Skin substitute graft claims sit at the highest-risk intersection in Medicare Part B billing. The reimbursement potential is real. So is the exposure. A single wound graft claim can represent thousands of dollars — and that same claim, submitted without proper wound graft claim verification, can come back as a recoupment demand years after you thought you were paid.
Most practices find out about their verification gaps the wrong way: an Additional Documentation Request from a Recovery Audit Contractor, a payment suspension on all current claims, or a $400,000 overpayment letter covering services from two years ago. By that point, the conversation is no longer about good clinical care. It is about whether your documentation can survive a clinical judgment audit by someone who was not in the room.
That is the problem this process solves.
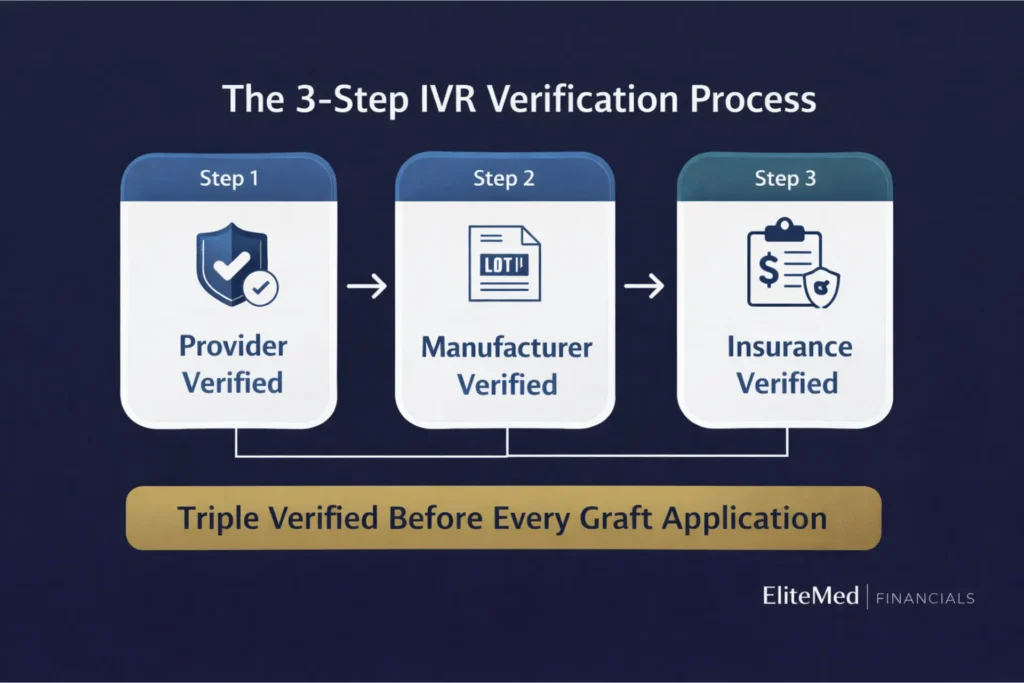
At EliteMed Financials, we run every wound graft claim through what we call the IVR Verification Process — three independent checks before a single graft is applied: Provider Verified, Manufacturer Verified, and Insurance Verified. This is what makes our program a triple verified wound care graft program. Not triple-checked at billing. Triple-verified before the procedure.
If you are applying skin substitute grafts and your current workflow does not confirm all three of these elements in advance, you are carrying audit risk you probably cannot see yet. This guide explains exactly what each step checks, why each one exists, and what happens to practices that skip them.
Wound Graft Audit Risk & Revenue Impact Calculator
Estimate your annual denial exposure and potential RAC audit liability based on your current graft billing volume and verification gaps.
Your Estimated Risk Profile
High RiskRisk Factor Breakdown
Schedule a free wound care billing review with our team. We will identify your actual gaps and show you exactly how the IVR verification process closes them.
This calculator provides estimates for educational purposes only. Actual denial rates, reimbursement values, and audit exposure vary by practice, payer mix, documentation quality, and MAC jurisdiction. The 2026 flat rate of $127/cm² is based on CMS CY 2026 PFS final rule. Consult an EliteMed billing specialist for a practice-specific assessment.
Table of Contents
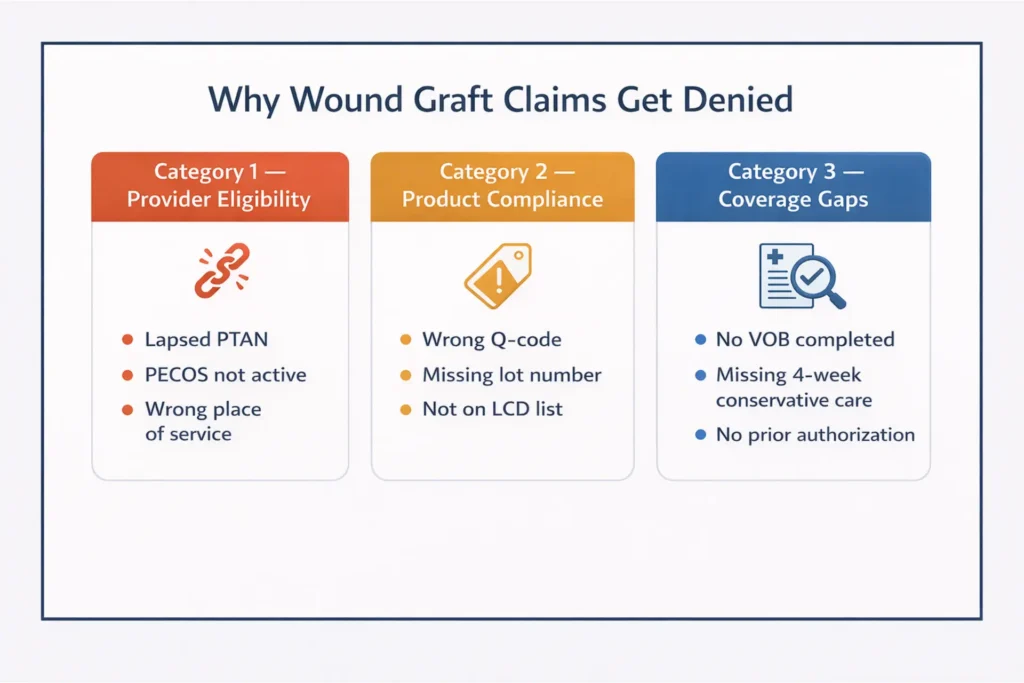
Why Wound Graft Claims Fail: The 3 Categories of Denial
There is a common misconception that wound graft denials are primarily clinical — that if the care was medically appropriate, the claim should pay. That is not how Medicare works. CMS and its contractors deny claims across three separate tracks, and most providers only think about one of them.
Category 1: Provider Eligibility Failures
This is the track that catches practices off guard because it has nothing to do with the wound or the product. It is entirely administrative.
If your performing provider is not actively enrolled in Medicare's PECOS system — Provider Enrollment, Chain, and Ownership System — at the time of service, the claim fails. Not on appeal. Not with additional documentation. It fails because Medicare does not recognize the provider as authorized to bill.
The PTAN, or Provider Transaction Access Number, is what Medicare uses to confirm that authorization. A lapsed PTAN means a denied claim. A PTAN linked to a different practice location than where the service was delivered means a denied claim. A supervising provider whose revalidation lapsed six months ago means the same thing.
CMS can — and does — recoup 100% of payments made under a non-enrolled provider. That exposure does not disappear when you correct the enrollment issue. The recoupment applies to every claim filed during the gap.
This is not theoretical. Ownership changes, group practice restructuring, and multi-location expansion all create enrollment gaps that billing teams do not catch in real time. By the time a UPIC (Unified Program Integrity Contractor) or RAC (Recovery Audit Contractor) runs a provider eligibility check against historical claims, the gap has already produced a liability.
Category 2: Product Compliance Failures
This is where the clinical confidence of most wound care providers creates a blind spot. You know the product works. You know you applied it correctly. But Medicare does not pay for products — it pays for correctly coded and documented products.
Every skin substitute graft product billed to Medicare requires an assigned HCPCS Q-code. That Q-code is not interchangeable. Q4101 is not Q4106. The Q-code must match the specific product's FDA classification and appear on your MAC's approved LCD product list.
When those three elements — product, Q-code, and LCD list — do not align, the denial is automatic. CMS Billing and Coding Article A57680 sets additional documentation requirements that most practices underestimate: the procedure note must include the exact product name, the manufacturer, the amount used, the amount discarded, the reason for any wastage, and the manufacturer's lot number or serial number.
Missing a lot number is not a technicality. In a post-payment audit, a missing lot number is treated as an unverifiable claim. The auditor cannot confirm the product existed, came from an authorized source, or was stored and handled correctly. That uncertainty resolves against the provider.
Category 3: Coverage Gaps
The third failure track is the one providers most often think they have covered — and most often don't.
A patient having active Medicare Part B does not mean the specific graft you want to apply is covered. Medicare covers skin substitute grafts under Local Coverage Determinations (LCDs) issued by Medicare Administrative Contractors (MACs). Those LCDs specify covered wound types, required documentation, frequency limits, and the list of approved products for each jurisdiction.
For traditional Medicare, prior authorization is not required — but that creates a false sense of security. Medicare pays first and audits later. If the claim does not meet LCD criteria, the money comes back. For Medicare Advantage plans, the problem surfaces differently: UHC, Humana, and Aetna require prior authorization before the procedure. Without it, there is no appeal on medical necessity grounds. The claim is simply not covered.
The four-week conservative care requirement sits in this category. Before a skin substitute graft is applied to a diabetic foot ulcer or venous leg ulcer, Medicare requires documented evidence that standard wound care — debridement, dressings, offloading, compression — was attempted and failed over a minimum of four weeks. A general note that "wound failed to heal with standard care" does not satisfy the requirement. A UPIC reviewing claims from three years ago will not give you the benefit of the doubt.
Tired of Wound Graft Claim Denials?
We Handle the Entire Billing Cycle.
From conservative care documentation to prior authorization, Q-code verification to six-year audit defense — our CPC-certified wound care billing team manages every step so you focus on patient care, not paperwork.
Step 1: Provider Verified — Confirming Your Eligibility Before a Single Claim Is Filed
Before we process a single graft claim, we confirm that the provider billing the service can legally bill it.
We run every provider through a full PECOS enrollment check. Not a quick NPI lookup — a cross-reference of the provider's NPI, TIN, PTAN, specialty taxonomy code, and practice location against Medicare's current enrollment database. We confirm active enrollment status, not just that an enrollment record exists.
The NPI Registry (NPPES) and PECOS are not the same system. A provider can appear in the NPI Registry — visible and searchable — while having a lapsed or inactive PECOS enrollment. That distinction trips up more practices than almost any other administrative error in wound care billing.
We also verify:
- Place of service alignment. Office billing (POS 11), wound care center (POS 22), and home-based service (POS 12) each carry different enrollment and supervision requirements. A mobile wound care provider billing under POS 12 without the correct enrollment structure faces automatic denials and retroactive exposure.
- Rendering versus supervising provider linkage. For incident-to services — where an NPP is delivering care under physician supervision — we confirm the supervising physician is enrolled, active, and physically present as required. An enrolled NPP under an unenrolled or opted-out supervising physician is a complete claim failure.
- OIG LEIE and SAM.gov exclusion screening. No matter how long a provider has been in practice, we run current exclusion list checks at enrollment and on a recurring basis. One excluded provider on your billing team can expose every claim they touched to recoupment under the False Claims Act.
- Revalidation deadlines. CMS requires Medicare providers to revalidate every five years, or sooner if triggered by a change in ownership or practice location. We track revalidation windows and flag approaching deadlines before they create a billing gap.
For practices transitioning to a new wound care program or adding a new location, we begin the enrollment confirmation before the first patient is scheduled. If you are currently applying grafts and have not confirmed active PECOS enrollment at each practice location where those claims are being filed, that is the first thing to fix.
Our credentialing and provider enrollment services handle the full Medicare enrollment process.
Step 2: Manufacturer Verified — NovaMed FDA Documentation, Q-Code Pre-Loading, and Chain of Custody
Product compliance is where most billing companies stop at documentation review. We go further upstream — to the point where the product is ordered.
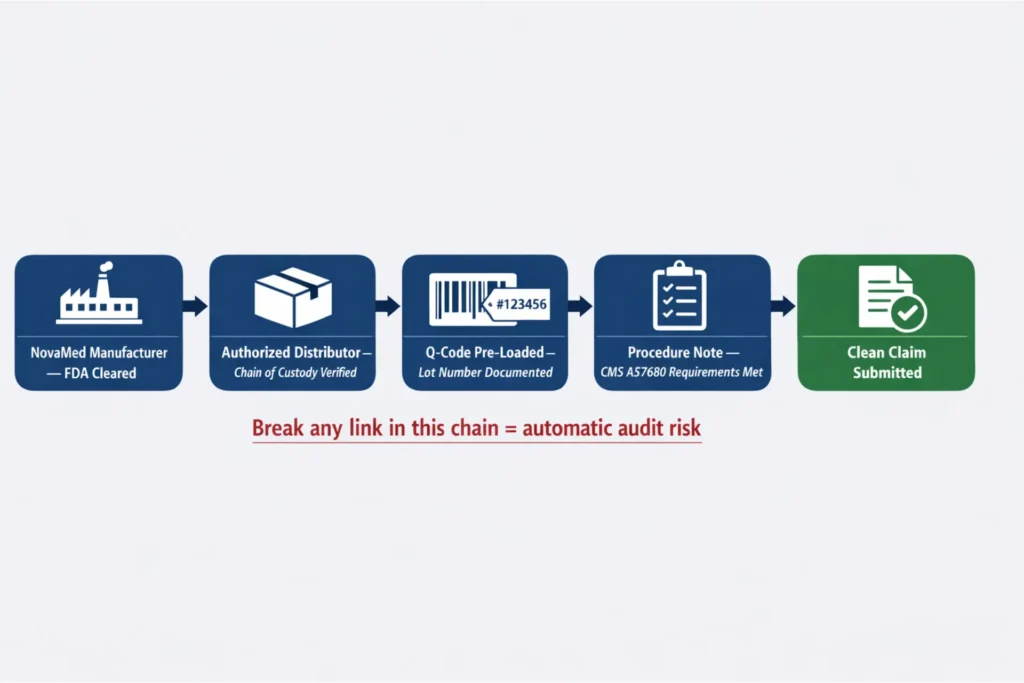
EliteMed works exclusively with NovaMed-authorized graft products, including DermaBind. Every product in our program enters the billing workflow with its Q-code pre-loaded — meaning the HCPCS code is confirmed and locked before the product ships to the practice. We do not assign Q-codes at billing time based on a lookup. The code is established from the product's FDA classification and its current status on the applicable MAC's LCD-approved product list.
This matters because Q-code assignments change. Products are added to and removed from MAC positive lists on an annual HCPCS update cycle. A product that was covered under your jurisdiction's LCD in January may not be listed by July. Without a real-time verification step at the product level, you may apply a graft that your billing team will code to a valid-looking Q-code that is no longer on the covered list for your MAC.
Why This Matters for Claims Protection
CMS Billing and Coding Article A57680 is the controlling document for skin substitute graft documentation requirements. It is specific about what the procedure note must contain for every graft application.
At a minimum, per A57680, the note must include: the product's exact name and manufacturer, size applied in square centimeters, amount used, amount discarded, the reason for any wastage, and the manufacturer's serial number, lot number, or batch number. Every element of that list has a corresponding denial or audit trigger when it is missing or inaccurate.
We address this at the product delivery stage. When NovaMed ships a product to our partner practice, the delivery record includes the lot number, expiration date, and storage confirmation. That documentation is embedded in the claim file before the provider writes a word of the procedure note. The lot number requirement is already satisfied.
Chain of custody means something specific here. An auditor asking about chain of custody is not asking a philosophical question about supply chain ethics — they want to see the shipping manifest, the receiver signature, the storage temperature logs if required, and confirmation that the product came from an FDA-registered, authorized distributor. Gray market sourcing — products obtained outside the direct manufacturer distribution chain — creates a documentation gap that auditors treat as a potential fraud indicator, regardless of the clinical quality of the care.
NovaMed Product Compliance Snapshot
Format this as a table block in WordPress. Column headers: Compliance Element | Requirement Source | EliteMed Program Status
| Compliance Element | Requirement Source | EliteMed Program Status |
| FDA clearance (510k / HCT/P / PMA) | CMS LCD coverage requirement | ✅ Pre-verified at product enrollment |
| HCPCS Q-code assignment | CMS HCPCS Workgroup / Annual update | ✅ Pre-loaded at point of shipment |
| Lot number documentation | CMS A57680 procedure note requirement | ✅ Embedded in delivery record |
| Authorized distributor chain | CMS supplier standards / FCA exposure | ✅ Verified at program enrollment |
| Wastage documentation template | CMS A57680 wastage reporting requirement | ✅ Provided with every product delivery |
| LCD approved product list status | MAC-specific positive list | ✅ Confirmed per jurisdiction before ordering |
| NDC to Q-code reconciliation | IOCE (Integrated Outpatient Code Editor) | ✅ Validated before claim submission |
See our full wound care graft program and authorized product details
The Only Triple-Verified Wound Graft Program
Provider verified. Manufacturer verified. Insurance verified — before a single graft is applied. Six years of claims protection built into every file we submit.
Enroll Once. Bill With Confidence Every Time.
- NovaMed / DermaBind authorized product access
- Q-codes pre-loaded at shipment — no billing guesswork
- Full VOB + LCD confirmation before every procedure
- 6-year documentation retention — audit-ready in 48 hours
- CPC-certified coding on every graft claim
No long-term contracts. Enrollment typically complete in 5–7 business days.
Step 3: Insurance Verified — Payer-Specific Eligibility, LCD Confirmation, and Prior Auth Status
Provider is confirmed. Product is confirmed. Now we confirm that the specific graft, applied to this specific wound, in this specific patient, will be covered by this specific payer under their current policy.
This is not a standard eligibility check. Every billing system can confirm that a patient has active Medicare Part B. That takes thirty seconds and tells you almost nothing useful about graft coverage. What matters is the next layer: which MAC jurisdiction covers this patient, which LCD policy governs graft coverage in that jurisdiction, whether the patient's wound type qualifies under that LCD, and whether this specific product is on that MAC's approved product list.
Those are four separate questions. Most pre-service workflows answer zero of them.
The Verification of Benefits Checklist We Run Every Time
Format as a checklist block or ordered list in WordPress.
- Patient Medicare Part B active status — confirmed, not assumed
- Primary payer determination — confirm Medicare is primary, not secondary to a working-aged group plan
- MAC jurisdiction identification — determines which LCD policy applies
- Wound type eligibility — DFU (ICD-10 L97.-), VLU (ICD-10 I83.0-, I87.2), pressure ulcer (L89.-), or other qualifying chronic wound
- Conservative care documentation — minimum 4 weeks of dated interventions with wound measurements
- Product on LCD-approved list — Q-code confirmed against MAC's current Group 1 covered product list
- Application count in current episode — confirm within frequency limits (varies by MAC)
- Wound improvement check — for 4th application and beyond, document 20–50% size reduction per LCD requirement
- Vascular status — ABI or TBI within 12 months (required for DFU patients in most LCD policies)
- Prior authorization — obtained for Medicare Advantage, UHC, Humana, Aetna, Cigna MA plans before scheduling
- ABN issued — when coverage is uncertain, Advanced Beneficiary Notice issued to patient before service
- Financial margin check — graft cost confirmed against 2026 flat-rate reimbursement of approximately $127/cm² before product is ordered
Why Payer Rules Vary — and Why That Matters
This is the piece most multi-state wound care practices underestimate. Your LCD policy is not national. It is issued by your MAC, and the rules differ — sometimes dramatically — between jurisdictions.
Novitas Solutions, under LCD L35041, limits applications to 2 per product within a 12-week period. National Government Services, under LCD L35125, allows between 4 and 8 applications per wound per year — but requires documented wound improvement after the 4th application. Miss that documentation requirement, and applications 5 through 8 are denied as over-utilization, even within the stated limit.
For Medicare Advantage plans, the workflow is fundamentally different. Traditional Medicare operates on a pay-and-audit model — they pay the claim, then audit it later. Medicare Advantage denies upfront without prior authorization. There is no path to medical necessity appeal if you did not get the PA before the procedure. United Healthcare, Humana, Aetna, and Cigna each maintain separate formulary lists for covered skin substitute products under their MA plans. A product covered by traditional Medicare Part B may not be covered under a specific MA plan at all.
Failing to confirm these payer-specific rules before application is not a billing problem. It is a revenue problem — and sometimes a compliance problem if you are billing for a service you did not have a legitimate expectation of being paid for.
MAC LCD Comparison Table — format as a table block in WordPress.
| MAC Name | LCD Policy | Max Applications | Key Requirement | Unique Restriction |
| Novitas Solutions | L35041 | 2 per product / 12 weeks | Conservative care 4+ weeks | Product-specific limit |
| NGS | L35125 | 4–8 per wound / year | Progress proof after 4th app | Denial after 8 without improvement |
| Noridian | Varies by state | 4–8 per wound / year | Clinical response dependent | >4 apps requires documented progress |
Read our wound care graft Medicare coverage guide — full LCD breakdown by MAC jurisdiction
Prior authorization guide for wound grafts
The 6-Year Claims Protection: What It Covers and How It Works
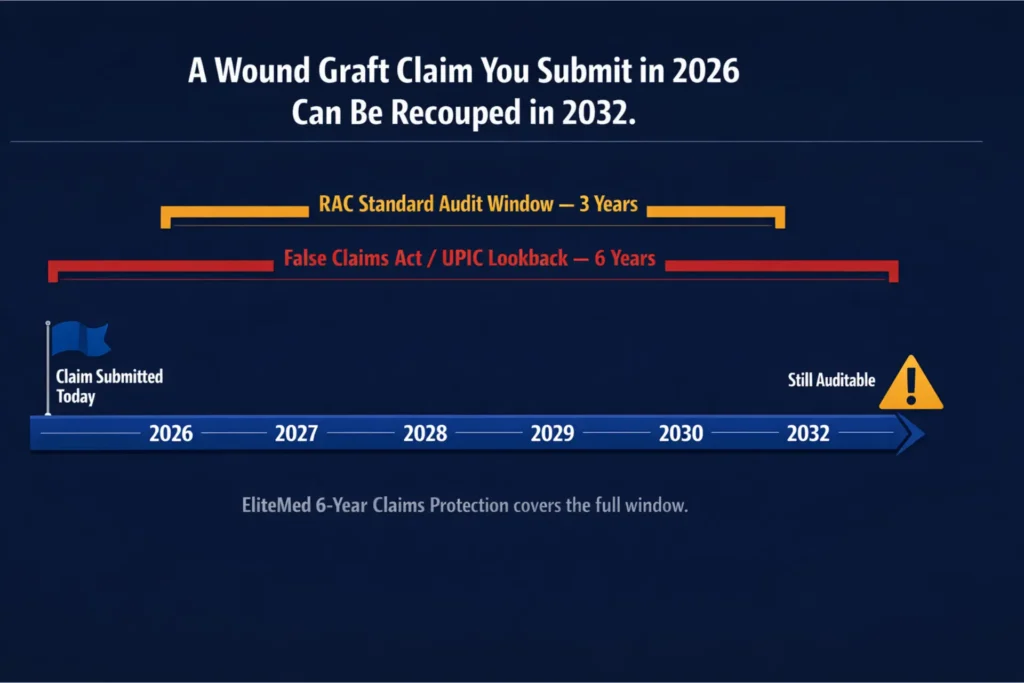
Here is the part of wound graft billing that most practices do not think about until it is too late.
Medicare's standard audit lookback under the False Claims Act extends six years — meaning a wound graft claim you submit today can be audited, reviewed, and recouped in 2032. Recovery Audit Contractors typically operate on a three-year lookback for routine overpayment reviews. UPICs, which handle program integrity investigations, and DOJ-referred FCA cases use the full six-year window. In fraud investigations, that window extends to ten years.
That is not hypothetical exposure. RAC and UPIC audit activity on skin substitute graft claims has intensified significantly in recent years, driven by the rapid growth in Medicare spending on cellular and tissue-based products and the well-documented history of overutilization patterns in this specialty.
Our wound graft billing protection covers the full exposure window. Every claim submitted through the EliteMed program is maintained with a complete documentation file — not just the claim data, but the provider eligibility snapshot at the time of service, the product delivery record with lot numbers, the VOB results, the prior authorization record, the wound measurements, and the conservative care log. For six years. Available for audit response within 48 hours.
Real-World Scenarios This Protection Covers
| SCENARIO 1 — The Mid-Point Trap: RAC Audit in 2029 Reviewing 2026 Claims A mobile wound care practice billed eight skin substitute applications for a diabetic foot ulcer patient in 2026. In 2029, a RAC issues an Additional Documentation Request (ADR) for all eight claims. The practice provides wound measurements for the first four applications showing appropriate improvement. But it cannot locate the clinical notes for applications five through eight — the EMR was migrated when they joined a larger health system, and some records did not transfer cleanly. The RAC recoups 100% of applications five through eight. Then it extrapolates across every similar patient from 2026, applying the same error rate across the sample. The demand letter arrives for $450,000. A complete six-year documentation file would have made that outcome impossible. |
| SCENARIO 2 — The Missing Lot Number: UPIC Investigation in 2030 Reviewing 2024 Claims A wound clinic was acquired by a larger health system in 2028. In 2030, a UPIC reviews graft wastage patterns from 2024. The original EMR was not fully migrated — detailed procedure notes and supplier invoices did not transfer. For a $3,200 graft claim from 2024, the clinic cannot produce the lot number or invoice confirming the product came from an authorized distributor. The UPIC deems the claim unverifiable. It then expands the review to 200 similar claims using statistical extrapolation. A claim that started as a $3,200 question becomes a six-figure exposure. |
| SCENARIO 3 — The Conservative Care Extrapolation: UPIC Reviewing 2022–2024 Claims A podiatry practice routinely applied grafts at or near the first visit for chronic venous leg ulcers without documenting four weeks of failed compression therapy. In 2028, a UPIC reviews a sample of 2022–2024 claims, finds zero compliance with the conservative care requirement, and uses statistical sampling to extrapolate across the practice's full graft claim history. The demand: $2.7 million. The outcome: practice closure. The conservative care documentation was never there to begin with. But the liability built silently for years before the UPIC found it. |
Denial management and audit response services for wound care practices
Wound care RCM services overview
How the Process Works in Practice: From Enrollment to First Application
The three-step IVR process is not a theoretical framework. It is a specific workflow with a specific timeline.
- Enrollment Call (Day 1) — You speak with an EliteMed wound care billing specialist. We collect your NPI, PTAN, TIN, taxonomy codes, practice addresses, and places of service. We also identify which MAC jurisdictions apply to your patient population so we can pull the correct LCD policies.
- Provider Verification (Days 1–3) — We run the full PECOS cross-reference, OIG exclusion screening, revalidation deadline check, and place-of-service enrollment verification. If there are gaps, we identify them immediately and begin remediation. No claim is processed through our system until the provider eligibility check is clean.
- Patient Identification and VOB (Before First Graft) — When you identify a patient for skin substitute grafting, you refer that patient to our team before scheduling the procedure. We run the full VOB and LCD confirmation — wound type, conservative care documentation period, product selection, payer-specific coverage, and prior authorization if required. You receive a clear recommendation: covered as planned, covered with modifications, or not recommended to proceed.
- Product Assignment (Before First Graft) — We confirm the correct NovaMed product for the wound type and jurisdiction. The Q-code is pre-loaded, the delivery documentation is prepared, and the product ships with a complete chain-of-custody record.
- Prior Authorization (If Required) — For Medicare Advantage and commercial payers requiring PA, we handle the submission and follow-up before the procedure date. We document the authorization number in the claim file.
- Claim Submission (Within 24–48 Hours of Service) — We submit the claim with the complete documentation package assembled and cross-validated before submission. Claim scrubbing catches coding mismatches before they reach the payer. No chasing documentation after the fact.
- Six-Year File Maintenance (Ongoing) — Every claim submitted through our program is maintained in a complete, audit-ready file for the full six-year lookback window. When you get an ADR, we respond within 48 hours with a complete documentation package.
For established providers with current credentialing, the typical timeline from enrollment call to first clean claim submission is five to seven business days.
Full revenue cycle management process for wound care practices
Medical billing services for small practices
A Word on Coding Accuracy — Because This Is Where Claims Quietly Bleed
No verification process is complete without coding precision. CPT 15271 covers graft application to the trunk, arms, or legs for the first 100 square centimeters. CPT 15275 covers the face, hands, feet, genitalia, and other specified anatomical sites. Billing 15271 for a diabetic foot ulcer instead of 15275 is not a minor error — it generates an automatic denial because the CPT code's anatomical descriptor does not match the wound location.
The KX modifier is required when applying the fourth or subsequent graft in a 12-week period to attest that LCD criteria continue to be met. Omitting it on claims that require it triggers a claim-level rejection.
JW and JZ modifiers govern wastage reporting. JW is used when a portion of a single-use product is discarded. JZ is used when the full dose is administered with no waste. Since 2023, CMS requires one or the other on every applicable biological product claim. Missing both means the claim fails the Integrated Outpatient Code Editor (IOCE) check.
These are not obscure details. They are the most common technical denial triggers on wound graft claims — and they are all preventable with a proper pre-submission coding review.
Medical coding services for wound care providers
Wound care billing codes — complete reference guide
Amniotic membrane graft billing — CPT codes and Q-codes
What People Most Often Ask About Wound Graft Claim Verification
How do I verify a wound graft claim before submitting it to Medicare?
Wound graft claim verification involves three separate checks before submission: confirming the provider is actively enrolled in PECOS with a current PTAN, confirming the product's Q-code matches the FDA-cleared product on the MAC's LCD-approved list with full lot number documentation, and confirming the patient's payer will cover the specific graft under the applicable LCD policy — including conservative care documentation, wound type eligibility, and prior authorization if the plan requires it.
What is the 4-week rule for wound care billing?
Medicare requires documentation that standard wound care — debridement, dressings, offloading for diabetic foot ulcers, or compression therapy for venous leg ulcers — was attempted and failed over a minimum of four consecutive weeks before a skin substitute graft is applied. The documentation must include specific dates, interventions performed, and wound measurements at each visit. A general statement that the wound failed conservative care is not sufficient.
Why did my wound graft claim get denied by Medicare?
Wound graft claims are denied for three primary reasons: the provider was not properly enrolled or the PTAN was inactive at the time of service; the product's Q-code did not match the FDA-cleared product or the product was not on the MAC's LCD-approved product list; or the clinical documentation did not demonstrate that the patient met the coverage criteria under the applicable Local Coverage Determination — including the four-week conservative care requirement and wound type eligibility.
How far back can Medicare audit wound graft claims?
Under the False Claims Act, Medicare's lookback period extends six years for standard overpayment reviews. Recovery Audit Contractors typically operate on a three-year window for routine audits. Unified Program Integrity Contractors and DOJ-referred fraud investigations use the full six-year window, and in cases involving the False Claims Act, that period can extend to ten years. Claims from 2025 and 2026 remain eligible for audit through 2031 and 2032 respectively.
Do I need prior authorization for a wound graft under Medicare?
Traditional Medicare Part B does not require prior authorization for skin substitute graft procedures — but it operates on a pay-and-audit model, meaning it pays the claim and reviews it later. Medicare Advantage plans, including most UHC, Humana, Aetna, and Cigna MA plans, require prior authorization before the procedure. Without it, there is no appeal available on medical necessity grounds.
How many wound graft applications does Medicare cover per wound?
Application limits vary by MAC jurisdiction and applicable LCD. Novitas Solutions under LCD L35041 limits applications to 2 per product within a 12-week period. National Government Services under LCD L35125 allows between 4 and 8 applications per wound per year, but requires documented wound improvement — typically 20 to 50 percent size reduction — after the fourth application. Exceeding frequency limits without documented wound progress is a top audit trigger.
What Q-codes are used for wound graft billing?
HCPCS Q-codes for skin substitute grafts are assigned by CMS based on each product's FDA classification and tissue type. Common codes fall within the Q4100 through Q41XX series. The correct Q-code for each product must be confirmed against the current HCPCS annual update and the MAC's LCD-approved product list for the relevant jurisdiction. Using an incorrect Q-code — even if the product itself is covered — results in automatic claim denial.
Full wound care billing Q&A and frequently asked questions
Outpatient wound care billing guide
Frequently Asked Questions About Wound Graft Claim Verification
What is wound graft claim verification, and why do I need a formal process for it?
Wound graft claim verification is the pre-billing process of confirming three things before a skin substitute is applied: that the provider is enrolled and eligible to bill, that the product has the correct Q-code and documentation to meet CMS requirements, and that the patient's specific payer will cover the procedure under the applicable LCD policy. Without a structured process, any one of these checks can fail — and you often do not find out until a RAC or UPIC issues an audit demand, sometimes years after the claim was paid.
What is PECOS and why does it matter for wound graft billing?
PECOS — the Provider Enrollment, Chain, and Ownership System — is the Medicare database that confirms whether a provider is authorized to bill Medicare. A provider can have an active NPI in the NPPES registry and still have an inactive or lapsed PECOS enrollment. Medicare does not pay claims filed under a provider who was not enrolled in PECOS at the time of service, and it can recoup all payments made during the enrollment gap. For wound care practices billing skin substitute grafts, PECOS status must be confirmed at every practice location before any claim is submitted.
What documentation does CMS require in the procedure note for every graft application?
Per CMS Billing and Coding Article A57680, the procedure note for each graft application must include: the exact name and manufacturer of the product, the size applied in square centimeters, the amount used and the amount discarded, the reason for any wastage, and the manufacturer's serial number, lot number, or batch number. The HCPCS Q-code billed must be consistent with the product and wound size documented in the note. Missing any element — especially the lot number — is treated as an incomplete claim in post-payment audit.
What is the difference between CPT 15271 and CPT 15275 for wound graft billing?
CPT 15271 covers skin substitute graft application to the trunk, arms, and legs for the first 100 square centimeters. CPT 15275 covers application to the face, hands, feet, and genitalia for the first 25 square centimeters. Billing 15271 for a diabetic foot ulcer — which is located on the foot — instead of 15275 is a location-based coding error that generates an automatic denial. The anatomical site descriptor in the CPT code must match the wound location documented in the procedure note.
How does the 2026 Medicare flat-rate reimbursement change affect wound graft billing?
Starting January 1, 2026, CMS implemented the CY 2026 Physician Fee Schedule final rule, reclassifying most skin substitute products from separately payable biologics to incident-to supplies reimbursed at a flat national rate of approximately $127 per square centimeter. Practices must now confirm that the purchase cost of the specific product does not exceed the flat-rate reimbursement before ordering — and that the product remains on the MAC's covered product list under the new classification.
What happens if my wound graft claim is audited and I cannot produce the documentation?
If you cannot produce the required documentation in response to an Additional Documentation Request (ADR), Medicare treats the claim as not supported and recoups the payment. ADR response windows are typically 20 to 45 days depending on the contractor. Missing the deadline has the same result as failing to produce the documentation. For claims reviewed by a UPIC, insufficient documentation can trigger extrapolation — the auditor projects the error rate across your full population of similar claims. The appeal process starts at Level 1 redetermination and runs through five levels, up to Federal District Court.
Can EliteMed Financials handle wound graft billing for a mobile wound care practice?
Yes. Mobile wound care billing carries specific enrollment requirements that differ from clinic-based practices — including place-of-service code validation (POS 12 for home-based services), supervision structure confirmation, and in some cases DMEPOS accreditation requirements for mobile suppliers. Our provider verification step addresses all of these. Mobile practices also face higher audit risk due to limited contemporaneous documentation opportunities, which is why our six-year file maintenance program is particularly valuable for mobile operations.
Conclusion — What Triple Verification Actually Buys You
The revenue risk in wound graft billing does not come from applying grafts that do not work. It comes from billing for grafts without confirmation that all three eligibility conditions were met before the procedure — provider, product, and payer coverage.
Triple verification does not slow down your wound care program. Practices that run through the IVR process before the first graft application submit cleaner claims, face fewer denials, and carry a defensible documentation file that survives audit review years later. The practices that skip verification — that assume provider enrollment is fine, that trust the product rep on Q-codes, that rely on standard eligibility checks for payer confirmation — are the ones getting ADR letters and payment suspension notices.
The financial exposure in wound care graft billing is long-tail. You can build liability quietly for years before it surfaces. The six-year claims protection in our program is not a bonus feature — it is what makes the entire approach defensible when a RAC or UPIC eventually looks.
If you are currently submitting wound graft claims without a formal three-step verification process, the question is not whether you have exposure. It is how much, and when you will find out.
Read our complete Medicare wound care billing guide
Revenue cycle management process overview

Enroll in the Only Triple-Verified Wound Graft Program
If you are applying skin substitute grafts and your current billing workflow does not run all three verification checks before the procedure, you are carrying risk that compounds with every claim you submit.
The EliteMed triple verified wound care graft program runs provider verification, manufacturer verification, and insurance verification before a single graft is applied. Every claim goes out with a complete documentation package. Every file is maintained for six years. When the audit comes — and for high-utilization graft programs, it usually does — you respond with everything the auditor needs in 48 hours.
This is wound graft billing protection built into the workflow, not bolted on after the denial.
The Only Triple-Verified Wound Graft Program
Provider verified. Manufacturer verified. Insurance verified — before a single graft is applied. Six years of claims protection built into every file we submit.
Enroll Once. Bill With Confidence Every Time.
- NovaMed / DermaBind authorized product access
- Q-codes pre-loaded at shipment — no billing guesswork
- Full VOB + LCD confirmation before every procedure
- 6-year documentation retention — audit-ready in 48 hours
- CPC-certified coding on every graft claim
No long-term contracts. Enrollment typically complete in 5–7 business days.