Wound care billing companies are not all built the same — and the difference between the right choice and the wrong one shows up directly in your denial rate, your days in AR, and how many skin substitute claims make it through to payment without a fight. This guide cuts through the marketing noise to show you exactly what separates a true wound care billing specialist from a generalist with a niche page, which criteria actually predict performance, and why graft billing capability is the single most important differentiator most practices overlook when they’re shopping for a billing partner.
Table of Contents
Why Wound Care Billing Requires a Specialist, Not a Generalist
Most practice managers don’t realize wound care billing is in a completely different weight class than general medical billing until they’re staring at a 30% denial rate and wondering why. The answer is almost always the same: the billing company they hired was built for family medicine, orthopedics, or multi-specialty groups — and wound care coding threw them into territory they weren’t trained for.
The Complexity Drivers That Make Wound Care Billing Different
Wound care sits at the intersection of multiple procedure-heavy CPT families, each with its own selection logic, modifier requirements, and payer-specific rules. Debridement alone has two completely separate code families — selective debridement (97597–97598) and surgical debridement (11042–11047) — where code selection depends on the deepest tissue layer removed, not what’s visible at the surface. A billing team that gets this wrong on every claim is quietly costing the practice thousands every month.
Layer in skin substitute application (CPT 15271–15278), NPWT (97605–97606 and G0278–G0280), hyperbaric oxygen therapy (99183–99184), and E/M visits billed with modifier -25 on the same date, and you have dual-coding requirements most generalist teams don’t have the training to handle. Then add the site-of-service differential — the same procedure billed in a physician office (POS 11) versus a hospital outpatient department (POS 22) generates different reimbursement, different modifiers, and different documentation requirements entirely.
The 2026 OPPS Final Rule reclassified skin substitute products as incident-to supplies, separating product payment from procedure payment under new APC structures. That “unpackaging” change means HOPDs in particular must completely relearn billing logic that worked fine for years. Most billing companies have not updated their workflows to match.
📊 DATA: OIG’s 2024 reporting flagged over $10 billion in Medicare Part B spending on skin substitutes, with widespread documentation deficiencies and patterns of overutilization. That level of scrutiny means your documentation and coding must survive MAC review — which requires a billing partner who understands LCD criteria, not just CPT codes.
The Revenue Impact of Getting It Wrong
The practical financial consequences of using a generalist billing team for wound care are predictable and quantifiable. Denial rates for wound care claims managed by generalist billers typically run 20–35%, compared to 8–12% when managed by specialists. The cost of a single denied skin substitute claim runs $2,000–$5,000 in direct write-off risk — and that doesn’t count the 30–60 minutes of denial rework cost on top of it.
For a practice applying 15 grafts per week, a 25% denial rate represents roughly $281,000 in annual lost revenue. A specialist billing company reduces that to under 10%, recovering approximately $168,000 more per year. The specialist premium in billing fees — typically 1–2% more than a generalist — pays for itself on the first month of graft billing alone.
In-house billing isn’t the answer either. When you fully load the cost of wound care billing staff — salaries, benefits, software, training, and turnover — you’re looking at 10–15% of collections. Outsourcing to a specialist typically costs 5.4–8%, with meaningfully better collection rates. The math is not close.
If you’re building a wound care program from scratch or auditing your current RCM setup, our wound care RCM guide breaks down the complete revenue cycle framework specifically for wound care practices.
The 7 Services Any Wound Care Billing Company Must Offer
Before you evaluate specific companies, get clear on the floor. A wound care billing company should not get credit for doing the basics — those are table stakes. Here’s what that baseline looks like, and what separates the top tier from the rest.
Core Service Checklist
A complete wound care billing company must deliver all seven of these without add-on fees or asterisks:
- Wound care CPT coding — full coverage of debridement (11042–11047, 97597–97598), skin substitute application (15271–15278), NPWT (97605–97606), HBOT (99183–99184), and E/M with modifier -25
- Insurance eligibility verification with product formulary check — not just demographic eligibility; product-level verification that confirms the specific skin substitute or CTP is covered under that patient’s plan before you order it
- Prior authorization management — end-to-end for all high-cost procedures including CTPs, HBOT, and NPWT; including UHC Medicare Advantage’s post-service, pre-pay review model
- Denial management and appeals — wound-specific, with denial root-cause analysis categorized by CPT family, not just a generic “rework” queue
- Medicare LCD compliance auditing — with active monitoring across MAC jurisdictions (L36690, L35041, L36377) and alerts when coverage criteria change
- MIPS/QPP performance tracking — wound healing rates and 30-day follow-up plans are now tied to CMS reimbursement; your billing company needs to own this
- Revenue cycle analytics with wound-specific KPI benchmarks — first-pass acceptance, denial rate by procedure type, net collection rate, days in AR, and AR over 90 days
The Advanced Services That Separate Top-Tier Firms
The billing companies that actually perform well for wound care practices don’t just check those seven boxes — they operate a layer deeper on every one of them. The difference shows up in graft billing specifically: dedicated Q-code management, JW/JZ modifier accuracy (the standard should be ≥99%), CMS-1500 Field 19 documentation with NDC/UPC and WAC data, and pre-service authorization tied to product selection rather than reactive PA submission after the product is already ordered.
The best firms also maintain a product-formulary matrix updated quarterly — so when UHC changes its non-porcine skin substitute review policy or a new LCD drops, their clients know before they bill, not after they deny.
For the complete wound care coding framework, our wound care billing and coding services page covers the full scope of what specialist-level coding management looks like in practice.
⚠️ KEY POINT: In 2026, 40–60% of skin substitute, HBOT, and NPWT claims require prior authorization. If a billing company doesn’t have a structured PA workflow that covers product formulary verification before you order the graft, they’re setting you up for retroactive denials.
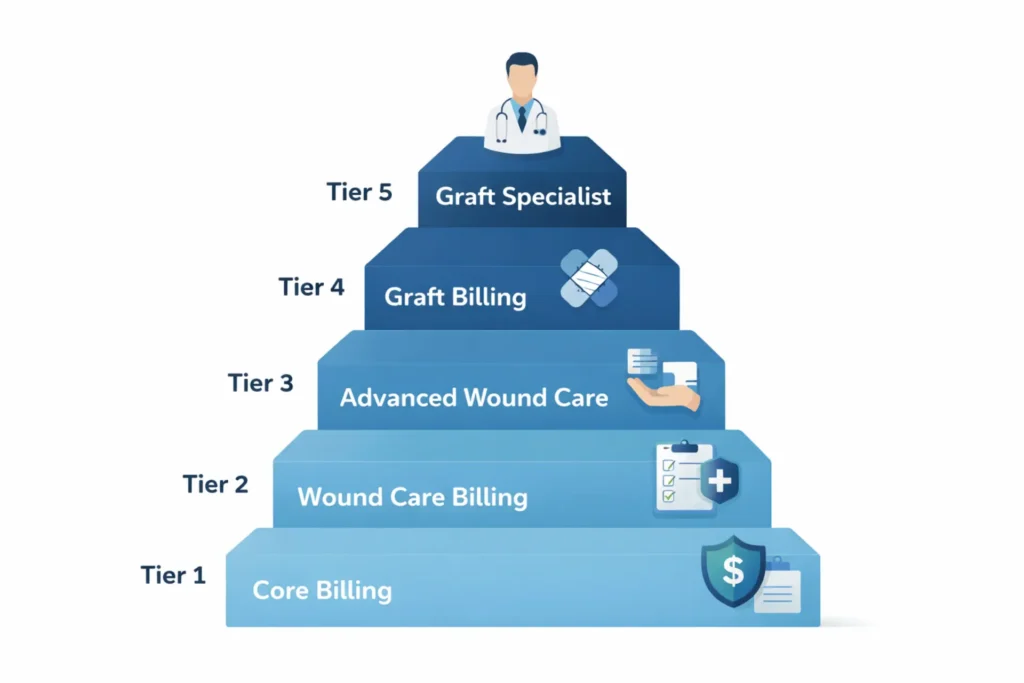
How to Evaluate Wound Care Billing Companies — The 5-Tier Criteria Framework
Before you sign anything, ask this question: can this company prove their performance with 12 months of wound-care-specific KPI data? If the answer is no, they’re operating without accountability. The five-tier framework below gives you a structured way to evaluate any billing company — and quickly identify where they’re weak.
Tier 1 — Core Billing Competency
Request 12-month trend reports broken out by procedure type: debridement, NPWT, HBOT, and skin substitute CTPs separately. A company that can only give you blended averages is hiding something.
- First-pass acceptance rate target: 85–95% (wound care); below 80% is a problem; below 70% on CTPs is a red flag
- Net collection rate target: 88–92% (specialist-managed); below 85% means revenue is leaking somewhere
- Days in AR target: 40–60 days; above 75 days indicates systemic follow-up failures
Tier 2 — Wound-Specific Compliance Knowledge
Ask them to show you their LCD matrix for your MAC jurisdiction. Can they tell you the difference between what CGS L36690 covers in Kentucky and Ohio versus what Novitas L35041 covers in Texas and Oklahoma? Do they know the implications of the December 2025 LCD withdrawal for practices that were relying on those coverage parameters? If they hesitate, they don’t have the depth your practice needs.
Tier 3 — Prior Authorization Depth
100% of CTP claims should be pre-authorized before service. HBOT and NPWT should be at 95%+. ADR response time should be guaranteed at 24–48 hours — anything over 72 hours for a high-dollar graft claim is unacceptable and almost always recoverable with the right workflow.
Tier 4 — Denial Management Strength
An overall appeal success rate of 60–75% is the target for documentation-based denials. If a company can’t categorize your denials by root cause — LCD failure, missing modifier, wrong CPT family, ICD-10 specificity issue — they cannot systematically prevent them. Ask them: “If we have a 15% denial rate, can you tell us in 30 days what’s causing it and show us a plan to fix it?” The answer tells you everything.
Tier 5 — Graft and Skin Substitute Specialist Depth
This is where 90% of billing companies fail. If their answer to graft billing is “we bill what the EMR sends,” you are not talking to a wound care specialist. A Tier 5 company maintains a product-specific Q-code matrix (updated quarterly), verifies product formulary coverage before the first application, manages UHC MA’s PCA-1-24-02596 post-service review workflow, achieves ≥99% JW/JZ modifier accuracy, and documents lot numbers and WAC/invoice data in CMS-1500 Field 19 as standard practice.
| Tier | Criterion | Benchmark | Red Flag |
|---|---|---|---|
| 1 | First-pass acceptance | 85–95% | <80% overall |
| 2 | LCD knowledge | Jurisdiction-specific matrix on file | “We follow CMS guidelines” (vague) |
| 3 | PA management | 100% CTPs pre-authorized | No PA tracking system |
| 4 | Denial management | 60–75% appeal success | Cannot categorize denials by type |
| 5 | Graft billing | ≥99% JW/JZ accuracy; Q-code matrix | “We bill what the EMR sends” |
Wound Care Billing Companies — What Each Specializes In
Here’s the honest comparison most of these companies won’t show you on their own websites. None of the following information is a criticism — each company has a legitimate use case. But knowing where each fits helps you make the right call for your practice.
| Company | Type | Key Strength | Graft Billing | Best Fit | Limitation |
|---|---|---|---|---|---|
| AltuMED | Specialty RCM | Modifier-aware coding; strong CPT families | Partial | Outpatient clinics, multi-specialty | No public KPI data; graft workflows implied but not documented |
| ARIA/CGM | Enterprise RCM | #1 KLAS for Ambulatory RCM (2026); hospital-grade workflows | Limited | HOPD, hospital-affiliated programs | Award is not wound-care-specific; enterprise focus may not suit independent practices |
| Medheave | Wound-focused platform | 15+ years wound-only experience; nationwide | Partial | Freestanding clinics, small/mid practices | No public KPI benchmarks; CTP workflow depth not documented |
| PRG | Generalist + wound vertical | 24/7 support; end-to-end billing | Mid-level | Multi-specialty groups with wound component | Wound care is one of many specialties — not the primary focus |
| MedStates | Multi-specialty | Strong CPT coding; prior auth handling | Basic | Practices wanting one vendor for all specialties | Least wound-specific on this list; LCD depth not demonstrated |
| MedCare MSO | MSO model | Billing + operations + compliance | Partial | Multi-site, high-volume centers | Less billing-only flexibility; higher operational overhead |
| SwiftCare | Generalist | Fast, responsive billing | Minimal | Small practices, low CTP volume | No documented graft-specific workflows |
| BillingFreedom | Low-cost generalist | Transparent pricing; accessible | Minimal | Budget-focused small practices | No wound specialization depth |
| Summit RCM | Specialty RCM | Denial management focus; wound experience | Partial | Mid-sized wound centers | No public KPI data |
| EliteMedFinancials | Wound care specialist | GRAFT TRACK; end-to-end from PA to claim; credentialing + digital growth | Full-stack | Practices with graft volume; growth-focused wound programs | Focused on wound care — not the choice for general multi-specialty billing |

The Gap That Separates EliteMedFinancials
The one thing missing from every competitor in this table is a dedicated, documented graft billing program. Skin substitute billing — Q-code management, product formulary verification, JW/JZ modifier accuracy, Field 19 documentation, and PA workflows by payer type — requires a protocol, not just billing awareness. GRAFT TRACK is that protocol. No competitor mentioned above offers an equivalent documented graft billing workflow tied to prior authorization management, audit defense, and revenue analytics at the product level.
Skin Substitute and Graft Billing — The Advanced Tier Most Companies Skip
This is where most wound care practices quietly lose the most money — not on debridement claims, not on NPWT, but on skin substitute and CTP claims where the billing is just complex enough to create consistent errors at every generalist billing company.
Why Graft Billing Requires Its Own Workflow
The issue isn’t the CPT code. CPT 15271–15278 is not complicated to identify. The problem is everything that surrounds it: the Q-code selection that identifies the specific product (Q4101 for Apligraf, Q4131 for EpiFix, Q4235 for AmnioRepair), the JW/JZ modifiers that track whether product was wasted, the Field 19 documentation that requires the product name, NDC/UPC, and WAC or invoice price, and the Field 23 that must contain the authorization number — and if any of those are missing or wrong, the entire claim denies.
Beyond the claim form itself, payer policy variation creates another layer. UHC Medicare Advantage’s PCA-1-24-02596 policy subjects non-porcine skin substitutes — everything human amniotic, cellular, or fish-derived — to post-service, pre-pay clinical review. That means a claim can clear the clearinghouse, sit in UHC’s queue, and get pulled for records review 30–45 days after submission. If your billing team doesn’t know that model exists, they’re not tracking the right pipeline.
The 2026 flat national reimbursement rate of $127.14 per square centimeter for non-BLA skin substitutes also changes the product economics completely. Practices buying products at $150–$200 per cm² and getting reimbursed at $127 need a billing partner who understands cost-to-reimbursement modeling and can help guide product selection accordingly.

What to Look for in a Graft-Specific Billing Partner
The standard is specific. Before you trust any billing company with your CTP claims, ask for these four things:
- Their product Q-code matrix — a documented list of covered products, their Q-codes, payer formulary status, and porcine/non-porcine classification (this determines review tier at UHC MA)
- Their JW/JZ modifier accuracy rate — it should be ≥99%, verified through internal audits
- Their PA workflow for CTPs — does it include product formulary verification before ordering, or only after the claim is submitted?
- Their Field 19 documentation protocol — does it include lot number, NDC/UPC, and invoice data as standard practice, or only when payers request it?
If the answer to any of these is “we handle it in the billing system” without a specific protocol, that’s a gap. Our amniotic membrane graft billing guide and skin substitute billing codes resource walk through exactly what product-level graft billing requires in practice.
GRAFT TRACK — The Verified Graft Program
GRAFT TRACK is EliteMedFinancials’ dedicated graft billing program — the only structured, documented graft billing workflow built end-to-end from insurance verification through clean claim submission and post-payment audit defense. It is included as part of our wound care billing services for practices that apply skin substitutes, not sold as an add-on.
The six components GRAFT TRACK manages for every graft application: product formulary verification before ordering, PA submission with product-specific documentation, status tracking to determination, determination documentation into the billing workflow, clean claim submission with complete Field 19/23/24G compliance, and denial management with appeal support if the claim is contested.
The Only Dedicated Graft Billing Protocol in the Market
If your practice applies skin substitutes or amniotic grafts, you need more than wound care billing — you need a protocol built specifically for CTPs. GRAFT TRACK manages every step from product formulary verification through prior authorization, clean claim submission, and post-payment audit defense.
Wound Care Billing Company Near Me vs. National Remote Services
Does Location Matter for Billing Quality?
The short answer is no — and the reason is worth understanding. When providers search for a wound care billing company near me, what they’re actually looking for is responsiveness, accountability, and someone who understands their payer mix. None of those things require a physical office in your zip code.
MAC jurisdiction knowledge — the state-specific LCD compliance that determines whether your claims survive post-payment review — is a training issue, not a geography issue. A specialist billing company in another state that maintains quarterly-updated LCD matrices for all MAC jurisdictions can serve a Texas wound care practice better than a local generalist who doesn’t know the difference between Novitas L35041 and First Coast L36377.
The billing companies that actually perform well for wound care practices long-term are the ones that give you a dedicated account manager (not a shared support queue), real-time claim visibility through a dashboard you can check yourself, guaranteed ADR response times in writing, and documented workflows for the procedures you actually bill. Those are what accountability looks like in billing — and none of them require your billing company to be nearby.
What to Verify When Evaluating Any Billing Partner
Whether you’re evaluating a company down the street or one operating nationally, ask the same questions. Does their team include wound-care-certified coders (CPC or COC with wound specialty experience)? What is their guaranteed ADR response time — and is it written into the contract as an SLA? How does the account management model work — dedicated manager or rotation queue? What EHRs do they integrate with directly (NetHealth WoundExpert, ModMed, Swift Medical, Epic wound modules)?
On offshore billing: the fundamental concern is not cost — it’s ADR response logistics, payer portal access, and LCD familiarity. Offshore billing can work for high-volume basic billing. For graft-heavy wound care practices with active MA plan volume and audit exposure, the risk profile of offshore billing typically outweighs the cost savings.
Cost and Pricing Models for Wound Care Billing Services
Pricing Models Explained
Three pricing models dominate the wound care billing market:
Percentage of collections (5.4–8%): The most common model for wound care specialists. Aligns vendor incentives with practice revenue — the billing company only earns more when you collect more. For graft-heavy practices, verify that PA management, denial appeals, and ADR response are included in the base percentage rather than charged as add-ons. Some companies charge $25–$100 per PA request separately, which can add 2–3% to your effective cost.
Per-claim pricing ($8–$15 per claim): More predictable month to month. Better for lower-volume practices with stable claim counts. Downside: per-claim models can reduce billing company incentive to aggressively follow up on denied claims — they’ve already been paid for the submission.
Flat monthly retainer ($2,500–$8,000): Works well when claim volume is consistent and higher. Easier to budget. Make sure the contract specifies what’s included — some retainer models exclude denial management above a threshold or charge separately for PA work.
| Practice Size | Best Model | Typical Cost Range |
|---|---|---|
| Small (1–2 providers, low CTP) | Per-claim or flat monthly | $8–$15/claim or $2,500–$4,500/month |
| Medium (3–8 providers, moderate CTP) | Percentage of collections | 5.4–7% with PA bundled |
| Large (multi-site, high CTP) | Percentage with volume discounts + KPI incentives | 4–6% with performance floors |
The True Cost Comparison — In-House vs. Outsourced vs. Specialist
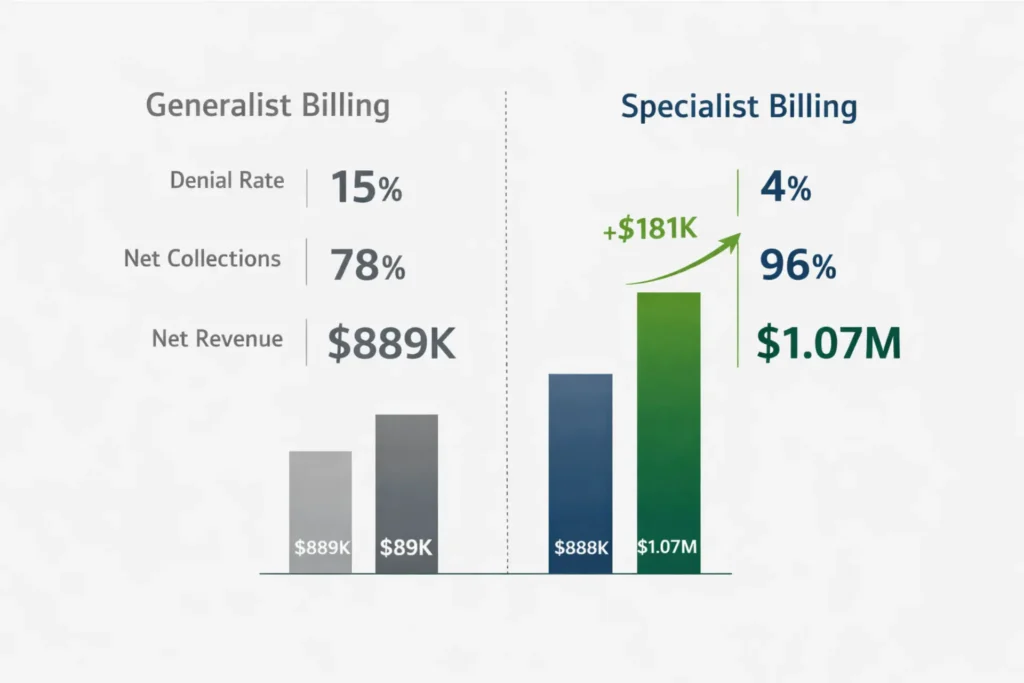
The ROI case for outsourced specialist wound care billing is straightforward. A mid-size practice with $1.2 million in annual collections managed by a generalist billing company at 5% with a 15% denial rate nets approximately $889,000 after fees and write-offs. The same practice with a specialist at 7% and a 4% denial rate nets approximately $1,071,000 — a $182,000 annual improvement, even with the higher fee.
In-house billing costs 10–15% of collections when you fully load salaries, benefits, software, training, and turnover. The number most practices use — “we only pay one person $55,000 a year” — leaves out $25,000–$35,000 in loaded costs, software licensing, and the revenue leakage from claims that never get followed up because that one person is also answering phones.
⚠️ KEY POINT: The cheapest billing company is often the most expensive mistake a wound care practice makes. Fee percentage is meaningless without denial rate data. Ask any vendor: “What is your denial rate specifically for skin substitute claims?” If they cannot answer that question, they are not tracking it — which means it’s probably not good.
For a deeper look at what outsourced billing means financially for wound care practices, our outsource wound care billing guide covers the full cost-benefit analysis with real practice scenarios.
Stop Losing Revenue to Avoidable Wound Care Denials
EliteMedFinancials delivers specialized wound care billing — from debridement coding and NPWT claims through skin substitute prior authorization, LCD compliance, MIPS reporting, and audit defense. One connected team. No generalist guesswork.
How to Make the Final Decision and Transition Smoothly
The 5-Question Evaluation Framework
Before you sign anything with any billing company — including us — get answers to these five questions in writing:
- “What is your first-pass acceptance rate for skin substitute claims specifically, based on 12-month data?” Not your overall first-pass rate. Not blended wound care. CTP claims specifically. If they cannot answer, they’re not tracking it.
- “How do you handle UHC Medicare Advantage’s post-service pre-pay review for non-porcine skin substitutes?” This question alone will identify whether the team has actual MA plan graft experience. Most billing companies don’t know the policy exists.
- “What is your ADR response time guarantee, and is it in the SLA?” 24–48 hours is the standard. More than 72 hours for a high-dollar CTP claim means revenue is at risk.
- “What is included in your base fee, and what triggers additional charges?” PA management, denial appeals, AR follow-up, and LCD monitoring should all be included. If any of those are add-ons, adjust the percentage comparison accordingly.
- “Who owns the billing data, and what is the AR transfer process if we exit?” The practice owns all data. Clean AR transfer with aging buckets by payer is non-negotiable. If the contract is vague on this, keep negotiating.
How to Transition Without Revenue Disruption
A well-managed billing company transition takes 4–8 weeks and doesn’t have to create a revenue gap. The practical steps:
- Week 0–2: Export your current AR ledger by payer and aging bucket. Document all open prior authorizations for ongoing graft treatment cycles. Request your denial history by procedure type from the outgoing vendor.
- Week 2–6: Parallel billing period — the new company processes new claims while the old vendor works existing denials per the agreed handoff. Establish the EDI and clearinghouse enrollment with your payers.
- Week 6–8+: Weekly KPI review calls. Monitor first-pass rates on early claims. Reconcile transferred AR. Establish your baseline for ongoing performance reporting.
The biggest risk during transition is not claim gaps — it’s losing track of open PA authorizations for patients mid-treatment cycle. If you have patients actively receiving graft applications, make sure the new billing company receives the full authorization history for each patient before go-live.
🔵 Compare Our Services — Free Consultation
EliteMedFinancials handles wound care billing, graft prior authorization, skin substitute coding, LCD compliance, MIPS reporting, credentialing, and practice growth services as one connected wound care program — not seven separate vendors.
We offer a structured 30-day onboarding protocol, dedicated account management, and guaranteed ADR response within 24–48 hours.
For practices also interested in provider credentialing and enrollment or medical coding services as part of a complete RCM setup, those services are available as part of our integrated RCM services platform.
Voice Search: Wound Care Billing Company Questions Answered {#voice-search}
These are the spoken questions wound care providers ask most frequently — answered directly.
Which company is best for wound care medical billing? The best wound care billing company depends on what your practice primarily bills. For high-volume skin substitute and graft programs, choose a company with documented graft billing workflows, product formulary verification, and a PA management protocol — not just a company that mentions “skin substitutes” on their website. EliteMedFinancials, AltuMED, Medheave, and Summit RCM are among the established wound-care-focused options, but only a company with a dedicated graft billing program addresses the full scope of CTP billing requirements.
How much does wound care billing cost per month? Wound care billing services typically cost 5.4–8% of net collections for a specialist company, or $2,500–$8,000 monthly on a flat retainer model for smaller practices. Per-claim pricing runs $8–$15 per submitted claim. In-house wound care billing costs 10–15% of collections when fully loaded with salaries, software, training, and turnover — making outsourced specialist billing the lower-cost option for most practices once collection rate improvements are factored in.
What is the difference between a wound care billing company and a regular billing company? A wound care billing company specializes in the CPT families, LCD compliance requirements, and payer policies specific to wound care — including debridement depth-based code selection, skin substitute Q-codes and product modifiers, NPWT and HBOT documentation requirements, and prior authorization workflows for cellular tissue products. A general medical billing company handles these as edge cases; a wound care specialist handles them daily. The difference shows up in denial rates — typically 8–12% with a specialist versus 20–35% with a generalist.
Does wound care billing require prior authorization? Yes, in 2026 approximately 40–60% of wound care procedures require prior authorization, including skin substitutes and CTPs, hyperbaric oxygen therapy, and negative pressure wound therapy for most payers. Medicare Advantage plans require pre-service authorization in most cases. UHC Medicare Advantage applies a post-service, pre-pay clinical review for non-porcine skin substitutes. Original Medicare Part B does not require front-end PA for most wound procedures, but post-payment audits through MACs and RACs function as retroactive authorization review.
How do I know if my billing company is handling skin substitute claims correctly? Request a denial rate report specific to skin substitute and CTP claims — not your blended denial rate. Ask whether they track JW/JZ modifier accuracy. Ask to see their product Q-code matrix. Request the last 90 days of first-pass acceptance data for CPT 15271–15278 claims. If they cannot provide these data points, they are not tracking graft billing at the level required to protect your revenue.
Can I switch wound care billing companies without losing revenue? Yes, with proper transition planning. A 4–8 week parallel billing period, clean AR export before departure, and EDI enrollment setup before go-live prevents the revenue gap most practices fear. The most critical step is transferring open prior authorization records for any patients actively receiving graft treatment — missing this creates mid-treatment denials on claims the old vendor never tracked. See our outsource wound care billing guide for the full transition protocol.
What credentials should a wound care billing specialist have? Wound care billing specialists should hold CPC (Certified Professional Coder) or COC (Certified Outpatient Coder) credentials through AAPC, ideally with documented experience in wound care coding specifically. CWCMS (Certified Wound Care Management Specialist) is also relevant for clinical-facing billers. More important than credentials alone is documented experience with skin substitute Q-codes, LCD compliance auditing, and prior authorization management for CTPs — credentials without workflow depth are not enough.
FAQ: Detailed Answers for Wound Care Practice Owners {#faq-section}
How is wound care billed?
Wound care is billed using CPT codes for each procedure type, matched to HCPCS/Q-codes for supply products, supported by ICD-10 diagnosis codes, and submitted via CMS-1500 or 837 electronic claims. Code selection depends on the type of wound treatment, the anatomical site, the depth of debridement, and the specific product applied. Reimbursement depends on payer-specific rules, facility vs. non-facility settings, and Local Coverage Determinations for chronic wounds and high-dollar biologics. The 2026 CMS final rules added stricter documentation requirements for skin substitute claims, including product-level documentation in CMS-1500 Field 19. See our wound care billing codes guide for the complete CPT code reference.
What CPT codes are used for wound care billing?
The primary wound care CPT code families are:
Debridement: 97597–97598 (selective) and 11042–11047 (surgical by depth)
Skin substitute application: 15271–15278 (by site and surface area)
NPWT: 97605–97606 (non-powered) and G0278/G0280 (powered)
HBOT: 99183–99184 (supervision and treatment)
E/M with procedures: 99213–99215 with modifier -25 on same-date encounters
Code selection within each family depends on anatomical site, depth of tissue involvement, and wound surface area. Our complete wound care billing codes guide covers the selection logic for each family.
What are the top denials in wound care billing?
The five most common wound care billing denial reasons in 2026 are:
Incorrect CPT selection — most often selecting 97597 (selective debridement) when documentation supports 11042 (surgical debridement), or vice versa; code selection should follow the deepest tissue layer removed
Missing or incorrect modifiers — failing to add modifier -25 when billing E/M and a procedure on the same day; incorrect use of -59 or -XS for bundled procedures
LCD documentation gaps — missing wound stage, wound duration, prior conservative treatment history, or vascular assessment required by the applicable MAC LCD
ICD-10 specificity failures — using non-specific diagnosis codes when the applicable LCD requires laterality, staging, or etiology specificity
Prior authorization errors — missing PA number in Field 23, applying a skin substitute without pre-authorization on a plan that requires it, or missing documentation to support post-service review at UHC MA
Who can bill for wound care services?
Wound care services can be billed by MDs, DOs, Nurse Practitioners (NPs), and Physician Assistants (PAs) practicing within their scope of licensure. Registered nurses can perform certain wound care procedures under physician supervision and may support incident-to billing rules when applicable. The billing credential that matters is not the clinician’s — it’s the coder’s. AAPC-certified coders with wound care coding experience, and billing staff trained on LCD compliance and graft-specific modifiers, are what determine whether claims get paid.
What is the difference between wound care billing and general medical billing?
Wound care billing is significantly more complex than general medical billing. While general billing typically handles single-family CPT codes with minimal stacking, wound care encounters combine multiple code families per visit—debridement (11042–11047, 97597–97598), E/M services with modifier -25, skin substitute applications (15271–15278), and product-specific Q-codes—all on one claim.
Wound care also requires active Local Coverage Determination (LCD) monitoring by Medicare Administrative Contractor (MAC) jurisdiction, especially for skin substitutes and HBOT. Prior authorization is required for 40–60% of advanced procedures in 2026, compared to occasional PA needs in general billing.
Denial rates tell the story: general medical billing averages 8–12%, while wound care practices using generalist billing see 20–35% denials. With a wound-care-specialist vendor, denial rates drop to 8–12%. Additionally, MIPS tracking for wound care focuses on wound-specific healing rates and 30-day follow-up metrics—far more specialized than standard quality measures.
Bottom line: Wound care billing is a distinct specialty requiring dedicated expertise in graft coding, LCD compliance, and prior authorization workflows. Treating it as “just another specialty” typically results in denial rates triple the industry average.
How long does it take to switch wound care billing companies?
A structured transition takes 4–8 weeks. Week 0–2 involves assessment and export of current AR and authorization records. Week 2–6 is the parallel billing period where the new company processes new claims while the old vendor works existing denials per the agreed protocol. Weeks 6–8+ cover first-wave KPI monitoring, AR reconciliation, and workflow optimization. Practices with active skin substitute treatment cycles should add 2 additional weeks to ensure all open prior authorizations are properly transferred to the new billing team before go-live.
What is the 2026 flat reimbursement rate for skin substitutes?
CMS implemented a flat national rate of $127.14 per square centimeter for non-BLA (Biologics License Application) skin substitutes effective with the 2026 Physician Fee Schedule Final Rule (CMS-1832-F). BLA-licensed products (Apligraf, Dermagraft) retain ASP+6% pricing. This change replaced the previous high-cost/low-cost classification structure and has significant product economics implications — practices billing products with acquisition costs above $127/cm² face an invoice-reimbursement gap that requires careful product selection management. For the full coverage and reimbursement context, see our Medicare wound care graft coverage guide.
Do wound care billing companies handle skin substitute claims?
Some do, and some do not — but more importantly, the ones that claim to handle CTPs vary enormously in how deep that expertise goes. Basic wound care billing companies will submit a CPT 15271 with a Q-code. A specialist billing company will verify product formulary coverage before ordering, manage prior authorization by payer type (including UHC MA’s post-service review model), populate Field 19 with NDC/UPC and WAC data, apply JW/JZ modifiers accurately, document lot numbers for audit traceability, and prepare audit-ready documentation for MAC review. That difference — between submitting a graft claim and protecting a graft claim — is worth examining carefully before you choose a billing partner.
Conclusion {#conclusion}
Wound care billing companies range from excellent to operationally dangerous for practices with graft volume, and the financial gap between choosing right and choosing wrong compounds every week. The evaluation framework in this guide gives you the specific questions to ask, the benchmarks to demand, and the red flags to reject — so you’re comparing actual performance data, not marketing promises. If your practice applies skin substitutes or amniotic grafts, your billing choice is not just an administrative decision. It’s a revenue protection decision that affects clinical program viability.
🔵 Ready to Replace a Generalist Billing Company With a Wound Care Specialist?
EliteMedFinancials delivers wound care billing, graft prior authorization, skin substitute coding, LCD compliance, MIPS reporting, and provider credentialing as one integrated wound care program.
We offer a structured transition protocol, dedicated account management, guaranteed 24–48 hour ADR response, and the only dedicated GRAFT TRACK verified graft billing program in the market.
🟢 Already Getting Graft Claim Denials?
Skin substitute and CTP denials are recoverable — but only if the appeal addresses the specific denial reason with targeted documentation. Our denial management team reviews your denied graft claims, identifies the root cause, rebuilds the appeal package, and manages every level of the appeal process.
Quick Reference Table — Wound Care Billing Companies 2026
| Topic | Reference |
|---|---|
| Core wound CPT families | 97597–97598, 11042–11047, 15271–15278, 97605–97606, 99183–99184 |
| Common CTP Q-codes | Q4101 (Apligraf) · Q4131 (EpiFix) · Q4235 (AmnioRepair) · Q4102 (Oasis) |
| Required modifiers | JC (graft used) · JW (wastage) · JZ (zero waste) · -25 (E/M same day) · -59/-XS (distinct procedure) |
| Key MAC LCDs | L36690 (CGS/KY-OH) · L35041 (Novitas) · L36377 (First Coast) |
| 2026 flat CTP rate | $127.14/cm² (non-BLA products) |
| UHC MA policy | PCA-1-24-02596 (non-porcine post-service review) |
| Target first-pass rate | 85–95% (specialist-managed) |
| Target net collection rate | 88–92% |
| Target denial rate | <12% (specialist); <25% (CTP-specific acceptable range) |
| Pricing range | 5.4–8% of collections (specialist); $2,500–$8,000/month (flat) |
| Standard PA turnaround | 3–5 business days (routine); 24–72 hours (urgent) |
External Resources:
- CMS Local Coverage Determination Database — Search current LCD policies by MAC jurisdiction for skin substitute coverage criteria
- AMA Prior Authorization Survey 2024 — Data on PA administrative burden, physician time costs, and patient care impact