacological management — is a code specifically for medication oversight. Here’s the critical NCCI restriction most practices miss:
In accordance with the National Correct Coding Initiative (NCCI), medication management (90863) and an E/M or psychotherapy service cannot be billed on the same day of service by the same provider.
This means if the visit focus extends beyond brief medication management into broader clinical discussion, the service is considered psychotherapy or E/M — not medication management. The WA State billing guide states explicitly: “If the client continues to experience signs and symptoms that require discussion beyond minimal psychotherapy, the focus of the service is broader and is considered psychotherapy rather than medication management.”
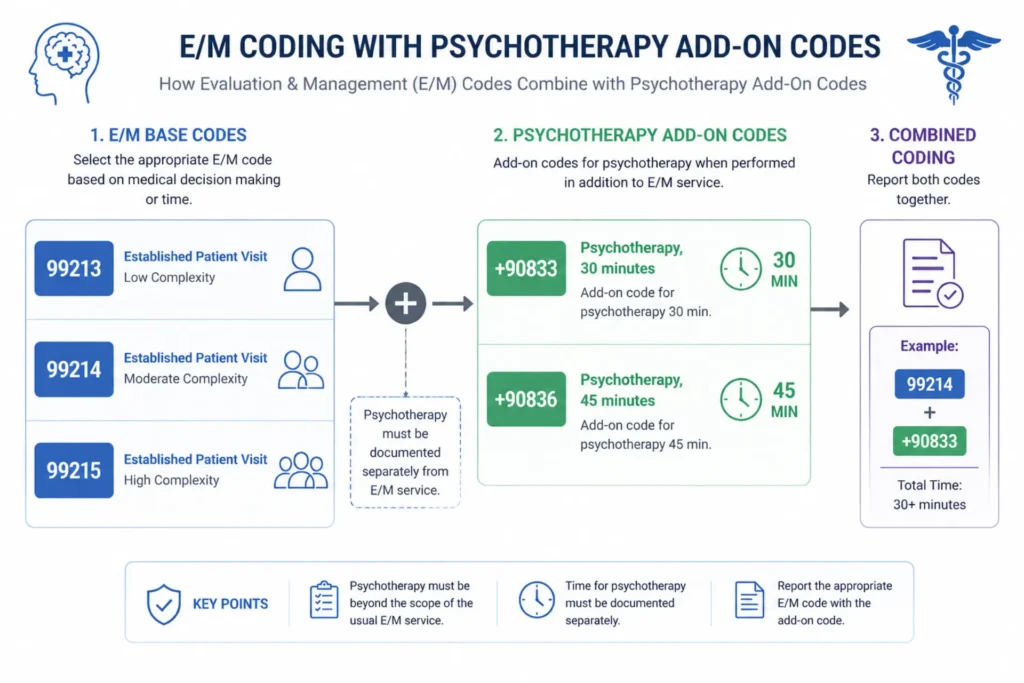
Psychotherapy Add-On Codes (+90833, +90836, +90838)
When a psychiatrist provides both E/M services and psychotherapy in the same visit:
- +90833 — psychotherapy add-on, 16–37 minutes
- +90836 — psychotherapy add-on, 38–52 minutes
- +90838 — psychotherapy add-on, 53+ minutes
These codes are never billed standalone. They require an E/M base code with modifier -25 on the E/M to indicate a significant, separately identifiable service. The E/M portion is selected by MDM. Time spent on E/M activities is not included in psychotherapy time — there must be no overlap.
Electroconvulsive Therapy (90870)
CPT 90870 covers ECT — limited to one treatment per client per day, billed by psychiatrists only. ECT requires prior authorization from most payers. In facility settings, the hospital bills the facility component on UB-04 while the psychiatrist bills the professional component on CMS-1500.
Transcranial Magnetic Stimulation (90867–90869)
- 90867 — TMS treatment plan development (1 per client per year)
- 90868 — TMS delivery session (up to 60 sessions)
- 90869 — TMS treatment redetermination (1 per client per year)
TMS is outpatient only. Prior authorization is required by virtually every payer. For medical coding accuracy, each session must document the treatment parameters and clinical response.
Documentation Requirements
According to the WA State Mental Health Services Billing Guide, medication management documentation requires 12 specific elements:
- Date and time of service
- Diagnosis (updated annually)
- Interim medication history
- Current symptoms and problems, including physical symptoms
- Problems, reactions, and side effects to medications or ECT
- Current mental status exam
- Any medication modifications
- Reasons for medication adjustments, changes, or continuation
- Desired therapeutic drug levels (if applicable)
- Current laboratory values (if applicable)
- Anticipated physical and behavioral outcomes
- Provider signature
Missing any of these elements in a medication management visit creates a CO-50 (medical necessity) denial risk during audit.
| Code | Category | Description | Time Rule | Key Billing Rule |
|---|---|---|---|---|
| 90791 | Evaluation | Diagnostic eval (no medical) | Untimed | No same-day psychotherapy; 1/client/year |
| 90792 | Evaluation | Diagnostic eval + medical | Untimed | Prescriber only; 1/client/year |
| 99213–99215 | E/M | Medication management visits | MDM-based | Use MDM when paired with psychotherapy |
| 90832 | Psychotherapy | 30-min therapy | 16–37 min | Time must be documented |
| 90834 | Psychotherapy | 45-min therapy | 38–52 min | Cannot overlap with E/M time |
| 90837 | Psychotherapy | 60-min therapy | 53+ min | Requires start/stop times |
| +90833 | Add-on | Therapy with E/M | ≥16 min | Requires E/M + modifier -25 |
| +90836 | Add-on | Therapy with E/M | ≥38 min | Requires E/M + modifier -25 |
| +90838 | Add-on | Therapy with E/M | ≥53 min | Requires E/M + modifier -25 |
| 90863 | Medication | Pharmacologic mgmt | ≥16 min | NOT with E/M same day (NCCI) |
| 90839 | Crisis | Crisis therapy initial | 30–74 min | Cannot combine with other psychotherapy |
| 90853 | Group | Group therapy | ~50 min | Cannot bundle with individual |
| 90870 | Procedure | ECT | N/A | 1 per client/day; facility + professional split |
| 90867–69 | Procedure | TMS sessions | 15–30+ min | Prior auth required; outpatient only |
| 90785 | Add-on | Interactive complexity | N/A | Requires base psychotherapy or eval code |
For a complete breakdown of mental health CPT codes and billing codes across all provider types, see our dedicated reference guides.
Psychiatric Nurse Practitioner Billing Codes
This is one of the most searched and least well-answered topics in psychiatric billing. PMHNPs represent a growing share of psychiatric providers, but billing rules vary significantly by state, payer, and supervision model.
Which Codes Can a PMHNP Bill?
Psychiatric nurse practitioners (PMHNP-BC) can bill most psychiatric CPT codes when their state scope of practice and payer contracts allow:
- 90791 — psychiatric diagnostic evaluation
- 90792 — psychiatric diagnostic evaluation with medical services (requires prescribing authority)
- 90832–90837 — standalone psychotherapy
- +90833, +90836, +90838 — psychotherapy add-ons with E/M
- 99202–99215 — evaluation and management codes
- 90863 — pharmacological management (same NCCI restrictions apply)
- 96127 — brief emotional/behavioral assessment
The key question is whether the PMHNP has prescribing authority in their state. CPT 90792 requires medical services — if your state restricts PMHNP prescribing or requires a collaborative practice agreement (CPA), that affects whether 90792 can be billed independently.
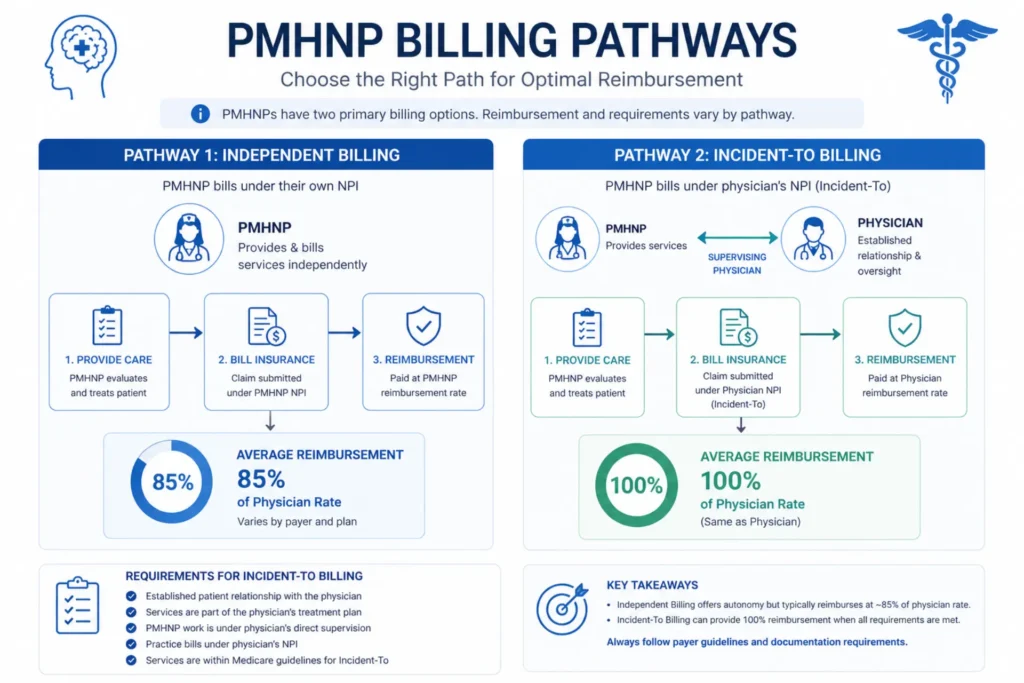
Independent Billing vs Incident-to
Independent (direct) billing: The PMHNP bills under their own NPI using taxonomy code 363LP0808X. Medicare reimburses at 85% of the Physician Fee Schedule (MPFS). The PMHNP must be enrolled in PECOS using CMS Form 855I.
Incident-to billing: The PMHNP bills under a supervising psychiatrist’s NPI. Reimbursement jumps to 100% MPFS — but only when all CMS incident-to requirements are met: the physician must establish the treatment plan, the physician must be immediately available (on-site or virtual per 2026 rules), and the service must continue an established plan of care.
The 15% reimbursement differential matters. For a PMHNP seeing 20 patients per week, the annual revenue difference between 85% and 100% reimbursement is roughly $18,000–$25,000 per year.
Taxonomy and Credentialing
Taxonomy code 363LP0808X identifies a Psychiatric-Mental Health Nurse Practitioner. Using the wrong taxonomy code — like the general NP code 363L00000X — can trigger CO-B7 credentialing denials. The taxonomy code must match across NPI registration, PECOS enrollment, CAQH profiles, and individual payer credentialing.
ANCC PMHNP-BC board certification is required for most payer panels and Medicare enrollment. For detailed guidance on credentialing for mental health providers, we’ve published a separate guide.
Common PMHNP Billing Mistakes
- Billing 90792 without prescribing authority in a restricted practice state
- Using general NP taxonomy instead of 363LP0808X
- Submitting claims before credentialing effective date → CO-B7 denial
- Billing 90863 same day as E/M (NCCI violation)
- Missing modifier -25 on E/M when billing with psychotherapy add-ons
- Not verifying whether the payer recognizes PMHNP as an independent billing provider
| Code Type | Example Codes | PMHNP Eligible? | Key Requirement |
|---|---|---|---|
| Diagnostic Evaluation | 90791, 90792 | Yes | 90792 requires prescribing authority |
| Psychotherapy | 90832, 90834, 90837 | Yes | Must meet time thresholds |
| E/M Services | 99202–99215 | Yes (if allowed) | MDM or time-based rules apply |
| Add-On Psychotherapy | +90833, +90836, +90838 | Yes | Requires E/M base + modifier -25 |
| Screening | 96127 | Yes | Per standardized instrument |
| Medication Management | 90863 | Conditional | Cannot bill with same-day E/M (NCCI) |
| Independent Billing | Own NPI | Yes (FPA states) | 85% MPFS Medicare reimbursement |
| Incident-to Billing | Physician NPI | Conditional | 100% MPFS; requires physician supervision |
How to Submit Psychiatric Claims to Major Insurance Providers
The claim submission workflow for psychiatric billing has more checkpoints than therapy-only billing. Miss one step and the claim either goes to the wrong payer or comes back denied for a reason that had nothing to do with the code you selected.
Step 1: Verify Psychiatric Benefits (Carve-Out Check)
Before the first appointment, run an EDI 270/271 eligibility verification transaction. But don’t stop there. You must identify whether the psychiatric benefit is carved out to a managed behavioral health organization (MBHO).
A patient with Aetna medical coverage might have psychiatric benefits administered by Carelon. If you submit the claim to Aetna, it comes back CO-109 — wrong payer. Check the insurance card for a separate behavioral health phone number. Call if the electronic verification doesn’t specify the carve-out.
Step 2: Prior Authorization
Many psychiatric services require prior authorization, especially:
- Initial psychiatric evaluations (some payers)
- TMS treatment series
- ECT procedures
- Inpatient psychiatric admissions
- Ongoing psychotherapy beyond session limits
Prior authorization numbers must appear on the CMS-1500 form. Missing authorization triggers CO-204 or CO-197 denials.
Step 3: Document and Code
Match the documentation to the code. A 99214 requires moderate MDM. A +90836 add-on requires 38–52 minutes of documented psychotherapy time. An ICD-10 diagnosis must link to a DSM-5-TR diagnosis that supports medical necessity.
Step 4: CMS-1500 Submission
Outpatient psychiatric professional claims go on the CMS-1500 form, submitted electronically as ANSI 837P transactions through a clearinghouse. Key fields:
- Diagnosis pointer mapping (A–L) — link each CPT code to the correct ICD-10
- Place of service: POS 11 (office), POS 02 (telehealth non-home), POS 10 (telehealth home)
- Modifiers: -25 on E/M when billing add-on psychotherapy, -95 for video telehealth, -FQ for audio-only Medicare
Step 5: Payer-Specific Routing
- Medicare Part B — direct submission through MAC
- Medicaid — state-specific managed care plans
- Commercial — may route to medical benefit or BH carve-out
- Optum/Carelon/Magellan — separate claim portals and authorization systems
Step 6: Denial Management
Common psychiatric claim denial codes:
- CO-97 — bundling denial (NCCI edit triggered — 90863 + E/M same day)
- CO-50 — not medically necessary (insufficient documentation for E/M level)
- CO-4 — modifier error (missing -25 on E/M with add-on psychotherapy)
- CO-11 — diagnosis mismatch (ICD-10 doesn’t support the billed service)
- CO-16 — missing information (incomplete CMS-1500 fields)
- CO-204 — authorization missing
- CO-29 — timely filing exceeded
Each denial has a correction pathway. CO-97 requires reviewing the NCCI edit pair and either rebilling with the correct code or appending modifier -59 if services were truly distinct. For a detailed denial resolution framework, see our guide on preventing and appealing mental health billing denials.
| Step | Process | Key Action | Risk If Missed |
|---|---|---|---|
| 1 | Eligibility | Verify coverage + carve-out payer | CO-109 wrong payer |
| 2 | Authorization | Obtain PA for TMS, ECT, inpatient | CO-204 / CO-197 |
| 3 | Documentation | Record diagnosis, time, MDM, notes | CO-50 medical necessity |
| 4 | Coding | Assign CPT + ICD-10 + modifiers | CO-11, CO-4 |
| 5 | CMS-1500 | Complete all claim fields | CO-16 missing info |
| 6 | Submission | Send via 837P through clearinghouse | Format rejection |
| 7 | Adjudication | Payer processes claim | CO-119 benefit limits |
| 8 | Denials | Review ERA (835) / EOB | CO-97, CO-50, CO-4 |
| 9 | Appeals | Corrections and resubmissions | CO-29 timely filing |
| 10 | Payment | Post ERA to patient account | Reconciliation errors |
Common CPT Codes for Psychotherapy Sessions in Psychiatry
Psychiatrists don’t just manage medications. Many provide psychotherapy — and the billing rules for psychotherapy in psychiatric practice are different from how a therapist bills the same service.
When a Psychiatrist Bills Standalone Therapy Codes
When a psychiatrist provides only psychotherapy — no medication adjustment, no medical evaluation — they bill the same standalone codes as any therapist:
- 90832 — 16–37 minutes face-to-face
- 90834 — 38–52 minutes face-to-face
- 90837 — 53+ minutes face-to-face
Some payers question psychiatrists billing standalone therapy. The documentation must clearly reflect that the session focused on psychotherapy — CBT, DBT, psychodynamic therapy, or another modality — without a medical management component.
Add-On Codes for Combined E/M + Therapy
The more common scenario in psychiatry: the provider spends part of the visit on medication management (E/M) and part on psychotherapy. This is where add-on codes come in:
- 99214 + 90833 — moderate MDM E/M + 16–37 min therapy (modifier -25 on 99214)
- 99214 + 90836 — moderate MDM E/M + 38–52 min therapy (modifier -25 on 99214)
- 99213 + 90833 — low MDM E/M + 16–37 min therapy (modifier -25 on 99213)
The E/M level is determined by MDM — not time — when billed with psychotherapy add-ons. Time spent on E/M activities does not count toward psychotherapy minutes. The two time pools must be completely separate.
Modifier -25: The Rule That Triggers Half the Denials
Modifier -25 on the E/M code tells the payer: “This E/M service was significant and separately identifiable from the psychotherapy.” Without -25, the payer sees two services and denies the add-on as CO-4 (modifier error) or CO-97 (bundling).
Documentation must support the modifier. The E/M note and the psychotherapy note should reflect distinct clinical activities. A single blended note that doesn’t separate the medication discussion from the therapy content will fail on audit.
The NCCI Medication Management Conflict
This is the rule most psychiatric practices get wrong:
NCCI edits prohibit billing medication management (90863) on the same day as an E/M code or psychotherapy code by the same provider.
If the visit starts as medication management but the clinical discussion extends into therapy, the service shifts to E/M + psychotherapy add-on. You cannot bill 90863 alongside 99214 or 90834. The codes are mutually exclusive on the same date of service.
When a psychiatrist provides both medication oversight and therapy in one visit, the correct billing is E/M + psychotherapy add-on — not medication management + therapy.
Time Documentation
Start and stop times are required for all psychotherapy codes. The documentation must show:
- When psychotherapy began and ended
- When E/M activities occurred (separately)
- Total face-to-face psychotherapy time
- That the times do not overlap
Audits frequently target 90837 and +90838 because of the high reimbursement and strict 53-minute threshold.
| Visit Scenario | Codes to Bill | Modifier | Time Requirement | Common Denial Risk |
|---|---|---|---|---|
| Therapy-only visit | 90834 | None | 38–52 min | Under-time CO-50 |
| Long therapy session | 90837 | None | 53+ min | Missing timestamps |
| E/M + brief therapy | 99213 + 90833 | -25 on E/M | ≥16 min therapy | Missing modifier CO-4 |
| E/M + extended therapy | 99214 + 90836 | -25 on E/M | ≥38 min therapy | Bundling CO-97 |
| Medication management only | 90863 | None | ≥16 min | Same-day E/M conflict |
| Combined med + therapy | 99214 + 90833/36 | -25 on E/M | Split time required | Double-counting time |
| Crisis psychotherapy | 90839 | None | 30–74 min | Improper combination |
| Group therapy | 90853 | None | ~50 min | Incorrect pairing |
Psychiatric Billing Software — Top Features to Look For
Choosing billing software for a psychiatric practice isn’t the same as choosing software for a therapy clinic. Psychiatrists need e-prescribing, E/M + add-on code logic, medication management templates, and NCCI compliance checking that most therapy-focused platforms don’t offer.
Must-Have Features for Psychiatry
Not every EHR or practice management system handles psychiatric billing well. These features separate platforms that work for psychiatrists from platforms that work for therapists:
- EPCS (Electronic Prescribing for Controlled Substances) — psychiatrists prescribe Schedule II–V medications. EPCS integration with DEA compliance and two-factor authentication isn’t optional. It’s a federal requirement.
- E/M + psychotherapy add-on auto-detection — software that recognizes when an E/M code is billed alongside a psychotherapy code and auto-appends modifier -25
- Medication management documentation templates — structured fields for the 12-element documentation checklist (diagnosis, medication history, side effects, lab values, mental status exam)
- NCCI edit alerts — real-time warnings when 90863 is billed same-day with E/M or psychotherapy
- DSM-5 to ICD-10 crosswalk — automated mapping from diagnostic criteria to billing codes
- Prior authorization tracking — dashboard for TMS, ECT, and inpatient authorization status
- Claim scrubbing — pre-submission validation of CPT codes, modifiers, diagnosis pointers, and payer rules
- ERA auto-posting (835) — automated payment posting from electronic remittance advice
- Eligibility verification (270/271) — with carve-out detection for behavioral health payers
- Telehealth integration — auto-population of modifier -95 or -FQ and correct POS codes (02 vs 10)
Software Comparison
| Platform | Cost Range | EPCS | Coding Automation | Prior Auth | Telehealth | Best For |
|---|---|---|---|---|---|---|
| TherapyNotes | $79–$99/mo | Yes | Basic | Limited | Yes | Solo / therapy-heavy |
| SimplePractice | $79–$99/mo | Yes | Basic | Basic | Yes | Solo / small group |
| Valant | $150–$250/mo | Yes | Advanced | Yes | Yes | BH groups (psychiatry focus) |
| AdvancedMD | $250–$400/mo | Yes | Advanced | Yes | Yes | Multi-specialty large practice |
| Kareo/Tebra | $100–$200/mo | Yes | Moderate | Basic | Yes | Mixed clinics |
| DrChrono | $150–$300/mo | Yes | Advanced | Moderate | Yes | Mobile-first practices |
| ICANotes | $100–$150/mo | Yes | Moderate | Limited | Yes | Psychiatry-focused EHR |
| Athenahealth | $300–$600+/mo | Yes | Advanced | Yes | Yes | Enterprise systems |
| Netsmart | Custom | Yes | Advanced | Yes | Yes | Public-sector BH orgs |
| Qualifacts | Custom | Yes | Advanced | Yes | Yes | Community BH organizations |
Software vs Outsourced Billing
Software handles claim transmission. It doesn’t resolve denials. When a CO-97 bundling denial comes back on a 90863 + 99214 same-day conflict, your biller needs to understand the NCCI logic, determine whether to rebill as E/M + psychotherapy add-on, and resubmit with correct codes and modifier -25. That’s an expertise question, not a software question.
For practices with denial rates above 10%, complex payer mixes (Medicare + Medicaid + commercial carve-outs), or limited administrative staff, outsourcing psychiatric billing is often more cost-effective than software alone. The real comparison isn’t software vs outsourcing — it’s control vs expertise. For detailed cost analysis, see our guide on mental health billing services cost.
Not Sure If Software Alone Can Handle Your Psychiatric Billing?
EliteMed Financials combines certified psychiatric coding expertise with full RCM — from E/M code selection to medication management documentation to payer-specific compliance.
Inpatient Psychiatric Billing — Unique Rules and Codes
No competitor ranking for “psychiatric billing services” covers inpatient billing. That’s a gap. If your practice includes hospital-based services or you’re billing for inpatient psychiatric care, this section is where the real complexity lives.
Professional vs Institutional Billing
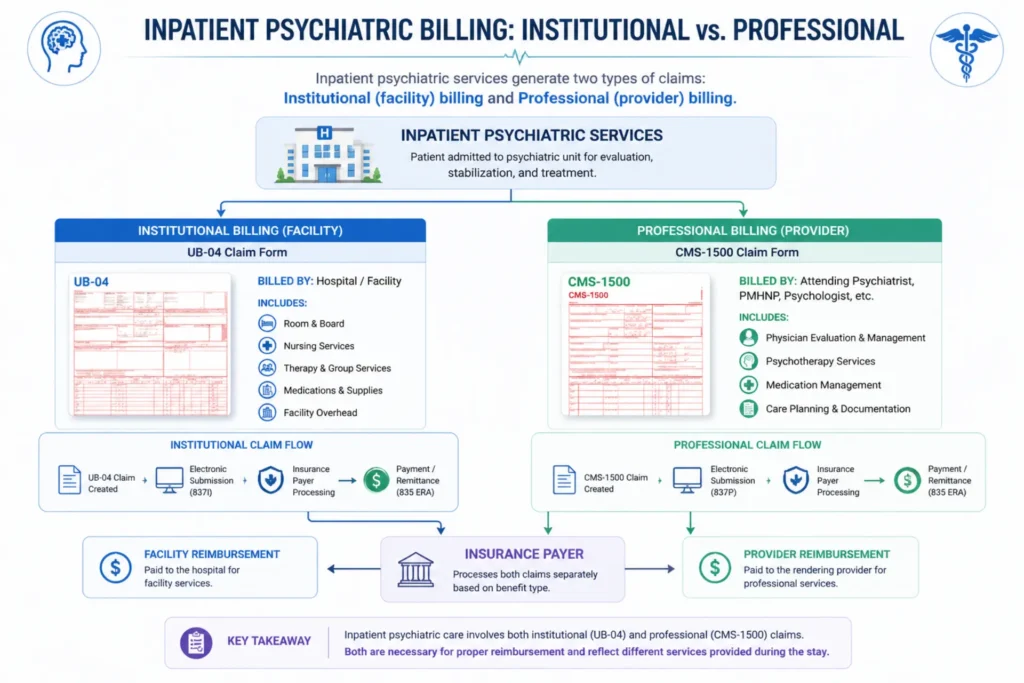
Inpatient psychiatric billing splits into two separate claims:
Institutional billing (UB-04 / 837I): The hospital submits facility charges — room and board, pharmacy (0250), laboratory (0300), nursing care, and ancillary services. These use revenue codes.
Professional billing (CMS-1500 / 837P): The psychiatrist, PMHNP-BC, or PA bills professional services — evaluations, therapy, ECT, rounds — under their individual NPI.
Both claims go to the same payer, but they’re processed separately. A hospital-employed psychiatrist can still bill professional services on CMS-1500 if billing under their individual NPI.
Revenue Codes for Inpatient Psychiatric Services
Revenue codes on the UB-04 define the room type and service category:
| Revenue Code | Description | Use Case |
|---|---|---|
| 0114 | Psychiatric — private room | Single-patient accommodation |
| 0124 | Psychiatric — semi-private room | Shared room (2-bed) |
| 0126 | Behavioral health / substance abuse | SUD-specific services |
| 0134 | Psychiatric — 3–4 bed room | Multi-bed unit |
| 0144 | Psychiatric — deluxe private | Premium accommodation |
| 0154 | Psychiatric — ward | General inpatient ward |
| 0204 | Psychiatric — intensive/other | Specialized intensive units |
| 0250 | Pharmacy | Medication charges |
| 0300 | Laboratory | Diagnostic testing |
| 0900 | Behavioral health general | General psychiatric services |
| 0911 | Psychiatric rehabilitation | Therapy and recovery programs |
Authorization Requirements
Inpatient psychiatric admissions require prior authorization. For Medicaid fee-for-service clients, specific EPA (Expedited Prior Authorization) numbers apply:
- EPA 870001610 — Involuntary Treatment Act (ITA) admissions
- EPA 870001611 — Voluntary admissions
The EPA number must appear in the Prior Authorization Number field on the claim. A new EPA is required whenever there’s a change in legal status, principal diagnosis, or hospital of service. Authorized days must match the PA record — unauthorized days are noncovered and must be billed on separate claim lines.
For managed care enrollees, authorization comes from the MCO or the MCO’s Behavioral Health Services Organization (BHSO).
The 24-Hour Evaluation Rule
Each person admitted to an inpatient psychiatric facility must be examined and evaluated by a licensed physician or P-ARNP within 24 hours of admission, or payment will be denied.
This isn’t a guideline. It’s a hard rule. No evaluation within 24 hours = no payment for that admission date. The evaluation is typically billed as 90791 or 90792, or as an initial inpatient E/M code (99221–99223).
Professional Services During Inpatient Stay
For each day of inpatient psychiatric care, allowable professional services include:
A day’s rounds plus one of the following:
- Individual psychotherapy (up to 1 hour)
- Multiple/family group therapy
- Group therapy
- ECT (90870 — limited to 1 per client per day)
- Narcosynthesis (90865)
Court testimony (CPT 99075) is billable per hearing for involuntary admission proceedings.
Split Billing When Care Focus Changes
When a patient’s care focus shifts from psychiatric to medical (or medical to psychiatric), services must be billed on separate claims. This happens when:
- A psychiatric inpatient develops a medical complication requiring primary medical management
- A medical patient develops an acute psychiatric crisis requiring psychiatric admission
Revenue codes change when the focus shifts. Documentation must clearly establish the date and clinical reason for the focus change.
Voluntary vs Involuntary Admission Billing
Legal status affects billing directly:
- SCI=V (voluntary) in the Special Claims Indicator field
- SCI=I (involuntary) in the Special Claims Indicator field
Voluntary and involuntary portions of a stay must be authorized separately and billed separately. For involuntary admissions under ITA, the payer does not cover past the 20th calendar day from initial detention without a length-of-stay extension certification from the BH-ASO.
Medicare Part A Exhaustion
Medicare Part A covers inpatient psychiatric care in general hospitals without a day limit, but freestanding psychiatric hospitals have a 190-day lifetime benefit limit. When Part A benefits are exhausted during a psychiatric stay, the hospital must obtain authorization for Medicaid payment as secondary payer.
Medicare’s Inpatient Psychiatric Facility Prospective Payment System (IPF PPS) reimburses using per diem rates adjusted by APR-DRGs (740–760, 770, 772–776), length of stay, severity of illness, and wage index. ECT receives an additional per-treatment adjustment.
Inpatient Psychiatric Billing Requires Specialized Knowledge
Authorization rules, revenue codes, split billing, Medicare Part A coordination, and the 24-hour evaluation requirement — EliteMed handles the complexity so your facility can focus on patient care.
Mental Health Billing Services →Outsource Psychiatric Billing — Benefits for Busy Practices
Most psychiatric practices face the same question every therapy practice faces: handle billing in-house or outsource it? The math usually favors outsourcing for psychiatry specifically because the coding is more complex.
What Outsourced Psychiatric Billing Includes
A specialized psychiatric billing company handles:
- Eligibility verification (270/271) with carve-out detection
- Prior authorization for TMS, ECT, and inpatient admissions
- Coding: 90792, E/M + psychotherapy add-ons, medication management
- Claim scrubbing (NCCI edits, modifiers, medical necessity)
- CMS-1500 submission via 837P through clearinghouses
- UB-04 coordination for inpatient psychiatric billing
- ERA/EOB payment posting (835 processing)
- Denial management — CO-97 bundling, CO-50 medical necessity, CO-4 modifier errors
- AR follow-up on unpaid claims
- Patient statements and balance management
- Credentialing — PECOS, CAQH, commercial payer enrollment
- Monthly reporting and analytics dashboards
The Real Cost Comparison
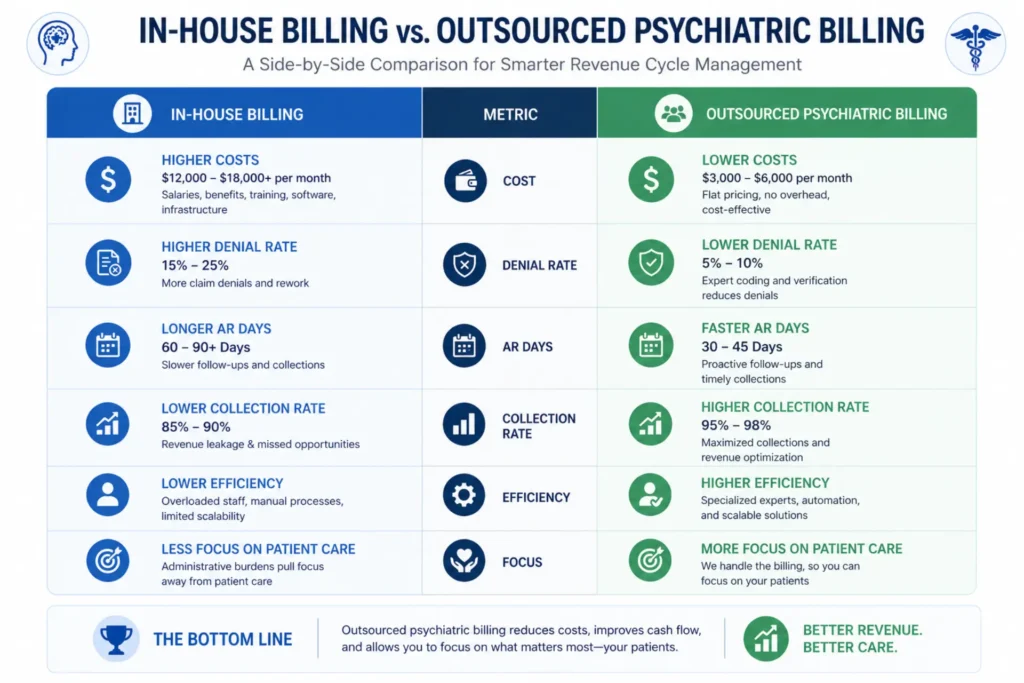
A fully loaded in-house psychiatric biller costs $70,000–$100,000 per year when you add salary, benefits, software licenses, clearinghouse fees, training, and management overhead.
Outsourcing at 6–8% of collections on $600,000 in annual revenue costs approximately $36,000–$48,000 per year.
The break-even point is roughly $700,000–$1,000,000 in annual revenue. Below that, outsourcing is almost always cheaper.
| Dimension | In-House | Outsourced | Advantage |
|---|---|---|---|
| Annual Cost | $70K–$100K | ~$36K–$54K (6–9%) | Outsourced |
| Denial Rate | ~15–20% | <5% | Outsourced |
| AR Days | 45–60 days | 28–35 days | Outsourced |
| Staffing | Requires hiring + training | Included in service | Outsourced |
| Expertise | General billing knowledge | Psychiatry-specialized | Outsourced |
| Scalability | Limited by staff | Highly scalable | Outsourced |
| Compliance Updates | Manual tracking | Vendor-managed | Outsourced |
When Outsourcing Makes Financial Sense for Psychiatry
- Solo psychiatrist — almost always cheaper than hiring a dedicated biller
- Small group (2–5 providers) — outsourcing or hybrid recommended
- Denial rate above 10% — outsource immediately while fixing root causes
- Complex payer mix (Medicare + Medicaid + multiple commercial carve-outs) — specialized routing expertise needed
- Adding inpatient services — UB-04 facility billing requires dedicated knowledge
- PMHNP practice — credentialing and taxonomy code management adds complexity
- High staff turnover — outsourcing provides continuity regardless of hiring challenges
For practices evaluating whether to outsource, see our guides on outsourcing mental health billing and how to choose a mental health billing service.
How to Choose a Psychiatric Billing Service for Small Practices
Choosing a billing partner for a psychiatric practice is different from choosing one for a therapy clinic. The vendor must understand dual-coding logic, NCCI restrictions, medication management rules, payer carve-outs, and — if applicable — inpatient facility coordination.
Questions to Ask Before Signing
- What percentage of your clients are psychiatric practices specifically (not general therapy)?
- Do you handle 90792, E/M + psychotherapy add-on coding, and 90863 NCCI conflicts?
- What is your average denial rate for psychiatric claims? (Target: <7–10%)
- What is your average days in AR? (Target: <30–35 days)
- Do you report net collections or gross collections?
- What is your fee structure? (Percentage, flat per claim, or retainer?)
- Do you handle credentialing and payer enrollment?
- Do you manage prior authorizations for TMS, ECT, and inpatient admissions?
- Can I export all billing data if I terminate the contract?
- Do you process small claims below $50? Or ignore them?
- What clearinghouse do you use? (Waystar, Change Healthcare, etc.)
Red Flags in Billing Company Proposals
- No HIPAA Business Associate Agreement (BAA) offered upfront — walk away
- Proprietary software with no data export — data lock-in trap
- Guaranteed 95%+ collections without seeing your data — no legitimate company guarantees results before reviewing your payer mix and denial patterns
- Reporting gross collections only — inflated numbers that hide real performance
- No psychiatric-specific experience — general medical billing companies applying therapy billing logic to psychiatric claims
- Denial management charged as add-on — it should be included in the base fee
- 90+ day termination notice — too restrictive for a service relationship
Net Collections vs Gross Collections
This is how billing companies hide poor performance.
Gross collections = total amount billed or claims submitted. A company can report “90% gross collections” while actually collecting only 70% of what’s contractually owed.
Net collections = actual revenue collected versus the allowed amount from payer contracts. This is the real number. Always verify by requesting sample monthly reports showing charges, contractual adjustments, payments, and write-offs.
Onboarding and Data Migration
A typical onboarding timeline runs 30–60 days:
- Payer enrollment verification and updates
- EDI enrollment (837P/835 setup) with clearinghouse
- Fee schedule configuration
- EHR integration and data mapping
- Legacy AR assessment (will the new company work your outstanding receivables?)
- Staff training on new workflows
- Parallel billing period (running both systems for 30 days)
The critical question: who owns outstanding AR if you terminate later? Get this in writing before signing.
Find Out How Much Revenue Your Psychiatric Practice Is Losing
EliteMed Financials provides psychiatric billing, coding, denial management, and full RCM — with denial rates under 5% and first-pass resolution above 95%.
Stop guessing. Let our team audit your current revenue cycle and show you what you’re missing.
| Criteria | What to Ask | Red Flag | Green Flag |
|---|---|---|---|
| Coding Expertise | Handle 90792, E/M, add-ons? | No psychiatry experience | Demonstrates real cases |
| Denial Rate | Average denial rate? | >12–15% | <7–10% |
| AR Days | Average AR days? | >45–60 days | <30–35 days |
| Fee Structure | What are fees? | Vague pricing | Clear % or flat fee |
| Data Ownership | Can I export data? | No access | Full CSV/EDI export |
| Contract Terms | Termination period? | 90+ days | 30–60 days |
| Reporting | Net or gross? | Gross only | Net collections |
| Credentialing | Included? | Not offered | Standard inclusion |
| Tech Stack | Clearinghouse? | Proprietary only | Standard integrations |
| Claims Handling | Small claims? | Ignored | Fully processed |
| Compliance | HIPAA BAA? | None offered | Signed BAA at onboarding |
| Support | Account manager? | Generic helpdesk | Dedicated contact |
Voice Search Q&A
What is psychiatric billing? Psychiatric billing is the process of submitting insurance claims for services provided by psychiatrists, psychiatric nurse practitioners, and physician assistants in mental health. It includes E/M codes for medication management, psychotherapy add-on codes, diagnostic evaluations like 90792, and procedures such as ECT and TMS.
What CPT codes do psychiatrists use? Psychiatrists commonly use CPT codes 90792 for psychiatric evaluations with medical services, 99213 through 99215 for E/M medication management visits, psychotherapy add-on codes 90833, 90836, and 90838, and procedure codes 90870 for ECT and 90867 through 90869 for TMS.
Can a psychiatric nurse practitioner bill independently? Yes, in states with full practice authority, a PMHNP can bill independently under their own NPI using taxonomy code 363LP0808X. Medicare reimburses at 85% of the Physician Fee Schedule for independent NP billing. In restricted states, incident-to billing under a supervising psychiatrist pays at 100%.
How much does outsourced psychiatric billing cost? Most psychiatric billing companies charge between 4% and 10% of net collections, with the average around 6 to 8 percent. For a practice collecting $600,000 per year, that works out to roughly $36,000 to $48,000 annually — typically less than hiring a full-time in-house biller.
What is the difference between 90791 and 90792? CPT 90791 is a psychiatric diagnostic evaluation without medical services. Any qualified mental health provider can bill it. CPT 90792 is a psychiatric diagnostic evaluation with medical services, requiring prescribing authority. Only psychiatrists, PMHNPs, and PAs with prescribing scope can bill 90792.
What is the 24-hour rule for inpatient psychiatric billing? Inpatient psychiatric admissions require that a licensed physician or psychiatric nurse practitioner examine and evaluate the patient within 24 hours of admission. If this evaluation does not occur within 24 hours, payment for the admission is denied.
Frequently Asked Questions
What is the difference between psychiatric billing and mental health billing?
Psychiatric billing is a subset of mental health billing that focuses on prescribing providers — psychiatrists, PMHNPs, and PAs. It includes E/M codes for medication management, diagnostic evaluations with medical services (90792), and procedures like ECT and TMS. General mental health billing covers therapy services billed by LCSWs, LPCs, and psychologists using psychotherapy codes.
Can a psychiatrist bill psychotherapy and medication management on the same day?
Not using 90863 and psychotherapy codes together. NCCI edits prohibit billing medication management (90863) on the same day as E/M or psychotherapy by the same provider. The correct approach for combined visits is E/M + psychotherapy add-on codes with modifier -25 on the E/M.
What modifier is needed for E/M with psychotherapy add-on codes?
Modifier -25 must be appended to the E/M code (99213, 99214, or 99215) when billing with psychotherapy add-on codes (+90833, +90836, or +90838). This modifier indicates the E/M service was significant and separately identifiable from the psychotherapy.
What taxonomy code should a PMHNP use for billing?
Psychiatric-Mental Health Nurse Practitioners should use taxonomy code 363LP0808X on all credentialing applications, NPI registrations, and payer submissions. Using the general NP taxonomy code 363L00000X can trigger CO-B7 credentialing denials.
How often can a psychiatrist bill 90792?
Most payers limit 90792 to one per client, per provider or group with the same billing NPI, per calendar year. CMS considers an extended break approximately 6 months from the last visit, at which point a new evaluation may be justified.
What are the revenue codes for inpatient psychiatric billing?
Common revenue codes include 0114 (private psychiatric room), 0124 (semi-private), 0134 (3–4 bed), 0154 (ward), 0204 (intensive/other), 0250 (pharmacy), and 0300 (laboratory). These are submitted on UB-04 forms for institutional billing.
What is the break-even point for outsourcing psychiatric billing?
For most psychiatric practices, the break-even threshold is roughly $700,000–$1,000,000 in annual revenue. Below that, outsourcing at 6–8% of collections is typically cheaper than hiring a full-time biller at $70,000–$100,000 fully loaded annual cost.
What are common denial codes in psychiatric billing?
The most frequent denial codes include CO-97 (bundling/NCCI edit — especially 90863 + E/M conflicts), CO-50 (medical necessity — insufficient documentation for E/M level), CO-4 (modifier error — missing -25), CO-B7 (provider not credentialed), CO-204 (authorization missing), and CO-29 (timely filing exceeded).
Does Medicare cover psychiatric services by nurse practitioners?
Yes. Medicare covers psychiatric services billed by PMHNPs who are enrolled through PECOS with board certification (ANCC PMHNP-BC). Independent PMHNP billing is reimbursed at 85% of the Medicare Physician Fee Schedule. Incident-to billing under a supervising psychiatrist qualifies for 100% reimbursement when CMS supervision requirements are met.
What documentation is required for medication management visits?
Medication management requires 12 documentation elements: date/time, current diagnosis, interim medication history, current symptoms (including physical), medication reactions and side effects, mental status exam, medication modifications, reasons for changes or continuation, desired drug levels, current lab values, anticipated outcomes, and provider signature.
Wrapping Up
Psychiatric billing operates in its own lane. It’s not therapy billing with medication added on top. It’s a dual-coding system where E/M, psychotherapy, medication management, and procedural billing all intersect — governed by NCCI edits, payer carve-outs, modifier rules, and documentation requirements that most general billing teams aren’t built to handle.
The practices that treat psychiatric billing like standard mental health billing are the ones running 15–20% denial rates. The practices that understand dual-code triage, modifier -25 logic, 90792 prescribing context, and the 90863 same-day restriction are the ones collecting what they’ve earned.
Whether you handle billing in-house with the right software, outsource to a specialized psychiatric billing partner, or run a hybrid model, the fundamentals in this guide are the operational baseline. Get them right, and your revenue cycle stops leaking money.
Psychiatric Billing, Coding, Credentialing & Full RCM
EliteMed Financials
We serve psychiatric practices nationwide — from solo psychiatrists to multi-site groups. HIPAA-compliant billing, certified coding, PMHNP credentialing, denial management, and complete revenue cycle management.