
Introduction: Why NEMT Audit Preparation Is Critical for Your Business Survival
Picture this scenario: You’ve spent years building your non-emergency medical transportation business. Your drivers are reliable, patients trust your service, and revenue has grown steadily. Then a letter arrives from your state Medicaid agency. It’s an audit notice—and suddenly everything you’ve built hangs in the balance.
This isn’t hypothetical. The 2022 OIG audit of New York’s NEMT program uncovered $196 million in improper payments, with a staggering 72% of audited claims found non-compliant. Most of these failures stemmed not from intentional fraud, but from documentation gaps that providers never knew existed until auditors came knocking.
Here’s what makes 2026 different from previous years: Federal and state agencies have shifted from reactive enforcement to proactive, AI-powered surveillance. CMS now employs sophisticated algorithms that flag billing anomalies in real-time, transforming “audit readiness” from an annual checklist into a continuous operational requirement.
The financial stakes couldn’t be higher. A single failed audit can trigger:
- Extrapolated recoupments often exceeding six figures
- Immediate contract terminations with brokers like ModivCare, MTM, and Veyo
- OIG exclusion from all federal healthcare programs
- False Claims Act violations carrying treble damages and potential criminal prosecution
But here’s the opportunity within this challenge: providers who master audit preparation don’t just survive—they thrive. Companies with robust NEMT compliance programs report 70% fewer major audit findings and 85% lower recoupment amounts compared to reactive competitors.
This guide delivers the actionable framework you need. Whether you’re a startup wondering if NEMT is a profitable business or an established provider seeking to strengthen your compliance posture, you’ll find specific checklists, regulatory citations, and prevention strategies that transform audit preparation from a burden into your competitive advantage.
What Is an NEMT Audit? Types, Triggers, and What Auditors Examine
Understanding the Fundamentals
An NEMT audit is a formal examination of your transportation operations designed to verify compliance with Medicaid regulations, state requirements, and contractual obligations. But auditors don’t simply review paperwork—they forensically reconstruct your service delivery by cross-referencing documentation, GPS data, billing claims, and operational records.
The 2026 audit environment has evolved significantly. CMS eliminated numerical scoring in favor of “Corrective Action Required” (CAR) classifications, emphasizing systemic improvement over punitive measures. However, this shift actually increases scrutiny because auditors now examine your root cause analysis and continuous improvement processes rather than just checking boxes.
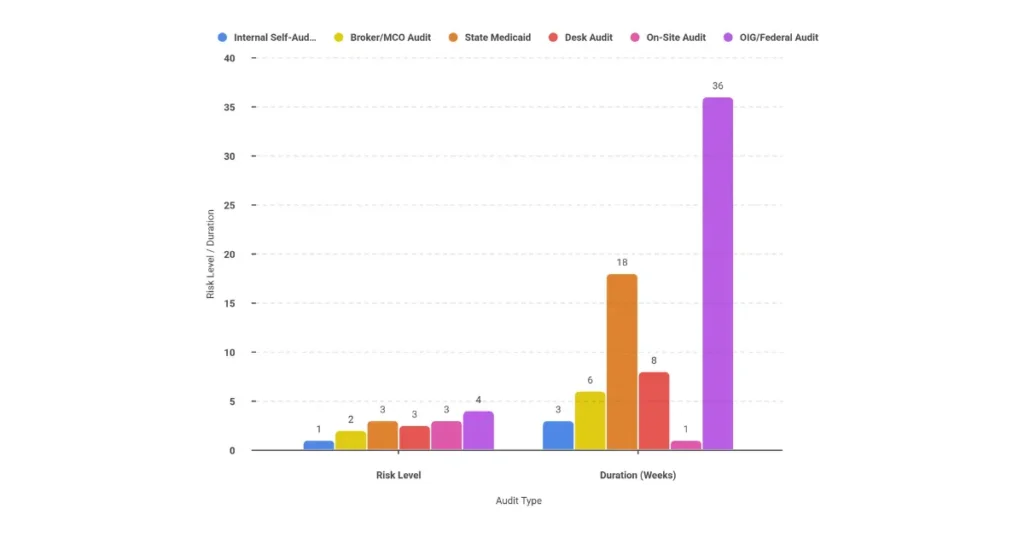
Types of NEMT Audits Comparison
| Audit Type | Conducted By | Primary Focus | Typical Duration | Risk Level |
|---|---|---|---|---|
| Internal Self-Audit | Your Compliance Team | Proactive gap identification | 2-4 weeks quarterly | Low (preventive) |
| Broker/MCO Audit | ModivCare, MTM, Veyo | Contractual compliance, service quality | 1-2 months | Medium |
| State Medicaid Audit | State Program Integrity | Billing compliance, documentation | 3-6 months | High |
| Desk Audit | Any regulatory body | Document review only | 30-60 days | Medium-High |
| On-Site Audit | State or Federal agencies | Physical inspection, interviews | 1-5 days on-site | High |
| OIG/Federal Audit | HHS Office of Inspector General | Fraud detection, statistical sampling | 6-12 months | Critical |
Common Audit Triggers That Demand Attention
Auditors don’t select providers randomly. Specific patterns and anomalies trigger their attention:
Data-Driven Triggers (68% of initial audits)
- Sudden spikes in mileage billing that deviate from historical patterns
- Consistent “rounding” of mileage to whole numbers
- Unusually high wheelchair-to-ambulatory service ratios
- Geographic impossibilities where trip times don’t match distances
- Overlapping trip claims suggesting billing for services not rendered
Complaint and Referral Triggers (22% of audits)
- Patient complaints about service quality or no-shows
- Whistleblower reports from current or former employees
- Referrals from managed care organizations
- Qui tam lawsuits filed under the False Claims Act
Administrative Triggers (10% of audits)
- New provider enrollment within past 24 months
- Ownership changes exceeding 5%
- Revalidation periods requiring updated documentation
- Random selection through CMS PERM sampling programs
What Do Auditors Actually Examine?
Understanding auditor methodology helps you prepare effectively. They employ a “forensic reconstruction” approach, examining every component of your service delivery chain.
Documentation Verification Auditors match trip logs to GPS coordinates with precise timestamps, verify patient signatures were captured at correct geographic locations, confirm Physician Certification Statements contain valid dates and proper credentials, and ensure prior authorization numbers correspond exactly to billed services.
Operational Compliance Your driver qualification files must demonstrate current licenses and required training. Vehicle inspection records need to show ADA compliance and proper maintenance. Safety equipment verification and testing records must be current and complete.
Billing Accuracy Every claim faces scrutiny for appropriate HCPCS code selection, mileage calculations matching GPS breadcrumb trails, timely filing within state-specific deadlines, and exact alignment between claims and trip documentation.
Understanding these examination areas is fundamental to mastering NEMT billing and preventing costly audit findings.
The 5 Essential Documents Auditors Always Request
Why These Documents Are Non-Negotiable
In 2026 enforcement actions, 94% of recoupments stem from documentation deficiencies rather than intentional fraud. Auditors view missing documentation as presumptive evidence of non-compliance—meaning if you can’t prove the service happened exactly as billed, you’ll face recoupment regardless of whether the trip actually occurred.
These five document categories form the foundation of your audit defense strategy.
1. Physician Certification Statement (PCS) Requirements
The PCS serves as your legal justification for medical necessity. Without a valid PCS, auditors consider every related claim an automatic overpayment, regardless of whether the patient genuinely needed transportation.
Critical Components Every PCS Must Include:
- Patient name and Medicaid ID number
- Specific medical condition justifying NEMT (generic statements like “needs transportation” won’t survive audit)
- Required mode of transportation (sedan, wheelchair van, stretcher)
- Frequency and duration of authorized trips
- Physician signature with NPI and credentials
- Date of signature with clear expiration date
Common PCS Deficiencies That Trigger Recoupment:
- Stamped or electronic signatures without documented physician review
- Expired forms with trips billed after the expiration date
- Incomplete clinical justification narratives
- Missing physician credentials or contact information
- Mode of transportation not matching billed service level
Understanding NEMT prior authorization requirements is essential for maintaining compliant PCS documentation.
2. Complete Trip Logs and Manifests
Trip logs serve as your primary evidence of service delivery. In 2026, electronic logs with GPS integration have become the expected standard rather than an optional enhancement.
Required Fields Under 42 CFR §431.53:
| Field Category | Required Information | Documentation Standard |
|---|---|---|
| Patient Data | Full name, Medicaid ID, DOB | Must match enrollment exactly |
| Service Details | Date, actual pickup/dropoff times | Actual times, not scheduled |
| Location Data | Exact addresses with suite numbers | GPS-verified coordinates |
| Vehicle Info | License plate, VIN | Auditable identification |
| Driver Info | Name, license number, signature | Current credentials verified |
| Verification | Patient/representative signature | Electronic with geolocation preferred |
| Mileage | Odometer readings, loaded miles | Calculated to hundredths |
No-Show Documentation Requirements: When patients don’t show for scheduled trips, you must document contact attempts with timestamps, retain records for billing purposes (many states allow no-show billing with proper documentation), and maintain GPS evidence that your vehicle arrived at the scheduled location.
3. Driver Qualification Files
A single unqualified driver can invalidate thousands of claims. Driver compliance represents one of the highest-risk audit areas because auditors can easily verify credential status and apply findings across all trips performed by non-compliant drivers.
Essential Driver Qualification File Components:
| Document Type | Requirement | Retention Period |
|---|---|---|
| Valid License | State-appropriate class, current | Active employment + 3 years |
| MVR | ≤6 points in most states | Annual updates, 7-year history |
| Background Check | 7-year multi-jurisdiction | Indefinite |
| OIG/LEIE Check | Monthly verification | Monthly documentation |
| Drug Testing | DOT 5-panel, pre-employment + random | 5 years negative, 1 year positive |
| Medical Card | DOT physical if applicable | Valid certificate on file |
| Training Certs | PASS, CPR, HIPAA, defensive driving | Indefinite with renewal tracking |
4. Vehicle Compliance Documentation
Your vehicles must demonstrate continuous safety and accessibility compliance throughout their service life. Auditors examine both daily operational records and periodic certification documentation.
Daily Documentation Requirements:
- Daily Vehicle Inspection Reports (DVIRs) signed by drivers before first trip
- Defect reports with repair verification before return to service
- Pre-trip safety checklist completion records
Periodic Documentation:
- State safety inspections (annual or semi-annual depending on jurisdiction)
- DOT biennial inspections for qualifying vehicles
- ADA lift certification and quarterly load testing
- Preventive maintenance logs at manufacturer-specified intervals
- Current registration and insurance certificates
5. Business and Enrollment Documents
Your organizational legitimacy forms the foundation of all audit responses.
Critical Records:
- Medicaid provider enrollment confirmation
- National Provider Identifier (NPI) Type 2
- State operating authority permits (TCP/CPUC in California, Article 19-A in New York, TxDMV livery plates in Texas)
- Certificate of Insurance with required coverage levels
- Business licenses and local permits
- SAM.gov registration and exclusion verification
Organizational Tip: Maintain a digital compliance binder with these documents organized by category, regularly updated, and accessible to your compliance team within 24 hours of any audit request. This preparation alone can reduce audit stress significantly and demonstrate organizational maturity to auditors.
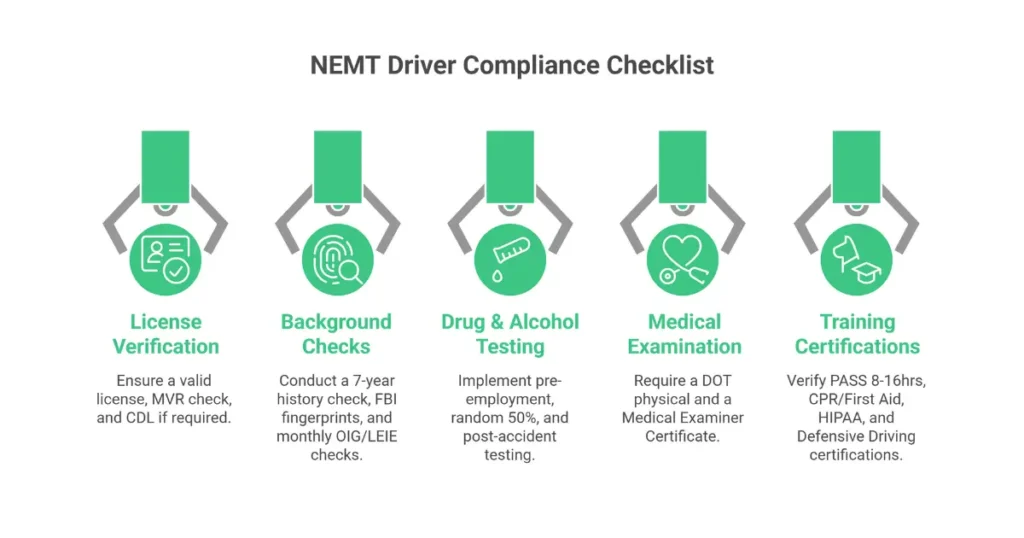
Driver Compliance Audit Checklist: Credentials, Training & Records
The 2026 Standard: Continuous Credential Monitoring
Driver compliance has evolved from periodic verification to continuous monitoring with automated alert systems. A trip performed by a driver with an expired credential—even one day past expiration—can result in 100% recoupment of that claim and trigger expanded sampling across all that driver’s trips.
Driver Licensing Requirements
Essential Verifications:
- Valid driver’s license appropriate for vehicle class
- Minimum 3 years driving experience (varies by state)
- Clean Motor Vehicle Record with ≤6 points in most jurisdictions
- CDL requirements for vehicles exceeding 15 passengers or 26,001 lbs GVWR
- State-specific endorsements where required
Monitoring Protocol:
- Monthly MVR checks through DMV portals or continuous monitoring services
- Automated expiration alerts 30 days before renewal deadlines
- Immediate suspension procedures for license violations
- Documentation of out-of-state license reciprocity acceptance
Background Check Standards
Required Screenings Under 42 CFR §1902(a)(87):
- 7-year multi-jurisdiction criminal history check
- FBI fingerprint-based verification (Level 2 in Florida and other states)
- National Sex Offender Public Website (NSOPW) check
- State nurse aide registry verification
- OIG/LEIE exclusion check with monthly verification
- SAM.gov exclusion verification
Disqualifying Offenses (Common Standards):
- Felonies involving violence, theft, or fraud within 10-year lookback
- Misdemeanors involving abuse or DUI within 5-year lookback
- Active exclusion from any federal healthcare program
- Pattern of serious traffic violations
Drug and Alcohol Testing Requirements
Testing Program Components:
| Test Type | Timing | Requirements |
|---|---|---|
| Pre-employment | Before first trip | DOT 5-panel urine test |
| Random | 50% drugs/10% alcohol annually | Consortium membership required |
| Post-accident | Following DOT criteria | Within specified timeframes |
| Reasonable Suspicion | Supervisor determination | Documented observations |
| Return-to-duty | After positive test | SAP evaluation required |
Documentation Standards:
- Medical Review Officer (MRO) verification reports
- Consortium/Third-Party Administrator (C/TPA) membership documentation
- FMCSA Clearinghouse queries and reporting records
- Record retention: 5 years for negative results, 1 year for positive results
Training Certification Requirements
Mandatory Training Programs:
| Training | Hours Required | Renewal Period | State Variations |
|---|---|---|---|
| PASS (Passenger Assistance) | 8-16 hours | Per state requirement | NC requires DHHS approval |
| CPR/First Aid | 4-8 hours | 2 years | AHA or Red Cross |
| HIPAA Privacy | 2-4 hours | Annual | HHS standards |
| Defensive Driving | 4-8 hours | 3 years | NSC or Smith System |
| Wheelchair Securement | 4-8 hours | Annual refresher | WC-19 standards |
| Bloodborne Pathogens | 2 hours | Annual | OSHA 29 CFR 1910.1030 |
Driver Compliance Checklist
Use this checklist to verify each driver file meets audit standards:
- Valid driver’s license (verified current, appropriate class)
- MVR on file (≤6 points, updated within 12 months)
- Background check complete (7-year history, all required databases)
- OIG/LEIE exclusion check (current month verified)
- Drug test results (pre-employment completed, random pool enrolled)
- Medical Examiner Certificate (if DOT-regulated, current and valid)
- PASS training certificate (state-approved, current)
- CPR/First Aid certification (current, proper provider)
- HIPAA training (completed within past 12 months)
- Defensive driving (completed within required timeframe)
- Wheelchair securement training (if applicable, current)
- Bloodborne pathogens training (completed within past 12 months)
- Signed acknowledgment of company policies
- Employment application and verification documents
Implementing systematic driver compliance management is essential for starting NEMT billing operations on a solid foundation.
Vehicle Compliance Audit Checklist: Inspections, Maintenance & Safety
The 2026 Standard: Smart Inspection Compliance
Vehicle compliance has evolved from paper checklists to integrated telematics systems. Your vehicles must demonstrate continuous safety through digital verification rather than periodic inspections alone.
Daily Pre-Trip Inspection Requirements
Mandatory DVIR Components Under 49 CFR §396.11:
- Tires: Pressure check and tread depth verification (≥2/32″ minimum)
- Brakes: Fluid levels, pad condition, parking brake function
- Lights and Signals: Headlights, brake lights, turn signals, hazard lights
- Safety Equipment: Fire extinguisher, first aid kit, emergency tools present
- Accessibility Features: Lift operation test, securement system check
- Climate Control: Heating and cooling functionality (72-78°F capability)
- Documentation: Driver signature, odometer reading, defect notation
Electronic Documentation Standards:
- Digital DVIR completion required before first trip of day
- Photographic evidence of any identified defects
- Automatic transmission to maintenance management system
- Repair verification documentation before vehicle return to service
- Retention: 3 months minimum (vehicle life +3 years recommended)
State and Federal Inspection Requirements
| Inspection Type | Frequency | Key Requirements | Applicable States |
|---|---|---|---|
| State Safety | Annual/Semi-annual | Brakes, tires, steering, lights | All states |
| DOT Biennial | Every 24 months | Comprehensive safety systems | Interstate operations |
| ADA Certification | Annual | Lift capacity, securement | All ADA vehicles |
| VSSI | Biennial | Vehicle Safety Systems | California |
| TLC B-26 | Semi-annual | Taxi & Limousine standards | New York City |
| DPS Annual | Yearly | Department of Public Safety | Texas |
ADA Accessibility Compliance
Wheelchair Lift Requirements:
- Minimum 800 lb lifting capacity
- Maximum 48″ deployment height
- Quarterly proof-load testing with documented results
- Annual calibration certification
- Monthly lubrication and maintenance documented
Securement System Standards:
- Four-point tie-downs meeting WC-19 standards
- Minimum 2,500 lb strap capacity
- Pre- and post-trip inspection documentation
- Annual load testing certification
- Proper storage and accessibility
Vehicle Interior Standards:
- Minimum 56″ interior height (60″ for larger vehicles)
- Clear floor space: 30″×48″ (facing) or 36″×60″ (side entry)
- Grab bars: 1.5-1.75″ diameter, 24-30″ vertical height
- Door width: ≥32″ clear opening
- ADA placards permanently and visibly affixed
Required Safety Equipment
Mandatory Equipment Checklist:
| Equipment | Specification | Inspection Frequency |
|---|---|---|
| Fire Extinguisher | 2A:10B:C rating | Monthly gauge check, annual service |
| First Aid Kit | OSHA-compliant contents | Monthly inventory, expiration tracking |
| Seatbelt Cutter | Accessible location | Monthly presence verification |
| Window Punch | Accessible location | Monthly presence verification |
| Spill Kit | Absorbents and PPE | Quarterly inventory |
| Reflective Triangles | 3 minimum | Monthly presence verification |
| BBP Kit | Gloves, sharps container | Quarterly inventory |
| Communication Device | Two-way radio or cellular | Daily function test |
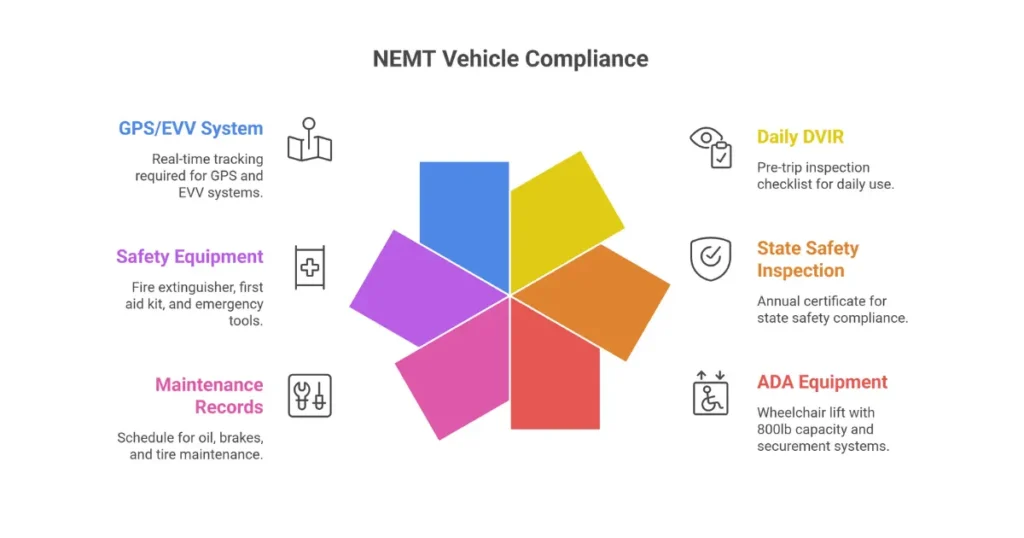
GPS and EVV Integration Requirements
21st Century Cures Act Compliance:
- Real-time GPS tracking with 1-5 second interval capture
- EVV visit verification capturing exact timestamps and geolocation
- Data transmission to state and broker portals (Sandata, HHAeXchange)
- Minimum 7-year data retention capability
- 500-foot geofencing accuracy for pickup/dropoff verification
System Verification Protocol:
- Monthly GPS accuracy testing against known reference points
- Quarterly EVV system audits for data integrity
- Regular broker portal synchronization verification
- Data backup and disaster recovery testing
Understanding which NEMT software solutions offer the best compliance features can significantly reduce your audit risk.
Vehicle Compliance Checklist
- Current state safety inspection certificate displayed
- DOT inspection current (if applicable)
- ADA lift certification current (quarterly test documented)
- Daily DVIR completed and filed
- Maintenance schedule current (oil, brakes, tires per manufacturer specs)
- Fire extinguisher serviced and gauge in green
- First aid kit complete with no expired items
- All safety equipment present and functional
- Registration current and displayed
- Insurance certificate current with required coverage
- GPS/EVV system operational and transmitting
- Vehicle age and mileage within contract limits
- ADA placards visible and compliant
- Interior cleanliness meets standards
Trip Documentation and Billing Compliance for Audits
The 2026 Standard: Forensic Documentation
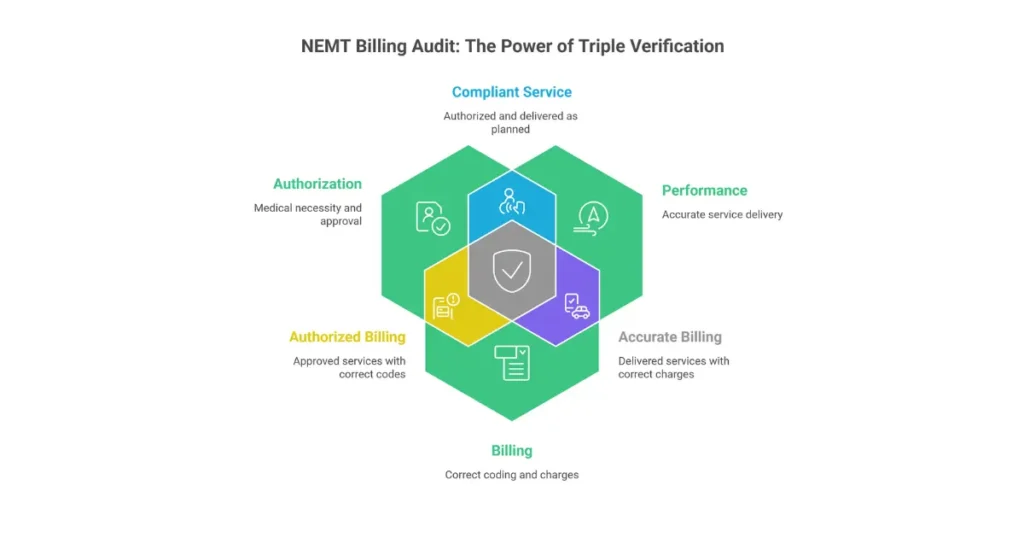
Trip documentation has transformed from basic record-keeping to forensic evidence creation. Every document must withstand scrutiny through metadata analysis and cross-referencing with multiple verification sources. Auditors employ “triple match” verification: comparing authorization, performance (GPS/logs), and billing for every sampled claim.
Required Trip Documentation Fields
Patient Information (Must Match Medicaid Enrollment Exactly):
- Full legal name
- Medicaid ID number (verified current eligibility)
- Date of birth
- Contact information (recommended for service verification)
Service Details:
- Service date (actual date of transport)
- Pickup and drop-off times (actual, not scheduled)
- Exact addresses including suite/apartment numbers
- Facility names when applicable
- Special instructions or accommodation needs
Vehicle and Driver Verification:
- Vehicle identification (VIN or license plate)
- Driver name and license number
- Odometer readings at pickup and drop-off
- Loaded mileage calculation (to hundredths of a mile)
Required Signatures and Attestations:
- Patient or authorized representative signature (electronic with geolocation preferred)
- Driver attestation of service delivery
- Escort/attendant signature if applicable
GPS and EVV Integration Standards
The 21st Century Cures Act mandates Electronic Visit Verification for Medicaid-funded transportation services. Your system must capture:
Required Data Elements:
- GPS breadcrumb trails at 1-5 second intervals throughout trip
- Exact pickup coordinates matched to documented address
- Exact dropoff coordinates matched to destination
- Real-time data transmission to state/broker aggregators
- Tamper-evident logging preventing after-the-fact modifications
Verification Standards:
- Coordinate matching within 500 feet of documented addresses
- Timestamp validation against facility operating hours
- Route analysis confirming mileage accuracy
- Anomaly detection flagging impossible trips
Prior Authorization Management
Understanding when prior authorization is required prevents claim denials and audit findings:
Services Typically Requiring Prior Authorization:
- Non-ambulatory transports (wheelchair, stretcher)
- Recurring trips (dialysis, chemotherapy, physical therapy)
- Long-distance transports (typically >20-100 miles, state-dependent)
- Out-of-state transports
Standing Order Requirements:
- Valid for 30-365 days depending on state
- Must specify frequency (e.g., 3x weekly)
- Requires physician signature with credentials
- Must match billed service level
For patients requiring regular treatment like dialysis transportation, proper standing order management is essential for billing compliance.
HCPCS Codes and Billing Accuracy
Common NEMT Procedure Codes:
| Code | Description | Documentation Required |
|---|---|---|
| A0130 | Non-emergency transportation | Trip log, signature, PCS |
| T2002 | Non-emergency transport, per trip | Trip log, signature |
| T2003 | Non-emergency transport, per trip (group) | Group manifest, all signatures |
| T2005 | Non-emergency transport, stretcher | Medical necessity, stretcher PCS |
| A0425/A0426 | Mileage codes | GPS-verified loaded miles |
Modifier Requirements:
- Origin/destination modifiers indicating pickup and dropoff locations
- Service level modifiers (U1-U9) where required by state
- UD modifier for pickup identification in some states
Timely Filing Requirements by State
| State | Filing Deadline | Notes |
|---|---|---|
| New York | 90 days | From date of service |
| California | 12 months | From date of service |
| Texas | 95 days | From date of service |
| Florida | 12 months | From date of service |
| Pennsylvania | 180 days | From date of service |
| Federal Standard | 365 days | Unless state specifies shorter |
Understanding state-specific Medicaid NEMT rates and filing requirements is crucial for billing compliance.
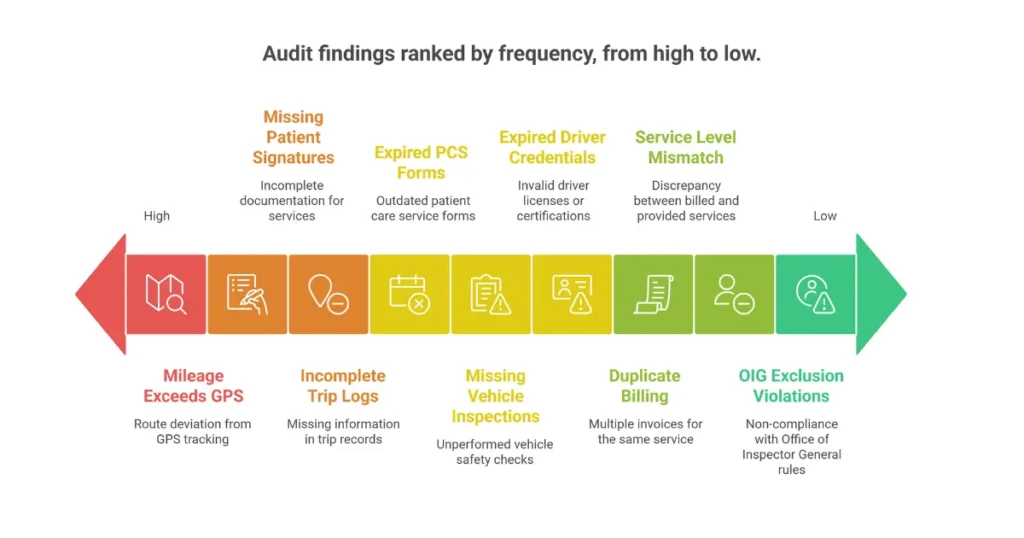
Common Billing Errors and Fraud Indicators
Documentation-Related Errors (Most Common):
- Missing patient signatures (found in 55% of audit samples)
- Incomplete trip logs (48% of reviews)
- Expired PCS forms (42% of providers)
- Non-contemporaneous entries created after service (35% of cases)
Billing-Specific Errors:
- Mileage exceeding GPS-calculated distance
- Duplicate claims for same patient/date/time
- Upcoding (billing wheelchair for ambulatory patient)
- Service level mismatches between PCS and claim
- Timely filing violations
Fraud Indicators That Trigger Criminal Investigation:
- Phantom trips (billing without GPS evidence of service)
- Batch signatures (multiple trips signed simultaneously)
- Geographic impossibilities (driver appearing in two locations)
- Deceased member billing
- Kickback arrangements with referral sources
Understanding NEMT denial codes helps identify documentation gaps before they become audit findings.
Record Retention Requirements
| Document Type | Federal Minimum | Recommended | Notes |
|---|---|---|---|
| Trip Records | 6 years | 10 years | State may require longer |
| PCS Forms | 6 years | 10 years | Until resolved if appealed |
| Driver Files | 3 years post-termination | 7 years | Some states require longer |
| Vehicle Records | Vehicle life + 1 year | Vehicle life + 3 years | Per 49 CFR §396.3 |
| Billing Claims | 6 years | 10 years | False Claims Act statute |
| GPS/EVV Data | Per state requirement | 7 years | 21st Century Cures Act |
| HIPAA Records | 6 years | 6 years | Per 45 CFR §164.530 |
HIPAA Compliance for NEMT Audit Readiness
The Unique HIPAA Challenges in NEMT
NEMT providers handle Protected Health Information (PHI) in uniquely vulnerable environments—moving vehicles, public spaces, and through multiple technology systems. In 2026, geographic data combined with medical information creates heightened compliance risks that auditors scrutinize intensively.
What Constitutes PHI in NEMT Operations?
Direct PHI Elements:
- Patient names and contact information
- Medicaid ID numbers and eligibility data
- Medical conditions listed on PCS forms
- Appointment details revealing health status
- Treatment facility information
Often-Overlooked PHI:
- GPS coordinates linking patient to healthcare facility
- Trip histories indicating treatment patterns (e.g., regular dialysis runs)
- Addresses that reveal healthcare visits when combined with destination
- Dispatch notes containing medical information
Key Insight: In NEMT, addresses become PHI when they reveal healthcare facility visits, and GPS coordinates become PHI when they track medical appointments. This expanded definition requires comprehensive protection protocols.
Privacy Rule Implementation
Minimum Necessary Standard Application:
- Drivers should see only pickup/dropoff details and essential accommodation needs—not full medical histories
- Dispatchers access only information necessary for scheduling
- Billing staff view only data required for claims submission
- Role-based access controls in all systems enforce these limitations
Patient Rights Under HIPAA:
- Right to access their PHI (must respond within 30 days)
- Right to request amendments to their records
- Right to accounting of disclosures
- Right to request restrictions on uses
Security Rule Requirements
Administrative Safeguards (45 CFR §164.308):
- Designated Privacy and Security Officers
- Annual risk assessments documented and retained
- Workforce security policies with access controls
- Contingency plans for data breaches
- Security management processes with regular updates
Physical Safeguards (45 CFR §164.310):
- Secure facility access controls
- Vehicle security for PHI storage (locked gloveboxes for manifests)
- Workstation security policies
- Device and media controls
- Secure disposal procedures (shredding, secure deletion)
Technical Safeguards (45 CFR §164.312):
- Unique user identification for all system access
- Automatic logoff after 5-15 minutes of inactivity
- Encryption of electronic PHI (AES-256 standard)
- Audit controls logging all access and modifications
- Integrity controls preventing unauthorized alteration
Business Associate Agreement Requirements
Entities Requiring BAAs:
- Transportation brokers (ModivCare, MTM, Veyo)
- Software vendors (dispatch, EVV, billing systems)
- Billing companies and revenue cycle partners
- IT support and cloud storage providers
- Any entity handling PHI on your behalf
Required BAA Provisions:
- Permitted uses and disclosures of PHI
- Safeguard requirements matching your security policies
- Breach notification requirements (typically within 60 days)
- Audit rights and inspection provisions
- Termination conditions and data return procedures
HIPAA Training Requirements
Mandatory Training Topics:
- PHI identification in NEMT operations
- Minimum necessary principle application
- Patient rights under HIPAA
- Breach recognition and reporting procedures
- Secure transportation practices
- Technology security protocols
Documentation Requirements:
- Initial training completion records within 30 days of hire
- Annual refresher training attendance
- Competency assessments demonstrating understanding
- Signed attestations retained for 6+ years
Breach Notification Protocols
What Constitutes a Breach:
- Unauthorized acquisition, access, use, or disclosure of PHI
- Compromises the security or privacy of information
- Presumed breach unless demonstrated low probability of compromise
Notification Timeline Requirements:
- Individuals: Within 60 days of discovery
- HHS: For breaches affecting 500+ individuals, immediately
- Media: For breaches affecting 500+ individuals in a state
- State Attorneys General: As required by state law (California requires 15 days)
HIPAA Compliance Checklist
- Privacy and Security Officers designated
- Annual risk assessment completed and documented
- Written policies and procedures in place
- All workforce members trained (documentation retained)
- BAAs executed with all business associates
- BAA inventory maintained and current
- Electronic PHI encrypted (at rest and in transit)
- Access controls implemented (unique IDs, role-based)
- Audit logs enabled and reviewed
- Breach response plan documented and tested
- Notice of Privacy Practices provided to patients
- Physical safeguards in place (locked storage, secure disposal)
How to Conduct an Internal NEMT Compliance Audit (Self-Audit)
The Strategic Value of Self-Audits
Internal compliance audits represent your most powerful defense against external findings. According to 2025 industry data, providers who conduct quarterly self-audits experience 70% fewer major audit findings and reduce recoupment amounts by an average of 85%.
Self-audits have evolved from periodic checks to continuous quality improvement systems. The goal isn’t just identifying problems—it’s building systems that prevent them from recurring.
Audit Planning and Scope Definition
Risk Assessment Framework: Before diving into document review, assess where your highest risks lie:
- Analyze denial patterns from past 90 days
- Review previous audit findings (internal and external)
- Identify new drivers or vehicles added recently
- Consider complaint trends or whistleblower reports
- Evaluate geographic or operational risk factors
Scope Determination:
- Select audit period (typically previous quarter)
- Determine sample size (2% of trips or minimum 200)
- Identify specific audit categories for examination
- Allocate resources and set realistic timeline (4-6 weeks typical)
Sampling Methodology
Statistical Sampling Approaches:
- Random sampling: Use Excel RAND() function for unbiased selection
- Stratified sampling: Sample across driver, vehicle, or service type categories
- Targeted sampling: Focus on high-risk areas identified in risk assessment
- Statistical validity: Target 95% confidence level with ±5% margin of error
Sample Size Guidelines:
- Small providers (<1,000 trips/month): 5% sample or 50 trips minimum
- Medium providers (1,000-5,000 trips/month): 2% sample
- Large providers (>5,000 trips/month): 1% sample or 200 trips minimum
- Always sample at least 95 trips for statistical validity
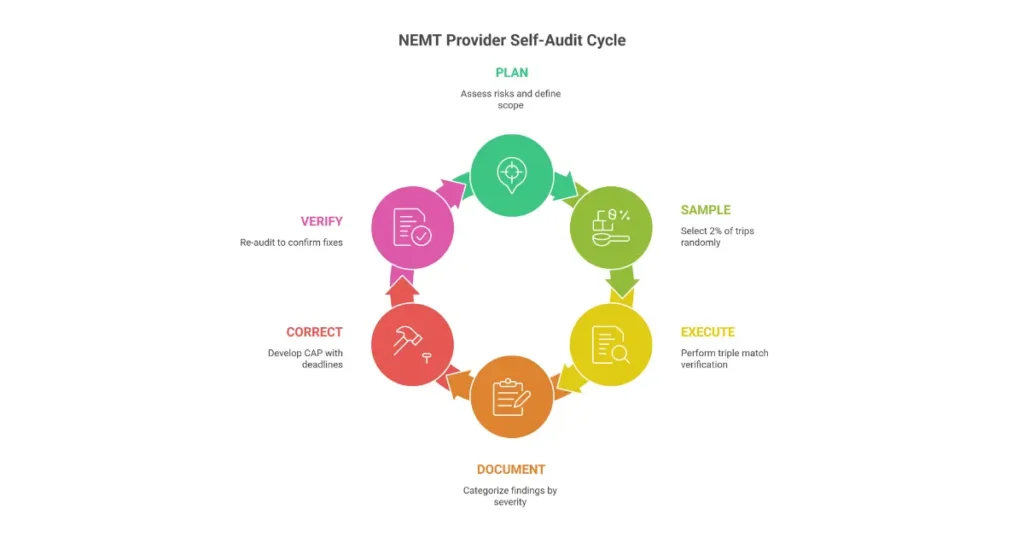
Audit Execution: The Triple Match Verification
For each sampled trip, verify the “triple match”:
1. Authorization Match
- Valid PCS on file covering service date
- Prior authorization number matches claim
- Service level authorized matches service level billed
- Physician signature current and credentials valid
2. Performance Match
- Trip log complete with all required fields
- GPS data confirms vehicle at pickup and dropoff locations
- Timestamps align with documented service times
- Mileage calculation matches GPS route
3. Billing Match
- HCPCS code appropriate for service provided
- Modifiers correctly applied
- Mileage billed matches GPS-verified distance
- Claim submitted within timely filing deadline
- No duplicate claims for same service
Finding Documentation and Categorization
Severity Classification:
- Critical: Fraud risk indicators, immediate action required (7-day remediation)
- Major: Systemic compliance gaps affecting multiple trips (30-day remediation)
- Minor: Isolated errors without pattern (60-day remediation)
- Observation: Recommendations for improvement, no formal action required
Root Cause Analysis: When findings emerge, dig deeper using the “Five Whys” technique:
- Why was the signature missing? (Driver forgot)
- Why did driver forget? (No reminder in system)
- Why no reminder? (System not configured properly)
- Why not configured? (Training gap in setup)
- Why training gap? (Onboarding process incomplete)
Root cause: Onboarding process needs signature capture training module.
Corrective Action Plan Development
Effective CAP Components:
- Specific description of finding and root cause
- Concrete corrective actions (not “improve documentation”)
- Responsible party assigned for each action
- Realistic deadline for completion
- Verification method to confirm fix implemented
- Prevention strategy to avoid recurrence
Sample CAP Entry:
| Finding | Root Cause | Corrective Action | Owner | Deadline | Verification |
|---|---|---|---|---|---|
| 15% of trips missing patient signature | Drivers not using signature app consistently | Implement hard-stop requiring signature before trip completion | Operations Manager | 30 days | System audit showing 0% incomplete trips |
Follow-up and Verification
Re-audit Protocol:
- Schedule targeted review 30-60 days after CAP implementation
- Sample same areas to verify improvement
- Document reduction in finding rate
- Escalate unresolved issues to leadership
Performance Metrics to Track:
- Finding closure rate: Target 100% within deadlines
- Recurrence prevention: Target <2% repeat findings
- Staff compliance: Target >95% adherence to new procedures
- Process improvement: Measurable efficiency gains
When to Seek External Assistance
Indicators That External Audit Help Is Needed:
- High-risk findings (>10% error rate) in any category
- First-time audit preparation with limited internal expertise
- Post-complaint or investigation situations
- Complex regulatory requirements exceeding staff knowledge
External Consultant Selection Criteria:
- CHC (Certified in Healthcare Compliance) certification preferred
- Demonstrated NEMT-specific experience
- References from similar-sized providers
- Clear deliverables and cost structure
For providers needing expert guidance, professional NEMT billing services can provide compliance support and audit preparation assistance.
Common NEMT Audit Findings and How to Avoid Them
The Financial Impact of Common Findings
Audit findings represent more than compliance failures—they’re direct threats to your financial stability. In 2025, the average NEMT audit recoupment exceeded $250,000 per provider, with findings typically falling into predictable, preventable categories.
Top 10 Audit Findings with Prevention Strategies
| Rank | Finding | Frequency | Recoupment Impact | Prevention Strategy |
|---|---|---|---|---|
| 1 | Missing patient signatures | 55% of audits | 100% of unsigned claims | Implement EVV with required signature capture |
| 2 | Mileage exceeds GPS distance | 68% of audits | Per-claim recoupment | Automated GPS-to-billing reconciliation |
| 3 | Incomplete trip logs | 48% of audits | 100% of incomplete claims | Mandatory field validation in dispatch software |
| 4 | Expired PCS forms | 42% of audits | All trips after expiration | PCS tracking system with 30-day alerts |
| 5 | Expired driver credentials | 35% of audits | All trips by that driver | Automated credential tracking with hard stops |
| 6 | Missing vehicle inspections | 40% of audits | All trips by that vehicle | Electronic DVIR with completion requirements |
| 7 | Duplicate billing | 25% of audits | 100% of duplicates plus penalties | Claims scrubbing before submission |
| 8 | Service level mismatch | 22% of audits | Difference in service levels | PCS-to-billing validation |
| 9 | OIG exclusion violations | 18% of audits | All trips by excluded driver | Monthly LEIE screening automation |
| 10 | Timely filing failures | 18% of audits | 100% of late claims | Filing deadline tracking with alerts |
Case Study Analysis: Learning from Others’ Mistakes
New York OIG Audit: $196 Million in Improper Payments
- Primary Issue: Lack of trip verification and broker oversight
- Finding: 72% of sampled claims lacked adequate service proof
- Lesson: Real-time GPS verification and contemporaneous documentation are non-negotiable
- Prevention: Implement triple-match verification for every claim before submission
Massachusetts Review: $14 Million Improper Payments
- Primary Issue: Documentation created after service delivery
- Finding: Timestamps and metadata revealed post-hoc documentation
- Lesson: Contemporaneous means at the time of service, not later that day
- Prevention: Mobile documentation apps that capture data in real-time with GPS timestamps
Oklahoma Audit: $6.9 Million Across 128,000 Claims
- Primary Issue: Medical necessity documentation failures
- Finding: PCS forms missing, expired, or lacking required clinical detail
- Lesson: PCS is the foundation—without it, all related claims fail
- Prevention: PCS validation before scheduling, with automatic service-date checks
Prevention Framework: The Layered Defense Model
Layer 1: System Controls (Prevent Errors)
- Mandatory fields in dispatch software
- Hard stops preventing dispatch of unqualified drivers
- Automated mileage calculation from GPS
- PCS expiration blocking for scheduling
Layer 2: Process Verification (Detect Errors)
- Daily log review by supervisor
- Weekly billing reconciliation
- Monthly credential verification
- Quarterly self-audits
Layer 3: Continuous Monitoring (Identify Patterns)
- Real-time compliance dashboards
- Trend analysis for emerging issues
- Benchmarking against industry standards
- Regular performance metric review
Technology Solutions for Finding Prevention
High-Impact Technology Investments:
- EVV with signature capture: Eliminates missing signature findings
- GPS-integrated billing: Prevents mileage inflation findings
- Credential tracking software: Automates driver compliance monitoring
- Claims scrubbing: Catches errors before submission
- Document management: Enables rapid audit response
The NEMT industry continues to grow, making compliance-focused technology investments increasingly important for competitive positioning.
What to Do When You Receive an Audit Notice
Immediate Response Protocol (First 48 Hours)
Receiving an audit notice triggers a critical timeline. Every action—or inaction—from this moment forward affects your outcome. Here’s your step-by-step response protocol:
Hour 1-4: Initial Assessment
- Read the entire notice carefully, noting scope and deadlines
- Identify audit type (desk, on-site, targeted, random)
- Determine review period and sample specifics
- Log notice details in compliance tracking system
- Calculate response deadline and establish milestones
Hour 4-24: Mobilization
- Issue formal document preservation order to all staff
- Halt routine document destruction processes
- Secure electronic data against modification
- Notify leadership team and legal counsel if warranted
- Inform brokers/MCOs of audit initiation
Hour 24-48: Team Assembly
- Designate Single Point of Contact (SPOC) for auditor communications
- Assign document gathering responsibilities
- Schedule daily coordination meetings
- Begin preliminary document inventory
- Acknowledge receipt to auditing entity in writing
Audit Response Team Composition
| Role | Primary Responsibilities | Time Commitment |
|---|---|---|
| Compliance Officer (Lead) | Overall coordination, auditor communication | 50-100% during response |
| Legal Counsel | Regulatory guidance, privilege protection | As needed |
| Operations Director | Service delivery documentation | 25-50% during response |
| Billing Manager | Claims and financial records | 25-50% during response |
| IT Specialist | Electronic data extraction | 25% during response |
| Department Representatives | Subject matter expertise | As needed |
Document Gathering and Organization
Priority System for Document Assembly:
- Critical Credentials: Driver licenses, insurance certificates, enrollment documents
- Primary Evidence: Trip logs, GPS data, PCS forms for sampled claims
- Supporting Documentation: Policies, training records, maintenance logs
- Supplemental Materials: Communications, meeting notes, system documentation
Organization Best Practices:
- Create indexed digital folders by audit sample item
- Use consistent naming conventions (e.g., “Claim12345-TripLog.pdf”)
- Prepare cover letter summarizing submission contents
- Include table of contents for easy navigation
- Complete quality check 48 hours before deadline
Communication Guidelines with Auditors
Professional Conduct Rules:
- Confirm receipt of all communications in writing within 24 hours
- Request clarification on ambiguous requirements promptly
- Provide status updates as milestones are reached
- Maintain written records of all communications
- Escort auditors during any on-site visits—never leave them unsupervised
What NOT to Do:
- Never admit fault or speculate about errors
- Don’t volunteer information beyond what’s requested
- Avoid informal or unrecorded conversations
- Don’t allow unsupervised access to staff or systems
- Never destroy or alter documents after receiving notice
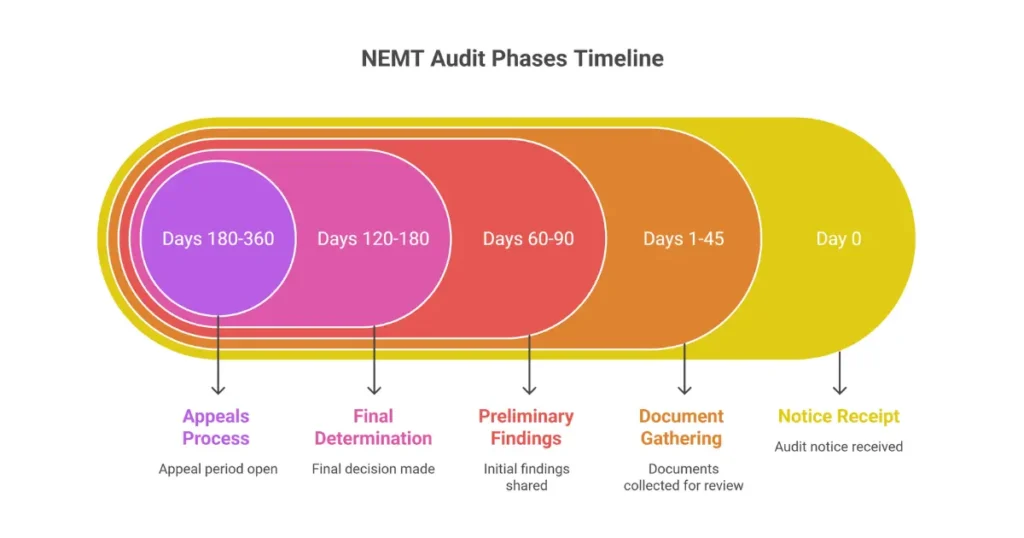
Audit Response Timeline
| Phase | Timeframe | Key Activities |
|---|---|---|
| Notice Receipt | Day 0 | Read, log, notify leadership |
| Mobilization | Days 1-3 | Preserve documents, assemble team |
| Document Gathering | Days 4-30 | Collect, organize, review |
| Quality Control | Days 30-40 | Verify completeness, accuracy |
| Submission | Days 40-45 | Submit with cover letter, index |
| Preliminary Findings | Days 60-90 | Review, prepare response if needed |
| Final Determination | Days 120-180 | Accept or initiate appeal |
| Appeal Process | Days 180-360 | If contesting findings |
Extension Request Strategy
When to Request an Extension:
- Complex document retrieval requirements
- Key personnel unavailability
- Technical difficulties accessing records
- Volume of records exceeding reasonable review time
How to Request:
- Submit written request before 50% of deadline has passed
- Provide specific justification (not “we need more time”)
- Suggest reasonable alternative deadline
- Document all extension communications
- Have contingency plan if extension is denied
Audit Outcomes: Appeals, Corrective Actions, and Recovery
Understanding Audit Determinations
The audit outcome represents your opportunity to challenge findings, demonstrate improvements, and manage financial impacts. Understanding the process helps you respond effectively.
Preliminary vs. Final Findings:
- Preliminary findings arrive 60-90 days after document submission
- You have opportunity to respond with additional evidence
- Final determination issued 120-180 days after submission
- Appeal rights begin from final determination date
Finding Categories Under 2026 CMS Framework:
- Corrective Action Required (CAR): Systemic issues requiring documented fix
- Observation: Recommendations without mandatory action
- No Finding: Compliant—no action required
Appeal Rights and Procedures
State-Specific Appeal Timelines:
| State | Initial Appeal Deadline | Process | Notes |
|---|---|---|---|
| New York | 60 days | Informal review, then 28 CFR §115.403 hearing | 100% recoupment if deadline missed |
| California | 90 days | DHCS ALJ review | Written submission required |
| Texas | 30 days | TMHP appeal, 120-day reopen option | Expedited process available |
| Florida | 25 days | AHCA appeal | Strict deadline enforcement |
| Pennsylvania | 33 days | OBMP review | Extension rarely granted |
| Federal | 60 days | 42 CFR Part 498 | Administrative then ALJ |
Grounds for Successful Appeals:
- Documentary evidence contradicting findings
- Statistical sampling methodology errors
- Procedural violations in audit conduct
- New information unavailable during initial review
- Misinterpretation of regulatory requirements
Appeal Success Factors:
- 30-50% success rate for well-documented appeals
- 60% success rate when challenging extrapolation methodology
- Strong GPS evidence most persuasive for trip disputes
- Statistical expert testimony helpful for sampling challenges
Corrective Action Plan Requirements
When CAP Is Required:
- Any finding classified as “Corrective Action Required”
- Multiple related findings suggesting systemic issues
- Repeat findings from previous audits
- Findings involving potential fraud indicators
Effective CAP Components:
- Root cause analysis using Five Whys or fishbone diagram
- Specific corrective actions (not vague commitments)
- Responsible party and deadline for each action
- Verification method demonstrating implementation
- Prevention strategy to avoid recurrence
- Timeline for completion (typically 30-90 days)
CAP Approval and Monitoring:
- Submit within specified timeframe (usually 30 days)
- Auditor review takes 15-30 days
- Modifications may be requested
- Quarterly progress reports often required
- Final verification and closure documentation
Recoupment Management
How Recoupment Is Calculated:
- Statistical extrapolation: Error rate from sample × total claims universe
- Example: 10% error rate in 50-claim sample applied to 10,000 claims = potential $500,000+ recoupment
- Lower Confidence Limit: Conservative statistical calculation reducing provider risk
- Interest typically accrues at 9.375% (CMS rate)
Payment Options:
- Lump sum: Full immediate payment (sometimes eligible for small discount)
- Extended Repayment Schedule: Monthly installments over 12-36 months
- Offset arrangement: Percentage withheld from future claims
- Hardship waiver: Reduced payment based on financial condition
Hardship Determination Criteria:
- Recoupment exceeds 10% of annual revenue
- Documentation of financial impact required
- May result in interest reduction or extended terms
- Quarterly review of continued hardship status
Business Recovery and Improvement
Immediate Actions Post-Audit:
- Implement all CAP requirements on schedule
- Communicate outcomes to staff appropriately
- Preserve broker relationships through transparency
- Adjust cash flow projections for any recoupment
- Review insurance coverage for audit-related costs
Long-Term Improvement Strategy:
- Increase self-audit frequency based on findings
- Invest in technology addressing identified gaps
- Enhance training programs for problem areas
- Consider external compliance assessment
- Benchmark against industry standards
For comprehensive billing and compliance support, professional medical billing services can help implement sustainable improvements.
Technology and Software for NEMT Audit Compliance
The 2026 Technology Imperative
Manual compliance processes are no longer viable given the volume of data and complexity of regulatory requirements in 2026. The right technology stack can reduce audit preparation time from 40+ hours to under 2 hours while cutting error rates by 60-80%.
NEMT Software Feature Comparison
| Feature | Audit Impact | Implementation Priority | Top Platforms |
|---|---|---|---|
| Automated Credential Tracking | 35% reduction in driver findings | Critical | Tobi, Traumasoft, RouteGenie |
| GPS/EVV Integration | 60% reduction in mileage disputes | Critical | All major platforms |
| Claims Scrubbing | 45% reduction in billing errors | High | TripSpark, Traumasoft, AngelTrack |
| Document Management | 50% faster audit response | High | Traumasoft, Momentm, Bambi |
| Compliance Dashboards | 30% improvement in monitoring | Medium | Tobi, Caretap, RouteGenie |
| Audit Report Generation | 80% time savings in preparation | High | All major platforms |
Essential Technology Categories
Compliance Management Software: Core capabilities should include automated credential tracking with expiration alerts, compliance monitoring dashboards, document management with retention enforcement, and audit trail documentation with tamper-evident logging.
GPS and EVV Systems: Must-have features include real-time tracking at 1-5 second intervals, EVV verification meeting 21st Century Cures Act requirements, geofencing accuracy within 500 feet, and 7-year data retention capability.
Billing and Claims Management: Look for automated claims scrubbing, duplicate detection, mileage verification against GPS, and timely filing deadline tracking with alerts.
Document Management: Essential features include OCR scanning and indexing, secure cloud storage with encryption, role-based access controls, and retention policy enforcement.
For detailed software comparisons, see our guide to the best NEMT software solutions.
ROI Analysis for Technology Investment
Quantifiable Benefits:
- Denial rate reduction: From 15-25% to <3% (average $50,000+ annual savings)
- Audit preparation time: From 40+ hours to <2 hours ($5,000+ labor savings per audit)
- Recoupment prevention: Average $250,000+ per prevented audit failure
- Administrative efficiency: 60-80% reduction in manual compliance work
Typical Payback Period:
- Small providers (1-5 vehicles): 3-4 months
- Medium providers (6-20 vehicles): 4-6 months
- Large providers (20+ vehicles): 6-9 months
Implementation Considerations
Software Selection Criteria:
- HIPAA BAA compliance commitment
- Broker API integration capabilities (ModivCare, MTM, Veyo)
- Reporting flexibility and customization
- Scalable cost structure
- Implementation timeline and support quality
- Training resources and documentation
Implementation Timeline:
- Planning and requirements: 2-4 weeks
- Configuration and setup: 4-6 weeks
- Data migration: 2-4 weeks
- Testing and validation: 2-3 weeks
- Training: 2 weeks
- Phased go-live: 4-8 weeks
For providers seeking comprehensive technology solutions, NEMT website development services can help build integrated compliance platforms.
Building a Compliance Culture: Staff Training and Continuous Improvement
The Foundation of Sustainable Compliance
Technology and checklists matter, but culture determines whether compliance becomes embedded in operations or remains a box-checking exercise. Providers with mature compliance cultures experience 40% lower audit findings compared to those relying solely on procedural controls.
Leadership-Driven Culture Development
Tone at the Top:
- Executive modeling of compliance priorities in daily decisions
- Regular communication from leadership about compliance importance
- Resource allocation demonstrating compliance is a priority, not an afterthought
- Performance evaluation inclusion of compliance metrics at all levels
- Visible leadership participation in training and compliance activities
Ethical Foundation Building:
- Clear organizational values emphasizing integrity over revenue
- Patient dignity and safety as core decision-making principles
- Transparent communication about challenges and improvements
- Accountability for ethical breaches without exception
Structured Training Program Design
Onboarding Training Requirements:
- Completion within 30 days of hire
- Content: HIPAA, PCS rules, EVV systems, safety protocols, company policies
- Duration: 8-16 hours depending on role
- Verification: Competency assessment with 80% minimum pass rate
- Documentation: Signed completion records retained 6+ years
Role-Specific Training:
- Drivers: PASS certification, wheelchair securement, defensive driving, customer service
- Dispatchers: PCS validation, scheduling ethics, documentation standards, EVV operation
- Billers: HCPCS coding, timely filing, claims accuracy, denial management
- Managers: Compliance oversight, audit response, risk management, performance metrics
Annual Refresher Requirements:
- Frequency: Annual minimum (semi-annual for high-risk areas)
- Duration: 4-8 hours depending on regulatory changes
- Content: Regulatory updates, lessons learned from audits, skill reinforcement
- Delivery: Hybrid approach (eLearning + in-person scenarios)
Compliance Officer Role and Authority
Qualifications:
- CHC (Certified in Healthcare Compliance) certification preferred
- 5+ years in NEMT operations or healthcare compliance
- Direct reporting to CEO/Board for independence
- Budget authority for compliance tools and external audits
- Unrestricted access to all operations and records
Core Responsibilities:
- Compliance program development and maintenance
- Training coordination and effectiveness monitoring
- Internal audit oversight and finding remediation
- Investigation coordination for compliance concerns
- Regular reporting to leadership on compliance status
Continuous Monitoring and Improvement
Key Performance Indicators:
| Metric | Target | Monitoring Frequency |
|---|---|---|
| Clean Claim Rate | >98% | Weekly |
| Denial Rate | <3% | Weekly |
| Training Completion | 100% | Monthly |
| Credential Compliance | 100% | Daily |
| Self-Audit Finding Rate | <2% | Quarterly |
| CAP Closure Rate | 100% on time | Monthly |
Continuous Improvement Framework:
- PDCA Cycle: Plan improvements, Do implementation, Check results, Act on findings
- Root cause analysis for all significant findings
- Process mapping for workflow optimization
- Benchmarking against industry standards
- Regular feedback collection from staff
Accountability and Recognition
Performance Integration:
- Compliance metrics in performance evaluations
- 20%+ of bonus/incentive tied to compliance performance
- Progressive discipline for violations (retraining → warning → termination)
- Recognition for compliance excellence (awards, public acknowledgment)
- Career advancement tied to compliance understanding
Recognition Programs:
- Quarterly awards for compliance excellence
- Public acknowledgment of improvements
- Financial incentives for audit success
- Success story sharing and celebration
- Professional development opportunities
NEMT Audit Preparation Questions Answered
What triggers a Medicaid transportation audit?
Medicaid audits typically trigger from automated data analytics that flag billing anomalies such as excessive mileage, overlapping trips, or unusual service ratios. Beyond data triggers, audits result from patient or whistleblower complaints, high-risk provider profiles including new enrollees, random statistical sampling through PERM programs, or referrals from managed care organizations detecting unusual patterns.
How often are NEMT providers audited?
Most NEMT providers face some form of audit annually. Broker audits occur quarterly or semi-annually, state Medicaid reviews happen every 2-3 years for typical providers, and OIG investigations target providers based on risk profiles. High-volume providers or those with previous compliance issues experience more frequent scrutiny, potentially facing multiple audit types simultaneously.
What are the 5 C’s of auditing?
The 5 C’s of auditing are Criteria (the standards being measured against), Condition (what was actually found during examination), Cause (why the discrepancy occurred), Consequence (the financial or safety impact of the finding), and Corrective Action (how the issue will be fixed and prevented from recurring). This framework guides both internal self-audits and external regulatory examinations.
What is the golden rule of auditing?
The golden rule of auditing is: “If it wasn’t documented, it wasn’t done.” Auditors consider undocumented services as presumed non-delivery, regardless of whether the service actually occurred. This principle emphasizes that contemporaneous, complete documentation is the only acceptable proof of service delivery—verbal assertions and post-hoc records carry no weight.
How far back can Medicaid audit?
Medicaid can generally audit 6 years back under federal law, though some states extend this to 10 years for fraud investigations. The False Claims Act allows 10-year lookbacks for fraud cases. Managed care contracts often specify 7-10 year retention requirements. This means you must maintain audit-ready documentation for at least a decade to be fully protected.
How should I prepare for an NEMT audit?
Begin by conducting quarterly self-audits of 2% of your trips, organizing all documentation into digital searchable systems, implementing automated credential tracking for drivers and vehicles, and training staff on proper documentation procedures. Create an audit response team and protocol before any notice arrives. Ensure your EVV/GPS systems meet current standards and verify that your billing processes align with state requirements.
What documents do NEMT auditors request?
Auditors consistently request Physician Certification Statements (PCS), complete trip logs with patient signatures, driver qualification files including licenses and training records, vehicle inspection and maintenance records, GPS/EVV data matching trip logs, billing claims with supporting documentation, prior authorizations, HIPAA compliance evidence, and business enrollment documents. Organize these by category for rapid retrieval.
What is a compliance audit checklist?
A compliance audit checklist is a structured verification tool covering every regulatory requirement across driver qualifications, vehicle safety, trip documentation, billing accuracy, HIPAA compliance, and administrative policies. It serves as both a preparation guide for internal audits and a defense mechanism ensuring nothing is missed when facing external examination.
How do I conduct a self-audit?
Start by selecting a random sample of trips (typically 2% or 200 minimum), then verify each against the “triple match” of authorization, performance (GPS/logs), and billing. Use state Medicaid manual checklists for completeness. Document all findings, categorize by severity, develop corrective action plans, and retest after implementation to verify fixes are effective.
What software helps with NEMT audit preparation?
Leading solutions include Traumasoft for comprehensive compliance features, RouteGenie for EVV integration, Tobi Cloud for AI-driven automation, TripSpark for routing and mileage verification, and AngelTrack for HIPAA-secure operations. These platforms automate credential tracking, documentation management, claims scrubbing, and audit report generation. See our detailed NEMT software comparison for feature analysis.
What do Medicaid auditors look for?
Auditors examine medical necessity justification through valid PCS forms, service delivery proof through complete logs with signatures and GPS verification, provider qualifications including current credentials for drivers and vehicles, billing accuracy with correct codes and mileage, and system integrity through EVV/GPS functionality. They reconstruct each sampled trip to verify the service occurred as billed.
What not to say during an audit?
Never admit fault, speculate about errors, volunteer unrequested information, or discuss findings informally. Avoid phrases like “We always do it this way” if it contradicts written policy. Don’t guess at answers—instead say “I’ll verify that information and provide documentation.” Never discuss potential penalties or acknowledge systemic problems without legal guidance.
What raises a red flag for an audit?
Major red flags include billing anomalies like sudden volume spikes or perfect mileage rounding, high denial rates exceeding 23%, complaint patterns from patients or staff, ownership changes, geographic clustering in known high-fraud areas, and data inconsistencies detected by automated monitoring. Any pattern suggesting services weren’t delivered as billed draws immediate attention.
How long does an NEMT audit take?
Timelines vary significantly: desk audits typically take 30-60 days, on-site audits 3-6 months from notice to findings, and comprehensive OIG investigations 6-12 months or longer. Appeals can add another 6-12 months. The total process from initial notice to final resolution often spans 9-18 months for complex cases.
What happens during an on-site audit?
Auditors physically inspect facilities and vehicles, review original documents, interview dispatchers and drivers (always with escorts present), observe operations, test EVV and GPS systems, verify vehicle compliance including ADA equipment, and examine physical record storage security. They may request ride-alongs to observe actual service delivery.
What happens if you fail an NEMT audit?
Consequences include financial recoupment often calculated through statistical extrapolation, mandatory Corrective Action Plans, payment suspensions ranging from 10-100% withholding, contract terminations with brokers, potential OIG exclusion from all federal healthcare programs, and in severe cases, criminal prosecution under the False Claims Act with treble damages.
How do I appeal audit findings?
File a written appeal within the specified timeframe (typically 30-60 days depending on state), provide documentary evidence contradicting findings, challenge statistical methodology if applicable, and request an Administrative Law Judge hearing if available. Consider engaging legal counsel for significant findings. Appeals succeed in 30-50% of cases with proper documentation.
What is a Corrective Action Plan (CAP)?
A CAP is a formal document detailing how you will fix identified deficiencies. Required components include root cause analysis identifying why the problem occurred, specific corrective actions with responsible parties and deadlines, verification methods proving implementation, and prevention strategies ensuring issues don’t recur. CAPs typically require completion within 30-90 days.
How are recoupment amounts calculated?
Auditors typically use statistical extrapolation, applying the error rate found in a sample to your entire claims universe for the audit period. For example, a 10% error rate found in a 50-claim sample could be applied to 10,000 claims, dramatically multiplying the recoupment amount. The Lower Confidence Limit method provides some statistical protection but still results in substantial recovery demands.
Can audit failures lead to Medicaid exclusion?
Yes, repeated compliance failures or evidence of fraud can lead to OIG exclusion, which bars you from all federal healthcare programs for a minimum of 5 years and often permanently. Exclusion effectively ends your ability to operate as an NEMT provider serving Medicaid patients and triggers immediate contract terminations with all payers.
What training is required for NEMT compliance?
Mandatory training includes HIPAA privacy and security (annual), PASS certification (8-16 hours initially with refreshers), CPR/First Aid (2-year renewal), defensive driving (3-year renewal), wheelchair securement for applicable staff, bloodborne pathogens (annual), and fraud awareness training. Document all training with signed completion records retained for at least 6 years.
How should driver files be organized for audits?
Organize digitally by driver with separate sections for licenses/MVRs (updated annually), background checks (7-year retention), drug tests (5-year retention for negative, 1 year for positive), training certificates (indefinite retention), and exclusion checks (monthly verification documentation). Use a checklist for each file to ensure completeness and track expiration dates systematically.
What vehicle documentation is required?
Maintain daily DVIRs (3-month minimum retention), annual or semi-annual state inspection certificates, ADA lift certifications with quarterly load testing, preventive maintenance logs following manufacturer specifications, current insurance certificates, registration documents, and safety equipment verification records. Organize by vehicle identification number for easy retrieval.
How does HIPAA apply to NEMT audits?
HIPAA requires protection of all Protected Health Information on trip logs, dispatch systems, and billing records. Auditors verify encryption at rest and in transit, access controls, Business Associate Agreements with all vendors handling PHI, staff training documentation, annual risk assessments, and breach response capabilities. HIPAA violations during audits can trigger separate OCR investigations and additional penalties.
What are common NEMT audit findings?
The most frequent findings include missing patient signatures (55% of audits), mileage exceeding GPS distance (68%), expired PCS forms (42%), incomplete driver credential files (35%), missing vehicle inspection records (40%), duplicate billing (25%), service level mismatches between PCS and claims (22%), and inadequate HIPAA safeguards (45%).
Additional Questions
What are the 7 steps in the audit process?
The seven steps in the NEMT audit process are planning (defining scope and objectives), notification (formal notice to the provider), fieldwork (document collection and verification), analysis (comparing findings against requirements), reporting (preliminary findings documentation), response (provider opportunity for rebuttal), and resolution (final determination and corrective actions). Each step has specific timelines and requirements that vary by state and audit type.
What are the 3 C’s of auditing?
The 3 C’s of auditing represent Compliance (adherence to regulatory requirements), Completeness (thorough documentation of all service elements), and Consistency (uniform application of standards across all operations). These three principles guide auditor evaluation—every trip must demonstrate compliance with applicable rules, complete documentation proving service delivery, and consistent application of procedures regardless of driver, vehicle, or patient.
What is most likely to trigger an audit?
Billing anomalies detected by automated monitoring systems are most likely to trigger NEMT audits. Specifically, patterns like consistent mileage rounding, geographic impossibilities where trip times don’t match distances, sudden volume increases, duplicate claims for the same service, and unusually high ratios of premium services to basic transportation draw immediate algorithmic attention and human review.
Why would someone get kicked off of Medicaid?
NEMT providers get excluded from Medicaid for fraudulent billing practices including phantom trips and upcoding, kickback schemes with referral sources, quality of care violations endangering patients, criminal convictions related to healthcare, professional license revocations, or repeated compliance failures despite corrective action opportunities. Exclusion bars the provider from all federal healthcare programs.
What is the biggest problem with Medicaid audits?
The biggest problem with Medicaid audits is statistical extrapolation, where error rates found in small samples get multiplied across entire claim universes. This methodology can transform minor documentation deficiencies into six-figure recoupment demands. A provider might have excellent overall compliance but face catastrophic financial consequences if the randomly selected sample happens to contain disproportionate errors.
How do I know if I’m being investigated by Medicaid?
Indications of Medicaid investigation include unusual document requests from payers without clear explanation, unexplained payment delays, reports from employees about inquiries from investigators, notification from professional licensing boards, formal audit notices, or contact from law enforcement. However, investigations often proceed secretly until evidence gathering is complete, so absence of obvious signs doesn’t guarantee you’re not under review.
Can you get audited for Medicaid?
Yes, all Medicaid providers face audit risk regardless of size or history. Audit probability increases based on billing volume, service types offered, geographic location in high-fraud areas, previous compliance issues, complaint history, and random statistical sampling programs. No provider is exempt—the question is not whether you’ll face audit but when and how prepared you’ll be.
What are the 4 types of audits?
The four primary audit types are financial audits examining billing accuracy and claims integrity, compliance audits verifying regulatory adherence across all operational areas, operational audits assessing process efficiency and effectiveness, and investigative audits targeting potential fraud or abuse. Each type uses different methodologies and has different implications for providers.
How to do an audit of a transport company?
To audit a transport company, begin with document review examining trips, driver credentials, and vehicle records. Then verify findings through field observation including ride-alongs and facility inspections. Interview staff using structured questions about procedures and training. Analyze data by comparing GPS records to billing claims. Test systems to verify EVV functionality. Finally, compile findings with severity classifications and improvement recommendations.
What are the 5 audit threats?
The five audit threats include detection risk (failure to identify existing issues), sampling risk (unrepresentative sample selection), non-sampling risk (procedural errors in audit execution), fraud risk (intentional deception by auditees), and compliance risk (regulatory violations not identified). Each threat requires specific mitigation strategies by both auditors and the organizations being audited.
What are the do’s and don’ts during an audit?
Do organize documents proactively, designate a single point of contact, answer questions honestly and concisely, document all interactions with auditors, maintain professional demeanor, and request clarification when questions are unclear. Don’t volunteer unrequested information, admit fault or speculate about errors, allow unsupervised auditor access, alter or destroy any records, discuss findings informally, or obstruct the audit process in any way.
Conclusion: Your NEMT Audit Preparation Action Plan
Prioritized Implementation Framework
Audit preparation in 2026 requires systematic, ongoing effort rather than last-minute scrambling. Based on everything covered in this guide, here’s your prioritized action plan:
Immediate Actions (First 30 Days):
- Conduct a comprehensive compliance gap analysis using the checklists in this guide
- Implement automated credential tracking for all drivers with hard-stop dispatch controls
- Establish quarterly self-audit schedule with 2% trip sampling minimum
- Organize all documentation into digital, searchable systems with consistent naming
- Designate and train your audit response team before you need them
Short-Term Improvements (Months 2-3):
- Implement EVV/GPS systems meeting 2026 standards if not already compliant
- Develop comprehensive training programs for all staff levels
- Create formal policies and procedures manual covering all compliance areas
- Establish continuous monitoring dashboards tracking key compliance KPIs
- Execute Business Associate Agreements with all vendors handling PHI
Ongoing Excellence (Months 4-12):
- Refine processes based on self-audit findings
- Enhance technology integration and automation
- Build compliance culture through recognition and accountability
- Develop relationships with legal and consulting resources
- Establish industry benchmarking and continuous improvement practices
The Competitive Advantage of Compliance
In the increasingly regulated NEMT marketplace, robust compliance preparation transforms from a defensive necessity to a strategic differentiator. Providers who excel at audit readiness experience higher broker contract renewal rates, faster payment cycles, lower operational costs through efficiency, reduced staff turnover through clear expectations, and enhanced market reputation enabling growth.
Your commitment to comprehensive audit preparation today directly determines your business viability tomorrow.
Professional Support Resources
For providers who need expert assistance with audit preparation, compliance program development, or billing optimization, Elite Med Financials offers comprehensive NEMT billing services designed to help transportation providers build robust compliance programs that withstand even the most rigorous audits.
Whether you need help with broker billing requirements, understanding Medicare Advantage NEMT benefits, or learning how patients book NEMT services, our team provides the expertise to transform compliance from your greatest vulnerability to your most valuable competitive advantage.
Downloadable Resources and Checklists
Essential Audit Preparation Tools
To support your NEMT audit preparation efforts, use these essential resources alongside this guide:
Primary Checklists:
- Driver Qualification File Checklist (Section 4 of this guide)
- Vehicle Inspection Compliance Checklist (Section 5)
- Trip Documentation Required Fields (Section 6)
- HIPAA Compliance Checklist (Section 7)
- Self-Audit Execution Framework (Section 8)
Related Resources:
- Complete NEMT Billing Guide – Detailed claims processing standards
- NEMT Compliance Guide – Comprehensive regulatory overview
- NEMT Denial Codes Guide – Understanding and preventing rejections
- State-by-State Medicaid NEMT Rates – Reimbursement standards
- Best NEMT Software Comparison – Technology solutions guide
External Authority References
For additional regulatory guidance and enforcement information:
- CMS Medicaid Transportation Coverage Guide – Federal program requirements
- HHS OIG Reports and Work Plan – Enforcement priorities and audit findings
This guide was developed by Elite Med Financials, specialists in healthcare revenue cycle management and NEMT compliance. For personalized audit preparation assistance or comprehensive billing services, contact our team for a consultation.

